
Abstract
Introduction
The objective of this study was to review and synthesize the current best evidence for the use of intraoperative navigation in the implantation of glenoid components in total shoulder prostheses.
Methods
We conducted a systematic, online search using PubMed, EMBASE, CCTR, and CINAHL using “Arthroplasty, Replacement”(Mesh) AND (shoulder) AND (navi* OR computer). Data on study design and quality as well as accuracy of positioning and complications were extracted independently and in duplicate. After assessment of study heterogeneity, DerSimonian-Laird random effect models were used to pool data from the individual studies.
Results
The systematic search revealed 359 manuscripts in total. After exclusion of duplicates and irrelevant publications, 6 groups of 247 shoulders from 5 studies were included. The pooled weighted mean difference for deviation from neutral version was −6.4° (95 %CI −7.9 to −5.3) in favor of navigation, which is consistent with a statistically significant difference (p < 0.01). In the navigation group, 2 superior glenoid screws were reported as perforating compared to 5 screws (1 inferior, 4 superior) in the control group. There was no difference in tilt at a WMD of 2.7 (95 %CI −1.4 to 6.8, p = 0.192).
Conclusions
Navigation allows for significantly more accurate glenoid version, but the clinical meaningfulness of the absolute improvement over standard techniques is questionable. However, navigation is a valuable teaching tool that might prove very beneficial not for the patient at hand, but for those treated by the operating surgeon in the future.
Level of evidence
Level II—meta-analysis of non-homogenous controlled trials.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Total shoulder replacement is an extremely successful treatment for glenohumeral osteoarthritis with consistent improvement of pain and function postoperatively [4]. However, symptomatic loosening and surgical revision occurred at roughly 1 % per year [23]. The most common reason for failure and revision of total shoulder replacement is failure of the glenoid component [18]. Various reasons for glenoid failure have been proposed, but not all were substantiated in later research [28].
Recent evidence showed that component design has a significant effect on loosening and revision, with pegged components being significantly better than keeled ones [28]. Cementation has been controversially discussed, but the prevailing part of the current evidence shows better results, i.e., less revisions, with sparingly cementing the glenoid [2, 15]. Radiolucency, however, seems to be a finding independent of later glenoid failure [28]. Castagna et al. showed very good results with a metal back glenoid component without implant associated problems [5].
One seemingly obvious risk factor for glenoid failure is, in consistency with other prostheses, is malpositioning of the component during implantation. Glenoid placement in total shoulder replacement is complicated by the often poor bone stock and changed anatomy of the glenoid, the lack of static anatomic landmarks, and the limited exposure of the shoulder [18]. As with other procedures with challenging surgical device positioning, intraoperative navigation has been suggested to aid with implantation [26]. A number of studies have tested the use of such techniques in shoulder replacement, but have produced inconsistent findings.
The objective of this study was to review and synthesize the current best evidence for the use of intraoperative navigation in the implantation of glenoid components in total shoulder prostheses. We hypothesize that navigation will lead to significantly better placement, i.e., version and inclination or tilt, of the glenoid component compared to standard surgical techniques.
Materials and methods
This study was conducted following the PRISMA statement published by the CONSORT group [14, 19].
Systematic search and strategy
We conducted a systematic review of the literature using the online databases PubMed, MEDLINE, EMBASE, CINAHL (Cumulative Index of Nursing and Allied Health), and CCTR (Cochrane Controlled Trial Register). We searched these electronic databases online for “(Arthroplasty, Replacement”[Mesh]) AND (shoulder) AND (navig* OR computer)” using these terms as keywords and exploded MeSH terms without restrictions in language or year of publication. The last search was performed on March 14, 2014.
We included studies directly comparing navigated versus standard total shoulder arthroplasty. In case of overlapping data, studies were merged as far as possible; completely overlapping studies were excluded. Further exclusion criteria were duplicates, no focus on positioning outcome, and studies with unacceptable high data attrition (>20 %). Eligible interventions were all total shoulder systems.
Extraction of relevant data
Eligibility of studies was assessed independently and in duplicate (PS, PV) and crosschecked to avoid errors. Disagreement was resolved by discussion or, if necessary, with the help of the senior author (PV). The bibliographies of all included studies were reviewed for additional relevant studies.
In detail, the following variables were extracted to describe study quality: level of evidence (I–V), randomization (yes/no), blinding (yes/no), attrition (yes/no), and power analysis (yes/no). Outcome data extracted were study size, type of prosthesis, version of implant, tilt of implant, and error in positioning.
Assessment of validity
We determined the level of evidence for all studies which were included and internal validity was further assessed using a modified Jadad scale, which ranges from 0 points (poorest result) to 3 points (best result), attributing 1 point for each randomization, blinding, and attrition [12].
Publication bias
An important threat for the validity of any meta-analysis is publication bias, also referred to as “file-drawer” bias, which means bias because of unidentified or unpublished studies. More often than not studies remain “in a desk drawer” because their results failed to reach statistical significance, causing an exaggerated high proportion of studies with significant results in the literature [27]. Publication bias among the included studies was assessed graphically using funnel plots and mathematically using Egger’s weighted regression [7].
Study heterogeneity
The presence of between-study heterogeneity was qualified by Cochrane’s Q test, using a p value of 10 % to adjust for the low power of this test in small samples, and quantified using the I 2 index. To assess the potential sources of such heterogeneity, meta-regressions were performed.
Quantitative data synthesis
To pool data, random effects models using the DerSimonian-Laird (random effects) method were constructed. These models postulate that the observed heterogeneity between studies in a meta-analysis is attributable to normally distributed individual effects around a common effect [6]. This assumption was assessed graphically in the forest plots.
All analyses were done per intention-to-treat, i.e., participants were included in the analysis by their initial allocation and their status at the final follow-up. Such an analysis produces a more conservative result with larger p values, but is also more realistic. For all endpoints we calculated weighted mean differences in degrees. All analyses were done for anatomical and reverse designs individually.
All calculations were performed using Intercooled STATA® 12 (StataCorp LP, College Station, TX). The level of significance for pooled estimates was set at 5 %.
Results
Study characteristics
Our search strategy generated 359 studies online and by citation tracking. After exclusion of duplicates, studies not focusing on clinical treatment or outcome, animal studies, studies without any intervention and one study with unacceptable high attrition, nine studies remained for analysis. The included 6 groups of 247 shoulders from 5 studies were published in between 2007 and 2013 in English.
Description of included studies
Anatomic TSA
Verborgt et al. investigated the influence of navigation on accuracy of placement of the glenoid component in reversed shoulder arthroplasty (RSA) by implanting RSA in 14 paired scapulohumeral cadaver specimens [29]. They studied glenoid component version and tilt and screw placement using CT scan and dissection and found computer navigation to be more accurate and more precise than standard instrumentation.
Kircher et al. performed a prospective, randomized clinical study of 2 groups of 10 patients each to investigate the accuracy of the glenoid positioning in the transverse plane using intraoperative navigation [13]. They measured glenoid version on axial CT scans preoperatively and 6 weeks postoperatively and found an improved accuracy in glenoid positioning in the transverse plane using intraoperative navigation.
In 2009, Ngyuen et al. tried to evaluate a computer-assisted technique to achieve a more accurate placement of the glenoid component in a cadaver study [22]. They randomly implanted in a traditional or computer-assisted technique and found it to be more accurate in achieving the correct version during all phases of glenoid implantation. They concluded that computer-assisted navigation leads to more accurate glenoid component placement in relation to traditional techniques.
Hoenecke et al. virtually implanted 3 different glenoid designs into 3-dimensional computed tomography-reconstructed models of 40 normal scapulae [10]. In addition, they performed cadaveric surgeries to measure glenoid width and height. The authors measured the incidence of perforation, malalignment of implants, and medialization of the implants. They found that the same scapulae that perforated during cadaveric surgery also perforated during virtual surgery and concluded that their results emphasize the need for accurate preoperative templating and for developing surgical navigation to improve implant fixation.
Reverse TSA
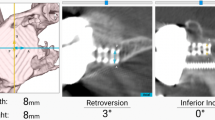
In 2013, Stübig et al. performed an in vitro on 3D navigated implantation of the glenoid in reversed shoulder arthroplasty [25]. Therefore, 27 implantations were undertaken using a Kirschner wire (12 cases) or by using a navigated drill (15 cases). They measured the position of the Kirschner wire and the insertion point of the glenoid. They found no significant difference between groups with respect to the glenoid drilling distance and the inferior tilt. However, in case of the axial plane they found significantly higher accuracy in the navigated group and conclude that accurate positioning of the glenoid baseplate might be improved in the axial plane using navigation. The parameters of these included studies are described in Table 1.
Publication bias
There was no evidence for publication bias for version (p = 0.543), tilt (p = 1.0), or error (p = 0.478) in Egger’s regression.
Heterogeneity
Between studies heterogeneity was not statistically significant for version (p = 0.586) with an I 2 index of 0 % or for error of placement (p = 0.735, I 2 = 0 %), even with anatomic and reverse designs pooled together, suggesting a common effect of navigation across both implant designs.
Pooled effect
Data for glenoid version were available for 117 navigated shoulder prostheses and 114 standard procedures. All procedures aimed at a neutral version of 0°. The weighted mean version of the navigated shoulders was 4.4 ± 0.41 (95 %CI 3.6–5.3). The weighted mean version of the standard shoulders was 10.6 ± 0.67 (95 %CI 9.3–11.9). The pooled weighted mean difference for deviation from neutral version for both anatomic and reversed designs was −6.4° (95 %CI −7.9 to −5.3) in favor of navigation, which is consistent with a statistically significant difference (p < 0.01). Broken into subgroups, this effect was −6.3° (95 %CI −7.6 to −5.0, p < 0.01) in favor of navigation for anatomical shoulder prostheses, and −9.9° (95 %CI −14.3 to −5.6, p < 0.01) for reverse designs. (Fig. 1).

Forest plot of the pooled effect of navigation. Horizontally, the effects from the individual studies are depicted, with a pooled average along the vertical dotted line. The solid vertical line represents a null effect, everything to the left favors navigation, to the right standard technique
Data for glenoid inclination were available for 22 navigated shoulder prostheses and 19 standard procedures. All procedures aimed at a neutral inclination. The weighted mean inclination of the navigated glenoids was 5.4 ± 0.54 (95 %CI 4.3–6.5). The weighted mean version of the standard shoulders was 1.3 ± 0.78 (95 %CI −0.2 to 2.9). This was consistent with a pooled weighted mean difference for inclination of 3.5° (95 %CI 1.5–5.4) in favor of navigation, which is consistent with a statistically significant difference (p < 0.01).
There was also a beneficial and statistically significant effect of navigation on the range of error in positioning, which was reduced by 5.2° (95 % 3.0–7.2) on average through the use of navigation (p < 0.001).
In the navigation group, 2 superior glenoid screws were reported as perforating compared to 5 screws (1 inferior, 4 superior) in the control group. However, all of them were reported from one study of 7 and 7 prostheses, with no further reporting of this complication in the other papers. Hence we refrained from formal analysis of this observation.
Finally, there was no difference in tilt at a WMD of 2.7 (95 %CI −1.4 to 6.8, p = 0.192).
Discussion
Summary of evidence
In this study was found strong evidence for a statistically beneficial effect of intraoperative navigation on glenoid positioning in both anatomic and reverse designs, confirming our study hypothesis. Briefly, navigation resulted in a better version of the glenoid as well as a lower range of error for implant version and inclination.
Total shoulder arthroplasty is an enormously successful treatment for the pain and dysfunction caused by arthritis of the glenohumeral joint. However, in contrast to the substantial effect on pain and function stands the risk of implant loosening and the need for subsequent revision. The most common reason for the revision of a shoulder prosthesis is glenoid loosening [18].
Among the most common reasons for glenoid loosening, in turn, is initial imperferct positioning of the glenoid component [18]. Positioning of the glenoid is complicated by the lack of reliable, static landmarks on the shoulder, the scarcity of bone stock, typically altered during the course of the disease, and the limited access to the scapula through any of the available approaches to the shoulder. Thus, interoperative navigation using computers or CT has been suggested to mend these problems, improve implant positioning and therefore, hopefully, increase implant survival.
Since the same factors—altered anatomy, missing landmarks, limited exposure—affect both procedures, anatomic and reverse implants, very similarily, we were not surprised to see very similar effects of navigation on implant position. Furthermore, navigation did not only lead to more accurate placement, but also to more reliable results, i.e., a reduction in the range of error of positioning. The difference in these seemingly redundant endpoints is important for the following reasons. While we did see a significant improvement in version statistically, we cannot gauge the clinical relevance of the extent of this change at roughly 6°. Moska et al. [21], as well as Gregroy et al. [8], have suggested that version in excess of 20° is associated with poorer outcomes, but no clear cut correlation between extent of version and risk of failure has been established yet, suggesting that some error in positioning is tolerated.
One important endpoint that has sadly been disregarded in most of the pertinent literature is hardware penetration, be it screws or the glenoid component itself, through the scapula. More often than not, the severe bone loss seen with advanced OA of the shoulder necessitates some deviation from neutral version to achieve better bone purchase. Also, a perfectly level component per se will not guarantee the best outcome if one or more screws affect periscapular structures, including nerves and vessels. Molonly et al. reported on the risk of suprascapular nerve damage by superior glenoid component screws, which often travel as close as 2 mm from the nerve [20]. Wang et al. report on a case of suprascapular nerve damage by a perforating superior screw in a patient receiving a reverse total shoulder replacement [30]. Hart et al. showed that in 3 out of 10 cadaveric specimens, a posterior screw touched either the suprascapular nerve or artery. These potentially catastrophic complications should be included in glenoid positioning [9].
The most commonly discussed point in navigated total joint replacement, be it for the shoulder or any other joint, is if the added complexity and increased OR time is offset by the incremental clinical benefit. Our data suggested that the improvement in version is statistically significant, but at 6° not substantial in size. Prior similar discussion of navigation for total knee replacement have shown that somewhat axiomatically chosen cut offs for increased risk of failure, such as 2° of valgus/varus for the knee, were not substantiated in large registry analyses [1, 17]. The same might very well be true for the shoulder, showing that a 6° change in version might not effect glenoid loosening substantially, especially in comparison to other risk factors such as cementing technique or implant design [28]. Unfortunately, no data exist on either changes in operative time or costs or failure rates with navigated and standard shoulder replacement banning an ideas of a cost-effectiveness analysis into the realm of speculative interpretation.
One beneficial aspect of navigated total joint replacement that has not been measured, or even mentioned, is its use as a teaching tool. While most high volume orthopedic surgeons will agree that navigation will not lead to a meaningful clinical improvement over standard procedures in but the worst cases, there is also considerable inherent agreement that the additional, quantitative visualization of the procedure is a valuable tool to improve surgical skills. Love et al. showed that computer navigation increases awareness to surgical errors such as moving cutting blocks or poor block fixation [16]. Schnurr et al. showed that computer navigation substantially improved accuracy of residents during early experiences with total knee replacement [24]. May be more interestingly, Iorio et al., in 2103, showed that the use of computer navigation can even improve surgical accuracy in surgeons with a wealth of TJR experience [11]. While it is likely that such a beneficial effect exists for total shoulder replacement as well, no data have been collected formally yet to support this notion.
Limitations
Our study has potential shortcomings. Like any meta-analyses, the validity of our findings depends on the validity of the primary studies. While the overall study quality of the included studies is low, such grading is not unusual, or not representative for that matter, for investigators of surgical and musculoskeletal issues. Secondly, the number of publications in this field is limited, and there is clinical heterogeneity. However, our formal assessment of heterogeneity has shown that a meta-analysis of the included data is possible and valid.
Conclusion
Navigation improves glenoid placement accuracy with statistical significance, but the clinical meaningfulness of the absolute improvement over standard techniques is questionable. However, navigation is a valuable teaching tool that might prove very beneficial not for the patient at hand, but for those treated by the operating surgeon in the future.
References
Bauwens K, Matthes G, Wich M, Gebhard F, Hanson B, Ekkernkamp A et al (2007) Navigated total knee replacement. A meta-analysis. J Bone Joint Surg Am 89:261–269. doi:10.2106/JBJS.F.00601
Boileau P, Avidor C, Krishnan SG, Walch G, Kempf JF, Mole D (2002) Cemented polyethylene versus uncemented metal-backed glenoid components in total shoulder arthroplasty: a prospective, double-blind, randomized study. J Shoulder Elb Surg 11:351–359. doi:10.1067/mse.2002.125807
Briem D, Ruecker AH, Neumann J, Gebauer M, Kendoff D, Gehrke T, Lehmann W, Schumacher U, Rueger JM, Grossterlinden LG (2011) 3D fluoroscopic navigated reaming of the glenoid for total shoulder arthroplasty (TSA). Comput Aided Surg 16(2):93–99. doi:10.3109/10929088.2010.546076
Bryant D, Litchfield R, Sandow M, Gartsman GM, Guyatt G, Kirkley A (2005) A comparison of pain, strength, range of motion, and functional outcomes after hemiarthroplasty and total shoulder arthroplasty in patients with osteoarthritis of the shoulder. A systematic review and meta-analysis. J Bone Joint Surg Am 87:1947–1956. doi:10.2106/JBJS.D.02854
Castagna A, Randelli M, Garofalo R, Maradei L, Giardella A, Borroni M (2010) Mid-term results of a metal-backed glenoid component in total shoulder replacement. J Bone Joint Surg Br 92:1410–1415. doi:10.1302/0301-620X.92B10.23578
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Egger M, Davey Smith G, Schneider M, Minder C (1997) Bias in meta-analysis detected by a simple, graphical test. BMJ 315:629–634
Gregory TM, Sankey A, Augereau B, Vandenbussche E, Amis A, Emery R et al (2013) Accuracy of glenoid component placement in total shoulder arthroplasty and its effect on clinical and radiological outcome in a retrospective, longitudinal, monocentric open study. PLoS One 8:e75791. doi:10.1371/journal.pone.0075791
Hart ND, Clark JC, Wade Krause FR, Kissenberth MJ, Bragg WE, Hawkins RJ (2012) Glenoid screw position in the Encore Reverse Shoulder Prosthesis: an anatomic dissection study of screw relationship to surrounding structures. J Shoulder Elb Surg 22:814–820. doi:10.1016/j.jse.2012.08.013
Hoenecke J, Heinz R, Hermida JC, Dembitsky N, Patil S, D’Lima DD (2008) Optimizing glenoid component position using three-dimensional computed tomography reconstruction. J Shoulder Elb Surg 17:637–641. doi:10.1016/j.jse.2007.11.021
Iorio R, Mazza D, Bolle G, Conteduca J, Redler A, Conteduca F et al (2013) Computer-assisted surgery: a teacher of TKAs. Knee 20:232–235. doi:10.1016/j.knee.2012.06.009
Jadad AR, Cook DJ, Jones A, Klassen TP, Tugwell P, Moher M et al (1998) Methodology and reports of systematic reviews and meta-analyses: a comparison of Cochrane reviews with articles published in paper-based journals. JAMA 280:278–280
Kircher J, Wiedemann M, Magosch P, Lichtenberg S, Habermeyer P (2009) Improved accuracy of glenoid positioning in total shoulder arthroplasty with intraoperative navigation: a prospective-randomized clinical study. J Shoulder Elb Surg 18:515–520. doi:10.1016/j.jse.2009.03.014
Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC, Ioannidis JP et al (2009) The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med 6:e1000100. doi:10.1371/journal.pmed.1000100
Litchfield RB, McKee MD, Balyk R, Mandel S, Holtby R, Hollinshead R et al (2011) Cemented versus uncemented fixation of humeral components in total shoulder arthroplasty for osteoarthritis of the shoulder: a prospective, randomized, double-blind clinical trial-A JOINTs Canada Project. J Shoulder Elb Surg 20:529–536. doi:10.1016/j.jse.2011.01.041
Love GJ, Kinninmonth AW (2013) Training benefits of computer navigated total knee arthroplasty. Knee 20:236–241. doi:10.1016/j.knee.2012.09.012
Mason JB, Fehring T, Fahrbach K (2007) Navigated total knee replacement. J Bone Joint Surg Am 89:2547–2548 (discussion 48–50. 89/11/2547-a pii)
Matsen FA 3rd, Clinton J, Lynch J, Bertelsen A, Richardson ML (2008) Glenoid component failure in total shoulder arthroplasty. J Bone Joint Surg Am 90:885–896. doi:10.2106/JBJS.G.01263
Moher D, Liberati A, Tetzlaff J, Altman DG, Group P (2009) Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ 339:b2535
Molony DC, Cassar Gheiti AJ, Kennedy J, Green C, Schepens A, Mullett HJ (2011) A cadaveric model for suprascapular nerve injury during glenoid component screw insertion in reverse-geometry shoulder arthroplasty. J Shoulder Elb Surg 20:1323–1327. doi:10.1016/j.jse.2011.02.014
Moska M, Duckworth D, Matsen F (1998) Contrasting the position of prosthetic joint surfaces in successful and failed shoulder arthroplasties. In: 7th International Congress on Shoulder Surgery, Sydney
Nguyen D, Ferreira LM, Brownhill JR, King GJ, Drosdowech DS, Faber KJ et al (2009) Improved accuracy of computer assisted glenoid implantation in total shoulder arthroplasty: an in vitro randomized controlled trial. J Shoulder Elb Surg 18:907–914. doi:10.1016/j.jse.2009.02.022
Papadonikolakis A, Neradilek MB, Matsen FA 3rd (2013) Failure of the glenoid component in anatomic total shoulder arthroplasty: a systematic review of the English-language literature between 2006 and 2012. J Bone Joint Surg Am 95:2205–2212. doi:10.2106/JBJS.L.00552
Schnurr C, Eysel P, Konig DP (2011) Do residents perform TKAs using computer navigation as accurately as consultants? Orthopedics 34:174. doi:10.3928/01477447-20110124-05
Stübig T, Petri M, Zeckey C, Hawi N, Krettek C, Citak M et al (2013) 3D navigated implantation of the glenoid component in reversed shoulder arthroplasty. Feasibility and results in an anatomic study. Int J Med Robot Comput Assist Surg 9:480–485. doi:10.1002/rcs.1519
Vavken P, Dorotka R Modeling the “minimally invasive surgery effect” in total joint replacement. Surgical Innovation 2011 (ahead of print)
Vavken P, Dorotka R (2011) The prevalence and effect of publication bias in orthopaedic meta-analyses. J Orthop Sci. doi:10.1007/s00776-011-0040-8
Vavken P, Sadoghi P, von Keudell A, Rosso C, Valderrabano V, Muller AM (2013) Rates of radiolucency and loosening after total shoulder arthroplasty with pegged or keeled glenoid components. J Bone Joint Surg Am 95:215–221. doi:10.2106/JBJS.L.00286
Verborgt O, De Smedt T, Vanhees M, Clockaerts S, Parizel P, Van Glabbeek F (2011) Accuracy of placement of the glenoid component in reversed shoulder arthroplasty with and without navigation. J Shoulder Elb Surg 20:21–26. doi:10.1016/j.jse.2010.07.014
Wang J, Singh A, Higgins L, Warner J (2010) Suprascapular neuropathy secondary to reverse shoulder arthroplasty: a case report. J Shoulder Elb Surg 19:e5–e8. doi:10.1016/j.jse.2009.10.004
Acknowledgments
This project was funded by the “Forschungsförderung 2012” of the Association for Orthopaedic Research (AFOR).
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sadoghi, P., Vavken, J., Leithner, A. et al. Benefit of intraoperative navigation on glenoid component positioning during total shoulder arthroplasty. Arch Orthop Trauma Surg 135, 41–47 (2015). https://doi.org/10.1007/s00402-014-2126-1
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00402-014-2126-1