
Abstract
Purpose
Posterior fossa ependymomas (PFE) are among the most frequently occurring solid tumors in children. Their definitive treatment is surgical excision and adjuvant radio-chemotherapy. This study aimed to investigate prognostic effects of age, H3K27me3 status, extent of resection, radiation treatment (RT), Ki67 index, WHO grade, and ATRX and H3K27M mutations in PFE patients.
Methods
This retrospective study included 42 pediatric patients with PFE who had undergone operation at our institution between 1996 and 2018. Patient demographics and treatment information were obtained from patient notes. Information on radiological location of tumors (median vs paramedian), extent of tumor resection, and recurrence was obtained from preoperative and postoperative magnetic resonance imaging. Formalin-fixed paraffin-embedded tumor samples were evaluated for H3K27me3 immunostaining, Ki67 index, WHO grades, and ATRX and H3K27M mutations. Tumor samples with global reduction in H3K27me3 were grouped as posterior fossa ependymoma group A (PFA) and those with H3K27me3 nuclear immunopositivity as posterior fossa ependymoma group B (PFB). We evaluated the cohort’s 5-year progression-free survival (PFS) and overall survival (OS).
Results
There were 20 (47.6%) female and 22 (52.4%) male patients in the cohort. The mean age of patients was 4.4 (range, 0.71–14.51) years. Overall, tumors in 31 (73.8%) and 11 (26.2%) patients were found to be PFA and PFB, respectively. There was no statistically significant age or sex difference between PFA and PFB. All patients received chemotherapy, whereas only 28 (66.6%) received RT. The WHO grades of PFA were statistically higher than those of PFB. There was no significant difference between PFA and PFB in terms of extent of resection, disease recurrence, and survival parameters. Nine of 42 tumor samples had ATRX mutations. One patient with PFA showed H3K27M mutation. Age, WHO grade, H3K27me3 status, and RT had no effect on patients’ PFS and OS. Patients with total surgical excisions had significantly better PFS and OS rates. Those with Ki67 < 50% also had better OS rates.
Conclusions
Determining H3K27me3 status by immunohistochemistry is a widely accepted method for molecular subgrouping of PFEs. Most of the reports in the literature state that molecular subgroups of PFEs have significantly different clinical outcomes. However, in our present series, we have shown that the extent of surgical excision is still the most important prognostic indicator in PFEs. We also conclude that the prognostic effect of H3K27me3 status–based molecular subgrouping may be minimized with a more aggressive surgical strategy followed in PFAs.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ependymomas account for almost 4.7% of primary intracranial tumors diagnosed within the pediatric and adolescent age group (0–19 years) [1]. Their incidence tends to decrease with age from 5.6% (0–14 years) to 4.5% (15–19 years) [2]. They are tumors of glial origin that are thought to develop from embryonic radial glial cells residing within the subventricular zone [3]. Nearly 60% of all pediatric ependymomas are within the posterior fossa [4]. Posterior fossa ependymomas (PFEs) are categorized histopathologically as grade II or grade III according to the presence or absence of necrosis and the frequency of mitotic figures. [5]. The classical treatment strategy is gross total surgical resection followed by adjuvant radiation treatment (RT) with or without chemotherapy [6, 7]. With all current treatment modalities, the 5-year progression-free survival (PFS) rates range between 26 and 57% [8, 9]. The most important prognostic indicator for PFEs is the extent of the surgical resection that was followed by RT [7, 8, 10, 11]. Although the histological grade was first postulated as a prognostic indicator, given that there is high interobserver variability about PFE grading, it is no longer accepted as reliable [5, 6, 12]. Ependymomas have also been investigated for molecular alterations. According to their site of origin, such as supratentorial, posterior fossa, or spinal cord, they show distinct molecular alterations [6, 13]. Based on these molecular alterations, two distinct groups of PFEs were reported: posterior fossa ependymoma group A (PFA) and posterior fossa ependymoma group B (PFB). The detected molecular differences characterizing these two distinct groups correlated with different patient outcomes, such that PFA patients had a worse prognosis than PFB patients [11, 14]. However, this data was collected from different centers with heterogenous treatment approaches. Our study is unique in terms of having a more homogeneous patient cohort, since all patients were operated on by the same neurosurgeon with the same neuroanesthesiology team through the same surgical approach. All patients were also treated by the same pediatric oncology and radiation oncology teams.
Within the scope of this data, our study aimed to test factors that had the potential to influence the prognosis in our PFE patient cohort. We analyzed the effects on prognosis of variables such as age, sex, extent of surgical resection, radiological localization, molecular subgroups, adjuvant RT, histological grade, Ki67 index, and mutation of ATRX. We also checked tumor specimens for H3K27M mutations. This is the first study in the literature that investigates the presence of ATRX mutation and its prognostic effects in PFEs.
Methods
Patient cohort
A total of 42 patients with PFE operated on in our institution between 1996 and 2018 were enrolled in the study. After obtaining informed consent from patients’ legal guardians, formalin-fixed paraffin-embedded (FFPE) tumor samples were collected.
Inclusion criteria were being operated on for posterior fossa tumor with a histological diagnosis of ependymoma and being under the age of 18 at the time of histological diagnosis. All patients were operated on by the senior author (M.M.Ö) through midline suboccipital craniotomies. All patients had preoperative and postoperative (at 36 h) cranial magnetic resonance imaging (MRI) with contrast. They also had postoperative whole spine MRI with contrast within 14 days of surgery as surveillance for possible spinal seeding. Radiologically median and paramedian tumor localization was determined according to the criteria postulated by U-King-Im et al. [15]. Total resection was defined as less than 5-mm residual tumor on postoperative MRI according to the Children’s Oncology Group guidelines [9]. Some patients did have residual tumors measuring less than 5 mm, some did have residual tumors measuring more than 5 mm, and some did have no measurable tumors at all in the postoperative scans. Residual tumor volumes in cubic centimeters were calculated by multiplying the width, length, and height divided by two (Width × Length × Height/2) [16, 17]. All patients were followed up with cranial MRI with contrast every 3 months and whole spine MRI every 6 months in the first 2 years after surgery. In the third, fourth, and fifth years, patients were followed up with cranial and whole spinal MRI with contrast every 6 months. Thereafter, they were followed up with cranial and spinal MRI with contrast on a yearly basis.
Clinical data, including from radiology, concerning extent of surgical resection and survival was collected by personnel blinded to molecular subgroup of the tumors. All adjuvant chemotherapy and radiation treatment (RT) were planned and introduced by the same pediatric neuro-oncology team. All patients received chemotherapy. Although we followed standard European chemotherapy protocols for each patient, since each protocol had evolved over years, we cannot describe a standard chemotherapy treatment for the entire cohort. For this reason, we excluded the chemotherapy variable while performing statistical analysis. Patients who were diagnosed as PFE between 1996 and 2009 and who were under the age of 3 at diagnosis did not receive RT to the tumor bed. Patients who were diagnosed with PFE in 2010 and later and who were aged under 2 years did not receive RT to the tumor bed.
Pathology and subgroup analysis
The archived material from the pathology specimens was reviewed by a single neuropathologist in terms of Ki67 index, histological grading, subgroup analysis and ATRX and H3K27M mutations.
Two cores, each 2 mm in diameter, were selected from each patient’s FFPE tumor tissue, and used to construct tissue microarray blocks. Anti-H3K27me3 (1:100, Genetex Pkwy Irvine, CA), anti-H3K27m (1:1000, RevMAb Biosciences USA), and anti-ATRX antibodies (1:650, Genetex Pkwy Irvine, CA) were performed on slides cut from these microarray blocks, based on each manufacturer’s instructions, using the Discovery XT processor (Ventana Medical Systems).
The cases with global reduction of H3K27me3 were characterized as PFA, and those with H3K27me3 nuclear immunopositivity as PFB. Diffuse ATRX nuclear immunopositivity was accepted as “intact” and the opposite was accepted as loss of immunoreactivity, suggestive of ATRX mutation. H3K27M was accepted as positive, suggestive of H3K27M mutation, when the tumor cells showed nuclear immunoreactivity. The result of the H3K27M-positive case was confirmed via Sanger sequencing.
Statistical analysis
Estimates of PFS and overall survival (OS) probabilities were analyzed by the Kaplan-Meier method. The log rank test was used to analyze the OS and PFS differences between patient subgroups. Survival data is reported as survival estimates along with 95% confidence intervals. The Fisher exact test was used to analyze associations between risk groups. Advanced multivariate analysis was not performed because of the small sample size of the cohort. All p values quoted are two-sided. Statistical analysis was performed using SPSS Statistics 20.0 software.
Results
Patient cohort
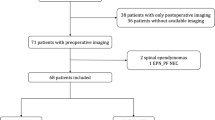
Forty-two pediatric patients, of whom 20 (47.6%) were female and 22 (52.4%) were male, were included in the study. The mean age of patients was 4.4 years (range 0.71–14.51). Thirty-one patients (73.8%) had PFAs, whereas 11 (26.2%) patients had PFBs (Fig. 1). There were 16 (51.6%) females and 15 (48.4%) males in the PFA group, and 4 (36.4%) females and 7 (63.6%) males in the PFB group. We did not find any significant difference in sex between the PFA and PFB groups (p > 0.05). The mean age of patients in the PFA group was 4.04 years (range 0.71–12.98), and 5.44 years (range 1.02–14.51) in the PFB group. Tumors were in paramedian locations in 27 (87.1%) PFA patients and 4 (36.4%) PFB patients. Thus the PFA ependymomas were more frequently paramedian (p = 0.03) (Fig. 2). There was no statistical difference between the ages of patients in the groups (p > 0.05). Although the gross total resection rate of PFA tumors was 61.3% (n = 19) and that of PFB tumors was 81.8% (n = 9), this difference did not reach statistical significance (p > 0.05). There were 19 (45.2%) WHO grade 2 and 23 (54.8%) WHO grade 3 tumors. Among the PFAs, 11 (35.5%) tumors were WHO grade 2, whereas 20 (64.5%) were WHO grade 3. Among the PFBs, 8 (72.7%) tumors were WHO grade 2, whereas 3 (27.3%) were WHO grade 3. The number of WHO grade 3 ependymomas was significantly higher in the PFA group (p < 0.05).

a, b: PFA tumor. a Tumor shows pseudorosette formation which is histologically typical for ependymomas (× 200, H&E). b H3K27me3 nuclear staining is lost in the tumor cells (× 100, anti-H3K27me3). c, d: PFB tumor. c ATRX nuclear staining is lost in the tumor cells in this example. Note the intact staining of endothelial cells (× 200, anti-ATRX). d H3K27me3 nuclear staining was intact in the tumor cells (× 200, anti-H3K27me3). e, f: H3K27M mutant PFA. e ATRX nuclear staining is intact (× 200, anti-ATRX). f Neoplastic cells show nuclear positivity with H3K27M mutation–specific antibody (× 200, anti-H3K27M).

a Axial section cranial MRI of a patient with PFA with paramedian localization (arrows). Arrowhead designates laterally displaced brainstem. b Postoperative MRI with contrast of the same patient, which confirms total surgical excision of tumor. Arrows point to the resection cavity, whereas arrowhead designates brainstem. c Axial section cranial MRI of another patient with PFA with paramedian localization (arrows). Arrowhead designates laterally displaced brainstem. d Postoperative MRI with contrast of the same patient, which shows residual tumor tissue (arrow) in front of brainstem (arrowhead). e Axial section cranial MRI of a patient with PFB with median localization (arrows). f Postoperative MRI with contrast of the same patient, which confirms total surgical excision of tumor. Arrows designate tumor-free resection cavity
The mean residual tumor size was 0.33 cm3 (range 0–6.25 cm3). Eight patients (72.7%) in the PFB group received RT, compared with 20 (64.5%) in the PFA group. All patients in the study cohort received chemotherapy. Tumors recurred in 14 (45.2%) patients in the PFA group and in 3 (27.3%) in the PFB group. The differences in disease recurrence rates between the two groups were not significant (p > 0.05). Ten PFAs recurred within posterior fossa, two PFAs recurred with spinal seedings, one PFA recurred with multiple supratentorial tumors, and one PFA recurred with extensive supratentorial and spinal seedings. All recurrent PFBs recurred within posterior fossa.
Ten patients (32.3%) in the PFA group and 3 (27.3%) in the PFB group had more than one operation during the follow-up period for recurrent tumors within posterior fossa. Eleven patients (35.5%) from the PFA group and 2 (18.4%) from the PFB group died during follow-up. The differences in recurrence and death rates between both groups did not reach significance (p > 0.05).
Nine tumors (21.4% of the entire cohort) showed loss of ATRX immunoreactivity, 8 (88.8%) of which were within the PFA group and 1 (11.2%) in the PFB group. This difference was not statistically different (p > 0.05). One patient’s tumor in the PFA group had immunopositivity for the H3K27M mutation (Fig. 1f). This tumor had intact ATRX (Fig. 1e) and had lost H3K27me3 immunoreactivity. Sanger sequencing verified that there was an H3K27M mutation (Fig. 3). The child was 1.5 years of age at the time of diagnosis, had undergone gross total excision followed by adjuvant chemotherapy, and he has been tumor-free during 86 months of follow-up. Demographic data on the entire patient cohort is summarized in Table 1.

The upper graphic shows h3k27m mutation with the green peak (a), which is not normally present in the h3k27m wild-type control tissue, as shown in the graphic below (b)
Survival analysis
The cohort’s median follow-up time was 5.4 (95% CI, 5.1–8.8) years. The 5-year PFS and OS rates were 55% (95% CI, 40%–75%) and 73% (95% CI, 59.6%–88.9%) respectively. The 5-year PFS rates were 45% (95% CI, 32%–71%) for the PFA group and 89% (95% CI, 73%–99%) for the PFB group. The 5-year OS rates were 65% (95% CI, 49%–85%) for the PFA group and 100% for the PFB group. PFS and OS estimates for the PFB group had a tendency to be better in comparison with the PFA group, but these findings are not significant (p > 0.05) (Fig. 4).

Survival of posterior fossa ependymoma patients according to methylation subgroups: a Progression-free survival (PFS). b Overall survival (OS)
PFS and OS estimates for PFEs with gross total resection are significantly longer than for PFEs with subtotal resection (p < 0.05) (Fig. 5). The overall survival (OS) estimate for PFEs with Ki67 index > 50% was shorter than for PFEs with Ki67 > 50% (p < 0.05) (Fig. 6).

Survival of posterior fossa ependymoma patients according to the extent of excision: a PFS. b OS

OS of posterior fossa ependymoma patients according to Ki67 index
Although PFS and OS estimates for PFEs with ATRX loss seemed to be better in comparison with their ATRX intact counterparts, this also was not significant (p > 0.05).
There was no significant relationship between RT and PFS and OS rates for PFEs in our cohort (p > 0.05).
Discussion
The standard treatment for pediatric PFE is gross total resection followed by RT with or without chemotherapy [6, 7, 18]. Patient age, paramedian tumor location, extent of resection, histological grade, Ki67 index, RT, and chemotherapy have been defined as prognostic indicators in pediatric PFEs in different clinical and pathological studies [12, 19,20,21].
Recent studies have focused on molecular and epigenetic alterations such as H3K27me3 and DNA methylation levels, decreased activity in polycomb repressive complex 2 (PRC2), chromosome 1 q gain, CXorf67 alterations, and 6q deletion as being potential prognostic indicators [6, 11, 22,23,24,25,26].
Among the widely accepted data from all these molecular studies is the identification of PFA and PFB subgroups via methylation profiling of the tumor genome [14]. Those epigenetic alterations correlate with immunohistochemical expression differences in H3K27me3 levels and DNA methylation status. Bayliss et al. reported that PFEs with lower H3K27me3 levels (PF−) have close similarities with molecularly defined PFA groups, whereas PFEs with normal levels of H3K27me3 (PF+) share close similarities with molecularly defined PFB groups [26]. According to those studies, PFA ependymomas show CpG island hypermethylation followed by silencing of PRC2. As a result, PFAs show decreased expression of differentiation genes. They tend to occur in the younger age group (< 3 years) and, at paramedian location, behave more aggressively, have lower total resection rates, and eventually reveal lower PFS and OS rates. On the other hand, PFB ependymomas do not show CpG island hypermethylation, are seen more commonly in young adults, are generally found in the midline location, and have a better prognosis [9, 27].
Some of the main aims of all the scientific work on PFE are to increase PFS and OS rates and to identify risk groups to decrease the toxic effects of RT and chemotherapy protocols by de-escalating doses of adjuvant treatment in low-risk patient groups.
In our study, we analyzed the prognostic values of age, extent of surgical resection, molecular subgroups, adjuvant RT, histological grade, ATRX immunoreactivity, and Ki67 index. ATRX mutations are seen in CNS tumors such as some IDH-mutant diffuse astrocytomas, some H3K27M-mutant gliomas, and some pilocytic astrocytomas with anaplasia [28, 29]. Most ATRX mutations are inactivating and show loss of ATRX immunoreactivity. ATRX loss was generally thought to be associated with a better prognosis until its presence was shown in pilocytic astrocytomas with anaplasia [28,29,30]. To date, our study is the first to present ATRX immunostain results in PFEs. There were 8 patients with tumors with loss of ATRX immunopositivity in the PFA group and 1 in the PFB group. The difference between PFAs and PFBs in terms of ATRX loss was not significant. Although patients with ATRX loss tend to live longer, this finding did not reach significance either. The failure of the differences in results relating to loss of ATRX to reach statistical significance can be attributed to the small number of patients in the cohort studied. H3K27M mutation was accepted specifically for the diagnosis of “diffuse midline glioma, H3K27M-mutant Grade IV” tumor by WHO 2016 [2]. However, a few recent studies or case reports have shown that such mutations are also detected, albeit infrequently, in localized tumors of midline structures such as pilocytic astrocytomas, gangliogliomas, and ependymomas [31]. There are three published cases of H3K27M-mutant PFAs in the literature, with no information about their long-term follow-up [32, 33]. The PFA case with H3K27M mutation in our patient cohort is the fourth reported case and has the longest follow-up period in the literature. Gross total resection was performed on this patient and he is still alive with no adverse event during the 86 months of the follow-up period, even though he has not received adjuvant RT.
Even if clinical studies and meta-analyses about PFEs have postulated other additional prognostic indicators, nearly all have agreed with the fact that gross total resection and adjuvant RT are the major determinants of prognosis [34,35,36]. In our patient cohort, the major prognostic indicator was total surgical resection. On the other hand, changing RT guidelines for PFEs over the years may explain why RT did not become a prognostic indicator in our study. Frequencies of PFE subgroups and their anatomical location in our cohort were almost concordant with the general literature, with a slightly higher frequency of PFBs [8, 37]. Although some studies state that PFA ependymomas have a tendency to occur more frequently in male patients, we did not find any sex predilection between PFE subgroups [14, 38]. There are other studies that support our results in that they did not find any sex predilection between PFE patients related to PFA and PFB subgroups [9]. We did not find significant differences in gross total resection rates between PFA and PFB ependymomas. This data differs from information in the literature, which states that PFA ependymomas have significantly lower gross total resection rates in comparison with PFB ependymomas [14]. This difference likely results from our aggressive surgical strategy, especially for laterally located PFA ependymomas. We did not find any statistical difference between PFA and PFB group ependymomas in terms of recurrent disease, number of deaths, PFS, and OS estimates, although our data show relatively larger differences in these parameters between the PFA and PFB groups. This may be explained by the small number of patients in our cohort or it may be because of the more aggressive surgical strategy followed, especially during operations on PFA ependymomas.
This raised a question in our minds. Is the worse prognosis in PFAs because of their low resection rates or because of their different methylation profiles in comparison with PFBs? If the reason is its low resection rates, can we minimize the difference in prognosis between PFAs and PFBs by following a more aggressive surgical strategy in PFAs?
The extent of resection may be the major confounding factor in multicenter studies since surgical strategies and neurosurgical practices may vary among pediatric neurosurgeons. One neurosurgeon may follow a safe but aggressive surgical strategy to excise nearly all of the PFAs in paramedian locations, and another may leave a considerable volume of the tumor behind with the idea of minimizing the potential damage to lower cranial nerves, facial nerves, and the brainstem [39]. The neurosurgical procedure in both patients may then be classified as total surgical resection according to the total resection cut-off tumor volume in the individual study.
The current study is more homogeneous in terms of surgical and adjuvant radio-chemotherapy practice since all patients were operated on by the same neurosurgeon, and all adjuvant treatments were planned and introduced by the same radiation oncology and pediatric neuro-oncology teams throughout the years.
The 5-year PFS and OS rates for the PFE range from 23–45% to 39–64% respectively in the literature [14, 35, 40, 41]. The 5-year progression-free and OS rates in our cohort are 55% (95% CI, 40%–75%) and 73% (95% CI, 59.6%–88.9%) respectively. From the literature, the 5-year PFS and OS rates for PFA range from 4349% to 50–67% respectively and the 5-year OS rates for PFB ependymomas are around 100% [6, 9, 22]. In our cohort for PFAs, these were 45 and 65% respectively and for PFBs they were 89% and 100% respectively. It would not be an objective evaluation if we were to compare PFS and OS rates in our cohort with those of other patient cohorts in the literature because total resection rates and adjuvant treatment strategies are different for each study.
Conclusion
Although many different variables are suggested as prognostic indicators in pediatric PFE patients, surgery is still the strongest, as proven by the current and other studies. Molecular subgrouping of PFE has important effects on prognosis but still needs to be validated by prospective studies with a larger cohort to be taken into account during the planning of tailored and de-escalating therapies. Survival differences between PFAs and PFBs may be minimized by increasing the total surgical excision rates, especially in laterally located PFAs. Despite all treatment efforts, PFS and OS rates of PFEs are still low. For this reason, more research into the molecular basis of the disease for future targeted therapies is needed.
References
Ostrom QT, Cioffi G, Gittleman H, Patil N, Waite K, Kruchko C, Barnholtz-Sloan JS (2019) CBTRUS statistical report: primary brain and other central nervous system tumors diagnosed in the United States in 2012-2016. Neuro-Oncology 21:v1–v100
Komori T, Sasaki H, Yoshida K (2016) Revised WHO classification of tumours of the central nervous system:summary of the revision and perspective. No Shinkei Geka 44:625–635
Poppleton H, Gilbertson RJ (2007) Stem cells of ependymoma. Br J Cancer 96:6–10
Dyer S, Prebble E, Davison V, Davies P, Ramani P, Ellison D, Grundy R (2002) Genomic imbalances in pediatric intracranial ependymomas define clinically relevant groups. Am J Pathol 161:2133–2141
Ellison DW, Kocak M, Figarella-Branger D, Felice G, Catherine G, Pietsch T, Frappaz D, Massimino M, Grill J, Boyett JM, Grundy RG (2011) Histopathological grading of pediatric ependymoma: reproducibility and clinical relevance in European trial cohorts. J Negat Results Biomed 10:7
Pajtler KW, Witt H, Sill M, Jones DT, Hovestadt V, Kratochwil F, Wani K, Tatevossian R, Punchihewa C, Johann P, Reimand J, Warnatz HJ, Ryzhova M, Mack S, Ramaswamy V, Capper D, Schweizer L, Sieber L, Wittmann A, Huang Z, van Sluis P, Volckmann R, Koster J, Versteeg R, Fults D, Toledano H, Avigad S, Hoffman LM, Donson AM, Foreman N, Hewer E, Zitterbart K, Gilbert M, Armstrong TS, Gupta N, Allen JC, Karajannis MA, Zagzag D, Hasselblatt M, Kulozik AE, Witt O, Collins VP, von Hoff K, Rutkowski S, Pietsch T, Bader G, Yaspo ML, von Deimling A, Lichter P, Taylor MD, Gilbertson R, Ellison DW, Aldape K, Korshunov A, Kool M, Pfister SM (2015) Molecular classification of ependymal tumors across all CNS compartments, Histopathological grades, and age groups. Cancer Cell 27:728–743
Ramaswamy V, Taylor MD (2016) Treatment implications of posterior fossa ependymoma subgroups. Chin J Cancer 35:93
Ramaswamy V, Hielscher T, Mack SC, Lassaletta A, Lin T, Pajtler KW, Jones DT, Luu B, Cavalli FM, Aldape K, Remke M, Mynarek M, Rutkowski S, Gururangan S, McLendon RE, Lipp ES, Dunham C, Hukin J, Eisenstat DD, Fulton D, van Landeghem FK, Santi M, van Veelen ML, Van Meir EG, Osuka S, Fan X, Muraszko KM, Tirapelli DP, Oba-Shinjo SM, Marie SK, Carlotti CG, Lee JY, Rao AA, Giannini C, Faria CC, Nunes S, Mora J, Hamilton RL, Hauser P, Jabado N, Petrecca K, Jung S, Massimi L, Zollo M, Cinalli G, Bognar L, Klekner A, Hortobagyi T, Leary S, Ermoian RP, Olson JM, Leonard JR, Gardner C, Grajkowska WA, Chambless LB, Cain J, Eberhart CG, Ahsan S, Massimino M, Giangaspero F, Buttarelli FR, Packer RJ, Emery L, Yong WH, Soto H, Liau LM, Everson R, Grossbach A, Shalaby T, Grotzer M, Karajannis MA, Zagzag D, Wheeler H, von Hoff K, Alonso MM, Tunon T, Schuller U, Zitterbart K, Sterba J, Chan JA, Guzman M, Elbabaa SK, Colman H, Dhall G, Fisher PG, Fouladi M, Gajjar A, Goldman S, Hwang E, Kool M, Ladha H, Vera-Bolanos E, Wani K, Lieberman F, Mikkelsen T, Omuro AM, Pollack IF, Prados M, Robins HI, Soffietti R, Wu J, Metellus P, Tabori U, Bartels U, Bouffet E, Hawkins CE, Rutka JT, Dirks P, Pfister SM, Merchant TE, Gilbert MR, Armstrong TS, Korshunov A, Ellison DW, Taylor MD (2016) Therapeutic impact of cytoreductive surgery and irradiation of posterior fossa ependymoma in the molecular era: a retrospective multicohort analysis. J Clin Oncol 34:2468–2477
Zapotocky M, Beera K, Adamski J, Laperierre N, Guger S, Janzen L, Lassaletta A, Figueiredo Nobre L, Bartels U, Tabori U, Hawkins C, Urbach S, Tsang DS, Dirks PB, Taylor MD, Bouffet E, Mabbott DJ, Ramaswamy V (2019) Survival and functional outcomes of molecularly defined childhood posterior fossa ependymoma: cure at a cost. Cancer
Healey EA, Barnes PD, Kupsky WJ, Scott RM, Sallan SE, Black PM, Tarbell NJ (1991) The prognostic significance of postoperative residual tumor in ependymoma. Neurosurgery 28: 666–671; discussion 671-662
Wani K, Armstrong TS, Vera-Bolanos E, Raghunathan A, Ellison D, Gilbertson R, Vaillant B, Goldman S, Packer RJ, Fouladi M, Pollack I, Mikkelsen T, Prados M, Omuro A, Soffietti R, Ledoux A, Wilson C, Long L, Gilbert MR, Aldape K, Collaborative Ependymoma Research N (2012) A prognostic gene expression signature in infratentorial ependymoma. Acta Neuropathol 123:727–738
Tihan T, Zhou T, Holmes E, Burger PC, Ozuysal S, Rushing EJ (2008) The prognostic value of histological grading of posterior fossa ependymomas in children: a Children’s Oncology Group study and a review of prognostic factors. Mod Pathol 21:165–177
Mack SC, Taylor MD (2017) Put away your microscopes: the ependymoma molecular era has begun. Curr Opin Oncol 29:443–447
Witt H, Mack SC, Ryzhova M, Bender S, Sill M, Isserlin R, Benner A, Hielscher T, Milde T, Remke M, Jones DT, Northcott PA, Garzia L, Bertrand KC, Wittmann A, Yao Y, Roberts SS, Massimi L, Van Meter T, Weiss WA, Gupta N, Grajkowska W, Lach B, Cho YJ, von Deimling A, Kulozik AE, Witt O, Bader GD, Hawkins CE, Tabori U, Guha A, Rutka JT, Lichter P, Korshunov A, Taylor MD, Pfister SM (2011) Delineation of two clinically and molecularly distinct subgroups of posterior fossa ependymoma. Cancer Cell 20:143–157
UK-I JM, Taylor MD, Raybaud C (2010) Posterior fossa ependymomas: new radiological classification with surgical correlation. Childs Nerv Syst 26:1765–1772
Kersemans V, Cornelissen B, Allen PD, Beech JS, Smart SC (2013) Subcutaneous tumor volume measurement in the awake, manually restrained mouse using MRI. J Magn Reson Imaging 37:1499–1504
Lundin P, Pedersen F (1992) Volume of pituitary macroadenomas: assessment by MRI. J Comput Assist Tomogr 16:519–528
Tsang DS, Burghen E, Klimo P Jr, Boop FA, Ellison DW, Merchant TE (2018) Outcomes after Reirradiation for recurrent pediatric intracranial ependymoma. Int J Radiat Oncol Biol Phys 100:507–515
Bennetto L, Foreman N, Harding B, Hayward R, Ironside J, Love S, Ellison D (1998) Ki-67 immunolabelling index is a prognostic indicator in childhood posterior fossa ependymomas. Neuropathol Appl Neurobiol 24:434–440
Rogers L, Pueschel J, Spetzler R, Shapiro W, Coons S, Thomas T, Speiser B (2005) Is gross-total resection sufficient treatment for posterior fossa ependymomas? J Neurosurg 102:629–636
Stuben G, Stuschke M, Kroll M, Havers W, Sack H (1997) Postoperative radiotherapy of spinal and intracranial ependymomas: analysis of prognostic factors. Radiother Oncol 45:3–10
Pajtler KW, Wen J, Sill M, Lin T, Orisme W, Tang B, Hubner JM, Ramaswamy V, Jia S, Dalton JD, Haupfear K, Rogers HA, Punchihewa C, Lee R, Easton J, Wu G, Ritzmann TA, Chapman R, Chavez L, Boop FA, Klimo P, Sabin ND, Ogg R, Mack SC, Freibaum BD, Kim HJ, Witt H, Jones DTW, Vo B, Gajjar A, Pounds S, Onar-Thomas A, Roussel MF, Zhang J, Taylor JP, Merchant TE, Grundy R, Tatevossian RG, Taylor MD, Pfister SM, Korshunov A, Kool M, Ellison DW (2018) Molecular heterogeneity and CXorf67 alterations in posterior fossa group A (PFA) ependymomas. Acta Neuropathol 136:211–226
Haresh KP, Gandhi AK, Mallick S, Benson R, Gupta S, Sharma DN, Julka PK, Rath GK (2017) Prognostic factors and survival outcomes of intracranial ependymoma treated with multimodality approach. Indian J Med Paediatr Oncol 38:420–426
Araki A, Chocholous M, Gojo J, Dorfer C, Czech T, Heinzl H, Dieckmann K, Ambros IM, Ambros PF, Slavc I, Haberler C (2016) Chromosome 1q gain and tenascin-C expression are candidate markers to define different risk groups in pediatric posterior fossa ependymoma. Acta Neuropathol Commun 4:88
Godfraind C, Kaczmarska JM, Kocak M, Dalton J, Wright KD, Sanford RA, Boop FA, Gajjar A, Merchant TE, Ellison DW (2012) Distinct disease-risk groups in pediatric supratentorial and posterior fossa ependymomas. Acta Neuropathol 124:247–257
Bayliss J, Mukherjee P, Lu C, Jain SU, Chung C, Martinez D, Sabari B, Margol AS, Panwalkar P, Parolia A, Pekmezci M, McEachin RC, Cieslik M, Tamrazi B, Garcia BA, La Rocca G, Santi M, Lewis PW, Hawkins C, Melnick A, David Allis C, Thompson CB, Chinnaiyan AM, Judkins AR, Venneti S (2016) Lowered H3K27me3 and DNA hypomethylation define poorly prognostic pediatric posterior fossa ependymomas. Sci Transl Med 8:366ra161
Zhang RR, Kuo JS (2017) Reduced H3K27me3 is a new epigenetic biomarker for pediatric posterior fossa ependymomas. Neurosurgery 81:N7–N8
Reinhardt A, Stichel D, Schrimpf D, Sahm F, Korshunov A, Reuss DE, Koelsche C, Huang K, Wefers AK, Hovestadt V, Sill M, Gramatzki D, Felsberg J, Reifenberger G, Koch A, Thomale UW, Becker A, Hans VH, Prinz M, Staszewski O, Acker T, Dohmen H, Hartmann C, Mueller W, Tuffaha MSA, Paulus W, Hess K, Brokinkel B, Schittenhelm J, Monoranu CM, Kessler AF, Loehr M, Buslei R, Deckert M, Mawrin C, Kohlhof P, Hewer E, Olar A, Rodriguez FJ, Giannini C, NageswaraRao AA, Tabori U, Nunes NM, Weller M, Pohl U, Jaunmuktane Z, Brandner S, Unterberg A, Hanggi D, Platten M, Pfister SM, Wick W, Herold-Mende C, Jones DTW, von Deimling A, Capper D (2018) Anaplastic astrocytoma with piloid features, a novel molecular class of IDH wildtype glioma with recurrent MAPK pathway, CDKN2A/B and ATRX alterations. Acta Neuropathol 136:273–291
Ebrahimi A, Skardelly M, Bonzheim I, Ott I, Muhleisen H, Eckert F, Tabatabai G, Schittenhelm J (2016) ATRX immunostaining predicts IDH and H3F3A status in gliomas. Acta Neuropathol Commun 4:60
Wiestler B, Capper D, Holland-Letz T, Korshunov A, von Deimling A, Pfister SM, Platten M, Weller M, Wick W (2013) ATRX loss refines the classification of anaplastic gliomas and identifies a subgroup of IDH mutant astrocytic tumors with better prognosis. Acta Neuropathol 126:443–451
Orillac C, Thomas C, Dastagirzada Y, Hidalgo ET, Golfinos JG, Zagzag D, Wisoff JH, Karajannis MA, Snuderl M (2016) Pilocytic astrocytoma and glioneuronal tumor with histone H3 K27M mutation. Acta Neuropathol Commun 4:84
Gessi M, Capper D, Sahm F, Huang K, von Deimling A, Tippelt S, Fleischhack G, Scherbaum D, Alfer J, Juhnke BO, von Hoff K, Rutkowski S, Warmuth-Metz M, Chavez L, Pfister SM, Pietsch T, Jones DT, Sturm D (2016) Evidence of H3 K27M mutations in posterior fossa ependymomas. Acta Neuropathol 132:635–637
Ryall S, Guzman M, Elbabaa SK, Luu B, Mack SC, Zapotocky M, Taylor MD, Hawkins C, Ramaswamy V (2017) H3 K27M mutations are extremely rare in posterior fossa group a ependymoma. Childs Nerv Syst 33:1047–1051
Perilongo G, Massimino M, Sotti G, Belfontali T, Masiero L, Rigobello L, Garre L, Carli M, Lombardi F, Solero C, Sainati L, Canale V, del Prever AB, Giangaspero F, Andreussi L, Mazza C, Madon E (1997) Analyses of prognostic factors in a retrospective review of 92 children with ependymoma: Italian pediatric Neuro-oncology group. Med Pediatr Oncol 29:79–85
Zacharoulis S, Ashley S, Moreno L, Gentet JC, Massimino M, Frappaz D (2010) Treatment and outcome of children with relapsed ependymoma: a multi-institutional retrospective analysis. Childs Nerv Syst 26:905–911
Hanzlik E, Woodrome SE, Abdel-Baki M, Geller TJ, Elbabaa SK (2015) A systematic review of neuropsychological outcomes following posterior fossa tumor surgery in children. Childs Nerv Syst 31:1869–1875
Khatua S, Ramaswamy V, Bouffet E (2017) Current therapy and the evolving molecular landscape of paediatric ependymoma. Eur J Cancer 70:34–41
Thompson YY, Ramaswamy V, Diamandis P, Daniels C, Taylor MD (2015) Posterior fossa ependymoma: current insights. Childs Nerv Syst 31:1699–1706
Sanford RA, Merchant TE, Zwienenberg-Lee M, Kun LE, Boop FA (2009) Advances in surgical techniques for resection of childhood cerebellopontine angle ependymomas are key to survival. Childs Nerv Syst 25:1229–1240
Kilday JP, Rahman R, Dyer S, Ridley L, Lowe J, Coyle B, Grundy R (2009) Pediatric ependymoma: biological perspectives. Mol Cancer Res 7:765–786
Zacharoulis S, Levy A, Chi SN, Gardner S, Rosenblum M, Miller DC, Dunkel I, Diez B, Sposto R, Ji L, Asgharzadeh S, Hukin J, Belasco J, Dubowy R, Kellie S, Termuhlen A, Finlay J (2007) Outcome for young children newly diagnosed with ependymoma, treated with intensive induction chemotherapy followed by myeloablative chemotherapy and autologous stem cell rescue. Pediatr Blood Cancer 49:34–40
Acknowledgments
We would like to thank Dr. Alp Inanıcı for his valuable cooperation during statistical data analysis of this study.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
This retrospective study was approved by ethical committee of Acibadem University School of Medicine, Istanbul, Turkey. Informed consent was obtained from patients’ legal guardians.
Conflict of interest
The authors declare that they have no conflict of interest.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Tanrıkulu, B., Danyeli, A.E. & Özek, M.M. Is H3K27me3 status really a strong prognostic indicator for pediatric posterior fossa ependymomas? A single surgeon, single center experience. Childs Nerv Syst 36, 941–949 (2020). https://doi.org/10.1007/s00381-020-04518-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-020-04518-5