
Abstract
Introduction
Intracranial pressure (ICP) monitoring and cerebral perfusion pressure (CPP) management are the current standards to guide care of severe traumatic brain injury (TBI). However, brain hypoxia and secondary brain injury can occur despite optimal ICP and CPP. In this study, we used brain tissue oxygen tension (PbtO2) monitoring to examine the association between multiple patient factors, including PbtO2, and outcome in pediatric severe TBI.
Materials and methods
In this prospective observational study, 52 children (less than 15 years) with severe TBI were managed with continuous PbtO2 and ICP monitoring. The relationships between outcome [Glasgow Outcome Score (GOS) and Pediatric Cerebral Performance Category Scale] and clinical, radiologic, treatment, and physiological variables, including PbtO2, were examined using multiple logistic regression analysis.
Results
Outcome was favorable in 40 patients (77%) and unfavorable (mortality, 9.6%; n = 5) in 12 (23%). In univariate analysis, the following variables had a significant association with unfavorable outcome: initial GCS, computed tomography classification, ICPpeak, mICP24, mICP, CPPlow, CPP<40, pupil reactivity, \({\text{PbtO}}_{2_{{\text{low}}} } \), PbtO2 < 5 mmHg, PbtO2 < 10 mmHg, \({\text{mPbtO}}_{{\text{2}}_{{\text{24}}} } \), and time–severity product. PbtO2 parameters had the strongest independent association with poor outcome in multiple regression analysis. In particular, when PbtO2 was <5 mmHg for >1 h, the adjusted OR for poor outcome was 27.4 (95% confidence interval, 1.9–391). No variables apart from PbtO2 were independently associated with mortality when controlled for PbtO2.
Conclusion
Reduced PbtO2 is shown to be an independent factor associated with poor outcome in pediatric severe TBI in the largest study to date. It appears to have a stronger association with outcome than conventionally evaluated measures.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
The goal of neurosurgical and critical care management of children with severe traumatic brain injury (TBI) is to avoid or ameliorate secondary injury to maximize the chance of a favorable outcome. Evidence from postmortem [9] and clinical studies [3, 4, 24] suggests that secondary brain hypoxia–ischemia contributes significantly to poor outcome. However, adherence to physiological targets for intracranial pressure (ICP) control, cerebral perfusion pressure (CPP) management, and respiratory function may not avoid brain hypoxia in all patients [5, 33]. This suggests that direct monitors of brain oxygenation that can be used continuously in the intensive care unit (ICU) may help guide patient care. However, continuous measures of brain oxygen have been infrequently used in pediatric neurocritical care. By contrast, brain tissue oxygen tension (PbtO2) monitors are used increasingly in adult TBI patients to obtain additional information to guide therapy. Furthermore, several studies in adult TBI demonstrate a relationship between low PbtO2 and poor outcome [17, 19, 32, 38, 40, 42, 43]. However, few studies have examined the association between PbtO2 and outcome in pediatric TBI [5, 21, 34], and these studies have included relatively few patients. In this study, we examined the relationship between PbtO2 and outcome in a larger (n = 52) group of children with severe TBI. This allowed us to control for other clinical, physiological, and treatment factors that may influence outcome to examine whether PbtO2 is an independent factor associated with outcome.
Materials and methods
Ethics approval for the study was obtained from the Institutional Review Boards of the Red Cross Children’s Hospital and the University of Cape Town.
Patient selection
Data from a consecutive series of pediatric patients who underwent PbtO2 and ICP monitoring for severe TBI at Red Cross Children’s Hospital between June 2006 and May 2008 were prospectively collected. All patients were less than 15 years old. Children with TBI were considered for intracranial monitoring if their postresuscitation Glasgow Coma Score (GCS) was ≤8 or deteriorated to this level after admission, unless extubation was planned early for an improving patient or brain death was imminent [GCS 2T/15, fixed and dilated pupils, and ‘black brain’ on computed tomography (CT) head scan]. Patients were resuscitated, underwent endotracheal intubation, and were mechanically ventilated in the pediatric ICU.
Patient management
The details of patient management have been previously described [5]. In general, patient care was based on the current recommendations for the management of severe TBI in children [1]. ICP was measured through a ventriculostomy or intraparenchymal monitor [Codman ICP Express (Codman, Raynham, MA, USA) and Camino (Integra Neurosciences, Plainsboro, NJ, USA)]. ICP was treated according to the guidelines for ICP management in children [2], which recommends a treatment threshold of 20 mmHg and a stepwise approach to treat ICP > 20 mmHg. We aimed to keep CPP > 50 mmHg in children >2 years old and >45 mmHg in children <2 years old. When an ICP monitor was placed, we also monitored and treated PbtO2. PbtO2 catheters (Licox®, Integra Neurosciences) were inserted into normal-appearing right frontal white matter if there were no localized lesions or in the hemisphere with the greater swelling or containing focal lesions. Data from patients were collected for analysis after a 2-h run-in period to avoid potential artifacts from a stabilizing catheter. Compromised (low) PbtO2 was defined as <20 mmHg and was treated using a hierarchical treatment algorithm that started with a search for a possible cause for low PbtO2. In the absence of a specific cause, the following measures were used depending on ICP, mean arterial pressure (MAP), arterial partial pressure of oxygen (PaO2), hemoglobin (Hb), arterial partial pressure of carbon dioxide (PaCO2), transcranial Doppler flow velocities, and status of autoregulation (when known): (1) elevated or borderline ICP was treated more aggressively when present, (2) the patient’s blood pressure (BP) was elevated to test PbtO2 at a higher CPP with volume infusion and/or inotropic support unless loss of autoregulation caused an ICP increase with elevated BP, (3) higher PaCO2 was tolerated to induce cerebral vasodilation if ICP was not elevated, (4) blood was transfused to increase Hb to ≥10 g/dl, and (5) the inspired fraction of oxygen (FiO2) was increased as an emergency temporary measure or if PbtO2 remained low despite optimization of the above parameters.
Data collection
Data collected included age, gender, mechanism of injury, initial clinical assessment (see below), length of time after injury, and injury to other systems. The following markers of potential prehospital clinical insults were recorded: initial hypoxia, initial MAP, initial systolic blood pressure less than 90 mmHg (SBP < 90), and initial Hb. Physiological monitoring data collected in the ICU included arterial blood gas (ABG) parameters, continuous pulse oximetry (SaO2), MAP, ICP, CPP, and PbtO2. Continuous data were recorded as hourly variables from nursing records.
Initial assessment
At admission and following resuscitation, patients were assessed using (1) postresuscitation GCS or the Pediatric Coma Scale [28] for preverbal children, (2) the motor component of the GCS, (3) the Pediatric Trauma Score [35], and (4) the Pediatric Index of Mortality score [31]. The type of TBI was classified according to the Marshall Classification based on the admission head CT scan findings [18], and patients were defined as having polytrauma or isolated TBI. Postresuscitation pupillary reactions were classified as bilaterally reactive (1), unilaterally nonreactive (2), or bilaterally nonreactive (3). The influence of medications was excluded.
Physiological variables
Intracranial monitoring was started as soon as possible after admission to the ICU and, in general, was continued until both ICP and PbtO2 were controlled for >48 h or until the patient died. Terminal data were excluded from analysis (defined as data collected after the diagnosis of brainstem death was made or when PbtO2 was 0 mmHg for >1 h).
PbtO2
The following PbtO2 values were calculated for each patient: lowest PbtO2 recorded during the monitored period (\({\text{PbtO}}_{2_{{\text{low}}} } \)), mean PbtO2 during the first 24 h of monitoring (\({\text{mPbtO}}_{{\text{2}}_{{\text{24}}} } \)), and the number of episodes of PbtO2 < 10 mmHg (PbtO2 < 10) or PbtO2 < 5 mmHg (PbtO2 < 5) experienced. Since brain injury is determined by both the depth and duration of brain hypoxia, we defined a measure of low PbtO2 that reflects both. Therefore, for each episode that PbtO2 was <10 mmHg (PbtO2 = X mmHg) in each patient, we calculated the value 10 − X mmHg. A PbtO2 of 10 mmHg is considered a critical tissue hypoxia threshold [26, 38]; therefore, 10-X represents the depth of hypoxia. Thereafter we averaged all of these (10 − X) values from each patient. This average was then multiplied by the number of episodes that PbtO2 was less than 10 mmHg in that patient. This was termed the time–severity product to reflect the overall brain hypoxia burden.
Intracranial pressure
The following ICP values were recorded for each patient: mean ICP for the duration of monitoring (mICP), mean ICP for the first 24 h of monitoring (mICP24), the number of episodes of ICP > 20 mmHg (ICP>20), the mean of all episodes of ICP>20 (mICP>20), and the highest ICP (ICPpeak) experienced.
Cerebral perfusion pressure
Potential CPP insults were calculated for each patient as initial CPP (CPPinitial), the lowest CPP experienced (CPPlow), and the number of episodes that CPP was <40 mmHg (CPP<40) and <50 mmHg (CPP<50).
Systemic oxygenation
Potential systemic hypoxic episodes were defined as PaO2 < 8 kPa (60 mmHg) obtained on ABG analysis, or SaO2 < 90% on peripheral oximetry or ABG. The lowest PaO2 (\({\text{P}}_{\text{a}} {\text{O}}_{{\text{2}}_{{\text{low}}} } \)) observed also was recorded.
Hemoglobin
Concentration of Hb (g/dl) was recorded as initial Hb (Hbinitial), lowest Hb (Hblow) and mean Hb for the duration of the ICU stay (mHb).
Treatment
The duration of monitoring was recorded in each patient. Treatment factors recorded included red blood cell transfusion (RBCT), hypertonic saline given (HTS; recorded as the number of times given), decompressive hemicraniectomy, the use of thiopentone, and use of inotropes to elevate BP.
Clinical outcome
The place (e.g., ICU or general ward) and time of deaths were recorded. Clinical outcome of survivors was determined from follow-up clinical visits, at least 6 months after injury, which included assessments by neurosurgeons, occupational therapists, speech therapists, pediatric developmental specialists, and school progress reports where appropriate. Outcome was assessed using the Glasgow Outcome Score (GOS) and the Pediatric Cerebral Performance Category Scale (PCPCS). The GOS [13] was dichotomized to unfavorable (1, death; 2, vegetative; and 3, severe disability) and favorable (4, mild disability; 5, minor; or no disability) outcome. The PCPCS [6, 7] was similarly dichotomized to favorable (1, normal; 2, mild disability; and 3, moderate disability) and unfavorable (4, severe disability; 5, coma or vegetative state; and 6, death) outcome.
Statistical analysis
All data were analyzed with R statistical computing (http://wwww.r-project.org) and Stata software (version 7.0, College Station, TX, USA). Relationships between clinical and physiological variables and outcome were examined with the Wilcoxon’s rank sum test for continuous variables and Pearson’s X 2 test for categorical variables. Variables with significant relationships in univariate analysis were entered into a stepwise multivariate logistic regression model. Limited covariates were used in individual models to ensure model stability. Separate models were constructed for individual PbtO2 parameters. Values were examined as continuous and dichotomized variables. Regression models were constructed separately for GOS (dichotomized into favorable and unfavorable outcome) and mortality. Results are reported as odds ratios (OR) and 95% confidence intervals (CI) for death and unfavorable outcome (severe disability and death). Significance was set at p = 0.05. Descriptive statistics are reported as mean ± SD or median and interquartile range (IQR) depending on distribution characteristics.
Results
Clinical characteristics
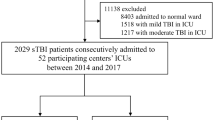
Fifty-two pediatric patients with severe TBI (GCS <8) received monitoring for ICP, CPP, and PbtO2 between June 2006 and May 2008. There were 39 boys (75%) and 13 girls. The age distribution was as follows: <2 years (n = 5, 9.6%), 2–3 years (n = 9, 17.3%), 4–7 years (n = 20, 38.5%), 8–11 years (n = 16, 30.8%), and 12–14 years (n = 2, 3.8%). Other baseline demographic and clinical variables on admission are summarized in Table 1. Mechanisms of injury were as follows: motor vehicle accident related in 40 (76.9%), crush injury in three (5.8%), gunshot wound in four (7.7%), blunt assault in two (3.8%), fall from a height in one (1.9%), stab to the head in one (1.9%), and inflicted injury (shaken baby syndrome) in one (1.9%). Penetrating injury accounted for 9.6% of cases (n = 5).
Early insults
Thirteen patients (25%) had an initial SBP<90 mmHg, and 14 (26.9%) had initial systemic hypoxia (SaO2 < 90% or PaO2 < 8 kPa) before or on admission to the hospital.
Treatment factors
Inotropes were used for BP support in 31 patients (60%). Thirty-four patients (65%) received RBCT. Forty patients (77%) received HTS to treat serum sodium<140 mmol/L or to treat elevated ICP. Ten patients received thiopentone (19.2%) and seven patients (13.5%) received decompressive craniectomy for elevated ICP refractory to conventional treatment.
Physiological factors
Median (IQR) length of time from injury to the start of PbtO2 monitoring was 9 h (7–16 h), and the median (IQR) duration of invasive monitoring was 5 days (3–7 days). Values for mICP, mICP24 and ICPpeak (median, IQR) were 14 mmHg (12–16 mmHg), 14 mmHg (11–18 mmHg), and 31 mmHg (22–44 mmHg), respectively. The median lowest (IQR) CPP was 43 mmHg (33–50 mmHg). Mean PbtO2 (excluding terminal data) was 34 ± 13 mmHg. Episodes of PbtO2 < 10 mmHg and of PbtO2 < 5 mmHg occurred in 27 (52%) and 12 patients (23%), respectively. Lowest PbtO2 and \({\text{mPbtO}}_{{\text{2}}_{{\text{24}}} } \) (median, IQR) were 10 mmHg (6–17 mmHg) and 28 mmHg (22–35 mmHg), respectively.
Outcome
Overall mortality for the whole group was 9.6% (n = 5). Of the patients who died, three died while in ICU (all within 24 h after head injury), and two died after discharge to the ward (both polytrauma patients who had respiratory related deaths). All deaths occurred in hospital and within 30 days of injury (median, 2 days after injury; range, 1–26). Survivors were followed up for at least 6 months (median, 10 months; range, 6–26 months). Dichotomized outcome results were the same when using GOS and PCPCS; therefore, further analysis was performed using the GOS. Outcome was unfavorable in 12 patients, including the five who died (23%) and favorable in 40 (77%). There were no vegetative survivors.
Factors associated with unfavorable outcome (severe disability or death)
The relationships between outcome (as the dependent variable) and clinical, physiological, and treatment factors examined using univariate analysis are summarized in Table 2. Variables that had significant relationships with unfavorable outcome in univariate analysis included initial GCS (p = 0.001), CT classification (p = 0.03), ICPpeak (p = 0.02), mICP24 (p = 0.02), mICP (p = 0.03), CPPlow (p = 0.03), CPP<40 (p = 0.03), pupil reactivity (p = 0.004), \({\text{PbtO}}_{2_{{\text{low}}} } \) (p < 0.0001), \({\text{PbtO}}_{2_{{\text{ $<$ 5}}} } \) (p < 0.0001), \({\text{PbtO}}_{2_{{\text{ $<$ 10}}} } \) (p < 0.0001), \({\text{mPbtO}}_{{\text{2}}_{{\text{24}}} } \) (p = 0.02), and the time–severity product (p < 0.0001).
Episodes of PbtO2 < 10 mmHg occurred in 40% (n = 16) of patients who had a favorable outcome and in 92% (n = 11) of patients who had an unfavorable outcome. PbtO2 < 5 mmHg occurred in 10% (n = 4) and 67% (n = 8) of patients with a favorable or unfavorable outcome, respectively. \({\text{mPbtO}}_{{\text{2}}_{{\text{24}}} } \) was 30.4 ± 8.9 mmHg in patients with favorable outcome and 21.9 ± 16.4 mmHg in patients with unfavorable outcome. PbtO2 decreased to 0 mmHg in all patients who developed brain death while being monitored (n = 3).
Multivariate analysis
Unfavorable outcome (GOS)
Variables that were significant in univariate analysis were then examined in multivariate analysis. Age was forced into the model because of its clinical importance. All PbtO2 parameters had significant relationships with outcome in multivariate analysis when analyzed as continuous or binary (Table 3) variables. In particular, when PbtO2 was <5 mmHg for >1 h, the adjusted OR for unfavorable outcome (severe disability or death) was 27.4. Similarly, when PbtO2 was <10 mmHg for >2 h, outcome often was poor (adjusted OR = 10.8). \({\text{mPbtO}}_{{\text{2}}_{{\text{24}}} } \) had a marginal relationship with outcome when analyzed as a continuous variable (p = 0.048) but not when analyzed as a binary variable (dichotomized at 16 mmHg, p = 0.062). Significant associations with outcome also were found for initial GCS, CT classification, ICPpeak, CPPlow, and PaO2 < 8 kPa when tested in multivariate models with some, but not consistently with all of the PbtO2 parameters. Table 3 summarizes the adjusted ORs for the multivariate results of PbtO2 parameters examined as dichotomized variables with outcome as the dependent variable.
Mortality
Variables that were significant in univariate analysis were entered into multivariate analysis. All PbtO2 parameters were independently associated with mortality. No other variables were independently associated with mortality when tested in models with PbtO2 parameters. Table 4 displays the multivariate results for dichotomized PbtO2 parameters tested with mortality as the dependent variable.
Discussion
In this study of 52 children (<15 years old) with severe TBI, we examined the relationships between outcome and clinical, physiological, and treatment factors, with an emphasis on PbtO2. The main findings were the following: (1) PbtO2 is an independent factor associated with mortality and unfavorable outcome in children with severe TBI, and (2) PbtO2 was reduced to lower values and for a longer duration of time in patients with poor outcome. Factors such as initial GCS, CT classification, peak ICP, and lowest CPP were significant in some but not all of the multivariate models for dichotomized outcome, and none of these were independently associated with mortality. These findings suggest that PbtO2 data may help guide severe pediatric TBI management.
PbtO2 thresholds and outcome
Several lines of experimental and clinical evidence suggest that a PbtO2 of 20 mmHg is a reasonable treatment threshold and that a PbtO2 < 10 mmHg is associated with poor outcome in adult TBI [11, 16, 17, 22, 37, 38, 40, 41]. Consistent with this, results of a preliminary series from our institution suggested that an increased depth and duration of PbtO2 < 20 mmHg was associated with poor outcome [5] and that this relationship was strongest when PbtO2 is <10 mmHg. However, there were too few observations of PbtO2 < 5 mmHg for meaningful analysis. In the present series, a PbtO2 of 20 mmHg was used a treatment threshold, and the current findings confirm and extend our previous observations and show a high likelihood of poor outcome when PbtO2 is <10 mmHg for >2 h or when PbtO2 was <5 mmHg for >1 h. These thresholds are consistent with human and animal studies that suggest that PbtO2 generally is <10 mmHg at critical thresholds of ischemia [12, 26]. Therefore, PbtO2 values between 15 and 20 mmHg may act as an early warning sign for impending oligemia or cell damage. However, in addition to perfusion-limited brain tissue hypoxia, diffusion limitation also may be significant. Tissue oxygen tension decreases nonlinearly in the extracellular space with increasing distance from the vessel [27]. In TBI, this distance may be increased due to diffusion barriers, such as cytotoxic cell swelling, perivascular edema, collapsed capillaries, and arteriovenous shunting in the microvasculature [20]. Therefore, PbtO2 may be a marker of both mechanisms of limited transport of oxygen to the cells.
To answer the question whether brain oxygen is an independent variable associated with outcome, we constructed separate models for individual PbtO2 parameters using stepwise multivariate logistic regression. Two points are important when interpreting the findings of this multivariate analysis. First, the model only examined variables that demonstrated a direct association with outcome; nonsignificant factors that may have been associated with outcome were not included. However, we did force age into the model because of its clinical importance. In addition, the other variables found to be associated with outcome in initial analysis [i.e., initial GCS, CT classification (Marshall grade), increased ICP, reduced CPP and pupil reactivity] are all common covariates associated with outcome in many clinical TBI studies. Second, the estimates of several odds ratios were imprecise with wide confidence intervals. Bearing these caveats in mind, our data show that PbtO2 is an independent factor associated with mortality and unfavorable outcome in children with severe TBI.
PbtO2 treatment and outcome
PbtO2 monitoring affords the clinician an opportunity to continuously monitor changes in brain oxygen in the ICU. The relationship between low PbtO2 and poor outcome and the high incidence of brain hypoxia despite conventional treatment [5, 33] suggests that PbtO2-directed treatment may benefit some TBI patients including pediatric patients. Although there is no class 1 evidence currently available, several lines of evidence support the concept of PbtO2-directed TBI care. An increase in PbtO2 is associated with improved brain metabolism in clinical TBI [36], greater mitochondrial ATP production [44], and attenuated secondary brain damage in experimental TBI models [23]. Augmented oxygen delivery reduces infarct volumes in animal stroke models [8, 30], and high flow oxygen therapy is associated with a transient improvement of clinical deficits and MRI abnormalities in patients with acute cerebral ischemia [29]. Historical case–control studies in adult TBI also suggest that PbtO2-directed treatment may be associated with improved outcome [19, 32].The site of the PbtO2 monitor is an important consideration because the area of brain tissue monitored is small [15, 16]. Therefore, it is our institutional practice to monitor in normal-appearing right frontal white matter if there is no focal injury. In these circumstances, the monitor is thought to reflect global oxygenation [14, 15, 25, 26, 39]. When there is focal pathology, we attempt to place a peri-lesional monitor, since pericontusional tissue has different physiological responses compared with normal white matter and is at higher risk of ischemia [10, 14].
Methodological limitations
There are several potential limitations to this study. First, the sample size is small; however, it is relatively homogeneous because it includes only children with severe TBI who were less than 15 years old. Second, the age range (9 months to 14 years old) represents wide differences in physiological thresholds. Ideally, a larger number of patients in each age category should be examined separately, as there may be age-related differences in threshold tolerance. However, few institutions treat large enough numbers of children with severe TBI for this to be accomplished easily in single-center studies. In this study, we included age in all multivariate models to control for its effect on the relationship between physiological variables and outcome. Third, outcome evaluation in children is difficult, and pediatric neuropsychological testing was not performed in this study. However, the GOS and PCPCS used in this study can be dichotomized easily to enable examination for associations with death and severe disability. These outcome assessments are used commonly in pediatric TBI, which allows for comparison with other studies. Fourth, this was not a pure observational study in that interventions were directed at low PbtO2, low CPP, and high ICP. Untreated values for each of these may have different associations with outcome parameters. Fifth, even though PbtO2 is associated with outcome, we did not examine the effect of interventions for low PbtO2; therefore, we cannot comment on which methods may be effective, what their adverse effects are, and what impact these may have on outcome. Finally, our PbtO2 data does not contain enough detail to allow us to conclude what is the lower limit of PbtO2 and what duration of brain hypoxia can be tolerated. Despite these limitations, we believe that our results show an independent association between low PbtO2 and poor outcome in pediatric TBI and a more consistent relationship with mortality and poor outcome than the traditional methods of monitoring used commonly in the pediatric ICU for patients with severe TBI (ICP and CPP). These findings suggest that future studies to examine the impact of interventions for low PbtO2 in children are warranted.
Conclusion
In this study of 52 children with severe TBI, the largest to date, we found that episodes of low PbtO2 have an independent association with poor outcome and mortality after pediatric severe TBI. In addition, PbtO2 appears to have a stronger relationship with outcome than ICP and CPP. These findings suggest that we may need to augment current monitoring strategies and reconsider treatment strategies recommended for the management of severe TBI in children.
References
Adelson PD, Bratton SL, Carney NA, Chesnut RM, du Coudray HE, Goldstein B, Kochanek PM, Miller HC, Partington MD, Selden NR, Warden CR, Wright DW, American Association for Surgery of Trauma, Child Neurology Society, International Society for Pediatric Neurosurgery, International Trauma Anesthesia and Critical Care Society, Society of Critical Care Medicine, World Federation of Pediatric Intensive and Critical Care Societies (2003) Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chapter 1: Introduction. Pediatr Crit Care Med 4(3 Suppl):S2–S4
Adelson PD, Bratton SL, Carney NA, Chesnut RM, du Coudray HE, Goldstein B, Kochanek PM, Miller HC, Partington MD, Selden NR, Warden CR, Wright DW, American Association for Surgery of Trauma, Child Neurology Society, International Society for Pediatric Neurosurgery, International Trauma Anesthesia and Critical Care Society, Society of Critical Care Medicine, World Federation of Pediatric Intensive and Critical Care Societies (2003) Guidelines for the acute medical management of severe traumatic brain injury in infants, children, and adolescents. Chapter 6. threshold for treatment of intracranial hypertension. Pediatr Crit Care Med 4(3 Suppl):S25–S27
Bouma GJ, Muizelaar JP, Stringer WA, Choi SC, Fatouros P, Young HF (1992) Ultra-early evaluation of regional cerebral blood flow in severely head-injured patients using xenon-enhanced computerized tomography. J Neurosurg 77(3):360–368
Chesnut RM, Marshall LF, Klauber MR, Blunt BA, Baldwin N, Eisenberg HM, Jane JA, Marmarou A, Foulkes MA (1993) The role of secondary brain injury in determining outcome from severe head injury. J Trauma 34(2):216–222
Figaji AA, Fieggen AG, Argent AC, Leroux PD, Peter JC (2008) Does adherence to treatment targets in children with severe traumatic brain injury avoid brain hypoxia? A brain tissue oxygenation study. Neurosurgery 63(1):83–91 (discussion 91–92)
Fiser DH (1992) Assessing the outcome of pediatric intensive care. J Pediatr 121(1):68–74
Fiser DH, Long N, Roberson PK, Hefley G, Zolten K, Brodie-Fowler M (2000) Relationship of pediatric overall performance category and pediatric cerebral performance category scores at pediatric intensive care unit discharge with outcome measures collected at hospital discharge and 1- and 6-month follow-up assessments. Crit Care Med 28(7):2616–20
Flynn EP, Auer RN (2002) Eubaric hyperoxemia and experimental cerebral infarction. Ann Neurol 52(5):566–572
Graham DI, Ford I, Adams JH, Doyle D, Teasdale GM, Lawrence AE, McLellan DR (1989) Ischaemic brain damage is still common in fatal non-missile head injury. J Neurol Neurosurg Psychiatry 52(3):346–350
Gupta AK, Hutchinson PJ, Al-Rawi P, Gupta S, Swart M, Kirkpatrick PJ, Menon DK, Datta AK (1999) Measuring brain tissue oxygenation compared with jugular venous oxygen saturation for monitoring cerebral oxygenation after traumatic brain injury. Anesth Analg 88(3):549–553
Hlatky R, Valadka AB, Goodman JC, Contant CF, Robertson CS (2004) Patterns of energy substrates during ischemia measured in the brain by microdialysis. J Neurotrauma 21(7):894–906
Hlatky R, Valadka AB, Gopinath SP, Robertson CS (2008) Brain tissue oxygen tension response to induced hyperoxia reduced in hypoperfused brain. J Neurosurg 108(1):53–58
Jennett B, Bond M (1975) Assessment of outcome after severe brain damage. Lancet 1(7905):480–484
Johnston AJ, Steiner LA, Chatfield DA, Coles JP, Hutchinson PJ, Al-Rawi PG, Menon DK, Gupta AK (2004) Effect of cerebral perfusion pressure augmentation with dopamine and norepinephrine on global and focal brain oxygenation after traumatic brain injury. Intensive Care Med 30(5):791–797
Kiening KL, Unterberg AW, Bardt TF, Schneider GH, Lanksch WR (1996) Monitoring of cerebral oxygenation in patients with severe head injuries: brain tissue PO2 versus jugular vein oxygen saturation. J Neurosurg 85(5):751–757
Lang EW, Mulvey JM, Mudaliar Y, Dorsch NW (2007) Direct cerebral oxygenation monitoring–a systematic review of recent publications. Neurosurg Rev 30(2):99–106 (discussion 106–107)
Maloney-Wilensky E, Gracias V, Itkin A, Hoffman K, Bloom S, Yang W, Christian S, Le Roux P (2009) Brain tissue oxygen and outcome after severe traumatic brain injury: A systematic review. Crit Care Med (in press)
Marshall LF, Bowers Marshall S, Klauber MR et al (1991) A new classification of head injury based on computerized tomography. J Neurosurg 75:S14–S20
Meixensberger J, Jaeger M, Vath A, Dings J, Kunze E, Roosen K (2003) Brain tissue oxygen guided treatment supplementing ICP/CPP therapy after traumatic brain injury. J Neurol Neurosurg Psychiatry 74(6):760–764
Menon DK, Coles JP, Gupta AK, Fryer TD, Smielewski P, Chatfield DA, Aigbirhio F, Skepper JN, Minhas PS, Hutchinson PJ, Carpenter TA, Clark JC, Pickard JD (2004) Diffusion limited oxygen delivery following head injury. Crit Care Med 32(6):1384–1390
Narotam PK, Burjonrappa SC, Raynor SC, Rao M, Taylon C (2006) Cerebral oxygenation in major pediatric trauma: Its relevance to trauma severity and outcome. J Pediatr Surg 41(3):505–513
Nortje J, Gupta AK (2006) The role of tissue oxygen monitoring in patients with acute brain injury. Br J Anaesth 97(1):95–106
Palzur E, Vlodavsky E, Mulla H, Arieli R, Feinsod M, Soustiel JF (2004) Hyperbaric oxygen therapy for reduction of secondary brain damage in head injury: an animal model of brain contusion. J Neurotrauma 21(1):41–48
Pigula FA, Wald SL, Shackford SR, Vane DW (1993) The effect of hypotension and hypoxia on children with severe head injuries. J Pediatr Surg 28(3):310–314 (discussion 315–316)
Rossi S, Balestreri M, Spagnoli D, Bellinzona G, Valeriani V, Bruzzone P, Maestri M, Stocchetti N (2000) Oxygen delivery and oxygen tension in cerebral tissue during global cerebral ischaemia: a swine model. Acta Neurochir Suppl 76:199–202
Scheufler KM, Lehnert A, Rohrborn HJ, Nadstawek J, Thees C (2004) Individual value of brain tissue oxygen pressure, microvascular oxygen saturation, cytochrome redox level, and energy metabolites in detecting critically reduced cerebral energy state during acute changes in global cerebral perfusion. J Neurosurg Anesthesiol 16(3):210–219
Scheufler KM, Rohrborn HJ, Zentner J (2002) Does tissue oxygen-tension reliably reflect cerebral oxygen delivery and consumption? Anesth Analg 95(4):1042–1048
Simpson D, Reilly P (1982) Pediatric coma scale. Lancet 2(8295):450
Singhal AB, Benner T, Roccatagliata L, Koroshetz WJ, Schaefer PW, Lo EH, Buonanno FS, Gonzalez RG, Sorensen AG (2005) A pilot study of normobaric oxygen therapy in acute ischemic stroke. Stroke 36(4):797–802
Singhal AB, Dijkhuizen RM, Rosen BR, Lo EH (2002) Normobaric hyperoxia reduces MRI diffusion abnormalities and infarct size in experimental stroke. Neurology 58(6):945–952
Slater A, Shann F, Pearson G, Paediatric Index of Mortality (PIM) Study Group (2003) PIM2: A revised version of the paediatric index of mortality. Intensive Care Med 29(2):278–285
Stiefel MF, Spiotta A, Gracias VH, Garuffe AM, Guillamondegui O, Maloney-Wilensky E, Bloom S, Grady MS, LeRoux PD (2005) Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring. J Neurosurg 103(5):805–811
Stiefel MF, Udoetuk JD, Spiotta AM, Gracias VH, Goldberg A, Maloney-Wilensky E, Bloom S, Le Roux PD (2006) Conventional neurocritical care and cerebral oxygenation after traumatic brain injury. J Neurosurg 105(4):568–575
Stiefel MF, Udoetuk JD, Storm PB, Sutton LN, Kim H, Dominguez TE, Helfaer MA, Huh JW (2006) Brain tissue oxygen monitoring in pediatric patients with severe traumatic brain injury. J Neurosurg 105(4 Suppl):281–286
Tepas JJ 3rd, Ramenofsky ML, Mollitt DL, Gans BM, DiScala C (1988) The pediatric trauma score as a predictor of injury severity: an objective assessment. J Trauma 28(4):425–429
Tolias CM, Reinert M, Seiler R, Gilman C, Scharf A, Bullock MR (2004) Normobaric hyperoxia-induced improvement in cerebral metabolism and reduction in intracranial pressure in patients with severe head injury: a prospective historical cohort-matched study. J Neurosurg 101(3):435–444
Valadka AB, Goodman JC, Gopinath SP, Uzura M, Robertson CS (1998) Comparison of brain tissue oxygen tension to microdialysis-based measures of cerebral ischemia in fatally head-injured humans. J Neurotrauma 15(7):509–519
Valadka AB, Gopinath SP, Contant CF, Uzura M, Robertson CS (1998) Relationship of brain tissue PO2 to outcome after severe head injury. Crit Care Med 26(9):1576–1581
van den Brink WA, Haitsma IK, Avezaat CJ, Houtsmuller AB, Kros JM, Maas AI (1998) Brain parenchyma/pO2 catheter interface: a histopathological study in the rat. J Neurotrauma 15(10):813–824
van den Brink WA, van Santbrink H, Steyerberg EW, Avezaat CJ, Suazo JA, Hogesteeger C, Jansen WJ, Kloos LM, Vermeulen J, Maas AI (2000) Brain oxygen tension in severe head injury. Neurosurgery 46(4):868–876 (discussion 876–878)
van Santbrink H, Maas AI, Avezaat CJ (1996) Continuous monitoring of partial pressure of brain tissue oxygen in patients with severe head injury. Neurosurgery 38(1):21–31
van Santbrink H, vd Brink WA, Steyerberg EW, Carmona Suazo JA, Avezaat CJ, Maas AI (2003) Brain tissue oxygen response in severe traumatic brain injury. Acta Neurochir (Wien) 145(6):429–438 (discussion 438)
Zauner A, Doppenberg EM, Woodward JJ, Choi SC, Young HF, Bullock R (1997) Continuous monitoring of cerebral substrate delivery and clearance: Initial experience in 24 patients with severe acute brain injuries. Neurosurgery 41(5):1082–1091 (discussion 1091–1093)
Zhou Z, Daugherty WP, Sun D, Levasseur JE, Altememi N, Hamm RJ, Rockswold GL, Bullock MR (2007) Protection of mitochondrial function and improvement in cognitive recovery in rats treated with hyperbaric oxygen following lateral fluid-percussion injury. J Neurosurg 106(4):687–694
Acknowledgements
Dr Figaji has received a grant from the South African–Swedish Links Programme (SIDA, National Research Foundation). Drs Figaji and Le Roux have also received a grant from the Integra Foundation for the study of cerebral perfusion pressure thresholds in children.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Figaji, A.A., Zwane, E., Thompson, C. et al. Brain tissue oxygen tension monitoring in pediatric severe traumatic brain injury. Childs Nerv Syst 25, 1325–1333 (2009). https://doi.org/10.1007/s00381-009-0822-x
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-009-0822-x