
Abstract
Objective
The objective was to report our positive experience of using dexamethasone to treat 13 patients with symptomatic slit ventricle syndrome (SVS).
Methods
Thirteen SVS patients who received dexamethasone during acute episodes were studied. The etiology for hydrocephalus was prematurity and intraventricular hemorrhage in 9 patients and neonatal meningitis, chorioamnionitis, Dandy–Walker variant, and congenital in 1 case each. The shunt was inserted at 1.8±1.0 months of age and SVS was diagnosed at 4.9±3.2 years of age.
Results
All patients reported relief and shorter duration of symptoms with dexamethasone. Surgical intervention was decided upon and carried out within 11±8 months of SVS diagnosis in 9 out of 13 patients. The other 4 are being monitored and continue to receive dexamethasone when needed.
Conclusions
Dexamethasone appears to be a useful treatment in acutely increased intracranial pressure caused by SVS. It can provide temporary relief during the decision-making process of whether and when to perform surgery.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Slit ventricle syndrome (SVS) is a catchall term for a combined clinical and imaging situation in which symptoms in a shunted child are associated with small ventricular spaces [3, 4, 9, 19].
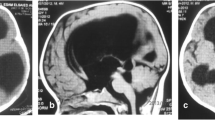
In its severe form, the clinical picture is one of acute or semi-acute headache, nausea, vomiting, and/or lethargy. The headaches are often precipitated by fever, activity or warm weather. They are episodic, typically presenting as pressure waves, often terminating in vomiting or hyperventilation, and are sometimes associated with bradycardia and systemic hypertension [3, 4, 12]. Neurological findings of ataxia, brain stem signs, and epileptic fits were reported as well [3, 17]. A computed tomography (CT) scan at the time of an attack shows small ventricles, but this finding is usually no different from scans that were done during periods of remission. The symptoms of SVS usually appear 2–5 years after a shunt had been placed during the first year of life, mostly in children with a small head circumference, under the 25th percentile [3, 4].
The treatment for SVS is aimed at either optimizing CSF drainage or at increasing calvarial volume. Therapeutic decision-making may not be easy due to the fact that although attacks are usually severe in nature, they subside spontaneously; moreover, the situation may be self-limiting in some children. Any noninvasive method that would be effective in relieving an acute attack and perhaps reducing the frequency of episodes would be helpful [1–3, 17].
We report our recent and positive experience with the use of corticosteroids in the treatment of symptomatic SVS attacks and discuss the indications and possible mechanism of action.
Materials and methods
We reviewed the charts of 13 children over the age of 5 years with ventricular shunts complicated by SVS that are being treated and followed in the Pediatric Neurosurgery Department in Dana Children’s Hospital. They all experienced attacks of headaches with or without vomiting, and slit or small ventricles were demonstrated on CT or magnetic resonance imaging (MRI). There were 9 boys and 4 girls whose mean age was 8.9±3.5 years (range 5–15). The patients’ data were retrieved from their medical charts and by questioning the parents on their child’s response to dexamethasone treatment.
Observations and results
The clinical details of the study participants are summarized in Table 1. The etiology of hydrocephalus was prematurity and intraventricular hemorrhage in 9 patients and neonatal meningitis, chorioamnionitis, Dandy–Walker variant, and congenital in 1 case each. The mean age at ventriculoperitoneal shunt insertion was 1.8±1.0 months, range 0.5–4 months. The average age at SVS diagnosis was 4.9±3.2 years (range 1–13). All patients had repeated ventriculoperitoneal shunt revisions before corticosteroid treatment, and one patient underwent cranial expansion for scaphocephaly (Table 1).
All the patients were treated by oral dexamethasone for at least one episode. The length of treatment ranged between 3 and 10 days: the daily dose was 0.5 mg/kg and the total dose ranged from 4 to 12 mg. Two patients were treated concomitantly by acetazolamide. All patients reported symptomatic relief within 48 h and shorter duration of the attack compared with previous attacks without the administration of dexamethasone. None of the children required an emergency surgical procedure, but the treatment did not prevent further attacks in most of them. Nine patients required surgical treatment for their SVS: bilateral subtemporal decompression in 6, lumboperitoneal shunt in 2, and an additional ventriculoperitoneal shunt in 2 (one patient underwent both bilateral subtemporal decompression and distal ventriculoperitoneal shunt). The mean interval between steroid treatment to surgery or last follow-up was 11±8 months. Two patients had recurrence of clinical symptoms of SVS after subtemporal decompression and dexamethasone was reinstated.
It was determined that four patients did not require a surgical procedure for SVS at the time of this study and they were treated conservatively by dexamethasone. One of them had a symptomatic trapped fourth ventricle, which was treated by steroids as well. One child underwent cranial expansion for scaphocephaly: he was treated by dexamethasone for SVS and did not require further surgery for SVS for the last 24 months of follow-up. Two patients had complications associated with steroid treatment: abdominal pain and skin infection. Both resolved within a short period and did not discourage further use of steroids (Table 1).
Discussion and conclusions
This is the first report in the English literature on the effects of dexamethasone on the symptomatology of acute SVS attacks. The treatment of SVS is often frustrating for the child, the family, and the treating physician. There are several surgical alternatives to treating resistant SVS attacks [3, 4, 17]. “Up-grading” the type of shunt-valve can occasionally prevent collapse of the ventricular system and therefore reduce the potential for proximal shunt obstruction [15]. Revising the obstructed ventricular catheter is dangerous due to a high incidence of bleeding and the technical difficulty of placing the tube through a small fluid space in an optimal trajectory [11]. Lumboperitoneal shunts have been also proposed for children with extraventricular obstruction [14, 16, 20]. Subtemporal decompression and other alternatives designed to increase the volume of the skull are often considered by parents as being “aggressive,” and these approaches are not always effective [5–7, 10, 13]. Antimigraine therapy with cyproheptadine (Periactin) or propanolol is helpful in some children who have subacute or chronic headaches with high intracranial pressure but a functioning shunt [8, 18].
Worrisome symptoms of SVS often happen during the night and mandate quick responses. None of the existing surgical alternatives offers resolution of symptoms in all patients. Some of the proposed procedures, especially proximal shunt revision, can have catastrophic results. An alternative means that is effective in alleviating an SVS attack and perhaps reducing the frequency of symptoms would be highly welcome.
The idea of giving steroids in this situation was initially empirical. Having been proved to be effective, we introduced it into our routine armamentarium of treatment options. We believe that all the patients in the current series had intermittent extraventricular hydrocephalus due a transient proximal shunt obstruction on a noncompliant brain. The fact that the ventricles have not been enlarged to any extent during an acute SVS attack is probably indirect evidence that there is no obstruction within the ventricular system. High pressure waves in these children should not, therefore, be expected to lead to herniation. In children with obtundation, bradycardia, and systemic hypertension, however, extreme care should be taken during the attack, preferably in an intensive care setting. Children with enlarging ventricles or with fluid spaces that are not collapsed should probably be immediately referred for a shunt revision. Trying to delay decisions in such situations may potentially lead to a disaster.
Treatment with dexamethasone can serve as a prompt way of lowering the intracranial pressure as a temporary measure until a decision regarding the surgical procedure with optimal timing can be made. This treatment carries a low risk of complications and may well prevent resorting to emergency procedures that entail a high risk of infection and other complications. Performing the surgical procedure on an elective basis enables a better work-up of the case and improved preparation of the patient for surgery.
In conclusion, short-term treatment with dexamethasone is effective in acute attacks of headaches, vomiting, and lethargy attributed to SVS. It can provide temporary relief during the decision-making process of whether and when to perform surgery.
References
Abbott IR, Epstein FJ, Wisoff JH (1991) Chronic headaches associated with a functioning shunt: usefulness of pressure monitoring. Neurosurgery 28:72–77
Baskin JJ, Manwaring KH, Rekate HL (1998) Ventricular shunt removal: the ultimate treatment of the slit ventricle syndrome. J Neurosurg 88:478–484
Benzel EC, Reeves JD, Kesterson L, Hadden TA (1992) Slit ventricle syndrome in children: clinical presentation and treatment. Acta Neurochir (Wien) 117:7–14
Bruce DA, Weprin B (2001) The slit ventricle syndrome. Neurosurg Clin N Am 36:709–717
Buxton N, Punt J (1999) Subtemporal decompression: the treatment of noncompliant ventricle syndrome. Neurosurgery 44:513–519
Cohen SR, Dauser RC, Newman MH, Muraszko K (1993) Surgical techniques of cranial vault expansion for increases in intracranial pressure in older children. J Craniofac Surg 4:167–176
David LR, Taylor RG, Argenta LC (1996) A technique for cranial bone expansion. J Craniofac Surg 7:151–155
Di Rocco C (1994) Is the slit-ventricle syndrome always a slit-ventricle syndrome? Childs Nerv Syst 10:49–58
Epstein F, Lapras C, Wisoff JH (1988) “Slit-ventricle syndrome”: etiology and treatment. Pediatr Neurosci 14:5–10
Epstein FJ, Fleischer AS, Hochwald GM, Ransohoff J (1974) Subtemporal craniectomy for recurrent shunt obstruction secondary to small ventricles. J Neurosurg 41:29–31
Gil Z, Siomin V, Beni-Adani L, Ben Sira L, Constantini S (2002) Ventricular catheter placement in children with hydrocephalus and small ventricles: the use of a frameless neuronavigation system. Childs Nerv Syst 18:26–29
Guzelbag E, Ersahin Y, Mutluer S (1997) Cerebrospinal fluid shunt complications. Turk J Pediatr 39:363–371
Holness RO, Hoffman HJ, Hendrick EB (1979) Subtemporal decompression for the slit-ventricle syndrome after shunting in hydrocephalic children. Childs Brain 5:137–144
Ide T, Aoki N, Miki Y (1995) Slit ventricle syndrome successfully treated by lumboperitoneal shunt. Neurol Res 17:440–442
Jain H, Sgouros S, Walsh AR, Hockley AD (2000) The treatment of infantile hydrocephalus: “differential-pressure” or “flow-control valves”. A pilot study. Childs Nerv Syst 16:242–246
Le H, Yamini B, Frim DM (2002) Lumboperitoneal shunting as a treatment for slit ventricle syndrome. Pediatr Neurosurg 36:178–182
Major O, Fedoresak I, Sipos L, Hantos P, Konya E, Dobronyi I, Paraicz E (1994) Slit-ventricle syndrome in shunt operated children. Acta Neurochir (Wien) 127:69–72
Obana WG, Raskin NH, Cogen PH, Szymanski JA, Edwards MS (1990) Antimigraine treatment for slit ventricle syndrome. Neurosurgery 27:760–763
Oi S, Matsumoto S (1987) Infantile hydrocephalus and the slit ventricle syndrome in early infancy. Childs Nerv Syst 3:145–150
Rekate HL (1993) Classification of slit-ventricle syndromes using intracranial pressure monitoring. Pediatr Neurosurg 19:15–20
Acknowledgements
We thank Esther Eshkol for editorial assistance.
Author information
Authors and Affiliations
Corresponding author
Additional information
A commentary on this paper is available at http://dx.doi.org/10.1007/s00381-004-1133-x
Rights and permissions
About this article
Cite this article
Fattal-Valevski, A., Beni-Adani, L. & Constantini, S. Short-term dexamethasone treatment for symptomatic slit ventricle syndrome. Childs Nerv Syst 21, 981–984 (2005). https://doi.org/10.1007/s00381-004-1132-y
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00381-004-1132-y