
Abstract
Purpose
Contemporary data regarding the effect of local treatment (LT) vs. non-local treatment (NLT) on cancer-specific mortality (CSM) in elderly men with localized prostate cancer (PCa) are lacking. Hence, we evaluated CSM rates in a large population-based cohort of men with cT1-T2 PCa according to treatment type.
Methods
Within the SEER database (2004–2014), we identified 44,381 men ≥ 75 years with cT1-T2 PCa. Radical prostatectomy and radiotherapy patients were matched and the resulting cohort (LT) was subsequently matched with NLT patients. Cumulative incidence and competing risks regression (CRR) tested CSM according to treatment type. Analyses were repeated after Gleason grade group (GGG) stratification: I (3 + 3), II (3 + 4), III (4 + 3), IV (8), and V (9-10).
Results
Overall, 4715 (50.0%) and 4715 (50.0%) men, respectively, underwent NLT and LT. Five and 7-year CSM rates for, respectively, NLT vs. LT patients were 3.0 and 5.4% vs. 1.5 and 2.1% for GGG II, 4.5 and 7.2% vs. 2.5 and 2.8% for GGG III, 7.1 and 10.0% vs. 3.5 and 5.1% for GGG IV, and 20.0 and 26.5% vs. 5.4 and 9.3% for GGG V patients. Separate multivariable CRR also showed higher CSM rates in NLT patients with GGG II [hazard ratio (HR) 3.3], GGG III (HR 2.6), GGG IV (HR 2.4) and GGG V (HR 2.6), but not in GGG I patients (p = 0.5).
Conclusions
Despite advanced age, LT provides clinically meaningful and statistically significant benefit relative to NLT. Such benefit was exclusively applied to GGG II to V but not to GGG I patients.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Over the last decade, three randomized controlled trials showed benefit for local treatment (LT) [i.e. radical prostatectomy (RP) or radiotherapy (RT)] vs. non-local treatment (NLT) (i.e. no surgery or radiation) in clinically localized prostate cancer (PCa) [1,2,3]. However, none of the them focused on subjects over 75-year-old, who were purposely excluded by study design. In consequence, the benefit of LT cannot be extrapolated to patients aged 75 years or older. Despite absence of phase III data, the European Association of Urology (EAU) [4] and the National Comprehensive Cancer Network (NCCN) [5] guidelines recommend either RP or RT in patients with localized PCa and life expectancy of more than 10 years. However, these recommendations are based on retrospective studies with small sample size relying on historic cohorts [6, 7]. This might limit their generalizability to contemporary patients.
Under this light, we aimed at assessing the effect of LT vs. NLT on cancer-specific mortality (CSM) in elderly (≥ 75 years) patients diagnosed with clinically localized cT1-T2 PCa. Furthermore, based on the pivotal role of life expectancy of more than 10 years in LT candidates, we tested actual 10 years survival rates according to treatment type: LT vs. NLT.
Materials and methods
Study cohorts
In the Surveillance Epidemiology and End Results (SEER) database (2004–2014), we focused on men over 75-year-old, with histologically confirmed adenocarcinoma of the prostate [International Classification of Disease for Oncology (ICD-O-3) code 8140 of the prostate (site code C61.9)] and validated prostate-specific antigen (PSA) data [8]. We only considered patients with localized prostate cancer cT1-T2, M0 and PSA < 20 ng/ml (EAU guidelines shows M1 PCa in 16% of individuals with PSA ≥ 20) [4], who underwent RP, RT (external beam radiotherapy) or NLT (no surgery or radiation) according to previously reported methodology [9, 10]. Patients who received watchful waiting, active surveillance or androgen deprivation therapy could not be identified in the SEER database as previously reported [9, 10]. In addition, patients receiving brachytherapy were excluded [11]. CSM was defined according to the SEER mortality code (code 28010). All other deaths were considered as other-cause mortality (OCM).
Statistics
Adjustment variables consisted of age, race (Caucasian, African American, unknown and other), marital status (married, unmarried, unknown), PSA, clinical T stage (cT1-T2), clinical N stage (cN0-NX-N1) and biopsy Gleason grade groups (GGG) [12], defined as GGG I (Gleason score 3 + 3), GGG II (Gleason score 3 + 4), GGG III (Gleason score 4 + 3), GGG IV (Gleason score 8) and GGG V (Gleason score 9-10). Moreover, patients were stratified according to D’Amico risk group classification [13]. According to treatment type, patients were categorized into three groups: RP, RT and NLT. Due to potentially important differences according to treatment received, we relied on two consecutives 1:1-nearest neighbor propensity score matches, which adjusted for potential baseline characteristic differences such as age, race, marital status, PSA, GGG and stage that might exist between RP and RT patients and between LT and NLT patients. First, patients underwent RP or RT were matched. Second, the cohort resulting from the first propensity score was matched with NLT patients [14].
Treatment type-stratified cumulative incidence rates were generated and compared with the Gray test for each GGG (I, II, III, IV and V) [15]. Univariable and multivariable (MVA) competing-risks regression (CRR) methodology assessed CSM, according to LT vs. NLT and GGG [16]. The latter accounts for the effect of OCM and provides the most unbiased estimate of CSM. Covariates included age, race, marital status, PSA, clinical stage, GGG and D’Amico risk group classification [13]. Moreover, 10 year OCM rates were assessed for LT and NLT patients. Finally, to expand the complexity of hypothesis testing, we repeated all previous analyses in the subset of patients with clinical lymph node stages cN0–NX.
All statistical tests were two-sided with a level of significance set at p < 0.05. Analyses were performed using the R software environment for statistical computing and graphics (version 3.3.0; http://www.r-project.org/).
Results
Clinical-pathologic characteristics
We identified 44,381 elderly (≥ 75 years) men with localized (cT1-T2, M0 and PSA < 20 ng/ml) PCa. Median age was 78 years [Interquartile range (IQR) 76–81). Most were Caucasian (35,884, 80.9%), married (29,107, 65.6%), harbored clinical stage cT1 (26,588, 59.9%) and belonged to GGG I (16,301, 36.7%). Median PSA was 7.5 ng/ml (IQR 5.3–10.7). Radical prostatectomy, RT or NLT were performed in 2569 (5.8%), 21,223 (47.8%) and 20,589 (46.4%) patients, respectively (Table 1).
Propensity score matching
The first propensity score matched cohort consisted of 5138 patients. Of those, 2569 (50.0%) underwent RP and 2569 (50.0%) underwent RT. The second propensity score matched cohort consisted of 9430 patients. Of those, 4715 (50.0%) underwent LT (RP or RT) and 4715 (50.0%) underwent NLT. No significant differences according to age, ethnicity, marital status, PSA, GGG and clinical stage existed within the first or the second matched cohorts (Supplementary Tables 1 and 2).
Survival analyses
Ten-year CSM rates recorded for RT and RP patients were 6.1 and 4.3% (p = 0.037) and resulted in a hazard ratio (HR) of 1.44 [95% CI (confidence interval) 1.02–2.04) (Supplementary Figure 1).
Ten year OCM-free survival rates recorded for NLT and LT patients were 50.6 (CI 53.5–47.7) and 63.5% (95% CI 60.6–66.4), respectively. Overall 5 and 7-year CSM rates, after accounting for OCM, were, respectively, 5.0 (95% CI 4.2–5.6) and 7.3% (95% CI 6.4–8.2) for NLT patients and 2.2 (95% CI 1.7–2.6) and 3.3% (95% CI 2.6–3.9) for LT patients (both p values < 0.001).
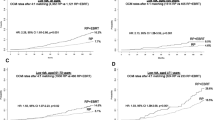
Five and 7-year CSM cumulative incidence rates recorded for GGG I NLT vs. LT patients were virtually the same: 1.4% (95% CI 0.7–2.1) vs. 1.2% (95% CI 0.5–1.9) and 2.4% (95% CI 1.3–3.5) vs. 2.2% (95% CI 1.2–3.2), respectively, (p = 0.4). Conversely, NLT GGG II, III, IV and V patients invariably exhibited higher CSM rates relative to LT counterparts. Specifically, 5- and 7-yr CSM rates for NLT vs. LT patients were 3.0% (95% CI 2.2–3.8) and 5.4% (95% CI 4.1–6.7) vs. 1.5% (95% CI 0.9–2.1) and 2.1% (95% CI 1.2–3.0) for GGG II (p < 0.001), 4.5% (95% CI 3.5–6.5) and 7.2% (95% CI 5.0–9.4) vs. 2.5% (95% CI 1.7–3.3) and 2.8% (95% CI 1.6–4.0) for GGG III (p = 0.001), 7.1% (95% CI 5.6–8.6) and 10.0% (95% CI 7.6–12.4) vs. 3.5% (95% CI 1.9–5.1) and 5.1% (95% CI 2.7–7.5) for GGG IV (p = 0.017), and 20.0% (95% CI 15.4–24.6) and 26.5% (95% CI 21.2–31.8) vs. 5.4% (95% CI 2.8–8.0) and 9.3% (95% CI 5.3–13.3) for patients with GGG V (p < 0.001) (Fig. 1).

Cumulative incidence plots depicting cancer-specific mortality rates stratified according to treatment for Gleason grade group I, II, III, IV and V localized cT1–T2 prostate cancer
In MVA CRR models that focused on the entire propensity score matched cohort, treatment specific HR predicting CSM was 2.25 (95%CI: 1.78–2.83, p < 0.001)-fold higher for, respectively, NLT vs. LT patients (Supplementary Table 3). In separate MVA CRR models stratified according to GGG (Table 2), treatment-specific HR predicting CSM for GGG I NLT patients did not differ (1.22, CI: 0.66–2.26) to their GGG I counterpart underwent LT (p = 0.5). Conversely, NLT patients with GGG II, III, IV and V exhibited 3.35- (95% CI 2.11–5.31), 2.57- (95% CI 1.57–4.19), 2.36- (95% CI 1.45–3.84) and 2.60-fold (95% CI 1.74–3.91) higher CSM rates, than LT patients (all p values < 0.001). Finally, virtually the same results were obtained for subgroup analyses focusing on cN0–NX stage patients (data not shown).
Discussion
Local treatment is controversial in patients with localized PCa aged 75 years or older based on potentially borderline life expectancy and marginal cancer-specific survival (CSS) benefit. None of the randomized controlled trials comparing NLT vs. LT in clinically localized PCa focused on patients above 75 years. Specifically, the Prostate, Lung, Colorectal, and Ovarian Cancer Screening Trial (PLCO) [1] and the Scandinavian Prostate Cancer Group Trial (SPCG) [2], which compared RP vs. observation, focused on patients aged less than 75 years. Similarly, the ProtecT trial [3], which compared RP vs. RT vs. active monitoring excluded patients aged more than 70 years. Based on this void, we decided to assess CSS in patients aged more than 75 years treated either with RP, RT or NLT. Our design differed from of that PLCO, SPCG and ProtecT because we focused on patients with localized disease only (cT1–T2, PSA < 20 ng/ml) and on those aged more than 75 years.
Our study showed several noteworthy findings. First, it indicated a clinically meaningful and statistically significant lower CSM in patients treated with LT vs. NLT. The net benefit recorded at 5 years ranged from 1.5 to 14.6%, while at 7 years of follow-up, it ranged from 3.3 to 17.2%, when GGG II to V patients were considered. This implies that LT should be considered in elderly men with localized PCa based on potential CSM reduction.
Second, stratified analyses according to GGG showed lower CSM rates in GGG II–V patients, but not in GGG I patients. This implies that LT may not represent ideal treatment for GGG I individuals and NLT should be considered instead. Our findings indirectly corroborate the results of non-interventional management of GGG I patients, especially in elderly individuals [17].
Third, it is particularly noteworthy that CSM benefit was also recorded in GGG II patients despite their intermediate characteristics [13]. In particular, our findings related to GGG II patients should be given attentive consideration, since active surveillance represents a treatment alternative in those men [18,19,20].
Fourth, we also examined OCM based on the consideration that CSM benefits are only valid if patients live long enough to enjoy a CSM reduction. Specifically, we focused on LT vs. NLT patients and performed stratified analyses according to GGG classification. Our results indicated that LT patients enjoyed higher OCM free-survival than the NLT counterparts. This validated the notion that the majority of patients selected for LT enjoyed a life expectancy that warrants such therapies.
Similarly, other investigators showed that LT could be safely performed in elderly men and that it could provide CSS benefit compared to NLT. For example, Mandel et al. [21]. included 13,997 RP patients and found that patients aged 75 years or older exhibited excellent long-term CSM-free survival (96.2% at 5 years). Kunz et al. [22]. included 1636 RP patients and found that advanced age (> 70 years) was not an independent predictor of CSM. Both authors concluded that advanced age should not be considered a contraindication to RP in healthy surgical candidates. Furthermore, Xylinas et al. demonstrated that even laparoscopic RP may be considered for localized PCa in elderly (> 75 years), well-selected patients. Finally, Dell’Oglio et al. [23]. evaluated CSS outcomes in elderly men aged 80 years or older found that RT was associated with more favorable CSM rates than NLT (HR 0.68, p < 0.001).
Our results are in agreement with other historical studies that are limited by inclusion of patients younger than 80 years. For example, Wong et al. [24]. enrolled 44,630 men (1991–1999) with organ-confined PCa, who underwent RP, RT or NLT. Their study suggested a survival advantage associated with LT for PCa in elderly men aged 65–80 years. Similarly, Liu et al. [25]. and Abdollah et al. [26]. showed a survival benefit associated with LT (RP or RT) compared to NLT. Liu et al. [25] included 5845 SEER Medicare patients, who underwent RP or NLT. Abdollah et al. [26]. compared RT vs. NLT in 404,604 men in the SEER database. Unlike our study, these investigators exclusively relied on historical data and only selected patients aged 65–80 years. Conversely, our study included patients aged ≥ 75 and provides most contemporary evidence that LT should be considered instead of NLT in this specific patient group, except for elderly patients with GGG I.
It should also be noted that elderly patients have a higher risk of being upgraded at RP compared to their young counterparts. According with the studies of Herlemann et al. [27]. and Busch et al. [28] the rate of upgrading ranged between 46 and 53% in elderly patients, and was much higher than in young patients (27–44%). The latter further supports LT use in elderly PCa patients.
Our study is not devoid of limitations. First, the SEER database does not include baseline performance status (Eastern Cooperative Oncology Group) and comorbidities. However, this limitation was obviated with CRR models that account for OCM, which represents a proxy of performance status and of significant comorbidities. Second, the SEER database also lacks information about RT dose (Gy), as well as information about RP type (open RP vs. robotic, retropubic RP vs. perineal RP, etc.). Third, due to sample size limitations, formal subgroup analyses and propensity score matching could be applied to cN sub-stages. Additionally, despite the sample size of the SEER database, the latter still represents a population sample with inherent limitations. Fourth, androgen deprivation therapy and chemotherapy data are not recorded in the SEER database. However, these therapies were likely administered in equal proportions in LT and NLT patients. Last but not least, we focused on cT1–T2 patients with PSA < 20 ng/ml treated with either RP or RT or NLT. These selection criteria may be interpreted as a narrow definition. However, it may also be argued that inclusion of patients with more advanced PCa (cT3 or higher stage, PSA valuesv > 20 ng/ml), that are treated with less-established treatment modalities than RP or RT, may not represent the typical profile of the usual elderly patients in whom the dilemma between LT vs. NLT may require consideration.
Conclusions
Despite advanced age, LT (RP or RT) provides a clinically meaningful and statistically significant benefit relative to NLT. Such benefit was confirmed for GGG II to V PCa but not for GGG I patients, where LT may be considered overtreatment. These observations should be considered in treatment decision making for elderly patients diagnosed with localized PCa.
References
Andriole GL, Crawford ED, Grubb RL et al (2009) Mortality results from a randomized prostate-cancer screening trial. N Engl J Med 360:1310–1319. doi:10.1056/NEJMoa0810696
Bill-Axelson A, Holmberg L, Garmo H et al (2014) Radical prostatectomy or watchful waiting in early prostate cancer. N Engl J Med 370:932–942. doi:10.1056/NEJMoa1311593
Hamdy FC, Donovan JL, Lane JA et al (2016) 10-Year outcomes after monitoring, surgery, or radiotherapy for localized prostate cancer. N Engl J Med 375:1415–1424. doi:10.1056/NEJMoa1606220
Mottet N, Bellmunt J, Bolla M et al (2017) EAU-ESTRO-SIOG guidelines on prostate cancer. part 1: screening, diagnosis, and local treatment with curative intent. Eur Urol 71:618–629. doi:10.1016/j.eururo.2016.08.003
Carroll PR, Parsons JK, Andriole G et al (2016) NCCN guidelines insights: prostate cancer early detection, version 2.2016. J Natl Compr Cancer Netw 14:509–519
Scosyrev E, Messing EM, Mohile S et al (2012) Prostate cancer in the elderly: frequency of advanced disease at presentation and disease-specific mortality. Cancer 118:3062–3070. doi:10.1002/cncr.26392
Richstone L, Bianco FJ, Shah HH et al (2008) Radical prostatectomy in men aged > or = 70 years: effect of age on upgrading, upstaging, and the accuracy of a preoperative nomogram. BJU Int 101:541–546. doi:10.1111/j.1464-410X.2007.07410.x
National Cancer Institute Surveillance, Epidemiology, and End Results Prostate-Specific Antigen Working Group, Adamo MP, Boten JA et al (2017) Validation of prostate-specific antigen laboratory values recorded in surveillance, epidemiology, and end results registries. Cancer 123:697–703. doi:10.1002/cncr.30401
Antwi S, Everson TM (2014) Prognostic impact of definitive local therapy of the primary tumor in men with metastatic prostate cancer at diagnosis: a population-based, propensity score analysis. Cancer Epidemiol 38:435–441. doi:10.1016/j.canep.2014.04.002
Leyh-Bannurah S-R, Budäus L, Pompe R et al (2017) North American Population-Based Validation of the National Comprehensive Cancer Network Practice Guideline Recommendation of Pelvic Lymphadenectomy in Contemporary Prostate Cancer. Prostate 77:542–548. doi:10.1002/pros.23292
Hoskin PJ, Rojas AM, Bownes PJ et al (2012) Randomised trial of external beam radiotherapy alone or combined with high-dose-rate brachytherapy boost for localised prostate cancer. Radiother Oncol J Eur Soc Ther Radiol Oncol 103:217–222. doi:10.1016/j.radonc.2012.01.007
Epstein JI, Zelefsky MJ, Sjoberg DD et al (2016) A contemporary prostate cancer grading system: a validated alternative to the Gleason score. Eur Urol 69:428–435. doi:10.1016/j.eururo.2015.06.046
D’Amico AV, Whittington R, Malkowicz SB et al (1998) Biochemical outcome after radical prostatectomy, external beam radiation therapy, or interstitial radiation therapy for clinically localized prostate cancer. JAMA 280:969–974
Mnatzaganian G, Davidson DC, Hiller JE, Ryan P (2015) Propensity score matching and randomization. J Clin Epidemiol 68:760–768. doi:10.1016/j.jclinepi.2015.01.002
Logan BR, Zhang M-J (2013) The use of group sequential designs with common competing risks tests. Stat Med 32:899–913. doi:10.1002/sim.5597
Scrucca L, Santucci A, Aversa F (2010) Regression modeling of competing risk using R: an in depth guide for clinicians. Bone Marrow Transplant 45:1388–1395. doi:10.1038/bmt.2009.359
Bokhorst LP, Valdagni R, Rannikko A et al (2016) A Decade of Active Surveillance in the PRIAS Study: an update and evaluation of the criteria used to recommend a switch to active treatment. Eur Urol 70:954–960. doi:10.1016/j.eururo.2016.06.007
Dall’Era MA, Klotz L (2017) Active surveillance for intermediate-risk prostate cancer. Prostate Cancer Prostatic Dis 20:1–6. doi:10.1038/pcan.2016.51
Musunuru HB, Yamamoto T, Klotz L et al (2016) Active surveillance for intermediate risk prostate cancer: survival outcomes in the sunnybrook experience. J Urol 196:1651–1658. doi:10.1016/j.juro.2016.06.102
Wong L-M, Tang V, Peters J et al (2016) Feasibility for active surveillance in biopsy Gleason 3 + 4 prostate cancer: an Australian radical prostatectomy cohort. BJU Int 117(Suppl 4):82–87. doi:10.1111/bju.13460
Mandel P, Kriegmair MC, Kamphake JK et al (2016) Tumor characteristics and oncologic outcome after radical prostatectomy in men 75-years-old or older. J Urol 196:89–94. doi:10.1016/j.juro.2016.01.009
Kunz I, Musch M, Roggenbuck U et al (2013) Tumour characteristics, oncological and functional outcomes in patients aged ≥ 70 years undergoing radical prostatectomy. BJU Int 111:E24–E29. doi:10.1111/j.1464-410X.2012.11368.x
Dell’Oglio P, Boehm K, Trudeau V et al (2016) Survival after conservative management versus external beam radiation therapy in elderly patients with localized prostate cancer. Int J Radiat Oncol Biol Phys 96:1037–1045. doi:10.1016/j.ijrobp.2016.05.004
Wong Y-N, Mitra N, Hudes G et al (2006) Survival associated with treatment vs observation of localized prostate cancer in elderly men. JAMA 296:2683–2693. doi:10.1001/jama.296.22.2683
Liu L, Coker AL, Du XL et al (2008) Long-term survival after radical prostatectomy compared to other treatments in older men with local/regional prostate cancer. J Surg Oncol 97:583–591. doi:10.1002/jso.21028
Abdollah F, Sun M, Schmitges J et al (2012) Competing-risks mortality after radiotherapy vs. observation for localized prostate cancer: a population-based study. Int J Radiat Oncol Biol Phys 84:95–103. doi:10.1016/j.ijrobp.2011.11.034
Herlemann A, Buchner A, Kretschmer A et al (2017) Postoperative upgrading of prostate cancer in men ≥ 75 years: a propensity score-matched analysis. World J Urol. doi:10.1007/s00345-017-2045-1
Busch J, Magheli A, Leva N et al (2014) Higher rates of upgrading and upstaging in older patients undergoing radical prostatectomy and qualifying for active surveillance. BJU Int 114:517–521. doi:10.1111/bju.12466
Author information
Authors and Affiliations
Contributions
MB: Protocol/project development, Data collection or management, Data analysis, Manuscript writing/editing. RP: Data collection or management. MM: Manuscript writing/editing. ZT: Data analysis. GG: Manuscript writing/editing. NF: Data analysis. Dt: Data analysis. MG: Data collection or management. FM: Protocol/project development. SFS: Data collection or management. AB: Protocol/project development. FS: Manuscript writing/editing. PIK: Manuscript writing/editing, Protocol/project development.
Corresponding author
Ethics declarations
Conflict of interest
The authors have stated that they have no conflict of interest.
Research involving human participants and/or animals
None.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Informed consent
None.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

{kind=link}
Cite this article
Bandini, M., Pompe, R.S., Marchioni, M. et al. Radical prostatectomy or radiotherapy reduce prostate cancer mortality in elderly patients: a population-based propensity score adjusted analysis. World J Urol 36, 7–13 (2018). https://doi.org/10.1007/s00345-017-2102-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00345-017-2102-9