
Abstract
Objective
To evaluate the performance of a multiparametric MRI radiomics-based nomogram for the individualised prediction of synchronous distant metastasis (SDM) in patients with clear cell renal cell carcinoma (ccRCC).
Methods
Two-hundred and one patients (training cohort: n = 126; internal validation cohort: n = 39; external validation cohort: n = 36) with ccRCC were retrospectively enrolled between January 2013 and June 2019. In the training cohort, the optimal MRI radiomics features were selected and combined to calculate the radiomics score (Rad-score). Incorporating Rad-score and SDM-related clinicoradiologic characteristics, the radiomics-based nomogram was established by multivariable logistic regression analysis, then the performance of the nomogram (discrimination and clinical usefulness) was evaluated and validated subsequently. Moreover, the prediction efficacy for SDM in ccRCC subgroups of different sizes was also assessed.
Results
Incorporating Rad-score derived from 9 optimal MR radiomics features (age, pseudocapsule and regional lymph node), the radiomics-based nomogram was capable of predicting SDM in the training cohort (area under the ROC curve (AUC) = 0.914) and validated in both the internal and external cohorts (AUC = 0.854 and 0.816, respectively) and also showed a convincing predictive power in ccRCC subgroups of different sizes (≤ 4 cm, AUC = 0.875; 4–7 cm, AUC = 0.891; 7–10 cm, 0.908; > 10 cm, AUC = 0.881). Decision curve analysis indicated that the radiomics-based nomogram is of clinical usefulness.
Conclusions
The multiparametric MRI radiomics-based nomogram could achieve precise individualised prediction of SDM in patients with ccRCC, potentially improving the management of ccRCC.
Key Points
• Radiomics features derived from multiparametric magnetic resonance images showed relevant association with synchronous distant metastasis in clear cell renal cell carcinoma.
• MRI radiomics-based nomogram may serve as a potential tool for the risk prediction of synchronous distant metastasis in clear cell renal cell carcinoma.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Renal cell carcinoma (RCC) is the seventh most common malignant tumour, killing more than 170,000 people worldwide in 2018 [1]. Clear cell RCC (ccRCC) is the primary histological subtype, accounting for approximately 90% of RCC [2]. CcRCC is an extremely aggressive urologic neoplasm. Approximately 30% of patients have distant metastases at the initial diagnosis (synchronous distant metastasis, SDM) [3], whereas approximately 20% of patients without distant metastases at initial nephrectomy will develop distant metastases during follow-up (metachronous distant metastasis) [4]. Among them, ccRCC with SDM has a distinct pathologic and molecular phenotype and results in a poor prognosis [5]. Early identification of SDM can ensure the reasonable, and effective treatments were timely offered or performed and eventually improve patient survival [6,7,8,9].
In general, urologists often evaluate the risk of SDM based on experience, such as the tumour size and clinical symptoms. The tumour size was indeed a valuable predictor for SDM (odds ratio (OR), 1.22 to 1.25) [10, 11]. However, small ccRCCs can also present SDM [12], and the tumours with similar size can demonstrate the different risks in SDM, so the overreliance on the tumour size can lead to the missed diagnosis of SDM. Furthermore, the clinical signs of SDM can be slight or even absent, which could lead to the ignorance of further investigation on SDM by the doctors.
Nowadays, many advanced imaging modalities can contribute to the detection or confirmation of SDM. However, it is of a massive economic and physical burden to use multiple imaging methods to check all potential metastatic sites for each patient with ccRCC; after all, RCC can metastasise to virtually any part of the human body [13]. Besides, sometimes even enough imaging examinations were performed, the risk of a missed diagnosis and misdiagnosis still exists due to the small size of suspicious metastases or an atypical radiographic appearance [14,15,16]. So, besides the tumour size, how we can precisely evaluate the personalised risk of the SDM with increased confidence raised our concern.
The SDM was closely related to the primary tumour. The nature of the primary tumour, such as histological grade, T staging, gene expression and functional characteristics, may be associated with distant metastases [3, 17, 18]. Medical imaging can noninvasively visualise the strong phenotypic difference that primary tumours exhibited [19]. Magnetic resonance imaging (MRI), as the preferred examination method for renal tumours, can provide abundant data related to anatomy, morphology and potential functionality based on its superior soft-tissue contrast, spatial resolution and multiple imaging sequences. Nevertheless, we cannot identify some potential features on a visual basis. As an emerging technique used to extract additional information from diagnostic clinical imaging, radiomics can extract high-throughput quantitative data from medical images and indirectly reflect tumour heterogeneity which could not be recognised by the naked eye [20]. The correlation between quantitative data and pathological phenotypes allows the noninvasive detection of tumour bio-behaviours [21]. Some studies have confirmed that radiomics features could be used as prognostic or predictive indicators [20, 21]. At present, radiomics for kidney cancer has demonstrated the ability in the prediction of histological subtype, pathologic grade and therapeutic effects [20, 22,23,24,25].
In this study, we will evaluate whether a multiparametric MRI radiomics-based nomogram can make individualised prediction of SDM in patients with ccRCC and facilitate the more precise selection of ccRCC patients for further investigation on SDM in clinical practice.
Materials and methods
Patients’ information
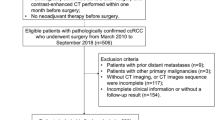
Ethical approval was obtained for this retrospective analysis, and informed consent was waived by the institutional review board of our hospital. In this study, one training cohort, an independent internal validation cohort and an external validation cohort were established, respectively. The training cohort and the internal validation cohort comprised a retrospective collection of patients with histologically confirmed ccRCC who visited our centre between January 2013 and October 2018 and from November 2018 to June 2019, respectively. The external validation cohort was established by collecting the patients in the other three medical centres between January 2015 and February 2019. CcRCC patients with SDM were consecutively collected, while patients without SDM were randomly selected according to the distribution of tumour size of ccRCC in the SDM group (4 cm/4–7 cm/7–10 cm/10 cm). The sample size ratio between the SDM group and the non-SDM group was 1:2, which was approximately in line with the incidence of SDM in ccRCC (1/4–1/3) [3]. SDMs were confirmed by biopsy or surgical pathology or follow-up (the suspicious metastases existing before nephrectomy gradually increased in size or number or decreased after molecularly targeted therapy between 6 months and 5 years of follow-up); the patients without SDMs were confirmed by no signs of distant metastases through whole-body imaging examinations before nephrectomy or no suspicious metastasis during follow-up. The enrolment of patients is displayed in Fig. 1, and the inclusion and exclusion criteria are listed in the Supplementary Material.

The flowchart of patient recruitment
MRI acquisition
MR images were acquired with 3.0 T scanners (Signa HDX and Discovery MR750, GE Healthcare) and consisted of six sequences including axial fat-suppressed T2-weighted imaging (T2WI), diffusion-weighted imaging (DWI), T1-weighted imaging (T1WI) and contrast-enhanced T1WI (corticomedullary phase, nephrographic phase and excretory phase (EP)). The detailed parameters of MRI sequences are described in Supplementary Table 1.
Clinicoradiologic model construction
Demographic and clinical data were collected by a urologist (Q.B.H.) from the medical records of the four institutions, which are defined in Table 1. Two radiologists (W.X. and X.B., with a 9-year experience and 5-year experience in abdominal MRI diagnosis, respectively) who were blinded to the clinical data and pathology results simultaneously evaluated the MR images at the picture archiving and communication system (PACS) workstation in consensus.
The differences of clinicoradiologic characteristic between ccRCC patients with and without SDM in the training cohort were analysed, then the clinicoradiologic characteristics with significant differences were selected to construct a clinicoradiologic model by multivariable logistic regression analysis. The calibration of the model was evaluated by the calibration curve and the Hosmer-Lemeshow test.
MR image segmentation and radiomics feature extraction and selection
Based on kidney MRI data from the PACS, the images from FS-T2WI, DWI, T1WI and contrast-enhanced T1WI were exported and uploaded to the RadCloud (Huiying Medical Technology Co., Ltd.) which was an available platform reliably used in previous studies [26, 27]. Then, except for the first and last slices, the outline of all contiguous slices of the entire tumour were delineated [28] and 1029 radiomics features were extracted from multiparametric MR images, respectively, including first-order features, shape features, second-order features and higher-order features derived from the robust transformation of first-order and second-order features. The transformation methods included exponential, square, square root, logarithmic and wavelet (wavelet-LHL, wavelet-LHH, wavelet-HLL, wavelet-LLH, wavelet-HLH, wavelet-HHH, wavelet-HHL and wavelet-LLL) transformations [29].
In the training cohort, before identifying the optimal features, the resampling strategy was adopted to improve the robustness of the selected features; namely, 90% of samples were randomly extracted 20 times, and feature selection was carried out each time to identify the features that were selected more than 5 times for subsequent analysis.
Based on 90% of the training samples extracted each time and all training samples used for the final determination of the optimal features, three methods were used for feature selection. First, a variance threshold method was applied to remove the undifferentiated variables, and features with variance < 0.8 were excluded from further analysis. Then, associations between the radiomics features and the metastatic status of ccRCC were analysed using SelectKBest and the features with nonsignificant difference (p ≥ 0.05) were further removed. Third, the least absolute shrinkage and selection operator (LASSO) regression with 10-fold cross-validation was used to identify the features with the best correlation and reproducibility [30, 31]. The intra- and inter-observer reproducibility was performed by reader 1 (X.B.) and reader 2 (M.F.W., with a 3-year experience), which was described in detail in the Supplementary Material.
The radiomics scores (Rad-scores) were obtained by calculating all the selected features via a linear combination for each lesion. The potential association of the Rad-score with SDM was assessed using a Mann-Whitney U test and verified by stratified analyses.
Radiomics-based nomogram construction
Combined clinicoradiologic characteristics and the Rad-score, a radiomics-based model was established based on multivariable logistic regression, which presented as a nomogram to predict the individual risk of SDM in ccRCC patients. The calibration curve was plotted to access the calibration of the nomogram, accompanied by the Hosmer-Lemeshow test.
Evaluation, verification and comparison of the two models’ performance
The prediction performance of the radiomics-based nomogram and the clinicoradiologic model was assessed by receiver operating characteristic (ROC) curve analysis. In the internal and external validation cohorts, logistic regression was applied to all patients to test the efficiency and reproducibility of the two models. Decision curve analysis (DCA) was implemented to evaluate the net benefits of the models at different threshold probabilities [32]. Moreover, the prediction performance of the nomogram in arbitrary subgroups of different sizes was also validated based on all ccRCC patients in the three cohorts.
Statistical analysis
All statistical analyses were performed with Stata/MP 14.0 (StataCorp) for Windows. The Mann-Whitney U test was used for the analysis of continuous variables, and the chi-square test was used for the analysis of categorical variables. A p value < 0.05 was considered statistically significant. All estimated p values were two-sided. Inter- and intra-class correlation coefficients (ICCs) greater than 0.80 were considered to have a good agreement. The discrimination ability of the models was evaluated and compared by the area under the ROC curve (AUC) (DeLong’s test).
Results
Patients information
In the training cohort, 126 patients with a solitary tumour were included (97 males and 29 females; mean age, 56.4 ± 9.8 years; 42 ccRCC patients with SDM and 84 ccRCC patients without SDM). In the internal validation cohort, 39 consecutive patients (24 males and 15 females; mean age, 54.5 ± 10.3 years; 13 with SDM and 26 without SDM) were included. In the external validation cohort, 36 patients (27 males and 9 females; mean age, 56.4 ± 9.8 years; 12 with SDM and 24 without SDM) were collected anonymously. The confirmation approaches and sites of metastases are shown in Table 2. The entire recruitment process is shown in the shape of a flowchart (Fig. 1). The clinicoradiologic and pathological characteristics of each patient in the training and validation cohorts are presented in Table 3 and Supplementary Table 2.
Clinicoradiologic model construction
According to multivariable logistic regression, three clinicoradiologic indicators (age, regional lymph node (RLN) and pseudocapsule) were incorporated into the model (the clinicoradiologic model) (Table 4). The model demonstrated no apparent departure from a perfect fit on the calibration curve (Fig. 2a) and yielded a nonsignificant statistic in the Hosmer-Lemeshow test (p = 0.794).

Calibration curves of the two models in the training cohort. a Calibration curve of the clinicoradiologic model and (b) the radiomics-based nomogram. The calibration curves describe the calibration of each model by comparing the SDM prediction risk with the SDM observations. The y-axis represents the observed SDM rate. The x-axis represents the predicted SDM risk. The diagonal represents a perfect prediction of an ideal model. The blue line segment near the x-axis visually shows the distribution of ccRCCs with and without SDM as the predicted probability increases. SDM, synchronous distant metastasis
Radiomics feature extraction and selection
Among the 126 patients in the training cohort, 64 features were identified by resampling and finally reduced to 9 potential predictive parameters according to the LASSO regression (Fig. 3a–d). The skewness, interquartile range (IQR), large area low grey level emphasis (LALGLE) and dependence variance (DV) of T2WI; skewness and DV of T1WI; kurtosis of DWI; and DV and grey level variance (GLV) of EP had satisfactory intra-observer (ICCs, 0.806–0.962) and inter-observer (ICCs, 0.865–0.994) reproducibility (see details in the Supplementary Material).

Radiomics analysis and model construction workflow. a Volumes of interest on the primary lesions of ccRCCs with and without SDM. The yellow regions indicate the renal lesions manually delineated on T2WI, DWI, T1WI and CE-T1WI. b According to a variance threshold of 0.8, sixty-four features were reduced to sixty-two potential predictors. c Fourteen radiomics features were further selected by univariate analysis (p < 0.05). d Nine optimal radiomics features were finally selected according to LASSO algorithm (10-fold cross-validation, alpha [the optimal value of the LASSO tuning parameter] = 1.7). e Distributions of the radiomics scores for each patient. CcRCC patients with SDM (red line) were more likely to obtain higher radiomics scores, while those without SDM (blue line) had the opposite. f Flowchart of radiomics analysis and model construction. CP, corticomedullary phase; NP, nephrographic phase; EP, excretory phase; SDM, synchronous distant metastasis; LASSO, the least absolute shrinkage and selection operator
The Rad-score was obtained by calculating the 9 optimal features via a linear combination for each lesion (Supplementary Table 3). The difference in the Rad-scores between ccRCC patients with and without SDM was significant in the three cohorts (Table 3). Stratified analysis showed that the significant correlation between the Rad-score and SDM was not affected by sex, tumour size, WHO/ISUP grade, MR scanner, etc. (Table 5). The Rad-score distributions are illustrated in Fig. 3e.
Radiomics-based nomogram construction
After logistic regression analysis, age, RLN, pseudocapsule and the Rad-score were included as independent predictors in the radiomics-based model (Table 4), which was presented as a nomogram (Fig. 4). Good calibration was observed for the prediction probability of SDM (Fig. 2b), and the Hosmer-Lemeshow test yielded a nonsignificant statistic (p = 0.811). The complete flowchart of radiomics analysis and model construction is presented in Fig. 3f.

Radiomics-based nomogram for the prediction of SDM in ccRCC patients. The radiomics-based nomogram was established by incorporating the pseudocapsule, radiomics score, the short axis of regional lymph node and age. The sum of the scores on the scoring ruler corresponding to the four predictors is the total score, and the scale values of the upper ruler corresponding to the total score are the risk of SDM. SDM, synchronous distant metastasis
Evaluation, verification and comparison of the two models’ performance
Using ROC curve analysis, the clinicoradiologic model yielded an AUC of 0.836 (95% CI, 0.761 to 0.910) in the training cohort, 0.731 (95% CI, 0.566 to 0.896) in the internal validation cohort and 0.677 (95% CI, 0.473 to 0.881) in the external validation cohort, respectively. The radiomics-based nomogram reached an AUC of 0.914 (95% CI, 0.864 to 0.963) in the training cohort, which was also validated in the internal cohort (AUC, 0.854 [95% CI, 0.736 to 0.971]) and the external cohort (AUC, 0.816 [95% CI, 0.661 to 0.971]) (Fig. 5a–c).

ROC curves of the radiomics-based nomogram and the clinicoradiologic model for the prediction of SDM in the three cohorts and decision curve analysis for the two models. Compared to the clinicoradiologic model, the radiomics-based nomogram obtained higher AUC values in the training cohort (a), the internal validation cohort (b) and the external validation cohort (c), showing higher predictive power. d Decision curve analysis for the two models. The net benefit versus the threshold probability was plotted. The threshold probability is the probability of SDM in this study, with values ranging from 0 to 100. The sensitivity and specificity of the model are calculated at each threshold to determine the net benefit. The green and black lines represent the hypothesis that all ccRCC patients and no ccRCC patients had SDM (which is used for reference to determine subsequent clinical management), respectively. The net benefits of the radiomics-based nomogram (red line) were superior to the benefits of the clinicoradiologic model (blue line) across most ranges of threshold probability. ROC, receiver operating characteristic curve; AUC, area under ROC curve; SE, sensitivity; SP, specificity
The comparison between the two models showed that the radiomics-based nomogram yielded higher AUC than the clinicoradiologic model in the training cohort (0.914 vs. 0.836, p = 0.004), internal validation cohort (0.854 vs. 0.731, p = 0.046) and external validation cohort (0.816 vs. 0.677, p = 0.011). DCA for the radiomics-based nomogram suggested that using the nomogram to predict SDM added more net benefit than the clinicoradiologic model (Fig. 5d).
Based on all ccRCC patients in the three cohorts, the AUCs of the radiomics-based nomogram among all the subgroups of different sizes of ccRCC are shown as follows: size ≤ 4 cm, 0.875 (95% CI, 0.728–1.000); size 4–7 cm, 0.891 (95% CI, 0.822–0.960); size 7–10 cm, 0.908 (95% CI, 0.833–0.983); and size > 10 cm, 0.881 (95% CI, 0.763–0.999) (Fig. 6).

ROC curves of the radiomics-based nomogram for the prediction of SDM in ccRCC subgroups of different sizes. The radiomics-based nomogram yielded good performance in all the subgroups of ccRCCs with primary tumour size ≤ 4 cm (a), size 4–7 cm (b), size 7–10 cm (c) and size > 10 cm (d). ROC, receiver operating characteristic curve; AUC, area under ROC curve; SE, sensitivity; SP, specificity
Discussion
The occurrence of SDM means more active treatment options for ccRCC [9] and poor prognosis for patients with ccRCC [3]. Early and accurate recognition of the status of SDM was vital for the management of patients with ccRCC. In this study, we established a radiomics-based model for predicting SDM in ccRCC patients by incorporating MRI-derived Rad-score, age, pseudocapsule and RLN. This model, visually displayed on nomogram in the form of scale [33], demonstrated impressive predictive efficiency (AUC, 0.816–914) in the three cohorts. Hence, this nomogram could provide evidence for the individualised identification of patients who need further examination on SDM.
Primary tumour size is an independent predictor of SDM in ccRCC patients [10, 11]. Nevertheless, the risk of SDM varies for tumours with the same size, and it is controversial whether the size of primary tumours in small renal masses (SRMs) is significantly correlated with the risk of SDM [34]. Zastrow et al [35] analysed the prognostic value of the primary tumour size based on their RCC database and found that there was no significant correlation between the size and the risk of SDM in T1a RCC. Their model by combining the primary tumour size and clinical indicators shows good predictive power for SDM of RCC (C-index, 0.82), but there is no evidence that this model can be used to predict the SDM of T1a RCC and available for other independent databases. In this study, we matched the dimensions of primary tumours between ccRCC patients with and without SDM, thus ensuring that the variability of candidate predictors was derived from the different metastatic status of ccRCC rather than the different tumour sizes. Compared with the model built by Zastrow et al [35], our radiomics-based nomogram has convincing prediction power for SDM in ccRCC subgroups of different sizes in both the training cohort and the independent validation cohorts including SRMs (AUC, 0.875–0.908), which indicated that intra-tumour imaging features other than tumour size could also be the predictors for SDM.
Besides the tumour size, some clinicoradiologic indicators associated with the malignant behaviour of ccRCC have been reported by previous works of literature, which also were confirmed in our study. Previously, Wei et al [36] demonstrated that the lack of a pseudocapsule had a remarkably adverse impact on the prognosis of ccRCC patients, and Karlo et al [37] showed that well-defined tumour margins were more common among ccRCC patients with a loss of von-Hippel-Lindau function, which indicates low tumour aggressiveness. Also, tumour thrombus and size of RLN were associated with metastasis in RCC [38, 39]. Similarly, our study revealed significant differences in these aspects between ccRCC patients with and without SDM. In this study, age, pseudocapsule and RLN were eventually used as independent predictors to construct the clinicoradiologic model. Compared with the clinicoradiologic model that only relied on clinical and imaging indicators, the final radiomics-based nomogram achieved higher prediction performance for SDM. Based on the training cohort data, DCA analysis revealed that using the radiomics-based nomogram to predict SDM in ccRCC patients offers more significant benefits than merely relying on clinical and imaging information.
Through the LASSO algorithm, a valid tool to reduce dimensionality and remove the redundancy of radiomics features [31], we ultimately selected nine features derived from six original features (skewness, kurtosis, IQR, DV, LALGLE and GLV) based on T2WI, T1WI, DWI and EP as independent features with the best reproducibility and significant relation to metastasis. In previous literature, kurtosis, skewness, IQR and LALGLE have been proven to be prognostic markers for patients with malignant tumours in ccRCC and other types of tumours [40,41,42,43,44]; for example, the kurtosis and skewness of apparent diffusion coefficient (ADC) map intensities and the IQR of contrast-enhanced CT attenuation values can be used to distinguish between low- (I–II) and high-stage (III–IV) ccRCCs [40, 41]. In our study, skewness, IQR, LALGLE of T2WI, skewness of T1WI and kurtosis of DWI could predict the status of SDM, which may suggest that these types of parameters were beneficial in predicting bio-behaviour of malignant tumours. Meanwhile, we discovered that the DV of T2WI and T1WI and the DV and GLV of EP were associated with the metastatic status of ccRCC, which have not been proposed before.
Our study had several limitations. First, as a retrospective study, the selection bias in patients’ enrolment cannot be completely avoided. Second, some SDMs were confirmed by radiological changes instead of histopathological results, although acceptable in clinical practice, which might lead to the omission of some metastases and weaken the substantiality of this study. Third, this MRI radiomics-based nomogram was only developed and validated on the 3.0 T MR scanners, so its generalisation needs to be further explored. Fourth, due to relatively small sample size and uneven distribution of metastatic sites of SDM, this study only involved in predicting whether the SDM exists instead of the more exciting topic—prediction of the exact location of SDM. However, we believe this study can lay a foundation for the application of radiomics methods to predict the site of SDM accurately. Finally, due to the administration of the gadolinium-based contrast agent for contrast-enhanced imaging, this MRI radiomics-based nomogram may be inapplicable to individuals with severe renal insufficiency.
In conclusion, the MRI radiomics-based nomogram established by combining the Rad-score, age, pseudocapsule and RLN can serve as a potential tool to facilitate the individualised prediction of SDM preoperatively and provide guidance for imaging tests and treatment decision-making.
Abbreviations
- AUC:
-
Area under the ROC curve
- ccRCC:
-
Clear cell renal cell carcinoma
- DCA:
-
Decision curve analysis
- EP:
-
Excretory phase
- MRI:
-
Magnetic resonance imaging
- Rad-score:
-
Radiomics score
- RLN:
-
Regional lymph node
- ROC:
-
Receiver operating characteristic
- SDM:
-
Synchronous distant metastasis
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A (2018) Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 68:394–424
Patard JJ, Leray E, Rioux-Leclercq N et al (2005) Prognostic value of histologic subtypes in renal cell carcinoma: a multicenter experience. J Clin Oncol 23:2763–2771
Kammerer-Jacquet SF, Brunot A, Pladys A et al (2017) Synchronous metastatic clear-cell renal cell carcinoma: a distinct morphologic, immunohistochemical, and molecular phenotype. Clin Genitourin Cancer 15:e1–e7
Dabestani S, Thorstenson A, Lindblad P, Harmenberg U, Ljungberg B, Lundstam S (2016) Renal cell carcinoma recurrences and metastases in primary non-metastatic patients: a population-based study. World J Urol 34:1081–1086
Donskov F, Xie W, Overby A et al (2020) Synchronous versus metachronous metastatic disease: impact of time to metastasis on patient outcome-results from the International Metastatic Renal Cell Carcinoma Database Consortium. Eur Urol Oncol. https://doi.org/10.1016/j.euo.2020.01.001
Gill DM, Hahn AW, Hale P, Maughan BL (2018) Overview of current and future first-line systemic therapy for metastatic clear cell renal cell carcinoma. Curr Treat Options Oncol 19:6
Kato S, Demura S, Murakami H, Tsuchiya H (2019) Surgical metastasectomy for renal cell carcinoma: which patients are the real candidates for surgery? Ann Transl Med 7:S273
Nizam A, Schindelheim JA, Ornstein MC (2020) The role of active surveillance and cytoreductive nephrectomy in metastatic renal cell carcinoma. Cancer Treat Res Commun 23:100169
Ljungberg B, Bensalah K, Canfield S et al (2015) EAU guidelines on renal cell carcinoma: 2014 update. Eur Urol 67:913–924
Kunkle DA, Crispen PL, Li T, Uzzo RG (2007) Tumor size predicts synchronous metastatic renal cell carcinoma: implications for surveillance of small renal masses. J Urol 177:1692–1697
Thompson RH, Hill JR, Babayev Y et al (2009) Metastatic renal cell carcinoma risk according to tumor size. J Urol 182:41–45
Guðmundsson E, Hellborg H, Lundstam S, Erikson S, Ljungberg B (2011) Metastatic potential in renal cell carcinomas ≤7 cm: Swedish Kidney Cancer Quality Register data. Eur Urol 60:975–982
Diaz de Leon A, Pirasteh A, Costa DN et al (2019) Current challenges in diagnosis and assessment of the response of locally advanced and metastatic renal cell carcinoma. Radiographics 39:998–1016
Rasmussen F (2013) Metastatic renal cell cancer. Cancer Imaging 13:374–380
Hou TC, Wu CC, Yang CR, Wang J (2010) Synchronous renal cell carcinoma and clear cell hepatocellular carcinoma mimicking metastatic disease. Pathol Res Pract 206:342–345
Lyu HL, Cao JX, Wang HY et al (2018) Differentiation between pancreatic metastases from clear cell renal cell carcinoma and pancreatic neuroendocrine tumor using double-echo chemical shift imaging. Abdom Radiol (NY) 43:2712–2720
Yu J, Xu Q, Huang DY et al (2017) Prognostic aspects of dynamic contrast-enhanced magnetic resonance imaging in synchronous distant metastatic rectal cancer. Eur Radiol 27:1840–1847
Mendoza DP, Dagogo-Jack I, Chen T et al (2019) Imaging characteristics of BRAF-mutant non-small cell lung cancer by functional class. Lung Cancer 129:80–84
Aerts HJ, Velazquez ER, Leijenaar RT et al (2014) Decoding tumour phenotype by noninvasive imaging using a quantitative radiomics approach. Nat Commun 5:4006. https://doi.org/10.1038/ncomms5006
Shinagare AB, Krajewski KM, Braschi-Amirfarzan M, Ramaiya NH (2017) Advanced renal cell carcinoma: role of the radiologist in the era of precision medicine. Radiology 284:333–351
Mazurowski MA (2015) Radiogenomics: what it is and why it is important. J Am Coll Radiol 12:862–866
Wang W, Cao KM, Jin SM, Zhu XL, Ding JH, Peng WJ (2020) Differentiation of renal cell carcinoma subtypes through MRI-based radiomics analysis. Eur Radiol. https://doi.org/10.1007/s00330-020-06896-5
Deng Y, Soule E, Samuel A et al (2019) CT texture analysis in the differentiation of major renal cell carcinoma subtypes and correlation with Fuhrman grade. Eur Radiol 29:6922–6929
Li ZC, Zhai GT, Zhang JH et al (2019) Differentiation of clear cell and non-clear cell renal cell carcinomas by all-relevant radiomics features from multiphase CT: a VHL mutation perspective. Eur Radiol 29:3996–4007
Bektas CT, Kocak B, Yardimci AH et al (2019) Clear cell renal cell carcinoma: machine learning-based quantitative computed tomography texture analysis for prediction of Fuhrman nuclear grade. Eur Radiol 29:1153–1163
Zhang Y, Zhu Y, Shi X et al (2019) Soft tissue sarcomas: preoperative predictive histopathological grading based on radiomics of MRI. Acad Radiol 26:1262–1268
Shu J, Tang Y, Cui J et al (2018) Clear cell renal cell carcinoma: CT-based radiomics features for the prediction of Fuhrman grade. Eur J Radiol 109:8–12
Kocak B, Ates E, Durmaz ES, Ulusan MB, Kilickesmez O (2019) Influence of segmentation margin on machine learning-based high-dimensional quantitative CT texture analysis: a reproducibility study on renal clear cell carcinomas. Eur Radiol 29:4765–4775
Zwanenburg A, Leger S, Vallières M, Löck S (2016) Image biomarker standardisation initiative - feature definitions. arXiv:1612.07003
Park JE, Park SY, Kim HJ, Kim HS (2019) Reproducibility and generalizability in radiomics modeling: possible strategies in radiologic and statistical perspectives. Korean J Radiol 20:1124–1137
Rao SJ (2003) Regression modeling strategies: with applications to linear models, logistic regression, and survival analysis. J Am Stat Assoc 98:257–258
Vickers AJ, Elkin EB (2006) Decision curve analysis: a novel method for evaluating prediction models. Med Decis Making 26:565–574
Balachandran VP, Gonen M, Smith JJ, DeMatteo RP (2015) Nomograms in oncology: more than meets the eye. Lancet Oncol 16:e173–e180
Klatte T, Patard JJ, de Martino M et al (2008) Tumor size does not predict risk of metastatic disease or prognosis of small renal cell carcinomas. J Urol 179:1719–1726
Zastrow S, Phuong A, von Bar I, Novotny V, Hakenberg OW, Wirth MP (2014) Primary tumor size in renal cell cancer in relation to the occurrence of synchronous metastatic disease. Urol Int 92:462–467
Wei X, Wang J, Liu L et al (2018) Evaluation of tumor pseudocapsule status and its prognostic significance in renal cell carcinoma. J Urol 199:915–920
Karlo CA, Di Paolo PL, Chaim J et al (2014) Radiogenomics of clear cell renal cell carcinoma: associations between CT imaging features and mutations. Radiology 270:464–471
Zisman A, Wieder JA, Pantuck AJ et al (2003) Renal cell carcinoma with tumor thrombus extension: biology, role of nephrectomy and response to immunotherapy. J Urol 169:909–916
Gershman B, Takahashi N, Moreira DM et al (2016) Radiographic size of retroperitoneal lymph nodes predicts pathological nodal involvement for patients with renal cell carcinoma: development of a risk prediction model. BJU Int 118:742–749
Huhdanpaa H, Hwang D, Cen S et al (2015) CT prediction of the Fuhrman grade of clear cell renal cell carcinoma (RCC): towards the development of computer-assisted diagnostic method. Abdom Imaging 40:3168–3174
Kierans AS, Rusinek H, Lee A et al (2014) Textural differences in apparent diffusion coefficient between low- and high-stage clear cell renal cell carcinoma. AJR Am J Roentgenol 203:W637–W644
Ng F, Ganeshan B, Kozarski R, Miles KA, Goh V (2013) Assessment of primary colorectal cancer heterogeneity by using whole-tumor texture analysis: contrast-enhanced CT texture as a biomarker of 5-year survival. Radiology 266:177–184
Yang Y, Wang WW, Ren Y et al (2019) Computerized texture analysis predicts histological invasiveness within lung adenocarcinoma manifesting as pure ground-glass nodules. Acta Radiol 60:1258–1264
Cui EM, Li ZY, Ma CY et al (2020) Predicting the ISUP grade of clear cell renal cell carcinoma with multiparametric MR and multiphase CT radiomics. Eur Radiol 30:2912–2921
Acknowledgements
We thank Dr. Lin Li (PhD) (Professor, Medical Statistics, Institute for Hospital Management Research, Chinese PLA General Hospital) for his guidance on the statistical analysis in this study.
Funding
We acknowledge the financial support from the National Natural Science Foundation of China (Grant No. 81971580) and from the Medical Big Data Research and Development Project supported by Chinese PLA General Hospital (Grant No. 2018MBD-023).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Guarantor
The scientific guarantor of this publication is Dr. Haiyi Wang.
Conflict of interest
The authors of this manuscript declare no conflict of interests.
Statistics and biometry
No complex statistical methods were necessary for this paper.
Informed consent
Written informed consent was waived by the institutional review board.
Ethical approval
Institutional review board approval was obtained.
Methodology
• Retrospective
• Diagnostic or prognostic study
• Multicentre study
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOCX 54 kb)
Rights and permissions
About this article

Cite this article
Bai, X., Huang, Q., Zuo, P. et al. MRI radiomics-based nomogram for individualised prediction of synchronous distant metastasis in patients with clear cell renal cell carcinoma. Eur Radiol 31, 1029–1042 (2021). https://doi.org/10.1007/s00330-020-07184-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-020-07184-y