
Abstract
Objectives
To explore the correlations between DCE-MRI quantitative parameters and synchronous distant metastasis and the clinicopathological factors in rectal cancers.
Methods
Sixty-three patients with rectal cancer (synchronous distant metastasis, n = 31; non-metastasis, n = 32) were enrolled in this study. Student’s t test and ANOVA were used to compare DCE-MRI parameters (K trans, K ep and V e ). The receiver operating characteristic (ROC) analysis was used to find the reasonable threshold of DCE-MRI parameters to differentiate lesions with synchronous distant metastasis from those without metastasis.
Results
The K trans, K ep , and V e value were significantly higher in the lesions with distant metastasis than in the lesions without distant metastasis (0.536 ± 0.242 vs. 0.299 ± 0.118 min-1, p < 0.001; 1.598 ± 0.477 vs. 1.341 ± 0.390 min-1, p = 0.022; and 0.324 ± 0.173 vs. 0.249 ± 0.091, p = 0.034; respectively). The K trans showed the highest AUCs of 0.788 (p < 0.001), with sensitivity of 61.29 % and specificity of 87.5 %, respectively.
Conclusions
DCE-MRI parameters may represent a prognostic indicator for synchronous distant metastases in patients with rectal cancer.
Key Points
• The K trans , K ep and V e values correlated with synchronous distant metastasis.
• Higher K trans , K ep and V e values were noted among patients with metastasis.
• DCE-MRI parameters might represent a prognostic indicator for synchronous distant metastases.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Preoperative rectal cancer staging is based on two key principles, namely, prognostic staging and defining the anatomy in order to plan treatment. Currently, many studies on preoperative MRI have concentrated on T and N staging and the circumferential resection margin (CRM). The application of multimodal neoadjuvant treatment on the basis of such MRI findings has markedly decreased local recurrence rates. However, distant metastasis (including synchronous and metachronous distant metastases) remains a problem in patients with rectal cancer [1].
Clinicopathological factors including TNM staging, lymphovascular invasion (LVI), histological tumour grade and pretreatment serum level of carcinoembryonic antigen (CEA) are widely accepted prognostic factors of rectal cancer [2–4]. A recent published study revealed that positive extramural vascular invasion, high T stage and positive regional lymph node metastasis are significantly associated with a high risk of synchronous distant metastasis [4].
The advent of quantitative MR imaging has facilitated an increased role for imaging in risk stratification. Specifically, dynamic contrast-enhanced magnetic resonance imaging (DCE-MRI) in combination with pharmacokinetic modeling of the contrast agent distribution in malignant tissue can be used to assess tumour microcirculation in vivo and noninvasively [5, 6]. It assesses the extravasation of paramagnetic contrast agents such as gadolinium-chelates and can be applied to organs with little motion such as the rectum [7]. However, to our knowledge, the actual clinical benefit of DCE-MRI to predict synchronous distant metastasis and the prognostic aspects in distant metastatic rectal cancer has not yet been well determined.
Therefore, the purpose of this retrospective study was to explore the correlations between DCE-MRI quantitative parameters and synchronous distant metastasis and the clinicopathological factors in rectal cancers.
Material and methods
Patients
This retrospective study was approved by our institutional review board and the requirement for informed consent was waived. Between September 2013 and December 2014, patients with pathologically confirmed rectal adenocarcinoma at our hospital were screened. Patients who underwent surgery alone after MRI examination were included in the study. Those patients were initially investigated via MRI of the rectum and a CT examination for both local and distant staging, and also followed up with a CT examination of the chest, abdomen and pelvis at 6 months post-diagnosis. Patients with the following criteria were excluded: (a) patients receiving any neoadjuvant treatment; (b) DCE-MRI not included in the MRI of the rectum; (c) patients who were lost to follow-up; or (d) images showing unacceptable distortion due to artefacts from metallic clips around the tumours.
MRI examination
All MRI examinations were performed using a 3.0-Tesla MRI scanner (MAGNETOM TrioTim, Siemens, Erlangen, Germany) with a 16-element pelvic phased-array coil. Non-enhanced MR imaging, including oblique axial T1-weighted 2D turbo spin-echo images (repetition time ms/echo time ms, 722/11; section thickness, 3.0 mm; intersection gap, 0.3 mm; field of view, 25 × 25 cm; and matrix, 384 × 326) and sagittal and oblique axial and oblique coronal T2-weighted 2D turbo spin-echo images (repetition time ms/echo time ms, 4,000/99; section thickness, 3.0 mm; intersection gap, 0.3 mm; field of view, 25 × 25 cm; and matrix, 384 × 326) were performed. Three pre-contrast Vibe 3D gradient-echo images (TR/TE 5.32/1.81, slice thickness, 3.0 mm, field of view, 25 × 25 cm, matrix 256 *161, 36 axial slices) with three different flip angles (5°, 10° and 15°) were acquired for the purpose of T1 mapping. Thereafter the DCE images (repetition time ms/echo time ms, 5.32/1.81; section thickness, 3.0 mm; intersection gap, 0.3 mm; field of view, 25 × 25 cm; and matrix, 256 × 161; number of phases, 25; temporal resolution,12.2 s; and the total imaging time, 5 min 5 s) were obtained. An automated injector system (Stellant MR Injection System, Medrad, Germany) was used to apply the Omniscan (GE HealthCare, 0.5 mmol/ml; Dosage (ml) = weight (kg) × 0.2 ml/kg) by bolus injection with a flow rate of 2.5 ml/s. MRI total acquisition time was around 30 min.
Imaging analysis
Two experienced radiologists with 10 and 4 years of experience, respectively, in abdominal imaging evaluated the data independently, blinded to all clinical information and the reference standard. For DCE-MRI parameter measurements, pharmacokinetic analysis was carried out using non-commercial software, Omnikinetics (GE Healthcare, Shanghai, China) with the two-compartment Extended Tofts model. A fully automated image-based individualised AIF (iAIF) estimation method was used as the AIF estimation method. The parameters including the volume transfer constant between blood plasma and extracellular-extravascular space (EES) (K trans, min-1), rate constant between EES and blood plasma (K ep , min-1) and volume of EES space per unit volume of tissue (V e ) were derived from the entire ROI for each patient. The radiologists manually drew ROIs along contours of the tumour, covering the whole lesion with the exclusion of the necrosis, peripheral fat and blood vessels based on T2-weighted images as a guide. After each ROI placement, colour-coded, pixel-wise, parametric perfusion maps of K trans, K ep and V e were generated with sample patients as shown in Fig. 1 [8].

A 73-year-old man with rectal carcinoma who had liver metastasis at initial staging. (a) On T-2-weighted turbo spin-echo (TSE) axial image, a mass (arrow) was seen. The colour-coded K trans map (b), K ep map (c) and V e map (d) shows mixed red, green and blue colours in the corresponding tumour with a K trans of 0.187 × 10−3 min-1, K ep 1.412 min-1 of and V e of 0.145
Clinicopathological examinations and follow-up
Clinicopathological prognostic factors were derived from the patients’ records including age, plasma carcinoembryonic antigen (CEA) level, T and N stage, and tumour differentiation grade. Pathological T and N stage, tumour differentiation grade and the presence of microscopic LVI were confirmed by a pathologist with 6 years of experience in pathology. The lymph node stage was categorized into negative (no metastasis in regional nodes), positive (including N1: metastasis in 1–3 nodes and N2: metastasis in four or more nodes). Tumour differentiation grade was categorized into three stages (well, moderately and poorly differentiated).
The lung and liver metastasis lesions that were pathologically confirmed either underwent surgery resection or biopsy. Among patients in whom the metastasis lesions were not pathologically confirmed, contrast-enhanced liver MRI or fludeoxyglucose–positron emission tomography/computed tomography (FDG–PET/CT) are used for more precise evaluation. A clinical follow-up of 6 months was undertaken to confirm the final results of distant metastases. Newly detected metastatic lesions within 6 months after the initial diagnosis and those with distant metastases at initial staging were considered synchronous metastasis.
Statistical analysis
Statistical analyses were performed using software (SPSS Statistics for Windows, version 20.0, IBM Corp, Armonk, NY, USA; MedCalc, version 11.5, Mariakerke, Belgium; and R, version 3.1.3). To test the reproducibility of DCE-MRI measurements independently obtained by two observers, intra-class correlation coefficient (ICC) values for the parameters of two DCE-MRI data sets were calculated with a 95 % confidence interval (CI). Differences in DCE-MRI parameters with regard to clinicopathological factors were tested. To compare the variables, the normality and homoscedasticity of the multiparametric data were tested using the Q-Q plots and the Levene tests. Data subjected to normal distribution were subjected to Student’s t test or analysis of variance (ANOVA). Conversely, data not subjected to normal distribution were analysed using the Mann-Whitney U test or Kruskal-Wallis H(K) test. Receiver operating characteristic (ROC) analyses were used to find a reasonable threshold of K trans, K ep and V e to differentiate lesions with synchronous distant metastasis from those without metastasis. For the ROC analyses, the area under the curve (AUC) was calculated and AUCs were compared using nonparametric methods [9] and optimal thresholds were obtained maximising the Youden index [10]. A p value less than 0.05 was considered statistically significant.
Results
Patients
Table 1 summarizes the clinicopathological characteristics. Among 63 enrolled patients, 31 patients were confirmed to have synchronous distant metastases. Among the 31 patients in the synchronous distant metastasis group, 21 were men and ten were women. The mean age was 58.5 years (range: 34–77). The mean tumour length was 4.84 cm (range: 2.32–7.9). The mean age in the non-metastasis group (n = 32; 18 men and 14 women) were 62.61 years (range: 35–78), respectively. The mean tumour length of the non-metastasis group was 4.36 cm (range: 0.8–7.46 cm).
Among the 31 patients in the synchronous distant metastasis group, 26 patients had distant metastases at the time of initial diagnosis and five patients showed newly developed liver metastases within 6 months of surgery. Hepatic metastases were the most common metastases (19 patients, 61.3 %) followed by lung metastases (nine patients, 29.0 %). Three patients (9.7 %) had both liver and lung metastases; distant lymph node metastases and adrenal gland metastases was not observed. Distant metastases were confirmed pathologically by surgery in 18 patients and by sequential radiological follow-up in 13 patients. Among them, five patients underwent FDG–PET/CT, five patients underwent hepatocyte-specific contrast-enhanced liver MRI and three patients underwent both PET/CT and hepatocyte-specific contrast-enhanced liver MRI for more precise evaluation.
The median time interval from MRI to surgery was 7 days (range: 3–27). Patients in the metastasis group received low anterior resection (LAR, n = 21), abdominoperineal resection (APR, n = 8) and extended resection (n = 2). Patients in the non-metastasis group received LAR (n = 19), APR (n = 12) and extended resection (n = 1).
DCE-MRI parameters
Comparison of the DCE-MRI parameters according clinicopathological status is shown in Table 2.
Higher K trans (greater flow and permeability) values from whole transverse ROIs obtained by DCE-MRI were noted among patients with synchronous distant metastasis than those without distant metastasis (p < 0.001). The k ep and V e were also significantly higher in the distant metastases group (p = 0.022 and 0.034, respectively). Figure 2 illustrates the distribution of K trans, K ep and V e values in the synchronous distant metastasis and non-metastasis group.

Boxplots showing K trans, K ep and V e in lesions with and without distant metastasis. K trans (a), K ep (b) and V e (c) were significantly higher in the lesions with distant metastasis than in the lesions without distant metastasis (0.536 ± 0.242 vs. 0.299 ± 0.118 min-1, p < 0.001; 1.598 ± 0.477 vs. 1.341 ± 0.390 min-1, p = 0.022; and 0.324 ± 0.173 vs. 0.249 ± 0.091, p = 0.034, respectively)
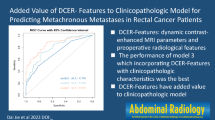
The ROC analysis was used to find the reasonable threshold of K trans, K ep and V e to differentiate lesions with synchronous distant metastasis from those without metastasis (Table 3). The K trans showed the highest AUCs with 0.788 (p < 0.001), with sensitivity of 61.29 % and specificity of 87.5 %, respectively. K trans showed a significantly higher AUC (0.788 vs. 0.645) than V e (p = 0.008). K trans and K ep showed a fair degree of accuracy (p = 0.165), as did K ep and V e (AUC: K ep 0.689, V e 0.645; p = 0.674).
The K trans, K ep and V e values of the pLVI positive group were significantly higher than those of the pLVI negative group (p < 0.001, p = 0.016 and 0.004; respectively) (Fig. 3).

Boxplots showing K trans, K ep and V e in the pLVI-positive and -negative groups. K trans (a), K ep (b) and V e (c) were significantly higher in the pLVI-positive group than the pLVI-negative group (0.562 ± 0.271 vs. 0.343 ± 0.151, p < 0.001; 1.659 ± 0.580 vs .1.372 ± 0.339, p = 0.016; and 0.358 ± 0.204 vs. 0.250 ± 0.078, p = 0.004, respectively)
The K trans and V e correlate with tumour histological grade, the K trans values increased from 0.193 (min-1, well differentiated) to 0.478 (min-1, poorly differentiated). The V e values increased from 0.171 (well differentiated) to 0.326 (poorly differentiated). In addition, a statistically significantly higher V e value was found in CEA ≥ 5 ng/ml group (p = 0.04).
No statistically significant correlations were found for K trans, K ep and V e values in tumours of different histological T and N stage.
In the evaluation of inter-observer agreement for the independent sets of DCE-MRI parameters, ICC values for each parameter showed an almost perfect level of agreement; 0.889 (95 % CI 0.829–0.950) for K trans, 0.862 (95 % CI 0.788–0.937) for K ep and 0.721 (95 % CI 0.581–0.861) for V e .
Discussion
In this study, we evaluated the usefulness of perfusion parameters derived from DCE-MRI for assessing the correlations with synchronous distant metastasis and the clinicopathological factors in rectal cancers. Our results showed that tumours with synchronous distant metastasis had higher K trans and K ep values. Angiogenesis is one of the fundamental factors in the formation of distant metastases [11]. In terms of biological explanations, we would propose that tumours with higher vascular permeability are more adherent to distant metastasis. DCE-MRI parameters K trans correlate with vascular permeability, and hence angiogenesis within tumour tissue. Similarly, higher K ep value represents greater blood return to vasculature. In addition, K ep is only affected by the contrast concentration and fractional volumes in the tumour EES and might thus more accurately reflect the tumour capillary permeability [12]. It is reported that DCE-MRI parameters permit the noninvasive estimation of tumour angiogenesis [5, 13], including rectal cancer [14]. Thus, the correlation between the imaging data and the distant metastases was not unexpected. These results are in line with the findings of other authors [6, 15].
In addition, with respect to the contrast agent exchange constant V e , in our study, V e was significantly higher in synchronous distant metastasis group. It has been shown that the loss of function of cell–cell adhesion molecules, such as e-cadherin, is a crucial step in tumour progression, both regional and metastatic [16–18]. This loss of function leads to a larger interstitial space, which is reflected by a higher V e on DCE-MRI. Our results were in agreement with those of a previous study in glioma [19, 20].
A preoperative CEA level ≥ 5 ng/ml was reported to be associated with the early distant metastasis [21, 22]. Villeneuve et al. [23] suggested that preoperative CEA level ≥ 10 ng/ml was prognostic factor in patients with lung metastasis from colorectal cancer. In our study, significant correlation was also found between CEA level and synchronous distant metastasis (data not show). In addition, a statistically significant higher V e value was found in CEA ≥ 5 ng/ml group (p = 0.04).
Regarding the Davenport et al. [24] investigation, V e seems to be a more robust and reproducible biomarker. However, our findings revealed lower accuracy of V e than K trans to access synchronous distant metastasis. Further research about the correlation between V e and synchronous distant metastasis is deemed necessary.
In our study, correlations were found between the K trans, K ep and V e values and pLVI status. Recent studies demonstrate that there is a significant difference in the incidence of metastatic disease between those with and those without mesorectal vascular invasion in rectal carcinoma [25, 26]. Venous invasion is an independent risk factor for local and distant recurrence and poorer overall survival [27, 28].
We used lymphovascular invasion instead of vascular invasion analysis on the basis of routine staining in this study. However, histopathological LVI may be a different entity from vascular invasion. Histologically, lymphatic vessels and blood vessels are both thin walled and tubular structures surrounded by endothelial cells and it is often not possible to accurately differentiate them without elastic tissue staining. As a result, the term ‘lymphovascular’ is usually used [29]. As the DCE-MRI parameters mainly characterize angiogenesis rather than lymphangiogenesis, the correlation between the imaging data and the vascular invasion should be assessed in future work. MRI-detected extramural vascular invasion (EMVI) is an independent risk factor for distant metastasis in rectal cancer [25, 26]. The comparison of the ability between DCE-MRI parameters and EMVI to predict distant metastasis was not addressed in this study.
The results of this study also imply that perfusion parameters may serve as an effective image-based indicator in the differentiation of tumour histological grade. The poorly differentiated rectal cancer typically presents with hypervascularity accompanied by increased permeability and leakiness. The MR contrast agents (in the present study, the Omniscan) that leak slowly through the intact basement membrane are able to escape more quickly through tumour vessels into the EES.
We are now in an era in which treatment is tailored according to individual risk. Early distant metastasis is associated with poor survival [21]. Control of distant metastasis is presently a major concern for the treatment of locally advanced rectal cancer [1]. Preoperative identification of distant metastasis is especially important for some reasons: first, patients with synchronous metastasis should undergo different treatment, such as neoadjuvant chemotherapy or metastasectomy. Neoadjuvant chemotherapy with a full systemic dose could have the potential to treat micrometastases before they can progress to more advanced and detectable metastases [30]. Some clinical trials including preoperative induction chemotherapy for intense systemic control before standard treatment have been performed [31]. The main targets of this type of clinical trial are patients with the greatest risk of distant metastasis. Our results indicate that DCE-MRI might be helpful to select candidates for associated clinical trials. Second, patients with high-risk findings on MRI could undergo liver-specific contrast-enhanced MRI or FDG–PET to detect hidden metastases. It has been shown that gadoxetic-acid-enhanced MRI at 3-T is significantly more sensitive than 64-row multidetector CT for the detection of small (<10 mm) hepatic metastases [32]. As we found a correlation between DCE-MRI data and the occurrence of synchronous distant metastases, further prospective investigations with more patients and a long-term follow-up are needed to assess the potential of DCE-MRI to predict survival.
There are some limitations in this study. First, we have proven the value of detection of synchronous distant metastasis; however, metachronous metastasis remains an uncertain area. Although prediction of synchronous metastasis has great value for treatment planning, the relapse-free survival of patients with rectal cancer is directly related to metachronous metastasis, rather than synchronous metastasis. Second, in this study, we chose patients who underwent surgery alone. Patients who received any neoadjuvant treatment were excluded for the following reasons: pathological results like tumour T staging, N staging, tumour differentiation grade and lymphovascular invasion may change after the preoperative chemoradiotherapy. Preoperative chemoradiotherapy may induce tumour downstaging or even pathological complete response (pCR) in some patients. Neoadjuvant treatment may influence the results of distant metastasis. This may predispose to selection bias. Third, the relatively small number of subjects and low number of patients with a subgroup of histological T1 stage and histologically well-differentiated grade may limit the applicability of results.
In conclusion, these findings in our study suggest that DCE-MRI data may represent a prognostic indicator for synchronous distant metastases in patients with rectal cancer. We believe that perfusion parameters derived from DCE-MRI might help to identify these high-risk patients before therapy.
Abbreviations
- AUC:
-
Area under the curve
- CEA:
-
Carcinoembryonic antigen
- DCE-MRI:
-
Dynamic contrast-enhanced magnetic resonance imaging
- EES:
-
Extravascular-extracellular space
- k ep :
-
Rate constant from EES to blood plasma (min-1)
- K trans :
-
Volume transfer constant between EES and blood plasma (min-1)
- LVI:
-
Lymphovascular invasion
- ROC:
-
Receiver operating characteristic
- V e :
-
EES volume per unit tissue volume
References
Engelen SM, Maas M, Lahaye MJ, Leijtens JW, van Berlo CL, Jansen RL et al (2013) Modern multidisciplinary treatment of rectal cancer based on staging with magnetic resonance imaging leads to excellent local control, but distant control remains a challenge. Eur J Cancer 49:2311–2320
Meguerditchian AN, Bairati I, Lagace R, Harel F, Kibrite A (2005) Prognostic significance of lymphovascular invasion in surgically cured rectal carcinoma. Am J Surg 189:707–713
Hong HS, Kim SH, Park HJ, Park MS, Kim KW, Kim WH et al (2013) Correlations of dynamic contrast-enhanced magnetic resonance imaging with morphologic, angiogenic, and molecular prognostic factors in rectal cancer. Yonsei Med J 54:123–130
Shihab OC, Moran BJ, Heald RJ, Quirke P, Brown G (2009) MRI staging of low rectal cancer. Eur Radiol 19:643–650
Li L, Wang K, Sun X, Wang K, Sun Y, Zhang G et al (2015) Parameters of dynamic contrast-enhanced MRI as imaging markers for angiogenesis and proliferation in human breast cancer. Med Sci Monit 21:376–382
Lollert A, Junginger T, Schimanski CC, Biesterfeld S, Gockel I, Duber C et al (2014) Rectal cancer: dynamic contrast-enhanced MRI correlates with lymph node status and epidermal growth factor receptor expression. J Magn Reson Imaging 39:1436–1442
Padhani AR (2002) Dynamic contrast-enhanced MRI in clinical oncology: current status and future directions. J Magn Reson Imaging 16:407–422
Tofts PS, Brix G, Buckley DL, Evelhoch JL, Henderson E, Knopp MV et al (1999) Estimating kinetic parameters from dynamic contrast-enhanced T(1)-weighted MRI of a diffusable tracer: standardized quantities and symbols. J Magn Reson Imaging 10:223–232
DeLong ER, DeLong DM, Clarke-Pearson DL (1988) Comparing the areas under two or more correlated receiver operating characteristic curves: a nonparametric approach. Biometrics 44:837–845
Schisterman EF, Perkins NJ, Liu A, Bondell H (2005) Optimal cut-point and its corresponding Youden Index to discriminate individual using pooled blood samples. Epidemiology 16:73–81
Fidler IJ, Ellis LM (1994) The implications of angiogenesis for the biology and therapy of cancer metastasis. Cell 79:185–188
Koo HR, Cho N, Song IC, Kim H, Chang JM, Yi A et al (2012) Correlation of perfusion parameters on dynamic contrast-enhanced MRI with prognostic factors and subtypes of breast cancers. J Magn Reson Imaging 36:145–151
Chen J, Qian T, Zhang H, Wei C, Meng F, Yin H (2016) Combining dynamic contrast enhanced magnetic resonance imaging and microvessel density to assess the angiogenesis after PEI in a rabbit VX2 liver tumor model. Magn Reson Imaging 34:177–182
Yeo DM, Oh SN, Jung CK, Lee MA, Oh ST, Rha SE et al (2015) Correlation of dynamic contrast-enhanced MRI perfusion parameters with angiogenesis and biologic aggressiveness of rectal cancer: preliminary results. J Magn Reson Imaging 41:474–480
Gollub MJ, Cao K, Gultekin DH, Kuk D, Gonen M, Sohn M et al (2013) Prognostic aspects of DCE-MRI in recurrent rectal cancer. Eur Radiol 23:3336–3344
Hanahan D, Weinberg RA (2000) The hallmarks of cancer. Cell 100:57–70
Christofori G, Semb H (1999) The role of the cell-adhesion molecule E-cadherin as a tumour-suppressor gene. Trends Biochem Sci 24:73–76
Herzig M, Savarese F, Novatchkova M, Semb H, Christofori G (2007) Tumor progression induced by the loss of E-cadherin independent of beta-catenin/Tcf-mediated Wnt signaling. Oncogene 26:2290–2298
Awasthi R, Rathore RK, Soni P, Sahoo P, Awasthi A, Husain N et al (2012) Discriminant analysis to classify glioma grading using dynamic contrast-enhanced MRI and immunohistochemical markers. Neuroradiology 54:205–213
Jia Z, Geng D, Xie T, Zhang J, Liu Y (2012) Quantitative analysis of neovascular permeability in glioma by dynamic contrast-enhanced MR imaging. J Clin Neurosci 19:820–823
Huh JW, Kim CH, Lim SW, Kim HR, Kim YJ (2013) Early recurrence in patients undergoing curative surgery for colorectal cancer: is it a predictor for poor overall survival? Int J Colorectal Dis 28:1143–1149
Wang L, Zhong XG, Peng YF, Li ZW, Gu J (2014) Prognostic value of pretreatment level of carcinoembryonic antigen on tumour downstaging and early occurring metastasis in locally advanced rectal cancer following neoadjuvant radiotherapy (30 Gy in 10 fractions). Colorectal Dis 16:33–39
Villeneuve PJ, Sundaresan RS (2009) Surgical management of colorectal lung metastasis. Clin Colon Rectal Surg 22:233–241
Davenport MS, Heye T, Dale BM, Horvath JJ, Breault SR, Feuerlein S et al (2013) Inter- and intra-rater reproducibility of quantitative dynamic contrast enhanced MRI using TWIST perfusion data in a uterine fibroid model. J Magn Reson Imaging 38:329–335
Sohn B, Lim JS, Kim H, Myoung S, Choi J, Kim NK et al (2015) MRI-detected extramural vascular invasion is an independent prognostic factor for synchronous metastasis in patients with rectal cancer. Eur Radiol 25:1347–1355
Kim YC, Kim JK, Kim MJ, Lee JH, Kim YB, Shin SJ (2016) Feasibility of mesorectal vascular invasion in predicting early distant metastasis in patients with stage T3 rectal cancer based on rectal MRI. Eur Radiol 26:297–305
Betge J, Pollheimer MJ, Lindtner RA, Kornprat P, Schlemmer A, Rehak P et al (2012) Intramural and extramural vascular invasion in colorectal cancer: prognostic significance and quality of pathology reporting. Cancer 118:628–638
Gunther K, Dworak O, Remke S, Pfluger R, Merkel S, Hohenberger W et al (2002) Prediction of distant metastases after curative surgery for rectal cancer. J Surg Res 103:68–78
Lim SB, Yu CS, Jang SJ, Kim TW, Kim JH, Kim JC (2010) Prognostic significance of lymphovascular invasion in sporadic colorectal cancer. Dis Colon Rectum 53:377–384
Glynne-Jones R, Anyamene N, Moran B, Harrison M (2012) Neoadjuvant chemotherapy in MRI-staged high-risk rectal cancer in addition to or as an alternative to preoperative chemoradiation? Ann Oncol 23:2517–2526
Chua YJ, Barbachano Y, Cunningham D, Oates JR, Brown G, Wotherspoon A et al (2010) Neoadjuvant capecitabine and oxaliplatin before chemoradiotherapy and total mesorectal excision in MRI-defined poor-risk rectal cancer: a phase 2 trial. Lancet Oncol 11:241–248
Scharitzer M, Ba-Ssalamah A, Ringl H, Kolblinger C, Grunberger T, Weber M et al (2013) Preoperative evaluation of colorectal liver metastases: comparison between gadoxetic acid-enhanced 3.0-T MRI and contrast-enhanced MDCT with histopathological correlation. Eur Radiol 23:2187–2196
Acknowledgements
The scientific guarantor of this publication is Hai-Bin Shi. The authors of this manuscript declare no relationships with any companies whose products or services may be related to the subject matter of the article. The authors state that this work has not received any funding. No complex statistical methods were necessary for this paper. Institutional Review Board approval was obtained. Written informed consent was waived by the Institutional Review Board. Methodology: retrospective, observational, performed at one institution.
Author information
Authors and Affiliations
Corresponding author
Additional information
Jing Yu and Qing Xu contributed equally to this work.
Rights and permissions
About this article

Cite this article
Yu, J., Xu, Q., Huang, DY. et al. Prognostic aspects of dynamic contrast-enhanced magnetic resonance imaging in synchronous distant metastatic rectal cancer. Eur Radiol 27, 1840–1847 (2017). https://doi.org/10.1007/s00330-016-4532-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00330-016-4532-y