
Abstract
Ankylosing spondylitis quality of life (ASQoL) is an instrument for assessing quality of life (QoL). The aims of this study were to assess the reliability of Persian version of ASQoL questionnaire and evaluation of QoL status and related factors in ankylosing spondylitis (AS). One hundred and sixty-three Iranian patients with AS who fulfilled modified New York criteria were enrolled. Patients were evaluated using questionnaires including demographic and clinical variables, Bath AS Disease Activity Index (BASDAI), Bath AS Functional Index (BASFI), fatigue, Bath AS Metrology Index, pain and ASQoL. Reliability and validity of Persian version of ASQoL were evaluated by test–re-test agreement, internal consistency and correlation with specific scales. Relationship of parameters with ASQoL was analyzed by multiple regression. Age, disease duration and ASQoL score (mean ± SD) were 37.74 ± 9.88, 14.49 ± 8.47 and 8.02 ± 5.28 years, respectively. Test–re-test reproducibility for ASQoL was good as assessed by intra-class correlation coefficient (ICC: 0.97, P < 0.001). Internal consistency was high (Cronbach’s alpha: 0.91). Convergent validity was confirmed by correlation of ASQoL score with specific scales (BASFI, r = 0.74, BASDAI, r = 0.6, fatigue, r = 0.56, depression, r = 0.24, intermalleolar distance, r = −0.44 and educational level, r = −0.37). Persian version of ASQoL is a valid and reliable scale to assess QoL in AS. Function, fatigue, mood, hip mobility and education are the factors which should be noted to achieve the best QoL.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Among the spondyloarthropathies, ankylosing spondylitis (AS) is a common chronic rheumatic disease. It affects mainly sacroiliac joint and spine with ascending pattern. Several characteristics including peripheral arthritis, enthesitis, extra-articular manifestations and associated morbidities are among the features in these patients [1–5]. Negative impact on functional status, quality of life (QoL), chronic disability, requiring help at work or withdrawing the job, and harmful effects regarding national healthcare and non-health care costs are the main outcomes of this disease in different populations [6, 7]. QoL assessed by ankylosing spondylitis quality of life (ASQoL) has been recognized as one of the representatives for the health status of AS patients. Furthermore, it has been described as one of the instruments for assessing the disease outcome and severity in these patients [8]. Particularly, it is a disease-specific scale to measure the effect of AS on health-related QoL from the patient’s perception [8]. This instrument was first introduced in 2003 for AS and includes 18 items related to different aspects of QoL. QoL level and knowledge about related factors may help rheumatologists, physicians, health and social workers to plan for strategies such as lifestyle modification, medications and educational programs to improve patients’ conditions.
Ankylosing spondylitis quality of life is a simple, rapid, reliable and valid scale for evaluating the impact of AS on different aspects of QoL including pain, stiffness, fatigue, mood, physical function and limitations in daily activities [8]. A reliable and valid Persian version of ASQoL may eliminate the effect of cross-cultural differences in items interpretation of ASQoL and help the health managers to assess the QoL of Iranian AS patients more precisely. Furthermore, knowledge about factors affecting the ASQoL and targeting these factors throughout clinical management may improve the health status and QoL of patients. Therefore, the primary objectives of this study were to assess the reliability and some validity aspects of the Persian version of ASQoL. The secondary objectives were to assess the QoL status and determine the more frequently affected aspects of QoL in Iranian AS patients.
Methods
Study population
One hundred and sixty-three patients with AS were consecutively enrolled into a cross-sectional study at the Iranian AS association, Iran Rheumatology Center and Rheumatology Clinic of Shariati Hospital (a tertiary hospital related to Tehran University of Medical Sciences) in Iran. All patients with the age of 16 and over, who fulfilled the modified New York criteria 1984 for diagnosis of AS and were interested to participate in the survey, were included in the study [9]. Patients with concomitant severe medical disorders at the time of study were not included. Informed consent compatible with the most recent version of the Helsinki Declaration was obtained from patients, and the survey was approved by ethics committee of Tehran University of Medical Sciences. Diagnosis of AS was confirmed by a qualified rheumatologist before enrolling.
A structured questionnaire was applied to collect the demographic and disease-related data and also co-morbidities. Disease activity was measured by BASDAI (from 0, no activity, to 10, maximum activity) [10, 11]. Spinal and hip mobility was assessed by BASMI (from 0, the best mobility, to 10, the worst mobility) [12]. Functional status was measured by BASFI (from 0, the best function, to 10, the worst function) [11, 13]. Fatigue was assessed by BASDAI-question 1 and visual analog scale 0–10. Morning stiffness was assessed by BASDAI-question 5 and visual analog scale 0–10. Nocturnal back pain and total back pain in last week were assessed by visual analog scale 0–10 [14]. Sacroiliitis grading (grade 2, 3 or 4) was assessed by standard sacroiliac radiography [9]. Depression was diagnosed by psychiatrist. HLA-B*27 status was evaluated by polymerase chain reaction with sequence-specific primer (PCR-SSP) and Olerup SSP™ HLA*B27 kit (Hasselstigen, Sweden). QoL was considered as a dependent variable and assessed by Persian version of self-administered ASQoL. ASQoL is a composition index made up of 18 items with dichotomous responses (yes = 1, no = 0) for each item [8]. The score range is 0–18, and the higher scores indicate the worse QoL. Ninety patients were asked to recomplete the ASQoL questionnaire, 48 h later (to the asssessments at the clinic), and send it back by prepaid mail. The feasibility, validity and reliability of Persian version of ASQOL were evaluated. All measurements were done in the afternoon, and physical measurements such as BASMI, finger-to-floor distance (cm), modified Shober (cm), chest expansion (cm), intermalleolar distance (cm), tragus-to-wall distance (cm), cervical rotation (degree), determining decrease in cervical slope, increase in thoracic kyphosis and decrease in lumbar lordosis were carried out by the same rheumatologist for measurement uniformity.
Translation of questionnaire
The original English version of ASQoL questionnaire was translated into Persian language by two Iranian physicians, considering cultural adaptation. Both translations were reviewed and combined into one by two rheumatologists. Afterward, the patients were interviewed to make sure that they understand all items and respond correctly. Back-translation to English was made by a linguist, and the last version was compared to the original version. Both seemed to be nearly identical. For Persian version of ASQoL, see supplement files.
Statistical analysis
SPSS for windows (version 18) was used for all statistical analysis. For presenting the continuous variables, mean ± standard deviation (SD) and for categorical variables, frequency (%) were used. Intra-class correlation coefficient (ICC) was used for test–re-test (on two occasions with 48-h interval) agreement and reliability of ASQoL. Internal consistency of ASQoL was measured by Cronbach’s alpha. Convergent validity was ascertained by evaluating the correlation of ASQoL with other disease-specific measurement instruments including BASMI, BASDAI and BASFI. Feasibility was evaluated by the time length for completing the ASQoL questionnaire and also the number of items without answer. Univariate analysis with simple linear regression model was used for evaluating the parameters which may influence ASQoL (supplement files). Only, the factors which were associated with ASQoL with P value equal to or less than 0.05 were included in a multivariate analysis (multiple linear regression) to determine the parameters which affect the ASQoL, independently. Cohen’s guidelines were also used for showing the strongest correlation with ASQoL. For comparing continuous variables, Mann–Whitney-U test and for comparing ASQoL scores on two occasions in test–re-test analysis, Wilcoxon signed ranks test were used. Spearman-rank correlation coefficient (r) was also applied to assess the correlations. A two-tailed P value less than 0.05 was considered significant in all analyses.
Results
Of the one hundred and sixty-three enrolled patients, 122 individuals (74.8 %) were HLA-B*27 positive with male/female ratio of 3.79. The age of patients at the time of study was 37.74 ± 9.88 (range 18–65) years, and disease duration was 14.49 ± 8.47 (range 1–44) years. Other demographic and clinical features of the patients are shown in Tables 1, 2. Good internal consistency between 18 items of ASQoL questionnaire filled by 163 AS patients was confirmed by Cronbach’s alpha: 0.91. The positive responses to 18 items of ASQoL are shown in Table 3. Of the 163 studied patients, ninety patients were asked to re-complete the ASQoL questionnaire, 48 h later (to the assessments at the clinic), and send it back by prepaid mail. Fifty-four individuals (60 %) sent back the completed questionnaires. Test–re-test analysis of ASQoL questionnaire (on two occasions with 48 h interval) in 54 patients showed good agreement and reproducibility (ICC = 0.97, P < 0.001). There was no significant differences between ASQol score at the two occasions (8.33 ± 5.13 and 8.33 ± 5.66, respectively, P = 0.42).
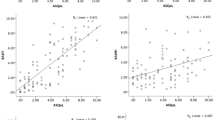
Correlation of ASQoL with BASFI, BASDAI, BASMI and other clinical and outcome measures are shown in Table 4. Among the clinical measurement scales, the strongest correlation of ASQoL was seen with BASFI (ρ = 0.74, P < 0.001) (Table 4). ASQoL score was significantly higher in patients with BASDAI ≥ 4 compared with BASDAI < 4 (10.16 ± 4.95 vs. 5.19 ± 4.29, respectively, P < 0.001). ASQoL score was also significantly higher in patients with BASFI > 5 compared with BASFI ≤ 5 (11.90 ± 4.33 vs. 5.32 ± 4.06, P < 0.001).
The time length for completing the ASQoL questionnaire by patients varied from 2 to 6 min, and all of the patients fully completed the questionnaire without missing answer.
Factors affected the ASQoL
Univariate analyses with simple linear regression model revealed the variables which significantly affected the ASQoL score (supplement files). The following variables were included: educational level, pack-years of smoking, age at diagnosis, nephrolithiasis, history of enthesitis and peripheral arthritis, chest expansion, finger-to-floor distance (cm), modified Schober (cm), tragus-to-wall distance (cm), intermalleolar distance (cm), cervical rotation (degrees, measured by goniometry), nocturnal back pain, total back pain, loss of lumbar lordosis, increase in thoracic kyphosis, decrease in cervical slope, BASMI, BASDAI, BASFI scores, fatigue and depression. Afterward, these variables were included into a multiple linear regression model with backward method. The final model revealed the parameters which affected the ASQoL score, independently (Table 5). No significant relationship was observed between ASQoL score and extra-articular manifestations in simple linear regression models (P > 0.05). However, nephrolithiasis was an exception among the extra-articular manifestations as significant association was observed between nephrolithiasis and higher ASQoL scores (P < 0.05). Also, significant relationship was not found between ASQoL score and other demographic and clinical variables including gender, age at disease onset, disease duration, body mass index (BMI) (kg/m2), physical activity level, occupational status (employed or unemployed), family history of AS, drug history and associated morbidities (diabetes mellitus, hyperthyroidism, hypertension and other cardiovascular disorders) (P > 0.05).
Discussion
Good agreement in test–re-test analysis of ASQoL, good internal consistency between ASQoL items and also significant correlation with other clinical measures confirmed the good reproducibility and validity for the provided Persian version of ASQoL questionnaire.
Comparing the ASQoL score of patients with AS in the current study (Iran) with other parts of the world revealed nearly the same QoL status for patients in Turkey and China [15, 16], the poorer QoL in United Kingdom, Tunisia and France [8, 17, 18], and higher QoL in Netherland, Canada, Australia and Spain [8, 19, 20]. Probable role of ethnicity and dissimilarities regarding the other demographic, psychosocial and clinical factors, sampling and also genetic polymorphisms can elucidate these variations.
In the current study, those ASQoL items which were influenced more frequently included the following: Condition gets me down, pain at all times, tired easily and feel like crying. According to our results, the most frequently affected aspects of QoL were observed in physical function, pain, fatigue and mood (depression). This result was partially similar to Zhao et al. [16] study in China and Haywood et al. [21] study in England and Scotland. In the study in China, fatigue, pain and depression got the highest scores, and in second study, fatigue, pain and physical function received the worst scores. ASQoL score as a QoL scale was also measured by Bodur et al. [22] and Yilmaz et al. [15] in Turkey. However, in both studies, the aspects which had the poorest status, obtained from SF-36 subscale scores and not from 18 items of ASQoL. The worst scores in the former study were seen in general health, physical role, bodily pain and vitality and in the latter survey were observed in general health and then physical role, emotional role and bodily pain, respectively. In present survey, several factors were found to influence ASQoL score. However, after controlling the effect of confounders, only BASFI, fatigue, depression, intermalleolar distance and educational level were found to have significant independent relationship with ASQoL. Compatible with our findings, ASQol was significantly correlated with disease duration, BASDAI, BASFI, BASMI, fatigue and pain in Bodur et al. study [22]. In their survey, QoL was worse in patients with lower educational status and smokers versus patients with higher educational status and non-smokers. QoL between patients with and without extra-articular manifestations (uveitis, IBD and mucocutaneous features) were not significantly different (similar to our study). Furthermore, a positive effect on QoL was observed in patients with regular exercise habit. Unfortunately, evaluating the influence of regular exercise was not possible in our study since exercise performance was not in a regular style in our patients. The results of Yilmaz et al. [15] study were also similar to our survey. They noted the significant correlation of ASQoL with BASDAI, BASFI, BASMI, total pain, night pain, fatigue, morning stiffness and erythrocyte sedimentation rate (ESR). Also, patients with peripheral arthritis obtained higher ASQoL scores compared with patients without peripheral joint involvement. Zhao et al. [16] showed significant correlation of ASQoL with BASFI, pain, BASDAI, BAS-G (Bath AS global score), ESR, BASMI and C-reactive protein (CRP). By considering the interaction of the clinical and laboratory measures and controlling the effect of confounders, BASFI persisted as the only significant factor which affected the ASQoL in their studies. In both Yilmaz et al. and Bodur et al. studies, BASDAI ranked the first among the related variables with ASQoL. Dissimilar to their studies, BASFI was the strongest parameter which affected the ASQoL in our survey and also Zhao et al. study (using Cohen’s guidelines). Moreover, it should be noted that dissimilar to the current study, the probable effect of confounding variables was not considered in Yilmaz et al. and Bodur et al. surveys.
Gordeev et al. [19] carried out a study to evaluate the role of contextual factors in health-related QoL of AS disease. In their investigation, the worse QoL was reported by the unemployed patients and also the patients who perceived more helplessness. Helplessness is a psychological status in which patients suppose that their efforts are unsuccessful to control the disease. Haywood et al. [21] also revealed the lower ASQoL score (better QoL) in employed patients versus unemployed ones. Conversely, no significant relationship was found between employment and ASQoL in our survey. Variations in the culture, familial support, age, disease duration and several other factors between the patients in present survey and other studies may have a role to elucidate this difference.
The limitations of this study were the lack of spinal radiographic assessment (Bath AS Radiological Index: BASRI) and laboratory evaluations (ESR and CRP). Due to the cross-sectional design of the study, directionality of the influences between quality of life and some of the investigated parameters was not explored definitely, which may explain the need to design a follow-up study in future. Psychological status including helplessness has been shown in previous studies that may influence the QoL [19]. Unfortunately, with the exception of depression, other psychological states were not accounted in the present study. However, assessing the influence of several clinical and demographical parameters and efforts to control the effect of probable confounding variables are among the advantages of current survey.
In conclusion, the results of current study revealed that the Persian version of ASQoL was a short, valid and reliable specific disease measurement scale which was feasible and easy to use for evaluation of disease outcome in AS. The most frequently affected aspects of health-related QoL (measured by ASQoL) in Iranian patients with AS were physical function, pain, fatigue and depression. Also, current study elucidated that health-related QoL was much more affected by BASFI, fatigue, depression, hip mobility (measured by intermalleolar distance) and educational level. Therefore, management strategies should be planned and focused more on (1) decreasing the fatigue and depression and (2) increasing the functional level (BASFI), hip mobility and educational level. To achieve better quality of life, efforts should be applied to improve physical function, pain, fatigue and psychological aspects of ASQoL.
References
Bodur H, Ataman S, Buğdaycı DS, Rezvani A, Nas K, Uzunca K et al (2012) Description of the registry of patients with ankylosing spondylitis in Turkey: TRASD-IP. Rheumatol Int 32(1):169–176. doi:10.1007/s00296-010-1599-7
Tayel MY, Soliman E, EI Baz WF, EI Labaan A, Hamaad Y, Ahmed MH (2012) Registry of the clinical characteristics of spondyloarthritis in a cohort of Egyptain population. Rheumatol Int 32(9):2837–2842. doi:10.1007/s00296-011-2068-7
Benegas M, Muñoz-Gomariz E, Font P, Burgos-Vargas R, Chaves J, Palleiro D et al (2012) Comparison of the clinical expression of patients with ankylosing spondylitis from Europe and Latin America. J Rheumatol 39(12):2315–2320. doi:10.3899/jrheum.110687
Collantes E, Zarco P, Muñoz E, Juanola X, Mulero J, Fernández-Sueiro JL et al (2007) Disease pattern of spondyloarthropathies in Spain: description of the first national registry (REGISPONSER) extended report. Rheumatology (Oxford) 46(8):1309–1315
Fallahi S, Jamshidi AR, Gharibdoost F, Mahmoudi M, Paragomi P, Nicknam MH et al (2012) Urolithiasis in ankylosing spondylitis: correlation with bath ankylosing spondylitis disease activity index (BASDAI), bath ankylosing spondylitis functional index (BASFI) and bath ankylosing spondylitis metrology index (BASMI). Caspian J Intern Med 3(4):508–513
Zhu TY, Tam LS, Lee VW, Hwang WW, Li TK, Lee KK et al (2008) Costs and quality of life of patients with ankylosing spondylitis in Hong Kong. Rheumatology (Oxford) 47(9):1422–1425. doi:10.1093/rheumatology/ken287
Boonen A, van der Heijde D, Landewé R, Guillemin F, Spoorenberg A, Schouten H et al (2003) Costs of ankylosing spondylitis in three European countries: the patient’s perspective. Ann Rheum Dis 62(8):741–747. doi:10.1136/ard.62.8.741
Doward LC, Spoorenberg A, Cook SA, Whalley D, Helliwell PS, Kay LJ et al (2003) Development of the ASQOL: a quality of life instrument specific to ankylosing spondylitis. Ann Rheum Dis 62(1):20–26. doi:10.1136/ard.62.1.20
van der Linden S, Valkenburg HA, Cats A (1984) Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum 27(4):361–368
Garret S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Callin A (1994) A new approach to defining disease status in ankylosing spondylitis: the bath ankylosing spondylitis disease activity index. J Rheumatol 21(12):2286–2291
Bidad K, Fallahi S, Mahmoudi M, Jamshidi A, Farhadi E, Meysamie A et al (2012) Evaluation of the Iranian versions of the bath ankylosing spondylitis disease activity index (BASDAI), the bath ankylosing spondylitis functional index (BASFI) and the patient acceptable symptom state (PASS) in patients with ankylosing spondylitis. Rheumatol Int 32(11):3613–3618. doi:10.1007/s00296-011-2186-2
Jenkinson TR, Mallorie PA, Whitelock HC, Kennedy LG, Garrett SL, Callin A (1994) Defining spinal mobility in ankylosing spondylitis (AS). The bath AS metrology index. J Rheumatol 21(9):1694–1698
Calin A, Garrett S, Whitelock H, Kennedy LG, O’Hea J, Mallorie P et al (1994) A new approach to defining functional ability in ankylosing spondylitis: the development of the bath ankylosing spondylitis functional index. J Rheumatol 21(12):2281–2285
Sieper J, Rudwaleit M, Baraliakos X, Brandt J, Braun J, Burgos-Vargas R et al (2009) The assessment of spondyloarhritis international society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rheum Dis 68(Suppl 2):ii1–ii44. doi:10.1136/ard.2008.104018
Yilmaz O, Tutoğlu A, Garip Y, Ozcan E, Bodur H (2012) Health-related quality of life in Turkish patients with Ankylosing spondylitis: impact of peripheral involvement on quality of life in terms of disease activity, functional status, severity of pain, and social and emotional functioning. Rheumatol Int. doi:10.1007/s00296-012-2510-5
Zhao LK, Liao ZT, Li CH, Li TW, Wu J, Lin Q et al (2007) Evaluation of quality of life using ASQoL questionnaire in patients with ankylosing spondylitis in a Chinese population. Rheumatol Int 27(7):605–611. doi:10.1007/s00296-006-0267-4
Hamdi W, Haouel M, Ghannouchi MM, Mansour A, Kchir MM (2012) Validation of the ankylosing spondylitis quality of life questionnaire in Tunisian language. Tunis Med 90(7):564–570 Article in French
Pham T, van der Heijde DM, Pouchot J, Guillemin F (2010) Development and validation of the French ASQoL questionnaire. Clin Exp Rheumatol 28(3):379–385
Gordeev VS, Maksymowich WP, Evers SM, Ament A, Schachna L, Boonen A (2010) Role of contextual factors in health-related quality of life in ankylosing spondylitis. Ann Rheum Dis 69(1):108–112. doi:10.1136/ard.2008.100164
Ariza–Ariza R, Hernández-Cruz B, López-Antequera G, Toyos FJ, Navarro-Sarabia F (2006) Cross-cultural adaptation and validation of a Spanish version of a specific instrument to measure health-related quality of life in patients with ankylosing spondylitis. Reumatol Clin 2(2):64–69. doi:10.1016/S1699-258X(06)73024-8 [Article in Spanish]
Haywood KLM, Garratt A, Jordan K, Dziedzic K, Dawes PT (2002) Disease-specific, patient-assessed measures of health outcome in ankylosing spondylitis: reliability, validity and responsiveness. Rheumatology (Oxford) 41(11):1295–1302
Bodur H, Ataman S, Rezvani A, Buğdayci DS, Cevik R, Birtane M et al (2011) Quality of life and related variables in patients with ankylosing spondylitis. Qual Life Res 20(4):543–549. doi:10.1007/s11136-010-9771-9
Acknowledgments
The authors gratefully appreciate all patients who participated and cooperated in this study. This survey was a part of the research project which was supported and funded by Rheumatology Research Center, Tehran University of Medical Sciences (code: 89-03-41-11076).
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article
Cite this article
Fallahi, S., Jamshidi, A.R., Bidad, K. et al. Evaluating the reliability of Persian version of ankylosing spondylitis quality of life (ASQoL) questionnaire and related clinical and demographic parameters in patients with ankylosing spondylitis. Rheumatol Int 34, 803–809 (2014). https://doi.org/10.1007/s00296-013-2888-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-013-2888-8