
Abstract
The objective of this study was to investigate the effects of Pilates on pain, functional status, and quality of life in patients with ankylosing spondylitis. The study was performed as a randomized, prospective, controlled, and single-blind trial. Fifty-five participants (30 men, 25 women) who were under a regular follow-up protocol in our Rheumatology Clinic with the diagnosis of AS according to the modified New York criteria were included in the study. The participants were randomly assigned into two groups: in group I, Pilates exercise program of 1 h was given by a certified trainer to 30 participants 3 times a week for 12 weeks, and in group II, designed as the control group, 25 participants continued previous standard treatment programs. In groups, pre-(week 0) and post treatment (week 12 and week 24) evaluation was performed by one of the authors who was blind to the group allocation. Primary outcome measure was functional capacity. Evaluation was done using the Bath Ankylosing Spondylitis Functional Index (BASFI). Exploratory outcome measures were Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Metrology Index (BASMI), Chest expansion, and ankylosing spondylitis quality of life (ASQOL) questionnaire. In group I, BASFI showed significant improvement at week 12 (P = 0.031) and week 24 (P = 0.007). In group II, this parameter was not found to have significantly changed at week 12 and week 24. Comparison of the groups showed significantly superior results for group I at week 24 (P = 0.023). We suggest Pilates exercises as an effective and safe method to improve physical capacity in AS patients. Our study is the first clinical study designed to investigate the role of Pilates method in AS treatment. We believe that further research with more participants and longer follow-up periods could help assess the therapeutic value of this popular physical exercise method in AS.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a chronic, inflammatory disorder characterized by pain and stiffness of the back and the sacroiliac joints [1]. Pain, reduced spine mobility, and decreased physical functioning are the major manifestations of AS. The basic goal of AS therapy should focus on reducing pain and morning stiffness, preventing skeletal deformity and maintaining correct posture, physical condition, and psychosocial health [2]. While pharmacological agents such as non-steroidal anti-inflammatory drugs (NSAID) and sulfasalazine have been traditionally used with varying therapeutic efficiency, the TNF antagonists, introduced and popularized more recently, have been a true milestone in AS treatment by reducing spinal inflammation and significantly improving quality of life as well as relieving pain [3, 4]. However, medical therapy alone has never been considered sufficient in clinical management of AS patients without physical therapy or exercise [5–8]. Exercise is known to contribute substantially to AS treatment by preserving spinal flexibility, preventing postural deformities, improving muscle strength, and reducing pain [6, 7]. “The importance of exercise in AS has been emphasized in the ASAS/EULAR (Assessment of SpondyloArthritis international Society/European League Against Rheumatism) recommendations for the management of AS [1] where exercise therapy is included in the 10 recommendations.” While there is consensus on the role of exercise in AS treatment, the review of the literature reveals that strict and precise guidelines with regard to the type and frequency of the exercises have not been delineated yet. In a recent review of six different physiotherapy interventions for AS reported during the last 5 years, one of the most striking conclusions was the importance of including core exercises in the modalities to preserve or enhance spinal mobility [9].
The Pilates body conditioning method, which was developed by Joseph H. Pilates during the First World War and enhanced and refined over the next 50 years, contains over 500 stretching and strengthening exercises [10]. Joseph Pilates believed that all muscles of the body should be strengthened and stretched, with the major emphasis placed upon the muscles of the center, or core, of the body, which he referred to as the powerhouse of the body [11].
While Pilates exercises mostly take place in training programs designated for healthy people as part of general fitness programs, it has recently been suggested as a therapeutic modality for several musculoskeletal disorders [12, 13]. La Touch et al. [14] have reported in a recent review that there were two randomized controlled trials and one clinical controlled trial studying the effects of Pilates on low back pain. Positive results have been reported in chronic low back pain (LBP) patients who enrolled in Pilates training programs in these studies [14, 15]. The positive results were attributed to the specific training applied to the core (abdomen and back) musculature and the resultant increase in the spinal resilience and improved mobility in the joints. All researchers studying the clinical effects of Pilates agreed that additional research in Pilates was necessary. In a study performed in our clinic, we observed improvement of quality of life and pain relief in Fibromyalgia syndrome (FMS) patients who were given a course of supervised Pilates exercises for a period of 3 months [16].
The purpose of this study is to investigate the effect of Pilates method on improving the functional capacity as a primarily goal and also secondarily on disease activity, spinal mobility, and quality of life of AS patients by stretching and strengthening the body core muscles.
Participants and method
A total of 55 participants (30 men, 25 women) who were under a regular follow-up protocol in our Rheumatology Clinic with the diagnosis of AS according to the modified New York criteria were included in the study. Their ages ranged between 28 and 69 (mean: 45.23 ± 10.73) and the duration of disease was 2–22 years (mean: 8.84).
None of the patients had any systemic problem contra-indicating exercising. Patients who had active peripheral arthritis, total spinal ankylosis, ESR over 50 mm/h, or CRP more than 10 times the normal value were excluded. The patients whose treatment regimens were changed during the last 2 months prior to the study were not included. The patients were allowed to continue their previous medication. However, they were requested not to use supplementary drugs or change the usual dosages throughout the study period, and for a more accurate pain assessment, they were asked not to take any pain killers in the morning of the assessment day. The participants were fully informed about the nature and purpose of the study and an informed consent was obtained from each of them. Approval by the local ethic committee for the study was obtained.
Treatment protocol
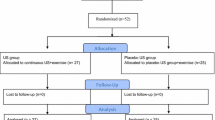
The participants were assigned randomly into two groups using random number table by the researcher other than the one who performed the evaluation throughout the study.
In group I, Pilates exercise program of 1 h was given by a certified trainer to 30 participants 3 times a week for 12 weeks. Exercise program followed the basic principles of Pilates method but particularly movements with low and medium difficulty levels were chosen to adapt the program to the physical capacity of the patients. Our protocol comprised 9 modules: postural education, search for neutral position, sitting exercise, antalgic exercises, stretching exercises, proprioceptivity improvement exercises, and breathing education. Resistance bands and 26 cm Pilates balls were used as supportive equipment.
In group II, designed as the control group, 25 participants continued previous standard treatment programs. The patients in the control group received usual care and were instructed to continue participating in their usual physical activity.
Pilates exercise was stopped at the end of the 12 week, and all participants were reevaluated at the end of the 24 week following the period of 12 weeks free from exercise.
Evaluation parameters
Evaluations were performed just before (week 0), immediately after (week 12), and 12 weeks following the treatment (week 24) by the same researcher who was totally unaware of the groups the participants belonged to, and all participants were requested not to give information to the examiner about their treatment protocol.
Primary outcome measure
Functional capacity
Evaluation was done using the Bath Ankylosing Spondylitis Functional Index (BASFI) for which the adaptation to the native language of the patients has been shown to be valid and reliable [17].
The BASFI is a set of 10 questions designed to determine the degree of functional limitation in people with AS. The participants were asked to indicate their level of ability with each of the activities during the past week on a horizontal 10 cm line (easy-to-impossible). BASFI score was calculated by dividing the sum of the scores obtained from 10 questions by 10 [18].
Exploratory outcome measures
Disease activity
Evaluation was done using the Bath Ankylosing Spondylitis Disease Activity Index (BASDAI) comprising a set of 6 questions for which the adaptation to the native language of the patients has been shown to be valid and reliable [19, 20]. This questionnaire includes the entire spectrum of AS symptoms related to fatigue, pain, swelling, and morning stiffness. The patients responded to each item indicating a point on the 10 cm line considering their status during the last week only. Since the items 5 and 6 were both related to morning stiffness, the average score was first calculated between them and then added to the scores of the first 4 items. The final average score, a value between 0 and 10, was found by dividing the total sum by 5.
Spinal mobility
Bath Ankylosing Spondylitis Metrology Index (BASMI), which was developed to assess spinal mobility in AS patients, was used [21]. BASMI index was obtained by measuring cervical rotation, tragus to wall distance, lumbar side flexion, modified Schober’s, intermalleolar distance, and scoring the limitations for each criterion between 0 and 2. Total score changed between 0 and 10.
Chest expansion
Chest expansion, which is a parameter not included in BASMI, was evaluated separately by measuring the increase in chest circumference at the level of the fourth intercostal after maximum inspiration following previous forced expiration.
Health quality
ASQOL (Ankylosing spondylitis quality of life) is a questionnaire specific for AS patients [22]. It has 18 questions to which the patients are asked to respond as yes or no depending on which answer applies best to them at the moment. All item scores are summed to give a total score or index which may range from 0 (good QoL) to 18 (poor QoL).
Statistical analysis
We did all statistical calculations under the supervision of the staff biostatistician using the SPSS 16.0 program. We tested the normality of the parameters by Shapiro–Wilk test. We used Wilcoxon test for the intra-group comparisons and T test and Mann–Whitney U test for comparisons between the groups after calculating the percent changes for measured values and the difference scores for overall score values. Categorical variables were compared using chi-square test and Fischer’s exact test. Any P value less than 0.05 was considered significant.
Results
One participant in group I was excluded from the study after he complained from increased back pain and 1 patient in group II was excluded since he failed to come for control evaluations. Evaluation was done in the remaining 53 participants. Table 1 shows data for age and week 0 values for the evaluation parameters in both groups. Pre treatment data showed no significant difference between two groups for any parameter.
Thirty-one percent of the patients received NSAID, 32% sulfasalazine, and 21% biological agent treatment regularly, while 17% percent did not use regular medication. Distribution of the patients according to medications did not show a significant difference between the groups (P > 0.05).
Primary outcome measure
In group I, BASFI showed significant improvement at week12 (P = 0.031) and week 24 (P = 0.007). In group II, this parameter was not found to have significantly changed at week 12 and week 24 (Table 2). Comparison of the groups showed significantly superior results for group I at week 24 (P = 0.023) (Table 3).
Exploratory outcome measures
In group I, BASMI, BASDAI, and chest expansion showed significant improvement (P = 0.005, P = 0.036, P = 0.002), while there was no significant change for ASQoL at week 12. In group II, no significant change was observed at week 12. Evaluations at week 24 showed improvement compared with week 0 only for BASMI in group I (P = 0.009) and worsening for BASDAI in group II while there was no significant change for other parameters in either group. (i.e., the parameters returned toward the baseline state of week 0).
Comparison of the two groups on the basis of the post treatment (both week 12 and week 24) percent changes and difference scores relative to pre treatment (week 0) values showed a significant difference for BASDAI at 12 week (P = 0.003) and BASMI at 24 week (P = 0.013) in favor of group I.
Discussion
The results of our study showed improvement for a period of up to 6 months in functional capacity, the primary outcome of the study, in AS patients who were given a course of Pilates exercises while no change in functional capacity was observed in the control group. Comparison of these two groups showed significant improvement in Pilates group at 24 week, but no statistically significant difference between the two groups at 12 week, suggesting that the beneficial effect of Pilates exercises has been evident in the longer term.
Functional capacity is known to decrease gradually in AS patients since the disease affects the joints of the spinal and peripheral joints such as the shoulder, hip, knee, and ankle [23]. Inflammation of the spinal and extraspinal joints and enthesis are evident even in the early stages of AS and this condition frequently leads to ankylosis of the vertebrae and severe limitation of spinal mobility. Importance of regular exercise programs supplementing medical therapy for improvement in functional capacity has been previously emphasized, and several studies investigating therapeutic effect of various exercise methods in AS patients have been reported [24–31]. Ince et al. [24] found a multimodal program of aerobic, stretching, and pulmonary exercises was superior to the control group without any physiotherapy in spinal mobility, work capacity, and chest expansion. Kraag et al. [28] compared the effectiveness of a group exercise program of 4 months and home therapy. They stated that there was a significant decrease in fingertip-to-floor distance in the study group, but no significant difference in pain, occiput-to-wall distances, and morning stiffness duration between the groups. Hidding et al. [30] compared the effectiveness of group and individualized therapies and reported that group therapy had more positive impact on global health and function, but did not provide a significant improvement in spinal mobility. Analay et al. [31] reported significant improvement in BASFI in the supervised exercise group in a study where they compared a standard home program group with an intensive exercise program under the supervision of a physiotherapist. On the other hand, in a more recent study, Karapolat et al. [28] failed to observe significant improvement in BASFI in either group (group-based exercise versus home-based exercise), while they obtained significantly positive results for BASDAI, BASMI, and pain, energy level, sleep, and emotional reaction parameters of Nottingham health profile in both groups. As a result, they suggested that home programs could be effective as well, easier to apply, and less expensive.
Whereas swimming is frequently recommended as a daily exercise for AS patients, we could find only one related study in the literature [32]. In this study, the patients were given a conventional exercise program in one group, conventional exercise plus swimming in another group, and conventional plus walking exercises in the last group. None of these groups showed improved functional capacity according to BASFI, while significant improvement in chest expansion (CE) was obtained in the swimming group. The researchers attributed their results to the lower BASFI scores compared with those of the other studies. Here, we should note that our study gave significantly better results with Pilates although the average BASFI scores were also relatively low.
According to Fernandez-de-Las-Penas et al. [33], not all exercises are beneficial for AS. They proposed the “global posture reeducation” (GPR), which is a physical therapy method dealing with the existence of different muscle chains that work in synergist function, may be effective for AS patients. At the end of their program, they found significantly better results for improvement in BASFI, BASDAI, and BASMI in the GPR group compared with the control group where only standard flexibility and pulmonary exercises were employed. The review of the literature on the role of exercise in AS treatment has suggested that further research is necessary to establish standardized and effective exercise programs [7–9].
Pilates, which has been gaining in popularity over the last decade, is a mind–body exercise intervention that addresses both the physical and mental aspects of pain with core strengthening, flexibility, and relaxation [10, 11, 34]. Pilates method gives precedence to the spine and focuses on controlled movement, posture, and breathing, which are obviously the basic goals of AS treatment [35]. Joseph Pilates believed that a stiff spine made people feel older and even if the limbs were fine, they would not function desirably unless one could comfortably control or move the spine, the center core of the body [36].
The increase in functional capacity observed in our study might have been obtained as a result of this specific focus of Pilates on the muscles supporting the spine [37]. Increased flexibility is thought to have led to improvement in BASFI scores by enabling the patients to perform better in movements such as unassisted sock-wearing, reaching upward, and bending forward that provided overall improvement in functional capacity [38, 39]. The essence of the Pilates technique is to strengthen and lengthen the body simultaneously while exerting complete control over it. You stretch the spine using the abdominal muscles and, conversely, stretch the abdominals using the muscles of the back. The hamstrings are stretched using the buttock muscles and buttocks using the hamstrings and so on. This sequential “dynamic stretching” has proven to be a safe and functional way to increase the flexibility [36].
While the functional capacity was the primary outcome of our study, we also employed the BASDAI scale to assess the role of Pilates on the disease activity of the patients as a secondary outcome. BASDAI scores showed improvement in the Pilates group immediately after the program but were not significantly different from pre treatment values at 24 week, while an increase in BASDAI scores were observed in the control group at 24 week compared with the pre treatment values. The negative result in the latter may be speculated to have been due to the possible negative effect of the awareness of the patients of the non-treatment group they belonged to. Improvement in BASDAI in the Pilates group may be attributed to the positive effect of Pilates on pain and fatigue. In a previous study, we observed these latter beneficial effects of Pilates in patients with fibromyalgia syndrome [16]. However, failure to observe sustained improvement 12 weeks after cessation of the exercise program obviously suggests that these patients should be given this exercise program regularly and continuously, corroborating our observation in FMS study where similar results were obtained in the long-term evaluations.
We also compared the BASMI scores in order to investigate more objectively the effect of Pilates exercises on restriction of joint range of motion (ROM) in addition to evaluation of the overall function assessed with BASFI. Our results showed significantly improved ROM in the Pilates group both at 12 and 24 weeks compared with pre treatment values and at 24 weeks compared with the control group.
Diminished chest expansion developing secondary to involvement of thoracic vertebrae and inflammation of the costovertebral, costosternal, and manubriosternal joints observed in AS patients results in restrictive respiratory failure that may present a challenging problem in AS treatment [40]. Since chest expansion (CE) is not included in BASMI parameters, we separately employed exploratory outcome CE in order to assess respiratory effect of Pilates. We observed significant improvement in chest expansion in Pilates patients immediately after the program. This finding is not unexpected since special emphasis has been made on correct and conscious breathing in the theory of Pilates and constant breath control accompanying and aiding the movements is an integral part of this method [36, 41]. However, comparison of the results in the two groups at 24 weeks showed that the improvement in respiration was not maintained in the longer term, suggesting longer exercise periods are necessary to observe more lasting positive results for chest expansion.
Decreased daily activity and quality of life may be observed in AS patients as a result of pain and emotional factors as well as functional limitations. The effect of Pilates on the quality of life was assessed using ASQoL which is a specific questionnaire for AS, and the results showed no significant improvement in quality of life of the patients in either Pilates or control group. However, it would not be realistic to expect better results in quality of life that depends on several factors such as pain, stiffness, sleep disorders, social isolation, and emotional problems with a relatively short period of exercise program particularly in an early onset chronic rheumatoid disease such as AS. The effect of exercise on AS has been addressed in a number of studies where generic quality scales such as health assessment questionnaire and Nottingham health profile were employed. Positive results for subscores of energy, pain, and emotional reaction of Nottingham health profile were reported in these studies [28, 42]. Since we could not find any study using ASQoL for the evaluation of quality of life in AS patients, we cannot compare our results with those of others for this parameter.
Compliance of the patients with the program has been at a high level with only one patient from each group quitting the study and no record of an inadvertent effect of the exercises except for one patient in Pilates group who complained of increased back pain at the end of the first month and was excluded. The MRI of the latter patient did not show any acute pathology and his pain was relieved by an analgesic treatment protocol in 2 weeks.
Before the conclusion, we must mention some limitations of our study model. First and the foremost limitation is the failure to design a study model where Pilates would be the sole therapeutic modality owing to the ethical principles which would not permit interruption of the ongoing medication of the patients. However, only the patients who had been given the same regimen for the last 2 months were included, and the regimen of each patient was kept unchanged during the study period. Relatively small participant number and short follow-up period may also be noted as the other limitation of the study.
In the light of the results of our study, we suggest Pilates exercises as an effective and safe method to improve physical capacity in AS patients. Our study is the first clinical study designed to investigate the role of Pilates method in AS treatment. We believe that further research with more participants and longer follow-up periods could help assess the therapeutic value of this popular physical exercise method in AS.
References
Zochling J, van der Heijde D, Burgos-Vargas R, Collantes E, Davis JC Jr, Dijkmans B, Dougados M, Géher P, Inman RD, Khan MA, Kvien TK, Leirisalo-Repo M, Olivieri I, Pavelka K, Sieper J, Stucki G, Sturrock RD, van der Linden S, Wendling D, Böhm H, van Royen BJ, Braun J (2006) ‘ASsessment in AS’ international working group; European League Against Rheumatism. ASAS/EULAR recommendations for the management of ankylosing spondylitis. Ann Rheum Dis 65:442–452
Dougados M, Dijkmans B, Khan M, Maksymowych W, van der Linden S, Brandt J (2002) Conventional treatments for ankylosing spondylitis. Ann Rheum Dis 61(Suppl III):40–50
Chen J, Liu C (2006) Is sulfasalazine effective in ankylosing spondylitis? A systematic review of randomized controlled trials. J Rheumatol 33:722–731
Reed MR, Taylor AL (2008) Tumour necrosis factor inhibitors in ankylosing spondylitis. Intern Med J 38:781–789
Zochling J (2008) Assessment and treatment of ankylosing spondylitis: current status and future directions. Curr Opin Rheumatol 20:398–403
van Tubergen A, Hidding A (2002) Spa and exercise treatment in ankylosing spondylitis: fact or fancy? Best Pract Res Clin Rheumatol 16:653–666
Dagfinrud H, Kvien TK, Hagen KB, Nghiem FT, Donohue JP (2008) Physiotherapy interventions for ankylosing spondylitis. Cochrane Database Syst Rev 23(1):CD002822
Elyan M, Khan MA (2008) Does physical therapy still have a place in the treatment of ankylosing spondylitis? Curr Opin Rheumatol 20:282–286
Nghiem FT, Donohue JP (2008) Rehabilitation in ankylosing spondylitis. Curr Opin Rheumatol 20:203–207
Friedman P, Eisen G (eds) (2005) The pilates method of Physical and mental conditioning, 10th edn. Penguin books ltd., London, England
Muscolino JE, Cipriani S (2004) Pilates and the ‘‘powerhouse’’I. J Bodyw Mov Ther 8:15–24
Levine B, Kaplanek B, Scafura D, Jaffe WL (2007) Rehabilitation after total hip and knee arthroplasty: a new regimen using Pilates training. Bull NYU Hosp Jt Dis 65:120–125
Blum CL (2002) Chiropractic and pilates therapy for the treatment of adult scoliosis. J Manipulative Physiol Ther 25:E3
La Touche R, Escalante K, Linares MT (2008) Treating non-specific chronic low back pain through the Pilates method. J Bodyw Mov Ther 12:364–370
Donzelli S, Di Domenica E, Cova AM, Galletti R, Giunta N (2006) Two different techniques in the rehabilitation treatment of low back pain: a randomized controlled trial. Eura Medicophys 42:205–210
Altan L, Korkmaz N, Bingol U, Gunay B (2009) Effect of pilates training on people with fibromyalgia syndrome: a pilot study. Arch Phys Med Rehabil 90:1983–1988
Yanik B, Gürsel YK, Kutlay S, Ay S, Elhan AH (2005) Adaptation of the Bath Ankylosing Spondylitis Functional Index to the Turkish population, its reliability and validity: functional assessment in AS. Clin Rheumatol 24:41–47
Calin A, Garrett S, Whitelock H, Kennedy LG, O’Hea J, Mallorie P, Jenkinson T (1994) A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J Rheumatol 21:2281–2285
Garrett S, Jenkinson T, Kennedy LG, Whitelock H, Gaisford P, Calin A (1994) A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol 21:2286–2291
Akkoc Y, Karatepe AG, Akar S, Kirazli Y, Akkoc N (2005) A Turkish version of the Bath Ankylosing Spondylitis Disease Activity Index: reliability and validity. Rheumatol Int 25:280–284
Jones SD, Porter J, Garrett SL, Kennedy LG, Whitelock H, Calin A (1995) A new scoring system for the Bath Ankylosing Spondylitis Metrology Index (BASMI). J Rheumatol 22:1609
Doward LC, Spoorenberg A, Cook SA, Whalley D, Helliwell PS, Kay LJ, McKenna SP, Tennant A, van der Heijde D, Chamberlain MA (2003) Development of the ASQoL: a quality of life instrument specific to ankylosing spondylitis. Ann Rheum Dis 62:20–26
Bostan EE, Borman P, Bodur H, Barça N (2003) Functional disability and quality of life in patients with ankylosing spondylitis. Rheumatol Int 23:121–126
Ince G, Sarpel T, Durgun B, Erdogan S (2006) Effects of a multimodal exercise program for people with ankylosing spondylitis. Phys Ther 86:924–935
Karapolat H, Akkoc Y, Sari I, Eyigor S, Akar S, Kirazli Y, Akkoc N (2008) Comparison of group-based exercise versus home-based exercise in patients with ankylosing spondylitis: effects on Bath Ankylosing Spondylitis Indices, quality of life and depression. Clin Rheumatol 27:695–700
Ortancil O, Sarikaya S, Sapmaz P, Basaran A, Ozdolap S (2009) The effect(s) of a six-week home-based exercise program on the respiratory muscle and functional status in ankylosing spondylitis. J Clin Rheumatol 15:68–70
Lim HJ, Moon YI, Lee MS (2005) Effects of home-based daily exercise therapy on joint mobility, daily activity, pain, and depression in patients with ankylosing spondylitis. Rheumatol Int 25:225–229
Karapolat H, Akkoc Y, Sari I, Eyigor S, Akar S, Kirazli Y, Akkoc N (2008) Comparison of group-based exercise versus home-based exercise in patients with ankylosing spondylitis: effects on Bath Ankylosing Spondylitis Indices, quality of life and depression. Clin Rheumatol 27:695–700
Kraag G, Stokes B, Groh J, Helewa A, Goldsmith CH (1994) The effects of comprehensive home physiotherapy and supervision on patients with ankylosing spondylitis -an 8-month followup. J Rheumatol 21:261–263
Hidding A, van der Linden S, Boers M, Gielen X, de Witte L, Kester A, Dijkmans B, Moolenburgh D (1993) Is group physical therapy superior to individualized therapy in ankylosing spondylitis? A randomized controlled trial. Arthritis Care Res 6:117–125
Analay Y, Ozcan E, Karan A, Diracoglu D, Aydin R (2003) The effectiveness of intensive group exercise on patients with ankylosing spondylitis. Clin Rehabil 17:631–636
Karapolat H, Eyigor S, Zoghi M, Akkoc Y, Kirazli Y, Keser G (2009) Are swimming or aerobic exercise better than conventional exercise in ankylosing spondylitis patients? A randomized controlled study. Eur J Phys Rehabil Med 45:449–457
Fernández-de-Las-Peñas C, Alonso-Blanco C, Morales-Cabezas M, Miangolarra-Page JC (2005) Two exercise interventions for the management of patients with ankylosing spondylitis: a randomized controlled trial. Am J Phys Med Rehabil 84:407–419
Segal NA, Hein J, Basford JR (2004) The effects of Pilates training on flexibility and body composition: an observational study. Arch Phys Med Rehabil 85:1977–1981
Sekendiz B, Altun O, Korkusuz F, Akın S (2007) Effects of Pilates exercise on trunk strength, endurance and flexibility in sedentary adult females. J Bodyw Mov Ther 11:318–326
Robinson L, Bass M (eds) (2005) Classic pilates method, Pan Books. Pan Macmillan, London
Herrington L, Davies R (2005) The influence of Pilates training on the ability to contract the Transversus Abdominis muscle in asymptomatic individuals. J Bodyw Mov Ther 9:52–57
Johnson EG, Larsen A, Wilson CA, MPT, Kennedy KL (2007) The effects of Pilates-based exercise balance in healthy adults. J Bodyw Mov Ther 11:238–242
Curnow D, Cobbin D, Wyndham J, Boris Choy ST (2009) Altered motor control, posture and the Pilates method of exercise prescription. J Bodyw Mov Ther 13:104–111
Sampaio-Barros PD, Cerqueira EM, Rezende SM, Maeda L, Conde RA, Zanardi VA, Bértolo MB, de Menezes Neto JR, Samara AM (2007) Pulmonary involvement in ankylosing spondylitis. Clin Rheumatol 26:225–230
Latey P (2002) Updating the principles of the Pilates method. J Bodyw Mov Ther 6:94–101
Kucukdeveci AA, McKenna SP, Kutlay S, Gürsel Y, Whalley D, Arasil T (2000) The development and psychometric assessment of the Turkish version of the Nottingham Health Profile. Int J Rehabil Res 23:31–38
Conflict of interest
There is no conflict of interest affecting the authors.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Altan, L., Korkmaz, N., Dizdar, M. et al. Effect of Pilates training on people with ankylosing spondylitis. Rheumatol Int 32, 2093–2099 (2012). https://doi.org/10.1007/s00296-011-1932-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-011-1932-9