
Abstract
The aim of our study was to evaluate effectiveness of ultrasound treatment applied with exercise therapy in patients with ankylosing spondylitis. Fifty-two patients, who were diagnosed according to modified New York criteria, were aged 25–60, and have spine pain, were randomly assigned to two groups. Ultrasound (US) and exercise therapy were applied to treatment group (27); placebo US treatment and exercise therapy were applied to control group (25). Patients were evaluated before treatment, at the end of treatment, and 4 weeks after the treatment. Daily and night pain, morning stiffness, patient global assessment (PGA), doctor global assessment (DGA), Bath Ankylosing Spondylitis Disease Activity Index (BASDAI), Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Metrology Index (BASMI), Ankylosing Spondylitis Quality of Life (ASQoL) questionnaire, Ankylosing Spondylitis Disease Activity Score (ASDAS) erythrocyte sedimentation rate (ESR), and ASDAS C-reactive protein (CRP) were used as clinical parameters. In US group, all parameters showed significant improvements at 2 and 6 weeks, in comparison with the baseline. In placebo US group, significant improvement was obtained for all parameters (except tragus-to-wall distance and modified Schober test at 2 weeks and lumbar side flexion and modified Schober test at 6 weeks). Comparison of the groups showed significantly superior results of US group for parameters of BASMI (p < 0.05), tragus–wall distance (p < 0.05), PGA (p < 0.01), and DGA (p < 0.05) at 2 weeks as well as for the parameters of daily pain (p < 0.01), PGA (p < 0.05), DGA (p < 0.01), BASDAI (p < 0.05), ASDAS-CRP (p < 0.05), ASDAS-ESR (p < 0.01), lumbar side flexion (p < 0.01), the modified Schober test (p < 0.01), and ASQoL (p < 0.05) at 6 weeks. Our study showed that ultrasound treatment increases the effect of exercise in patients with ankylosing spondylitis.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a widespread chronic inflammatory rheumatic disease manifested by inflammatory back pain [1]. The disease is a major subtype and a main outcome of an inter-related group of spondylarthritis [2]. Inflammatory back pain, asymmetrical peripheral oligoarthritis (predominantly of the lower limbs), enthesitis, and specific organ involvement such as anterior uveitis, psoriasis, and chronic inflammatory bowel disease are clinical features of this group [1].
Besides pain, bone bridgings and syndesmophytes in spine also cause consisting severe limitations in the coming period of patients with AS. Ankylosis of spine affects the daily life activities adversely, which results in functional failure and diminishing workforce participation.
The main purposes of the AS treatment are to reduce symptoms of pain, stiffness, and fatigue, to restore and maintain correct posture, to provide physical and psychosocial functionality, and to improve long-term health-related quality of life [3].
The most appropriate treatment of AS patients is a combination of pharmacological and non-pharmacological methods [4, 5]. Physical therapy and exercise are significant part of the non-pharmacological treatment. There are many studies showing that exercise treatment is beneficial [6, 7]. The number of studies showing the effectiveness of physical therapy modalities in AS is limited [8, 9].
Therapeutic ultrasound is among the commonly used physical modalities for treating musculoskeletal disorders [10]. US’s degree of clinical benefit as a physical therapy treatment remains uncertain [11, 12]. Thermal effects of US are thought to cause changes in nerve conduction velocity, an increase in enzymatic activity, and changes in contractile activity of skeletal muscles as well as an increase in collagen tissue extensibility, an increase in local blood flow, and an increase in pain threshold, reducing muscle spasm [13]. Non-thermal effects of US are due to alteration of cell membrane activity, vascular wall permeability, and facilitation of soft tissue healing [14].
In the only study so far that examines the efficacy of US treatment on AS patients, 30 patients were randomly divided into two groups called medical treatment (MT) group and the physical therapy (PT) group [8]. MT group received medical and exercise treatment, while the PT group additionally was treated with physical therapy agents (US and infrared). A total of 20 sessions, each of which consisted of infrared radiation for 30 min and 1.5 watt/cm2 US for 10–20 min, were applied to the paravertebral muscles in PT group. Both groups received an exercise program consisting of respiratory, postural, and stretching exercises, once a day, for 30 min. Quality of life was evaluated by SF-36 and Nottingham Health Profile (NHP); emotional status was evaluated by Beck Depression Scale (BDS). Comparison of the two groups showed significantly superior results for PT group in terms of pain during rest, movement, and night, SF-36, NHP, and BDS. Researchers suggested the use of physical therapy agents in the treatment of AS due to improvements achieved not only on pain but also on life quality and emotional status. Despite common use in clinical practice, the literature investigating the effects of US in AS patients is lacking [8]. The aim of this study was to investigate the effect of US treatment when added to exercise therapy on pain, morning stiffness, disease activity, function, spinal mobility, and quality of life in patients with AS.
Materials and methods
A randomized, prospective, double-blind, placebo-controlled trial was conducted. Patients aged between 25 and 60 years who fulfilled the modified New York criteria for AS with a moderate degree of spinal pain assessment score of ≥4 on Numerical Rating Scale (NRS; 0–10 scale) were elected for participation in the study. This study included fifty-two patients matching those criteria. They were under the regular follow-up protocol in our outpatient clinic. Exclusion criteria were the presence of malignancy, systemic problems, infection, and pregnancy. Furthermore, patients who had received TNF inhibitors, corticosteroids injection for sacroiliac joint in the previous 12 weeks, any physical modalities for spinal area in the previous 12 weeks, and/or any disease-modifying anti-rheumatic drug with a change in dosage in the previous 6 months were excluded. Detailed blood analysis was performed. The study was approved by the Human Research Ethics Committee. The patients were informed about the aim and nature of the study. Informed consent was obtained from all patients prior to inclusion in the study.
Treatment protocol
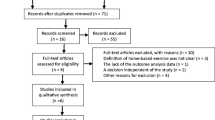
The study protocol was a randomized, placebo-controlled, double-blind design. A total of 52 patients were randomly assigned to two groups. The patients in US group (n = 27) received continuous US using 5 cm2 head US device (Enraf–Nonius Sonopuls 434) (frequency 1 MHz, intensity 1.5 watt/cm2, duration 15 min), and placebo US group (n = 25) received placebo US with an inactive probe. The therapy was applied to the patients for ten sessions (i.e., working days of following 2 weeks) (Fig. 1). The physiotherapist applied US with slow circular movements using the transducer head over the both sides of the paravertebral cervical, thoracal, lumbar spine for 5 min to each part. The physiotherapist moved the applicator at the same rate and pressure as for the placebo US group keeping the appliance off. The physician and the patients did not know that which patients received US or placebo US during the study. US was not consistently applied to the same area in both treatment and placebo groups. The physiotherapist applied US with slow circular movements, using the transducer head over the both sides of the paravertebral cervical, thoracal, lumbar spine. Therefore, there was a little increase in heat in both groups. Heat increase difference between the groups was barely recognizable, so the blinding was maintained. Both groups were given instructions on the exercise program which contained postural exercises; back-strengthening exercises of the cervical, thoracic, and lumbar spine; and stretching of the erector spine muscle, hamstring muscles, pelvic muscles, and breathing exercises.

Flow diagram of participation and withdrawals for patients in ultrasound and placebo ultrasound groups
Patients did the exercises five times a week for 30 min under supervision of the therapist who also applied US during the treatment for 2 weeks. After US treatment was completed, home exercise programs were given. These home exercise programs included identical exercises for all patients. Same physiotherapist showed exercise program. Patients were requested to repeat the exercises individually, five times a week for 30 min throughout 4 weeks after the US treatment.
Randomization
Randomization was done by a computer-generated list of numbers, and group allocation was concealed. An independent person who was blinded to the research protocol and not otherwise involved in the trial operated the random assignment.
Evaluation parameters
The ASAS working group has developed patient-centered disease activity, functional disability, and quality of life assessment instruments for AS called core set. The assessment instruments have found widespread use for clinical record keeping and assessment of response to the treatment [15]. In our study, assessments were performed in three stages: First, at the beginning of the treatment then immediately after the treatment (2 weeks following the beginning of the treatment) and finally 6 weeks after the beginning of the treatment (4 weeks after the end of the treatment), all by a physician who was blinded to the patients according to core set.
Outcome measures
Both groups were evaluated for pain (daily and night), stiffness, PGA, DGA with Numerical Rating Scale (NRS) (0–10) (the patient normally suffered during the week immediately prior to answering the questions). The disease activity was assessed by BASDAI (0–10), ASDAS-CRP, and ASDAS-ESR. The functional status of patients with AS was assessed by the BASFI (0–10). The spinal mobility of AS patients was assessed by the BASMI (0–2) and chest expansion. BASMI includes intermalleolar distance, modified Schober, tragus-to-wall distance, cervical rotation, and lumbar lateral flexion. Besides total BASMI score, scores belonging to each component of BASMI were also compared between the groups. ASQoL (0–18) is used to evaluate the quality of life of patients with AS. Turkish validity and reliability studies were conducted for all these questionnaires [16–18].
Medications of patients were not changed during the study. All patients were using nonsteroidal anti-inflammatory drugs (NSAID). The patients in both groups were informed about the disease and significant points that they should consider in daily life as an AS patient.
Statistical analysis
Number Cruncher Statistical System (NCSS) 2007, Power Analysis and Sample Size (PASS) 2008, and Statistical Software (Utah, USA) were used for statistical analysis. Student t test software was used in evaluating the study data for comparing statistical methods (average, standard deviation, median, frequency, and ratio) alongside quantitative data and parameters that show normal distribution. Mann–Whitney U test was used in the comparison of two groups that do not show normal distribution. Repeated-measures ANOVA (repeated-measures analysis of variance) was used for intragroup examination of normally distributed variables, while adjusted Bonferroni test was used in post hoc comparisons. Friedman test and Wilcoxon signed-rank test were used in non-normally distributed variables of intragroup evaluations. Yates continuity test was used in the comparison of qualitative data. Significance was evaluated at p < 0.05 level.
Results
Pretreatment data showed no significant difference between the two groups in the demographic characteristics, medication, disease duration, and sick leave (Table 1). Also pretreatment data showed no significant difference between the two groups in evaluation parameters except chest expansion, BASFI, and CRP level (Table 2). In US group, all parameters showed significant improvements at 2 and 6 weeks, in comparison with the beginning of the treatment (Table 2). In placebo US group, significant improvement was obtained for all parameters (except tragus-to-wall distance and modified Schober test at 2 weeks, and lumbar side flexion and modified Schober test at 6 weeks) (Table 2).
Comparison of the groups showed significantly superior results of US group for parameters of BASMI, tragus-to wall distance, PGA, and DGA at 2 weeks, as well as for the parameters of daily pain, PGA, DGA, BASDAI, ASDAS-CRP, ASDAS-ESR, lumbar side flexion, the modified Schober test, and ASQoL at 6 weeks (Table 3). In both groups, there were no significant differences in CRP and ESR levels at 2 and 6 weeks compared to pretreatment. No side effects and no complications of either treatment protocol were observed.
Discussion
Results of our study showed that more significant improvement was obtained in AS patients to whom US was conducted to spinal area together with exercise than patients in control group for pain at daytime, disease activity, lumbar mobility, and quality of life.
There are many studies that demonstrate the positive effects of US in other painful musculoskeletal diseases. Ebadi et al. conducted a study in 50 patients with chronic low back pain (CLBP) who were randomly assigned to two groups. Semi-supervised exercises were given to both groups, while the intervention group received continuous US and the control group received placebo US totally for 10 sessions three times a week. Significantly better improvement in Functional Rating Index was reported in the US group [19].
In another study, 59 patients with CLBP were randomized into three groups. Group I received an electrical stimulation (ES) program and exercise treatment, group II received an US treatment and exercise treatment, while group III received only exercise treatment. They found that US and ES treatments have a positive impact on pain, isometric strengthening of the extensor muscle group, and quality of life in patients with CLBP in comparison with the control group [20].
In our study, US group similarly had significantly superior results in decrease of spinal pain at 6 weeks. US rises thermal molecular motion resulting in a tissue temperature increase. That leads to changes in nerve conduction velocity, a rise in pain threshold, an increase in the flexibility of tissue collagen and local blood flow, and a decrease in muscular spasm [13, 21]. It has been shown that allogenic substances leave the affected area with vasodilatory effect of heat. Heat leads to muscle relaxation with reflex stimulation of type Ib fibers and Golgi tendon organs, reducing efferent gamma-muscular activity. Analgesic effect occurs indirectly as a result of reduced muscle tone. Thermoreceptors, which transmit the message proximally to the dorsal horn and may also inhibit transmission of the painful stimulus according to the gate control theory, are stimulated by the heat [22]. Non-thermal effects of US are cavitation and microflows which change the permeability of the cell membrane and accelerate soft tissue healing [23]. Morrisette et al. showed that continuous application of US at 1 MHz of 1.5 or 2 W/cm2 generates sufficient heat in lumbar periarticular tissues to induce theoretical therapeutic effects (i.e., pain reduction, stiffness reduction of the tissue healing, collagen elasticity change) of US [24]. Therefore, we applied the US treatment in the frequency and intensity (1 Hz, 1.5 W/cm2) reported to be efficient. In the study of Sari, 30 patients were randomly divided into medical (MT) and the physical therapy (PT) groups. MT group received medical and exercise treatment, while the PT group was additionally treated with physical therapy agents (US and infrared). Both groups received exercise programs which contained respiratory, postural, and stretching exercises, once a day, for 30 min. Comparison of the two groups showed significantly superior results for PT group in parameters of pain, SF-36, NHP, and BDS [8]. In our study, infrared radiation was not used. There are not many studies in the literature showing that US is effective for rheumatoid arthritis [25]. In one of those studies, 50 patients were randomly divided into US and placebo US groups. US was applied in water to the dorsal and palmar aspects of the hand (frequency undetermined, intensity 0.5 watts/cm2, duration 10 min) continuously using a circular round head. The treatment regimen lasted 3 weeks, for a total of ten sessions. Results showed notably significant increase in grip strength in the treatment group compared with placebo, expressed as weighted mean difference. Significantly better results were achieved in the US group in terms of wrist dorsal flexion, duration of morning stiffness, number of swollen joints, and number of painful joints. No statistically significant difference was found between the groups in terms of decrease in proximal interphalangeal circumference. No harmful side effects were reported [26]. A significant recovery in pain, disease activity, mobility, and quality of life was found in the US group compared with the placebo US group in our study. We did not find statistically significant difference between groups in duration of morning stiffness.
There are also studies indicating that US is not efficient. In a review by Ebadi et al. [11], authors determined that there was not any high-quality evidence supporting US’s effect in improving pain or quality of life in patients with non-specific chronic LBP. In another review, authors concluded that US’s effect is only based on empirical experience and there are no well-designed controlled studies proving such effect. On the other hand, they bring forward the question whether US treatment may enhance the effect of exercise therapy in musculoskeletal disorders [12].
In another study showing the efficacy of physical therapy modalities in the treatment of AS, the patients in group I (n = 19) received low-level laser therapy (LLLT) (1.2 J, 30 mW) and group II (n = 18) received placebo laser with an inactive probe for 10 sessions. There was no statistical difference between groups in terms of VAS at rest and during movements, morning stiffness, PGA, BASDAI, BASFI, and ASQoL scores in pretreatment, second and eighth weeks [9].
Exercise therapy has been shown to be effective in the management of AS patients [27–31]. In a study by Lim et al., 50 patients were assigned into two groups: first group received exercise program, 30 min per day for 8 weeks and the control group did not receive any treatment. Significant improvement in VAS pain, fingertip-to-floor distance (FFD), and BASFI was achieved in the exercise group when compared to the control group [27]. Uhren et al. evaluated exercise and changes in health status in patients with AS. They concluded that exercise reduces stiffness, pain, and increases function [29]. Sweeney et al. compared the effect of a 6-month home-based exercise therapy with a non-intervention control group. Significant difference was found in favor of the exercise group for pain. However, they reported no difference in BASDAI and BASFI [30]. In the study of Kraag which included 53 AS patients divided into two groups, treatment group received a 4-month home exercise program and disease information, while the other group received no treatment. The educational program was not described, but the treatment objectives were disease education, pain control, and improved posture and function. Following the 4-month intervention period, a significant improvement was observed in the treatment group for mobility and physical function. No significant differences between the groups were found for VAS pain [31].
In our study, placebo US group showed significant improvement for all parameters (except for tragus-to-wall distance and modified Schober test at 2 weeks, and lumbar side flexion and modified Schober test at 6 weeks). We observed that exercise therapy given together with US is more useful than sole exercise therapy with regard to pain, PGA, disease activity, lumbar mobility, and quality of life. Although there was a difference in baseline CRP, BASFI, and chest expansion scores between the groups, no difference was present in baseline BASMI scores and in most other parameters (pain, morning stiffness, BASDAI, and ASDAS) related to inflammation and disease activity. We interpreted that this difference in baseline did not affect results of our study.
In a study investigating the efficacy of balneotherapy in patients with AS, 60 patients were randomly assigned to two groups. Group I received balneotherapy and exercise program and patients in group II received only the same exercise program. Balneotherapy was reported to improve the disease activity and functional parameters in AS patients over a relatively short period; its positive effects were not found to be significantly superior to exercise alone in the medium term [32].
A comprehensive review presented that an individual home-based or supervised exercise program produces better results in treatment of AS compared to no intervention, while supervised group physiotherapy produces better results than home exercises. Furthermore, combined inpatient spa–exercise therapy conducted after group physiotherapy was observed to produce better results than group physiotherapy alone [6].
In conclusion, application of continuous US treatment with exercise therapy resulted in significant recovery in terms of pain, stiffness, lumbar mobility, disease activity, and quality of life in patients with AS. US group had no significant benefits when compared to placebo group in terms of night pain, morning stiffness, BASFI, BASMI, chest expansion, tragus-to-wall distance, cervical rotation, and intermalleolar distance at 6 weeks.
Therapeutic US can be used as a safe and effective physical treatment modality in the management of patients with AS. US itself is a low-cost treatment method. However, duration of treatment, which is 10 days, may impose an indirect cost, due to loss of productivity and transport costs, etc. Further long-term studies are needed to evaluate cost-effectiveness of adding US treatment to exercise therapy. Also long-term observation with larger samples is required to investigate the long-term efficacy.
References
Braun J, Sieper J (2007) Ankylosing spondylitis. Lancet 369:1379–1390
Van Der Linden S, Baeten D, Maksymowygh WP (2013) Ankylosing spondylitis. In: Firestein GS (ed) Kelley’s textbook of rheumatology, 9th edn. Elsevier Science, Philadelphia, pp 1202–1220
Zochling J, van der Heijde D, Burgos-Vargas R et al (2006) ASAS/EULAR recommendations for the management of ankylosing spondylitis. Ann Rheum Dis 65:442–452. doi:10.1136/ard.2005.041137
Braun J, van den Berg R, Baraliakos X et al (2011) 2010 update of the ASAS/EULAR recommendations for the management of ankylosing spondylitis. Ann Rheum Dis 70:896–904. doi:10.1136/ard.2011.151027
Braun J, Sieper J (2004) Biological therapies in the spondyloarthritides—the current state. Rheumatology (Oxford) 43:1072–1084. doi:10.1093/rheumatology/keh205
Dagfinrud H, Hagen KB, Kvien TK (2008) Physiotherapy interventions for ankylosing spondylitis. Cochrane Database Syst Rev 23:CD002822. doi:10.1002/14651858.CD002822.pub3
Altan L, Korkmaz N, Dizdar M, Yurtkuran M (2012) Effect of Pilates training on people with ankylosing spondylitis. Rheumatol Int 32:2093–2099. doi:10.1007/s00296-011-1932-9
Sari H, Cakmak B, Can G (2003) Impact of physical therapy agents on quality of life and emotional status in ankylosing spondylitis. Turk J Phys Med Rehab 49:8–12
Aydın E, Gunduz OH, Akcan E, Akyuz G (2013) Effectiveness of low level laser therapy on pain and functional status in ankylosing spondylitis. Turk J Phys Med Rehab 59:299–303. doi:10.4274/tftr.23255
Miller DL, Smith NB, Bailey MR et al (2012) Overview of therapeutic ultrasound applications and safety considerations. J Ultrasound Med 31:623–634
Ebadi S, Henschke N, Nakhostin Ansari N, Fallah E, van Tulder MW (2014) Therapeutic ultrasound for chronic low-back pain. Cochrane Database Syst Rev 14(3):CD009169. doi:10.1002/14651858
Gam AN, Johannsen F (1995) Ultrasound therapy in musculoskeletal disorders: a meta-analysis. Pain 63:85–91
Chan AK, Myrer JW, Measom GJ, Draper DO (1998) Temperature changes in human patellar tendon in response to therapeutic ultrasound. J Athl Training 33:130–135
Allen RJ (2006) Physical agents used in the management of chronic pain by physical therapists. Phys Med Rehabil Clin N Am 17:315–345
Sieper J, Rudwaleit M, Baraliakos X et al (2009) The Assessment of SpondyloArthritis international Society (ASAS) handbook: a guide to assess spondyloarthritis. Ann Rhem Dis 68(Suppl 2):ii1–ii44. doi:10.1136/ard.2008.104018
Yanik B, Gürsel YK, Kutlay S, Ay S, Elhan AH (2005) Adaptation of the Bath Ankylosing Spondylitis Functional Index to the Turkish population, its reliability and validity: functional assessment in AS. Clin Rheumatol 24:41–47. doi:10.1007/s10067-004-0968-6
Akkoc Y, Karatepe AG, Akar S, Kirazli Y, Akkoc N (2005) Turkish version of the Bath Ankylosing Spondylitis Disease Activity Index: reliability and validity. Rheumatol Int 25:280–284. doi:10.1007/s00296-003-0432-y
Duruoz MT, Doward L, Turan Y et al (2013) Translation and validation of the Turkish version of the ankylosing spondylitis quality of life (ASQoL) Questionnaire. Rheumatol Int 33:2717–2722. doi:10.1007/s00296-013-2796-y
Ebadi S, Ansari NN, Naghdi S et al (2012) The effect of continuous ultrasound on chronic non-specific low back pain: a single blind placebo-controlled randomized trial. BMC Musculoskelet Disord 13:192. doi:10.1186/1471-2474-13-192
Durmus D, Durmaz Y, Canturk F (2010) Effects of therapeutic ultrasound and electrical stimulation program on pain, trunk muscle strength, disability, walking performance, quality of life, and depression in patients with low back pain: randomized-controlled trial. Rheumatol Int 30:901–910. doi:10.1007/s00296-009-1072-7
Meakins A, Watson T (2006) Longwave ultrasound and conductive heating increase functional ankle mobility in asymptomatic subjects. Phys Ther Sport 7:74–80
Lehmann JF, Delateur BJ (1990) Diathermy and superficial heat, laser and cold therapy. In: Kottke FJ, Lehmann JF (eds) Krusen’s handbook of physical medicine and rehabilitation. W. B. Saunders Company, Philadelphia, pp 283–367
Susan LM, Karen JS (2007) Therapeutic Ultrasound. In: Susan LM, James WB, Thomas PN Jr (eds) Modalities for therapeutic intervention, 5th edn. EA Davis Company, Philadelphia, pp 85–109
Morrisette DC, Brown D, Saladin ME (2004) Temperature change in lumbar periarticular tissue with continuous ultrasound. J Orthop Sports Phys Ther 34:754–760. doi:10.2519/jospt.2004.34.12.754
Casimiro L, Brosseau L, Welch V et al (2002) Therapeutic ultrasound for the treatment of rheumatoid arthritis. Cochrane Database Syst Rev 3:CD003787. doi:10.1002/14651858.CD003787
Konrad K (1994) Randomized, double-blind, placebo-controlled study of ultrasonic treatment of the hands of rheumatoid arthritis patients. Eur J Phys Med Rehabil 4:155–157
Lim HJ, Moon YI, Lee MS (2005) Effects of home-based daily exercise on joint mobility, daily activity, pain and depression in patients with ankylosing spondylitis. Rheumatol Int 25:225–229. doi:10.1007/s00296-004-0536-z
Viitanen JV, Lehtinen K, Suni J, Kautiainen H (1995) Fifteen months’ follow-up of intensive inpatient physiotherapy and exercise in ankylosing spondylitis. Clin Rheumatol 14:413–419
Uhrin Z, Kuzis S, Ward MM (2000) Exercise and changes in health status patients with ankylosing spondylitis. Arch Intern Med 160:2969–2975. doi:10.1001/archinte.160.19.2969
Sweeney S, Taylor G, Calin A (2002) The effect of a home–based exercise intervention package on outcome in ankylosing spondylitis: a randomized controlled trial. J Rheumatol 29:763–766
Kraag G, Stokes B, Groh J, Helewa A, Goldsmith C (1990) The effects of comprehensive home physiotherapy and supervision on patients with ankylosing spondylitis. A randomized controlled trial. J Rheumatol 17:228–233
Altan L, Bingol U, Aslan M, Yurtkuran M (2006) The effect of balneotherapy on patients with ankylosing spondylitis. Scand J Rheumatol 35:283–289. doi:10.1080/03009740500428806
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
Duygu Silte, Ilknur Aktas, Feyza Unlu Ozkan, Meryem Kaysin, and Nuray Girgin declare that they have no conflict of interest.
Human and animal rights
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Şilte Karamanlioğlu, D., Aktas, I., Ozkan, F.U. et al. Effectiveness of ultrasound treatment applied with exercise therapy on patients with ankylosing spondylitis: a double-blind, randomized, placebo-controlled trial. Rheumatol Int 36, 653–661 (2016). https://doi.org/10.1007/s00296-016-3441-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00296-016-3441-3