
Abstract
The objective of this non-randomised controlled trial was to evaluate the impact of group-based exercise programme and a home-based exercise programme on Bath Ankylosing Spondylitis Indices, depression and quality of life in patients with ankylosing spondylitis (AS). Approximately 41 patients in a rehabilitation unit were divided into two groups, either group- or home-based exercise programme. Exercise sessions were performed three times a week for a period of 6 weeks. The patients were compared before and after the rehabilitation programme, with respect to Bath Ankylosing Spondylitis Functional Index (BASFI), Bath Ankylosing Spondylitis Disease Assessment Index (BASDAI), Bath Ankylosing Spondylitis Metrology Index (BASMI), Beck Depression Inventory (BDI) and The Nottingham Health Profile (NHP). A statistically significant improvement was observed on BASDAI, BASMI and energy, pain, reaction of emotional and sleep subscores of NHP in both exercise groups after the exercise programme (p < 0.05). No statistically significant changes were detected in BASFI, BDI and social and mobility subscores of NHP in both exercise groups (p > 0.05). No statistically significant differences were found between the two exercise programmes (p > 0.05). Group and home-based exercise programmes are efficient in improving symptoms and mobility and had an important effect on quality of life in patients with AS. Home-based exercise programme, as it is cheaper, more easily performed and efficient, may be preferable for the management programme in AS.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Ankylosing spondylitis (AS) is a chronic rheumatic disorder affecting mainly the axial skeleton, which progressively limits spinal and thoracic mobility throughout the course of the disease. AS involves inflammation and pain in many joints and spine, which cause physical outcomes such as reduced physical activity, reduced spinal mobility, stiffness, fatigue, sleep disturbances, and psychological consequences such as depression [1]. The purpose of the therapy is to reduce pain and stiffness, to prevent postural deformities, to maintain the patient’s maximal potential movement and psychosocial health [2, 3]. Several studies have reported beneficial effects of exercise on symptom severity, spinal mobility, muscle strength, functional capacity, cardiovascular capacity, and psychological status [2–4]. Therefore, physiotherapy is the cornerstone of the management programme in AS.
Most of the studies examined the effect of supervised exercise programs rather than unsupervised exercise in patient with AS [3, 5]. The Cochrane review data indicated that supervised group exercise programmes were better than home-based exercise programmes. However, in clinical practice, group-based exercise programmes for the rehabilitation of the patients with AS are not used except in a few centres in university hospitals in Turkey. These patients are generally prescribed home-based exercises. Furthermore, there are quite few studies that compared the efficacies of home- and hospital-exercise programmes in patients with AS [3, 5, 6]. Because of heterogeneous interventions and outcome measures, still however, there is not a consensus on the appropriate quantity, quality or intensity of exercise that is necessary to promote better health and function in this population [2, 7]. For this reason, we aimed to investigate and compare the impact of group- and home-based exercise programme symptoms, functional and mobility status as well as depression and quality of life in patients with AS.
Materials and methods
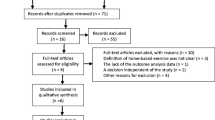
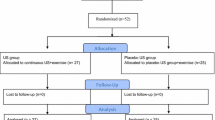
Forty-one patients diagnosed with AS according to the modified New York criteria aged 18–75 years were allocated into study. They were recruited from the Physical Medicine and Rehabilitation Department of Ege University Hospital and the Rheumatology Division of 9 Eylul University Hospital in Izmir, Turkey. Subjects were eligible to participate in the programme if they were an outpatient without complication and able to understand the content of questionnaire and exercise programme. Exclusion criteria were inability or unwillingness to participate in physiotherapy, systemic organic involvement, severe co-morbidity of heart, lung, liver or kidneys. Additionally, the patients, who had been practising regular exercises during the previous 6 months, were also not included in the study. The health status of the patients was clinically stable. Each volunteer gave their written consent to participate in this study. The patients who could participate in the group-based exercise programme were included in group I. The patients who had problems in transportation or getting permission from their work were allocated to the home-based exercise group (group II). Of the initial 41 patients, 3 patients failed to complete the programme: 2 who had transport problems (group I) and 1 because of unwillingness to exercise (group II).
Measurements
The following assessments were performed for all the subjects before and after the exercise programme.
Bath Ankylosing Spondylitis Functional Index
The Bath Ankylosing Spondylitis Functional Index (BASFI) consists of eight questions on daily activities and two additional questions that assess patients’ ability to cope with everyday life. Each question is answered on 10-cm horizontal visual analog scale (VAS). The VAS have no distinguishing marks except the words “easy” and “impossible” at either end of the line to indicate the direction of the severity. The mean of the ten scales results in the BASFI score (0–10), with higher scores indicating more severe impairment [8, 9].
Bath Ankylosing Spondylitis Disease Assessment Index
The Bath Ankylosing Spondylitis Disease Assessment Index (BASDAI) is a self-administered questionnaire consisting of six questions relating to the five major symptoms fatigue, spinal pain, joint pain/swelling, areas of localised tenderness and morning stiffness, measured in terms of both severity and duration. The patients were asked to mark the degree to which they had experienced aforementioned symptoms over the previous week. Each of the first five questions are answered on 10-cm, unmarked, horizontal VAS, except for the words “none” and “very severe” on the left and right ends, respectively, while the scale for quantity of morning stiffness is graded every 15 min between 0 h and 2 h. The mean of the two scores on morning stiffness is calculated. The total BASDAI score is obtained by converting the last score for the overall index (0–50) to a 0–10 scale [10, 11].
Bath Ankylosing Spondylitis Metrology Index
The Bath Ankylosing Spondylitis Metrology Index (BASMI) is composed of five measurements: cervical rotation, tragus-to-wall distance, lateral flexion, modified Schober’s distance and intermalleolar distance. Each measurement indicates either 0 (mild disease involvement), 1 (moderate disease involvement), or 2 (severe disease involvement) points, resulting in a total BASMI score of 0–10 [12].
The Nottingham Health Profile
The Nottingham Health Profile (NHP) consists of two parts. Part I contains 38 yes/no items in six dimensions: pain, physical mobility, emotional reactions, energy, social isolation and sleep. Part II contains seven general yes/no questions concerning daily-living problems. The two parts may be used independently, and part II is not analysed in this study. Part I is scored using weighted values which give a range of possible scores from zero (no problems at all) to 100 (presence of all problems within a dimension) [13, 14].
Beck Depression Inventory
Beck Depression Inventory (BDI) is a 21-item test presented in multiple-choice format which purports to measure presence and degree of depression. Responses are made on a four-point, minimally-anchored scale, ranging from 0 to 3, with 3 representing the most severe symptoms [15].
Exercise programme
Prior to the start of the programme, educational sessions and individual counselling were performed by physiatrist about AS. All of the patients were trained how to correctly perform the exercises by a physiotherapist. For each of the exercises, participants were provided with simple, step-by-step written instructions with illustrations. Group I patients were treated with a group-exercise programme composed of respiratory exercises, stretching, mobilization and strengthening exercises for lower, upper extremity and back muscles 3 days a week and 45 min a day under the supervision of the same physiotherapist for 6 weeks. Group II patients practised the same exercises individually at home 3 days a week for 6 weeks. A warm-up exercise in the form of a 10-min walk was always performed before the primary exercise session, finishing with 10 min of cool-down activities. The exercise included movements of flexion, extension, lateral flexion, and rotation of the cervical and lumbar spine, as well as extension, flexion, abduction, adduction, and rotation of both the upper and lower extremities at the beginning of the session. Free weights were used for resistance exercises, in the form of hand-held dumbbells and ankle cuff weights available in 0.5–1 kg increments. For each muscle group, participants were instructed to perform up to two sets of ten repetitions each through full range of motion. Resistance exercises were performed using the following techniques: overhead press, lateral shoulder raise, overhead triceps, single row, upright row, biceps curl, hip extension, hip abduction, calf raise, squat, sit-to-stand, hamstring curl and ankle flexion–extension. Flexibility exercises were primarily stretching of the major muscle groups (biceps, triceps, rhomboid, trapezius, hamstrings, quadriceps, hip flexors, calf, gluteus and the hip adductors). Respiratory exercises consisted of pursed-lip breathing, expiratory abdominal augmentation and synchronization of thoracic and abdominal movement.
Statistical analysis
Data were introduced in the Statistical Package for the Social Sciences (SPSS) package, version 11.5. Baseline demographic and clinical characteristics were compared using the independent samples t test or Mann–Whitney U test. The repeated measurements analysis of variance (ANOVA) was used to compare groups with regard to parameters obtained before and after rehabilitation, and it was also used to assess inter-group differences. Correlations between the variables were tested with a non-parametric (Spearman, for ordinal data) and parametric (Pearson, for metric data) correlation analysis.
Results
Thirty eight patients have completed the study. Demographic details of both groups I and II are presented in Table 1. When the exercise groups were compared, no statistically significant differences were found in the demographic characteristics (p > 0.05). Similarly, both groups were comparable with respect to BASMI, BASFI, BASDAI, NHP and BDI scores before the onset of the exercise programme (p > 0.05).
A statistically significant improvement was observed in BASDAI, BASMI and energy, pain, emotional reaction and sleep subscores of NHP in both of the exercise groups after completion of the exercise programme (Table 2; p < 0.05). In comparison of the two exercise groups, only a difference in favor of group I in the sleep subscore of NHP was found among BASDAI, BASMI and energy, pain, emotional reaction and sleep subscores of NHP (p < 0.05). No statistically significant changes were detected in BASFI, BDI and social and mobility subscores of NHP in either exercise groups (Table 2; p > 0.05). No significant difference was detected between the exercise groups as far as BASFI, BDI, social and mobility subscores of NHP were concerned (p > 0.05, Table 2).
Discussion
Results of our study have revealed a significant improvement in the level of mobility, disease characteristics and most of the quality-of-life scores of AS patients with both exercise programmes. As reported by the studies in the literature, exercise programmes are effective on symptoms, mobility and functional capacity in the short term; but their effects in the long term are still being questioned [2, 13]. In the Cochrane review was stated that home-based exercise programmes are better than not exercising at all; and supervised exercise programmes are superior to home-based exercise programmes when functionality and mobility are considered [2, 6]. Relevant literature mostly introduces studies, in which supervised exercise programmes are carried out on AS patients [3, 5]. It has also been reported that factors such as sharing experiences with other patients and being encouraged for exercising in group-exercise programmes are important in terms of increasing compliance and psychological comfort of the patients; yet it has also been stated that satisfactory proofs cannot be provided for this argument [2, 16, 17]. Nevertheless, the number of studies comparing supervised and unsupervised exercises is still not sufficient [18]. It is noted in the studies that most clinicians recommend home-based exercise programmes, as supervised exercises require more time and money [18]. Our observations in clinical practices also support this point. At the end of our study, improvements were observed in both exercise programmes, and a distinct difference was not detected between the two groups in terms of improvement. This outcome carries importance for revealing the fact that home-based exercise programmes widely recommended by most clinicians are useful and that they do not provide different results from supervised exercise programmes. In the light of the existing findings and evidences, it is difficult to explain which exercise protocol is more effective on AS patients [2, 19]. For example, it has been reported in a study that an exercise programme carried out for 200 min/week and for at least 5 days reveals significant improvement in pain, stiffness and functional disability; and that exercises of shorter time and lesser intensity do not show the same effect [18]. In this respect, it is important to prepare a special programme for each patient taking into consideration the patient’s age, duration of disease, living conditions, physical characteristics and psychological condition.
It is noted that in early- and late-stage AS, different exercises provide improvement at different doses at different parameters [6, 20]. Pain and stiffness in early stage are thought to stem from inflammation rather than mechanic reasons, and therefore the recognition of improvement by exercise is considered relevant. There are also interpretations indicating that patients have less spinal fusion in the early stage, they practice the exercises more willingly, the amount of catecholamine and endorphin secretion increases, and these secretions have analgesic and anti-inflammatory effect [21]. It was observed that the exercises were more effective on pain and stiffness in AS patients who were monitored for 15 years or less than those patients monitored for more than 15 years [18]. On the other hand, Vitanen and Heikkila [22] have put forward that there is not a direct relationship between improvement and duration of the disease. It has also been reported that there is no relation between intensity of exercise and health status in AS patients monitored for more than 15 years because these patients generally exercise less [18]. Most of the patients in our study are being monitored with AS diagnosis for more than 15 years. Our study has revealed that duration of the disease has a relation with pain and mobility. However, any additional investigation for evaluating the effect of duration of disease on the exercise could not be carried out.
In our study, BASDAI scores have revealed improvement in both exercise groups. Although Sweeney et al. [23] note in their study that there is no difference between exercise group and control group in terms of BASDAI, the study of Karatepe et al. [9] reports a significant improvement. Fenandez-de-las Penaas et al. [24], supporting our research results, found that a significant difference was not observed between supervised and unsupervised exercise groups in terms of stiffness.
The reason to assess the BASMI index is that it is the only validated index in the peer-reviewed literature assessing the status of the axial skeleton in patients with AS [24]. In this study, mobility level, which was assessed with BASMI, improved significantly in both exercise groups. There is no consensus on standard measurements for mobility assessment; different areas are selected for each study, and even the mobility assessment has not been made in some studies [18, 25]. The effect of home-based exercise on spinal mobility has not been proven yet, but its efficacy is acknowledged [9, 20]. Although group exercise is stated to be effective on mobility, some measurements do not reveal any change [6]. Despite the fact that an improvement was observed in both groups in our study, a significant difference was not recognised between the groups. It should be taken into consideration that the average BASMI score of neither group is high. Improvements in all scale scores of assessment in our study point to the positive effect of exercises.
The functional status assessed with BASFI score did not improve in either group-based exercise patients or home-based exercise patients. Furthermore, no difference was observed between the two exercise groups. BASFI scores of our patients were found to be lower than the patient scores in other studies [3, 22]. Therefore, a major improvement may not have been noted. Similar to our study, some researchers have reported the positive effect of exercise programmes on functional state, whereas some researchers have not detected any difference between home-based exercises and the control group [3, 6, 9, 20, 23].
General life-quality assessment scales have not been widely used in studies related to AS [18]. Yet, it is evident that there should necessarily be an improvement in these patients’ quality of life in order to talk about the success of treatment. In our study, the improvement in most of NHP scores through both exercise programmes is a significant indicator for our success in treatment.
To date, most studies of AS have focused on physical health and outcomes rather than on the impact of the disease on psychological health [2, 4, 5]. It has been emphasised that increased disease activity and functional disability are related to poor mental health [26]. In our study, the psychosocial status evaluated with BDI did not show any significant change in either group. The reason behind the higher BDI scores in some studies compared to the scores of the patients in our study may be a possibility [1, 3]. Consequently, as psychological symptoms of patients with AS also affect the quality of life, this factor should be taken into consideration in the evaluation of patients and should be included in the assessment stages of the treatment success.
The compliance of the patients to physiotherapy interventions is dependent on their motivation. As these interventions are time-consuming, it is important to give information and education programmes about the usefulness of the exercises to the patients to increase compliance. We believe that informing the patients beforehand about the disease and the significance of exercising is effective for increasing motivation. Most of the AS patients do not exercise regularly, and their compliance declines in the long term [13, 22]. It has been reported that the patients with less disability exercise less when compared to the patients with more disabilities [16]. These results reveal the necessity of rendering the exercises more interesting and gripping and therefore the significance of motivation. Only three patients did not complete the study due to transportation problems and unwillingness. The patients in our study regularly attended the exercise programme, and at the end of the programme they pronounced the positive effects they had benefited from.
The strong aspects of our study may be counted as the evaluation of functional state, psychological state and quality of life within the scope of a single study and the comparison of group-based and home-based exercise programmes, on which sufficient number of studies have not been carried out in the literature [3, 5, 6].
Our study also has some limitations. As group-based exercise programme is related to time and money, we grouped the patients not randomly but according to their own request. We could not follow the patients after the exercise programme; therefore this prevented us from detecting long-term effects. As in most studies, men outnumbered women also in our study group [3, 4, 17]. However, number of women/men in home-based exercise group was close to one another unlike in other studies. Yet, it is still not easy to generalise the research results for both sexes. We could not group the patients as earlier and later than 15 years; but examining the effects related to the duration of the disease was not within the scope of our study’s objective. Thus, we only evaluated whether there was a relation with the duration of the disease. We think that there is need for further studies, in which exercise programmes with different durations and intensity are compared, to provide treatment guidelines.
Reviews that are prepared to give information about the efficacy of exercises in AS patients have implicated the difficulties in preparing exercise guidelines [2]. One of the issues attributed utmost emphasis is the insufficient number of studies on the efficiency of supervised and unsupervised exercise programmes. The results of our study are significant in terms of both noting the above-mentioned point and revealing that neither of the two different exercise programmes has distinctive superiority over one another. In this respect, we believe that our study results will constitute a useful source for other studies and preparation of treatment guidelines.
In conclusion, group-based and home-based exercise programmes are efficient in improving symptoms and mobility and have an important effect on the quality of life in patients with AS. No significant differences were found between the two exercise programmes. Home-based exercise programme may be preferable for the management programme in AS, as it is cheaper, performed more easily and more efficient.
References
Lim HJ, Lim HS, Lee MS (2005) Relationship between self-efficacy and exercise duration in patients with ankylosing spondylitis. Clin Rheumatol 24:442–443
Dagfinrud H, Kvien TK, Hagen KB (2005) The Cochrane review of physiotherapy interventions for ankylosing spondylitis. J Rheumatol 32:1899–906
Analay Y, Ozcan E, Karan A et al (2003) The effectiveness of intensive group exercise on patients with ankylosing spondylitis. Clin Rehabil 17:631–636
Ince G, Sarpel T, Durgun B et al (2006) Effects of multimodal exercise program for people with ankylosing spondylitis. Phys Ther 86:924–935
Helliwell P, Abbott CA, Chamberlain MA (1996) A randomised trial of three different physiotherapy regimes in ankylosing spondylitis. Physiotherapy 82:85–90
Hidding A, van der Linden S, Boers M et al (1993) Is group physical therapy superior to individualized therapy in ankylosing spondylitis? A randomized controlled trial. Arthritis Care Res 6:117–125
Santos H, Brophy S, Calin A (1998) Exercise in ankylosing spondylitis: how much is optimum. J Rheumatol 25:2156–2160
Calin A, Garrett S, Whitelock H et al (1994) A new approach to defining functional ability in ankylosing spondylitis: the development of the Bath Ankylosing Spondylitis Functional Index. J Rheumatol 21:2281–2285
Karatepe AG, Akkoc Y, Akar S et al (2005) The Turkish versions of the Bath Ankylosing Spondylitis and Dougados Functional Indices: reliability and validity. Rheumatol Int 25:612–618
Akkoc Y, Karatepe AG, Akar S et al (2005) A Turkish version of the Bath Ankylosing Spondylitis Disease Activity Index: reliability and validity. Rheumatol Int 25:280–284
Garrett S, Jenkinson T, Kennedy LG et al (1994) A new approach to defining disease status in ankylosing spondylitis: the Bath Ankylosing Spondylitis Disease Activity Index. J Rheumatol 21:2286–2291
Jenkinson TR, Mallorie PA, Whitelock HC et al (1994) Defining spinal mobility in ankylosing spondylitis (AS). The Bath AS Metrology Index. J Rheumatol 21:1694–1698
Carr-Hill RA, Kind P (1989) The Nottingham Health Profile. Soc Sci Med 28:885
Kucukdeveci AA, McKenna SP, Kutlay S et al (2000) The development and psychometric assessment of the Turkish version of the Nottingham Health Profile. Int J Rehabil Res 23:31–38
Beck AT, Ward CH, Mendelson M et al (1961) An inventory for measuring depression. Arch Gen Psychiatry 4:561–571
Hider S, Wong M, Ortiz M et al (2002) Does a regular exercise program for ankylosing spondylitis influence body image. Scand J Rheumatol 31:168–171
Fankenbach A (2003) Disability motivates patients with ankylosing spondylitis for more frequent physical exercise. Arch Phys Med Rehabil 84:382–383
Uhrin Z, Kuzis S, Ward M (2000) Exercise and changes in health status in patients with ankylosing spondylitis. Arch Intern Med 160:2969–2975
Santos H, Brophy S, Calin A (1998) Exercise in ankylosing spondylitis: how much is optimum. J Rheumatol 25:2156–2160
Kraag G, Stokes B, Groh J et al (1994) The effect of comprehensive home physiotherapy and supervision on patients with ankylosing spondylitis—an 8-month follow-up. J Rheumatol 21:261–263
Pedersen BK, Bruunsgaard H, Klokker M et al (1997) Exercise-induced immunomodulation–possible roles of neuroendocrine and metabolic factors. Int J Sports Med 18(Suppl 1):S2–S7
Viitanen JV, Heikkila S (2001) Functional changes in patients with spondylarthropathy. A controlled trial of the effects of short-term rehabilitation and 3-year follow-up. Rheumatol Int 20:211–214
Sweeney S, Taylor G, Calin A (2002) The effect of a home based exercise intervention package on outcome in ankylosing spondylitis: a randomized controlled trial. J Rheumatol 29:763–766
Fernandez-de-las-Penaas C, Alonso-Blanco C, Morales-Cabezas M et al (2005) Two exercise interventions for the management of patients with ankylosing spondylitis. Am J Phys Med Rehabil 84:407–419
Heikkila S, Viitanen JV, Kautiainen H et al (2000) Sensitivity to change of mobility tests; effect of short term intensive physiotherapy and exercise on spinal, hip, and shoulder measurements in spondylarthropathy. J Rheumatol 27:1251–1256
Da Costa D, Dritsa M, Ring A et al (2004) Mental health status and leisure-time physical activity contribute to fatigue intensity in patients with spondylarthropathy. Arthritis Rheum 51:1004–1008
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Karapolat, H., Akkoc, Y., Sarı, İ. et al. Comparison of group-based exercise versus home-based exercise in patients with ankylosing spondylitis: effects on Bath Ankylosing Spondylitis Indices, quality of life and depression. Clin Rheumatol 27, 695–700 (2008). https://doi.org/10.1007/s10067-007-0765-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10067-007-0765-0