
Abstract
This prospective multicenter study was performed to clarify the efficacy and safety of micafungin (MCFG) as an empirical antifungal therapy for suspected fungal infection in patients with hematological disorders and neutropenia. Three hundred and eighty-eight patients were enrolled; 151 patients with possible fungal infection diagnosed by radiological imaging or serological testing and 237 patients with refractory fever were included in this study. The mean dose and duration of treatment with MCFG were 154.6 mg/day and 14.0 days, respectively. The clinical response rate for patients with possible fungal infection and refractory fever was 60.1% and 65.3%, respectively. Even in persistent neutropenic patients with a neutrophil count of <500/μL throughout the MCFG treatment, the clinical response rate was 46.9%. Ninety-one drug-related adverse events (DAEs) were observed in 56 patients (14.4%) and 9 serious DAEs were observed in 6 patients (1.5%). Neither daily dose nor duration of MCFG treatment affected the incidence of DAEs. It was confirmed that MCFG has adequate clinical efficacy and is safe for the treatment of suspected fungal infections in patients with hematological disorders and neutropenia.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Invasive fungal infections (IFIs) are a serious concern in the management of immunocompromised patients with hematological disorders. Empirical antifungal therapy is recommended for neutropenic patients with persistent fever despite the administration of broad-spectrum antibacterial agents, because early diagnosis of IFIs is difficult and the delayed treatment of fungal infection often produces poor outcomes [1, 2]. With empirical antifungal therapy, the spectrum of activity and toxicity profile of antifungals should be adequately taken into account.
Micafungin (MCFG), a member of the echinocandin antifungal family, which specifically inhibits the synthesis of 1,3-β-d-glucan, a primary component of fungal cell walls [3–5], showed potent antifungal activity against both Candida spp. and Aspergillus spp. in in vitro as well as in vivo studies [6–11]. The efficacy and safety of MCFG against both Candida and Aspergillus infections has also been demonstrated in several clinical trials [11–16]. MCFG was first launched for candidiasis and aspergillosis in Japan in 2002, and has now been approved for these same indications in China and the Middle East. Although MCFG is only approved for candidiasis in the USA and Europe, it is recommended as salvage therapy for aspergillosis in the Clinical Practice Guideline of the Infectious Diseases Society of America [17]. MCFG is now the most prescribed empirical antifungal therapy for febrile neutropenia in Japan [18]. Several reports of studies regarding the safety and efficacy of MCFG for suspected fungal infections in patients with hematological disorders are available [19–25]. However, fewer than 200 subjects were included in these studies.
We hereby report the results of a clinical study of the efficacy and safety of MCFG in 388 Japanese patients with hematological disorders and neutropenia who received empirical antifungal therapy for suspected fungal infections.
Patients and methods
Study design
The prospective, multicenter, open, observational study was conducted between April 2005 and September 2006 under the Japanese regulation, Good Post-marketing Study Practice, at 166 institutions in Japan. Investigators registered patients who met the following inclusion criteria at a central office within 6 days after the initiation of MCFG treatment.
The protocol of this study was reviewed and approved by the Ministry of Health, Labour and Welfare. The Institutional Review Board also approved the protocol according to the rules of each institution before this study started. Since this study was designed as an observational study, informed consent was not necessarily obtained from all patients.
Inclusion criteria
Patients with neutropenia (<1,000/μl) and clinical symptoms/findings such as fever, cough, sputum, dyspnea, chest pain, and pharyngeal pain were enrolled if they met any of the following criteria: (1) those who had possible fungal infection diagnosed either by radiological imaging (chest X-ray or CT) or serological testing (1,3-ß-d-glucan or galactomannan), (2) those who had refractory fever defined as an unexplained persistent fever (axillary temperature > 37.5°C) after broad-spectrum antibacterial treatment for 2 days or longer.
The definition of possible fungal infection proposed by EORTC/MSG [26] was modified and utilized in this study. Radiological imaging had to show lower respiratory tract abnormality, either a halo sign, infiltration, or a cavity. Serologic tests consisted of the Platelia Aspergillus test (Fujirebio, Tokyo, Japan) to detect Aspergillus galactomannan antigen by enzyme-linked immunosorbent assay (cutoff value 0.5), and the 1,3-ß-d-glucan test (cutoff value 11.0 pg/mL for the Wako glucan test, Wako Pure Chemical Industries, Osaka, Japan; and cutoff value 20 pg/mL for the Fungitec G Test, Seikagaku Corporation, Tokyo, Japan).
Treatment schedule and dose
Physicians treated the patients according to the dosage and administration stated in the package insert of MCFG. The patients were treated with MCFG for 5 days to 4 weeks at a dose of 50–150 mg by intravenous administration over 30 min of a dose of 75 mg or less, and over 1 h of a dose exceeding 75 mg, once daily. In severe cases, the dose could be increased to 300 mg/day, depending on the symptoms. The concomitant use of other antifungals was permitted if necessary.
Efficacy assessment
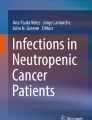
The efficacy evaluation algorithm defined in our previous report [22] was slightly modified. Efficacy at the end of treatment with MCFG was assessed based on improvement in positive clinical symptoms/findings, radiological imaging (chest X-ray or CT scan), and fungal serological testing (1,3-ß-d-glucan or galactomannnan). The criteria for a positive clinical response are as follows: “Marked improvement” (defervescence, an axillary temperature of <37.0°C, and disappearance of clinical symptoms/findings), “improvement” (defervescence, an axillary temperature of <37.5°C or improvement of at least 1.0°C from the baseline temperature of ≥39.0°C, and reduction of clinical symptoms/findings), “no change” or “aggravation” (increase in body temperature or aggravation of clinical symptoms/findings). The criteria for the radiological imaging response are as follows: “Eradication” (disappearance of infiltrates), “improvement” (decrease in infiltrates), “no change,” “aggravation” (increase in existing infiltrates or appearance of new infiltrates), or “not applicable.” The criteria for the serological response are as follows: “Improvement” (decrease in values), “no change,” “aggravation” (increase in values), or “not applicable.” The clinical response (effective or ineffective) was determined using an algorithm based on the assessment of all three indexes (Fig. 1).

Algorithm for efficacy evaluation
Safety assessment
All adverse events including abnormal laboratory findings observed after the start of MCFG treatment were recorded. The seriousness and causal relationship of the adverse events were determined by the investigator. Seriousness was classified into the three levels of “mild,” “moderate (neither mild nor serious),” and “serious” in accordance with the ICH Harmonised Tripartite Guideline [27]. All adverse events were followed up until they had resolved. The causal relationship between the adverse event and MCFG was defined as probable, possible, not related, or unassessable. Adverse events determined as probable and possible were defined as drug-related adverse events (DAEs).
Before the start of this study, an advisory board composed of the authors of this article was appointed to review the validity of the diagnosis and the evaluation of efficacy and safety by each investigator.
Results
Patient characteristics and MCFG treatment
The baseline profile of the 388 patients enrolled in this study is shown in Table 1. The patients consisted of 234 males (60.3%) and 154 females (39.7%). The mean age and body weight were 57.8 years (range 17–94) and 56.9 kg (range 30–90), respectively. The main underlying hematological disorders were acute leukemia (61.3%), non-Hodgkin’s lymphoma (18.3%), and myelodysplastic syndrome (10.8%). The number of patients who had undergone hematopoietic stem cell transplantation (HSCT) was 76 (19.6%). One hundred and fifty-one patients (38.9%) were classified as having possible fungal infection diagnosed by positive radiological imaging (104 patients) or serological testing (47 patients), and 237 patients (61.1%) were classified as having refractory fever.
The positive rates of the radiological imaging, plasma (1,3)-ß-d-glucan test and plasma galactomannan test were 29.9% (104/348), 13.1% (47/360), and 2.4% (2/82), respectively. Among 104 patients with positive radiological imaging, 59 were diagnosed by X-ray, 16 were diagnosed by CT, and the remaining 29 were diagnosed by both methods. Patients with a neutrophil count of <500/μL before treatment with MCFG occupied 88.4%. Two hundred and forty patients (61.9%) had received other oral antifungals before the treatment with MCFG.
Dose and duration of MCFG treatment
The mean daily dose of MCFG was 154.6 mg, and 68.8% of the patients were treated with 150 mg MCFG. The mean duration of MCFG treatment was 14.0 days, and 62.6% of the patients completed the treatment within 14 days (Table 2).
Efficacy
The overall clinical response rate, excluding four non-evaluable patients, was 63.3% (243/384) (Table 3). No difference in the response rate was observed between the main underlying hematological disorders such as acute leukemia (63.9%), non-Hodgkin’s lymphoma (65.2%), and myelodysplastic syndrome (61.0%). The response rate in patients who had undergone HSCT was 63.2% (48/76), and that in patients with MCFG monotherapy was 63.8% (238/373).
The clinical response rate by each diagnosis was 60.1% (89/148) in patients with possible fungal infection and 65.3% (154/236) in patients with refractory fever.
The clinical response rate was evaluated in detail by neutrophil count as shown in Table 4. Even in persistent neutropenic patients whose neutrophil count was <500/μL throughout the treatment with MCFG, the response rate was 46.9% (61/130). The response rate by the duration of neutropenia in 130 patients whose neutrophil count was <500/μL throughout the treatment was 39.3% (11/28) for up to 7 days, 53.6% (30/56) for between 8 and 14 days, and 43.5% (20/46) for between 15 and 28 days. The clinical response rate by the duration of refractory fever under antibacterial treatment is shown in Table 5. The response rate in patients with refractory fever for 48, 72, and 96 h or longer before MCFG treatment was 94.1% (16/17), 66.7% (32/48), and 62.0% (106/171), respectively.
Excluding 19 patients who lacked follow-up radiological imaging after MCFG treatment, the improvement rate in the chest X-ray, or computed tomography was 51.8% (44/85).
Excluding 14 patients whose serological test data (1,3-ß-d-glucan) were not available after MCFG treatment, 1,3-ß-d-glucan levels fell below the cutoff value in 24 of 33 patients (72.7%). None of the 24 patients whose plasma 1,3-ß-d-gulucan fell below the cutoff value showed aggravation of clinical symptoms/findings. The clinical response was “effective” in 14 patients, and “ineffective” in the remaining 10 patients.
Among the 141 patients who experienced treatment failure with MCFG, blood culture was positive in 25 patients (17.7%) during the treatment period; namely Gram-positive bacteria in 19, Gram-negative bacteria in 3, and fungi in 3 (Scedosporium sp., Cryptococcus terreus, and Candida parapsilosis).
Safety
Among the 388 patients, 91 DAEs were observed in 56 patients (14.4%) (Table 6). The most common DAEs were hepatic function abnormalities including elevation of alanine aminotransferase, aspartate aminotransferase, and serum bilirubin. These DAEs were observed in 38 patients (9.8%). Since five DAEs occurred after the discontinuation of MCFG in four patients, their recovery was not evaluated. Of the remaining 86 DAEs, 8 led to discontinuation of MCFG. Thirteen DAEs, including these 8 events, recovered after discontinuation of MCFG, and 53 events recovered without discontinuation of MCFG. Thirty-five events recovered within 14 days, 22 events between 15 and 28 days, and 9 events more than 28 days after the onset of the adverse event.
Nine serious events were observed in six patients at a dose of 150 mg or less, while there was a possibility that underlying diseases or concomitant drugs might have contributed. Excluding two patients in whom the DAEs were observed after the end of MCFG treatment, MCFG treatment was not discontinued due to the DAEs in the other four patients. The outcomes of eight serious events could not be followed up because the patients died due to the underlying disease, and the remaining one event recovered while the patient was on MCFG treatment.
The incidence of DAEs by maximum daily dose was 10.8% (8/74) for 100 mg or less, 16.5% (44/267) for 150 mg, and 8.5% (4/47) for 200 mg and higher (Table 7). The incidence of DAEs by duration of MCFG treatment was 11.5% (28/243) for up to 14 days, 11.1% (8/72) for 15–21 days, and 27.4% (20/73) for 22 days and longer. The incidence of DAEs was higher in patients who were treated with MCFG for 22 days and longer, and 38 DAEs including 20 hepatobiliary disorders were observed in these 20 patients. However, the number of DAEs observed 22 days after the start of MCFG treatment or later was only ten events in seven patients. Among 20 hepatobiliary disorders reported in patients treated with MCFG for 22 days and longer, 80.0% (16/20) were observed within 21 days.
The incidence of DAEs in patients on MCFG monotherapy and those on combination therapy with another antifungal was 14.3% (54/373) and 18.2% (2/11), respectively. There was no difference in the incidence of DAEs between the patients with or without other oral antifungals before MCFG treatment (14.6% and 14.2%, respectively).
Discussion
Our study was designed to focus on patients who received empirical therapy for persistent febrile neutropenia and the efficacy rate was 63.3% (243/384). Of the 384 patients, 148 were diagnosed as possible fungal infection by positive radiological imaging or serological testing and 236 were diagnosed as refractory fever. The clinical response rate in patients with possible fungal infection and refractory fever were 60.1% (89/148) and 65.3% (154/236), respectively. According to the definition of “preemptive therapy” in recent reports [28, 29], it may be appropriate to apply this term to the treatment of the 148 patients with possible fungal infection in this study; however, this definition is still controversial. No inclusion criteria concerning treatment with other antifungals were set, but 97.2% (377/388) of patients included in this study were treated with MCFG monotherapy. The efficacy rate in this study, 63.3% (243/384), was comparable to that in our previous study in patients with hematological disorders, 68.0% (134/197) [22], though there are differences in the patients’ background, especially, the neutrophil count at enrollment. Besides our previous study [22], several reports on the safety and efficacy of MCFG for suspected fungal infections in patients with hematological disorders are available [19–21, 23–25]. Most of these studies have been conducted in small-sized populations (fewer than 55 patients), except for the study by Kubiak et al., which, however, was retrospective and lacked radiological and serological data.
Empirical treatment with other antifungals, caspofungin, itraconazole, voriconazole, and liposomal amphotericin B, has been studied in randomized controlled trials in patients with neutropenia and persistent fever [30–33]. In these comparative studies, a clinical response rate of 26–50% was reported, and was assessed by the five-component endpoint: (1) Absence of any breakthrough fungal infection during therapy or within 7 days after the completion of therapy, (2) survival for 7 days after the completion of therapy, (3) successful treatment of any baseline fungal infection, (4) no premature discontinuation of study drug because of drug-related toxicity or lack of efficacy, and (5) resolution of fever during neutropenia. In our study, the first two endpoints were not used as components of the efficacy endpoint. In fact, breakthrough fungal infection was seen in three patients in this study, and all of them were assessed to be ineffective by the algorithm based on the assessment of clinical symptoms/findings and radiological imaging and serological testing. As a result, absence of an efficacy endpoint regarding breakthrough fungal infection did not affect efficacy in this study. The clinical response rate, assessed by the latter three endpoints, was 46.9% (61/130) in patients with a neutrophil count remaining <500/μL throughout treatment. This result suggests that MCFG may be an alternative to caspofungin, itraconazole, voriconazole, and liposomal amphotericin B, although comparative studies of MCFG and other antifungal agents have not been conducted.
The usefulness of the 1,3-ß-d-glucan assay was also confirmed in this study. The test kit was developed in Japan [34], and is now widely utilized to diagnose fungal infections [18]. In the revised EORTC/MSG guidelines, measurement of 1,3-ß-d-glucan is newly added to the microbiological criteria, and it is recommended to be used for an early diagnosis of probable invasive fungal disease by Aspergillus or Candida [35]. The 1,3-ß-d-glucan was measured in most of the patients included in this study. Forty-seven of 360 patients (13.1%) were positive for 1,3-ß-d-glucan, and were diagnosed with possible fungal infection. The possibility of false-positive results seemed unlikely in these patients, because patients who were treated with cellulose-based dialysates, surgical gauze containing glucan, blood preparations (gamma globulin, albumin), antibiotics containing glucan (amoxicillin-clavulanic acid), or other glucan-containing drugs (Schizophyllan, Lentinan), which are reported to cause false-positive results of 1,3-ß-d-glucan testing [36], were not applicable. The widespread use of antifungal prophylaxis with fluconazole or itraconazole was reported in Japan [18], and 61.9% of patients (240/388) had received these drugs before the treatment with MCFG. This may explain the low positive rate of 1,3-β-d-glucan in this study. None of the 24 patients whose plasma 1,3-ß-d-glucan fell below the cutoff value showed aggravation of clinical symptoms/findings, and the clinical response in 14 of these 24 patients was “effective.” These results support the use of 1,3-ß-d-glucan as a practical marker to monitor the course of patients’ condition. Recently, the usefulness of preemptive/presumptive therapy using high-resolution CT and galactomannan has been reported [28, 29]. However, it seems that the attention to the diagnosis of invasive candidiasis is lacking in these study. By adding 1,3-ß-d-glucan testing to CT and galactomannan testing, a more refined strategy and better results are anticipated.
The clinical response rate in patients with a persistent fever was 65.3% (154/236). Concerning efficacy as analyzed by the duration of refractory fever in this study, the response rate in patients with refractory fever for at least 48, 72, or 96 h before MCFG treatment was 94.1% (16/17), 66.7% (32/48), and 62.0% (106/171), respectively. The contribution of previously administered antibacterial agents to the higher efficacy rate could not be completely ruled out in the patients with earlier MCFG treatment. The appropriate timing to start empirical antifungal therapy should be carefully and appropriately considered based on various aspects such as the clinical data and the symptoms of each patient in clinical practice.
Regarding the safety of MCFG, DAEs were observed in 14.4% (56/388), and mild or moderate hepatic function abnormalities were reported as frequent adverse events. This result is consistent with that of the previous report [22, 23]. Several serious DAEs were reported in this study. However, the physicians suggested the possibility that underlying diseases or concomitant drugs other than MCFG might have contributed to all of these serious DAEs. No tendency between daily dose and incidence of DAEs was found in this study. Although the incidence of DAEs seemed higher in patients treated for long duration, most of DAEs including hepatobiliary disorders were observed relatively early after the start of MCFG treatment.
In conclusion, the high clinical efficacy and safety profile of MCFG for suspected fungal infections in patients with hematological disorders and neutropenia was confirmed in this study. These results suggest that micafungin is a useful drug for empirical antifungal therapy.
References
Hughes WT, Armstrong D, Bodey GP, Bow EJ, Brown AE et al (2002) Guidelines for the use of antimicrobial agents in neutropenic patients with cancer. Clin Infect Dis 34:730–751
Wingard JR (2004) Empirical antifungal therapy in treating febrile neutropenic patients. Clin Infect Dis 39:S38–S43
Tomishima M, Ohki H, Yamada A, Takasugi H, Maki K et al (1999) FK463, a novel water-soluble echinocandin lipopeptide: synthesis and antifungal activity. J Antibiot (Tokyo) 52:674–676
Hatano K, Morishita Y, Nakai T, Ikeda F (2002) Antifungal mechanism of FK463 against Candida albicans and Aspergillus fumigatus. J Antibiot (Tokyo) 55:219–222
Chandrasekar PH, Sobel JD (2006) Micafungin: a new echinocandin. Clin Infect Dis 42:1171–1178
Tawara S, Ikeda F, Maki K, Morishita Y, Otomo K et al (2000) In vitro activities of a new lipopeptide antifungal agent, FK463, against a variety of clinically important fungi. Antimicrob Agents Chemother 44:57–62
Nakai T, Uno J, Otomo K, Ikeda F, Tawara S et al (2002) In vitro activity of FK463, a novel lipopeptide antifungal agent, against a variety of clinically important molds. Chemotherapy 48:78–81
Ikeda F, Wakai Y, Matsumoto S, Maki K, Watabe E et al (2000) Efficacy of FK463, a new lipopeptide antifungal agent, in mouse models of disseminated candidiasis and aspergillosis. Antimicrob Agents Chemother 44:614–618
Matsumoto S, Wakai Y, Nakai T, Hatano K, Ushitani T et al (2000) Efficacy of FK463, a new lipopeptide antifungal agent, in mouse models of pulmonary aspergillosis. Antimicrob Agents Chemother 44:619–621
Maesaki S, Hossain MA, Miyazaki Y, Tomono K, Tashiro T et al (2000) Efficacy of FK463, a 1, 3-β-D-glucan synthase inhibitor, in disseminated azole-resistant Candida albicans infection in mice. Antimicrob Agents Chemother 44:1728–1730
Ikeda F, Tanaka S, Ohki H, Matsumoto S, Maki K et al (2007) Role of micafungin in the antifungal armamentarium. Curr Med Chem 14:1263–1275
Kohno S, Masaoka T, Yamaguchi H, Mori T, Urabe A et al (2004) A multicenter, open-label clinical study of micafungin (FK463) in the treatment of deep-seated mycosis in Japan. Scand J Infect Dis 36:372–379
de Wet NT, Bester AJ, Viljoen JJ, Filho F, Suleiman JM et al (2005) A randomized, double blind, comparative trial of micafungin (FK463) vs. fluconazole for the treatment of oesophageal candidiasis. Aliment Pharmacol Ther 21:899–907
de Wet N, Llanos-Cuentas A, Suleiman J, Baraldi E, Krantz EF et al (2004) A randomized, double-blind, parallel-group, dose–response study of micafungin compared with fluconazole for the treatment of esophageal candidiasis in HIV-positive patients. Clin Infect Dis 39:842–849
Kuse ER, Chetchotisakd P, da Cunha CA, Ruhnke M, Barrios C et al (2007) Micafungin versus liposomal amphotericin B for candidaemia and invasive candidosis: a phase III randomised double-blind trial. Lancet 369:1519–1527
Pappas PG, Rotstein CM, Betts RF, Nucci M, Talwar D et al (2007) Micafungin versus caspofungin for treatment of candidemia and other forms of invasive candidiasis. Clin Infect Dis 45:883–893
Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP et al (2008) Treatment of aspergillosis: clinical practice guidelines of the infectious diseases society of America. Clin Infect Dis 46:327–360
Fujita H, Yoshida M, Miura K, Sano T, Kito K et al (2009) Management of infection in patients with acute leukemia during chemotherapy in Japan: questionnaire analysis by the Japan adult leukemia study group. Int J Hematol 90:191–198
Ishikawa T, Takata T, Tomoyose T, Masuda M, Nakachi S et al (2006) The efficacy of micafungin as an empiric therapy for febrile neutropenic patients refractory to antibacterial agents. Jpn J Chemother 54:125–128
Yanada M, Kiyoi H, Murata M, Suzuki M, Iwai M et al (2006) Micafungin, a novel antifungal agent, as empirical therapy in acute leukemia patients with febrile neutropenia. Intern Med 45:259–264
Toubai T, Tanaka J, Ota S, Shigematsu A, Shono Y et al (2007) Efficacy and safety of micafungin in febrile neutropenic patients treated for hematological malignancies. Intern Med 46:3–9
Tamura K, Urabe A, Yoshida M, Kanamaru A, Kodera Y et al (2009) Efficacy and safety of micafungin, an echinocandin antifungal agent, on invasive fungal infections in patients with hematological disorders. Leuk Lymphoma 50:92–100
Kubiak DW, Bryar JM, McDonnell AM, Delgado-Flores JO, Mui E et al (2010) Evaluation of caspofungin or micafungin as empiric antifungal therapy in adult patients with persistent febrile neutropenia: a retrospective, observational, sequential cohort analysis. Clin Ther 32:637–648
Goto N, Hara T, Tsurumi H, Ogawa K, Kitagawa J et al (2010) Efficacy and safety of micafungin for treating febrile neutropenia in hematological malignancies. Am J Hematol 85:872–876
Park JS, Kim DH, Choi CW, Jeong SH, Choi JH et al (2010) Efficacy and safety of micafungin as an empirical antifungal agent for febrile neutropenic patients with hematological diseases. Acta Haematol 124:92–97
Ascioglu S, Rex JH, de Pauw B, Bennett JE, Bille J et al (2002) Defining opportunistic invasive fungal infections in immunocompromised patients with cancer and hematopoietic stem cell transplants: an international consensus. Clin Infect Dis 34:7–14
ICH Harmonised Tripartite Guideline, Current step 4 version, dated 27 October 1994: Clinical Safety Data Management: definitions and Standards for Expedited Reporting E2A. http://www.ich.org/LOB/media/MEDIA436.pdf. Accessed: October 1994
Maertens J, Theunissen K, Verhoef G et al (2005) Galactomannan and computed tomography-based preemptive antifungal therapy in neutropenic patients at high risk for invasive fungal infection: a prospective feasibility study. Clin Infect Dis 41:1242–1250
Cordonnier C, Pautas C, Maury S et al (2009) Empirical versus preemptive antifungal therapy for high-risk, febrile, neutropenic patients: a randomized, controlled trial. Clin Infect Dis 48:1042–1051
Walsh TJ, Finberg RW, Arndt C, Hiemenz J, Schwartz C, National Institute of Allergy and Infectious Diseases Mycoses Study Group (1999) Liposomal amphotericin B for empirical therapy in patients with persistent fever and neutropenia. N Engl J Med 340:764–771
Boogaerts M, Winston DJ, Bow EJ, Garber G, Reboli AC, Schwarer AP et al (2001) Itraconazole Neutropenia Study Group. Intravenous and oral itraconazole versus intravenous amphotericin B deoxycholate as empirical antifungal therapy for persistent fever in neutropenic patients with cancer who are receiving broad-spectrum antibacterial therapy. Ann Intern Med 135:412–422
Walsh TJ, Pappas P, Winston DJ, Lazarus HM, Petersen F, Raffalli J et al (2002) National Institute of Allergy and Infectious Diseases Mycoses Study Group. Voriconazole compared with liposomal amphotericin B for empirical antifungal therapy in patients with neutropenia and persistent fever. N Engl J Med 346:225–234
Walsh TJ, Teppler H, Donowitz GR, Maertens JA, Baden LR et al (2004) Caspofungin versus liposomal amphotericin B for empirical antifungal therapy in patients with persistent fever and neutropenia. N Engl J Med 351:1391–1402
Obayashi T, Yoshida M, Mori T, Goto H, Yasuoka A et al (1995) Plasma 1,3-β-D-glucan measurement in diagnosis of invasive deep mycosis and fungal febrile episodes. Lancet 345:17–20
de Pauw B, Walsh TJ, Donnelly JP, Stevens DA, Edwards JE et al (2008) Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 46:1813–1821
Yoshida M (2006) Usefulness of determination of β-D-glucan in the diagnosis of deep mycosis—experience in Japan. Med Mycol 44(Sup 1):S185–S189
Acknowledgments
Financial support for this study was provided by Astellas Pharma Inc., Tokyo, Japan. The authors acknowledge all the institutions contributing to this study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yoshida, M., Tamura, K., Imamura, M. et al. Efficacy and safety of micafungin as an empirical antifungal therapy for suspected fungal infection in neutropenic patients with hematological disorders. Ann Hematol 91, 449–457 (2012). https://doi.org/10.1007/s00277-011-1316-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-011-1316-y