
Abstract
To elucidate the progression of gastric marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue (MALT) type, we analyzed a case presenting simultaneously with MALT lymphoma of the stomach and lung, and a gastric high-grade diffuse large lymphoma. The rearranged immunoglobulin heavy chain (IgH) variable regions were analyzed using a polymerase chain reaction (PCR)-based assay. Clonal relationship was shown between the gastric high-grade and the pulmonary low-grade lymphoma. The gastric MALT lymphoma was not related to the other manifestations. Translocation t(11;18) was not detected in the gastric high-grade lymphoma. MALT lymphomas at various locations and with different histologies may derive from a common precursor cell. Lymphomas at identical sites may have different stem cells.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Non-Hodgkin’s lymphoma (NHL) of the mucosa-associated lymphoid tissue (MALT) can be found in different organs such as the stomach, lung, and salivary glands, all of which are primarily free of lymphoid tissue. Although marginal zone B-cell lymphoma of MALT type (MALT lymphoma) have an indolent clinical course, dissemination within one organ or multifocal occurrence within different organs can be observed [11]. Since one-third of low-grade gastric MALT lymphoma samples shows high-grade components, the progression of low-grade to high-grade lymphomas has been suspected. To investigate the clonal relation between B cells, one can take advantage of the B-cell “fingerprint,” the specific rearranged immunoglobulin heavy chain (IgH) variable region (VH), as determined by polymerase chain reaction (PCR). Alternatively, karyotypic markers may be utilized. Since the translocation t(11;18) typical for MALT lymphoma was detected in extranodal low-grade MALT lymphoma but not in extranodal high-grade or nodal NHL, a progression from low- to high-grade MALT lymphoma was considered to be unlikely [1, 2, 4, 8]. Analysis for the rearranged IgH variable region revealed controversial results concerning clonal identity for the disseminated lesions as well as for low- and high-grade components [6, 7, 9].
To further elucidate the relationship of different MALT lymphoma manifestations, we report the molecular analysis of a patient who suffered from a low-grade lymphoma of MALT type of the lung, a low-grade gastric MALT lymphoma, and a gastric high-grade NHL. To obtain the clonal relationship between these different manifestations, we investigated the IgH rearrangement in the lymphoma cells by PCR for the framework (FR) 2 region VH fragment.
Materials and methods
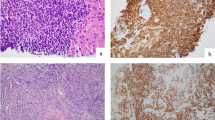
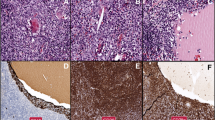
We analyzed tissue samples of a 69-year-old woman presenting with (1) a low-grade MALT lymphoma of the lung, (2) a low-grade gastric MALT lymphoma, and (3) a high-grade diffuse large B-cell NHL of the stomach. All histological slides were reviewed by one pathologist (M.S.).
The DNA was extracted from the formalin-fixed paraffin-embedded tissue with the commercially available Qiagen Tissue Kit (Qiagen, Hilden, Germany) as recommended by the manufacturer. The PCR assay for the FR2 fragment was carried out as described previously [12]. For fluorescence-stained fragment length analysis, the 5’ oligonucleotide primer was labeled with FAM dye. The PCR results were analyzed using a denaturating polyacrylamide gel, and the electrophoresis was carried out on an automated DNA sequencer ABI 377 (Perkin Elmer, Foster City, Calif., USA). The band distribution was evaluated using the Genescan software (Perkin Elmer, Foster City, Calif., USA). For detailed sequence analysis of the IgH variable region, the PCR fragments were cloned using the TA cloning Kit (Invitrogen, Groningen, The Netherlands). For each tumor sample, 7–20 clones were sequenced with the cycle sequencing method using the Big Dye Terminator Kit (Perkin Elmer, Foster City, Calif., USA) as recommended by the manufacturer. The sequence analysis was carried out on an automated DNA sequencer ABI 377 (Perkin Elmer, Foster City, Calif., USA). The determined VH alleles were aligned to published germline sequences using the Lasergene software (DNA-Star, Boston, Mass., USA) [3, 13]. The integrity of each DNA sample was demonstrated by amplification of the interferon-beta gene as a reference as described [12].
For the detection of the t(11;18)(q21;q21), interphase fluorescence in situ hybridization (FISH) was performed on a 3-µm-thick section from the biopsy of the high-grade gastric lymphoma. From both low-grade gastric and lung MALT lymphomas no tissue was left for FISH analyses. After deparaffinization with xylene and pretreatment with pepsin and RNAse, FISH was performed using PAC clones 59N7 and 166G16 as previously described [5]. This FISH assay detects the 5’API2-3’MLT fusion resulting from the t(11;18), which is evidenced by a fusion of the hybridization signals of PAC 166G16 (spans the API2 gene on chromosome 11) and PAC 59N7 (contains genomic sequences immediately downstream of the MLT gene on chromosome 18).
Results
A dominant monoclonal PCR band for the IgH rearrangement was shown for each tumor location (i.e., low-grade lung, low-grade stomach, high-grade stomach) (data not shown). When DNA sequence analysis was performed, and the sequences were aligned against each other, we found no major clonal identity/relation between the low-grade gastric MALT lymphoma and the high-grade gastric NHL (Fig. 1). Surprisingly, DNA sequence analysis revealed a clonal relationship between the high-grade gastric NHL and the low-grade lung MALT lymphoma (Fig. 1).

Clonal relationship of the IgH gene of three different lymphoma manifestations in one patient. The upper part shows the allele distribution for the low-grade MALT lymphoma of the lung, the high-grade gastric NHL, and the low-grade gastric MALT lymphoma. In the lower part the grade of homology between the detected alleles and the germline sequences is shown. In all cases a minority of determined sequences revealed nonfunctional rearrangements for the IgH variable region. The second line of the lower part shows the relationship between the analyzed clones and the detected alleles. The nonfunctional rearrangements are not shown. Thus, the number of given clones does not equal the number of analyzed clones
On detailed analysis, in the gastric MALT lymphoma sample two different VH alleles, VH3–15 (five of nine clones) and VH3–30.5 (two of nine clones) were detected. The allele VH3–15, which was dominant in the low-grade gastric MALT lymphoma, was found in only 1 of 20 clones analyzed from the high-grade lesion of the stomach (Fig. 1). In this sample, however, two dominant clones were detected. For one of these a clear assignment was not possible, since the sequence showed the identical grade of homology with VH4–61 and VH4–59 alleles. In addition, the VH3–23 allele was detected in 3 of 20 of the analyzed clones from the high-grade NHL sample. The allele VH4–61/VH4–59 and the VH3–23 were also and solely found in the lung MALT lymphoma sample.
Figure1 shows the distribution of the alleles and the relationship between the different lymphoma samples in this patient. The translocation t(11;18) was not demonstrated in the analyzed material of the high-grade gastric lymphoma in our case.
Discussion
There have been discrepant results with regard to the clonal relationship between low- and high-grade extranodal lymphomas of MALT type [1, 2, 4, 7]. In the patient presented here suffering from extranodal lymphomas at different locations, no relation was found between the low-grade gastric MALT lymphoma and the low-grade MALT lymphoma of the lung. The low-grade gastric MALT lymphoma showed no clonal relation to the high-grade gastric NHL. Surprisingly, we found the vast majority of clones to be identical between the low-grade MALT lymphoma of the lung and the high-grade gastric NHL. These results may point to a clonal independence between both the low-grade lymphoma manifestation in the lung and the gastric MALT lymphoma. The manifestation of the gastric high-grade NHL was therefore not a result of a progression from the gastric MALT lymphoma. The lung MALT lymphoma and the gastric high-grade NHL showed almost identical allelic distributions. Therefore, the high-grade gastric NHL may have emerged from the low-grade MALT lymphoma of the lung in this patient.
The absence of the translocation t(11;18) in extranodal high-grade MALT lymphoma may suggest an independent development of simultaneous low- and high-grade MALT lymphoma [5, 7]. This is challenged by the patient presented whose data point to a more complex biology of MALT lymphomas. It cannot be excluded that t(11;18)-positive MALT lymphomas exhibit behavior of progression distinct from negative cases. t(11;18)-positive MALT lymphomas usually do not seem to transform to higher histological grades (for a review, see [10]). The absence of the t(11;18) in the high-grade gastric lymphoma analyzed in our patient would support this assumption. Since too few tissue was available for analysis, translocation t(11;18) could not be analyzed in the low-grade lesions of the lung as well as of the stomach.
In conclusion, the case presented here points to a more complex biology of the phenomenon of tumor progression of extranodal lymphomas, making it likely that low-grade lesions may indeed progress into high grades, even at different locations.
References
Akagi T, Motegi M, Tamura A, Suzuki R, Hosokawa Y, Suzuki H, Ota H, Nakamura S, Morishima Y, Taniwaki M, Seto M (1999) A novel gene, MALT1 at 18q21, is involved in t(11;18)(q21;q21) found in low-grade B-cell lymphoma of mucosa-associated lymphoid tissue. Oncogene 18:5785–5794
Auer IA, Gascoyne RD, Connors JM, Cotter FE, Greiner TC, Sanger WG, Horsman DE (1997) t(11;18)(q21;q21) is the most common translocation in MALT lymphomas. Ann Oncol 8:979–985
Cook GP, Tomlinson IM, Walter G, Riethman H, Carter NP, Buluwela L, Winter G, Rabbitts TH (1994) A map of the human immunoglobulin VH locus completed by analysis of the telomeric region of chromosome 14q. Nat Genet 7:162–168
Dierlamm J, Baens M, Wlodarska I, Stefanova-Ouzounova M, Hernandez JM, Hossfeld DK, De Wolf-Peeters C, Hagemeijer A, Van den Berghe H, Marynen P (1999) The apoptosis inhibitor gene API2 and a novel 18q gene, MLT, are recurrently rearranged in the t(11;18) associated with the mucosa-associated lymphoid tissue lymphomas. Blood 93:3601–3609
Dierlamm J, Baens M, Stefanova-Ouzounova M, Hinz K, Wlodarska I, Maes B, Steyls A, Driessen A, Verhoef G, Gaulard P, Hagemeijer A, Hossfeld DK, De Wolf-Peeters C, Marynen P (2000) Detection of t(11;18)(q21;q21) by interphase fluorescence in situ hybridization using API2 and MLT specific probes. Blood 96:2215–2218
Du MQ, Xu CF, Diss TC, Peng HZ, Wotherspoon AC, Isaacson PG, Pan LX (1996) Intestinal dissemination of gastric mucosa-associated lymphoid tissue lymphoma. Blood 88:4445–4451
Matolcsy A, Nagy M, Kisfaludy N, Kelenyi G (1999) Distinct clonal origin of low-grade MALT-type and high-grade lesions of a multifocal gastric lymphoma. Histopathology 34:6–8
Ott G, Katzenberger T, Greiner A, Kalla J, Rosenwald A, Heinrich U, Ott MM, Muller-Hermelink HK (1997) The t(11;18)(q21;q21) chromosome translocation is a frequent and specific aberration in low-grade but not high-grade malignant non-Hodgkin’s lymphomas of the mucosa associated lymphoid tissue (MALT)-type. Cancer Res 57:3944–3948
Peng H, Du M, Diss TC, Isaacson PG, Pan L (1997) Genetic evidence for a clonal link between low and high-grade components in gastric MALT B-cell lymphoma. Histopathology 30:425–429
Starostik P, Patzner J, Greiner A, Schwarz S, Kalla J, Ott G, Muller-Hermelink HK (2002) Gastric marginal zone B-cell lymphomas of MALT type develop along 2 distinct pathogenetic pathways. Blood 99:3–9
Thieblemont C, Berger F, Dumontet C, Moullet I, Bouafia F, Felman P, Salles G, Coiffier B (2000) Mucosa associated lymphoid tissue lymphoma is a disseminated disease in one third of 158 patients analyzed. Blood 95:802–806
Thiede C, Alpen B, Morgner A, Schmidt M, Ritter M, Ehninger G, Stolte M, Bayerdorffer E, Neubauer A (1998) Ongoing somatic mutations and clonal expansion after sure of Helicobacter pylori infection in gastric mucosa associated lymphoid tissue (MALT) B-cell lymphoma. J Clin Oncol 16:3822–3831
Tomlinson IM, Walter G, Marks JD, Llewelyn MB, Winter G (1992) The repertoire of human germline VH sequences reveals about fifty groups of VH segments with different hypervariable loops. J Mol Biol 227:776–798
Author information
Authors and Affiliations
Corresponding author
Additional information
Supported in part by Deutsche Krebshilfe (70–2251-Ne1) and the Kempkes Stiftung
Rights and permissions
About this article
Cite this article
Alpen, B., Wündisch, T., Dierlamm, J. et al. Clonal relationship in multifocal non-Hodgkin’s lymphoma of mucosa-associated lymphoid tissue (MALT). Ann Hematol 83, 124–126 (2004). https://doi.org/10.1007/s00277-003-0763-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00277-003-0763-5