
Abstract
Purposes
To verify the relationship between muscle volume and muscular strength of different cross-sectional areas (CSAs) of the gluteus maximus and medius, and to clarify the effective evaluation index.
Methods
Twenty healthy adults were enrolled in this cross-sectional study. Magnetic resonance images were evaluated, and CSAs of the gluteus maximus and medius were calculated. Calculation sites were the peak CSA, lowest end of the sacroiliac joint CSA, and just above the femoral head CSA. Muscle volume and muscular strength were measured. The correlation between muscular CSA, muscle volume, and muscular strength was verified using Pearson’s correlation coefficient (p < 0.05). One-way analysis of variance and the Tukey–Kramer test were used to verify differences in each CSA (p < 0.05).
Results
A significantly positive correlation was found between muscular CSA, muscle volume, and muscular strength of both muscles (p < 0.05). For the gluteus maximus, the muscular CSA calculated just above the femoral head showed a significantly larger value than that calculated at the lowest end of the sacroiliac joint (p < 0.05). For the gluteus medius, the peak CSA and muscular CSA calculated at the lowest end of the sacroiliac joint were significantly larger than that calculated just above the femoral head (p < 0.05).
Conclusions
The maximum CSA of the gluteus maximus was found just above the femoral head and that of the gluteus medius was near the lowest end of the sacroiliac joint; hence, CSAs should be calculated at these sites. The CSA reflected muscle volume and strength.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Background
In physical therapy, evaluation of the cross-sectional area (CSA) is an objective assessment of the muscles. However, the measurement site recommended for measuring the CSA of muscles is unclear. Orthopedic diseases often exhibit dysfunction, and representative symptoms are muscle weakness. Therefore, in order for patients to reacquire motion, evaluation of muscle mass is often aimed at the improvement of muscle function.
To objectively evaluate the muscles, the muscle volume can be evaluated based on an image. In case of invasive treatment, image evaluation of an osteoarthritic hip is often performed with computed tomography (CT) or magnetic resonance imaging (MRI), and the muscular CSA and muscle volume are calculated using the obtained data. Moreover, in evaluating muscle volume, the tracing method is used. The tracing method is defined as the calculation of the muscle volume by measuring the CSA at each slice and then adding them, and many studies have used this method [2, 5, 9, 15]. Furthermore, to calculate muscle volume, it is necessary to calculate the CSA from all slices. However, muscle volume is reported to be stronger than the CSA and to reflect peak muscular strength [4]. Further, a single evaluation of CSA cannot be used to determine the shape of the muscle [6], although the muscle volume reflects the shape of the muscle more than the CSA [13].
The presence of a metal in the body after surgery may affect the calculation of the CSA [7, 10]. Therefore, it is important to clarify the effective evaluation index of CSA that reflects muscular strength and muscle volume. However, in some studies, the relationships between muscular strength and muscle volume have been reported with CSA as an evaluation index, but the recommended sites for evaluation have not been clarified [9]. Muscle volume strongly reflects muscular strength and is calculated by adding the muscle CSA. Therefore, we think that muscular strength and muscle volume may strongly reflect a larger cross-sectional area.
The purposes of this study were to verify the relationship between muscle volume and muscular strength of different muscular CSAs at measurement sites by focusing on the gluteus medius and gluteus maximus, and to clarify the effective evaluation index.
Methods
Subjects
The subjects were 20 healthy adult volunteers who were selected randomly. The subjects were free from any diseases, such as orthopedic, heart, and neurologic diseases, surgery, psychosis.
The study protocol was explained to all participants verbally and in writing, and written consent was obtained from all participants before the measurement commenced in Niigata Bandai Hospital. This study was approved by Niigata Bandai Hospital (approval number 54).
Measurement parameters
The target muscles were the gluteus maximus and gluteus medius, which have different innervations. We measured these muscles because they are the primary acting muscles of the hip extensors and abductors. Parameters measured and analyzed were muscle volume of the gluteus maximus and gluteus medius, CSA measured at the lowest end of the sacroiliac joint, CSA measured just above the femoral head, peak CSA, and muscular strength in extension, abduction, internal rotation, and external rotation.
For muscular strength, the main directions of movement of the gluteus maximus were extension and external rotation and those of the gluteus medius were abduction and internal rotation. The stance or skill side was analyzed as well [2].
MRI measurement and calculation method of muscle volume and CSA
Participants were screened for contraindications against MRI by skilled MRI technicians. MRI was performed using an MRI system (Signa HDe, GE Healthcare, Waukesha, WI, USA). The imaging conditions were as follows: coronal T1 fast-spin echo, field of view 400 × 400, 3 mm slice gapless, echo time 10.1 ms, repetition time 450 ms, and voxel size 320/400 × 192/400 × 3.0 ms.
Participants were in the supine position and remained steady so that the line connecting the upper anterior iliac spines on both sides was perpendicular to the bed. Moreover, the position of the hip joint was taken between the inside and the outside of the hip joint.
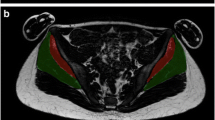
After magnetic resonance images were analyzed using ZedHip (Lexi Co., Ltd., Tokyo, Japan), a cross-section of each muscle was traced, and its CSA was calculated. The tracing method was performed by measuring the periphery of the target muscle on the image and calculating the CSA [5, 15]. All CSAs calculated from the origin and endpoint of the muscle were added to determine muscle volume [5, 15]. The gluteus maximus and medius were identified according to the report of Zacharias et al. [15] (Fig. 1).

Gluteus maximus and gluteus medius. Magnetic resonance image acquired at the lowest end of the sacroiliac joint
Measurement of muscular strength
Muscular strength was measured using a handheld dynamometer (µTas F-1, Anima, Tokyo, Japan) on the same day as the MRI examination. For muscular strength, the main directions of movement of the gluteus maximus were extension and external rotation and those of the gluteus medius were abduction and internal rotation (Fig. 2). In the muscular strength measurement, the limb position was based on the method of Thorborg et al. [12]. They reported various measurements of limb positions. In the present study, the supine and prone positions were adopted during the measurement (Fig. 2). The task was maximal isometric contraction for 5 s, and the peak value was taken as the representative value of each subject from the two measured values.

Measurement method of muscle strength
Statistical methods
All the above-mentioned parameters were computed for each subject, averaged over the entire sample, and reported as average ± standard deviation. To verify the relationship between the muscle CSA, volume, and strength measured at each height, the correlation of each muscle volume, CSA, and strength was tested using Pearson’s correlation coefficient. Differences in measured CSAs were verified using one-way analysis of variance and the Tukey test (p < 0.05). SPSS, version 21 (IBM Corp., Armonk, NY, USA) was used to perform all the statistical analyses. The significance level was set at p < 0.05.
Results
The study subjects were aged 26.7 ± 2.1 years, with a height of 165.3 ± 9.3 cm and body weight of 55.5 ± 11.5 kg. The muscle volume of the gluteus maximus was 726.2 ± 9.6 cm3. The CSA with the largest cross-section was 4.6 ± 0.9 cm2, CSA measured at the lowest end of the sacroiliac joint was 2.7 ± 0.9 cm2, and CSA measured at the femoral head was 4.3 ± 0.8 cm2. Values of muscular strength were 21.5 ± 6.2 kgf in extension and 11.7 ± 4.0 kgf in external rotation.
The muscle volume of the gluteus medius was 313.0 ± 77.2 cm3. The largest CSA was 3.3 ± 0.6 cm2. The CSA measured at the lowest end of the sacroiliac joint was 3.1 ± 0.7 cm2, and the CSA at the femoral head was 1.7 ± 0.5 cm2. Values of muscular strength were 12.5 ± 4.0 kgf in abduction and 13.0 ± 4.7 kgf in internal rotation.
Muscle volume, each muscle CSA, and muscular strength of the gluteus muscles all showed a significant positive correlation. In particular, the peak CSA of the gluteus maximus and that just above the femoral head showed extensional strength (peak: r = 0.577, p < 0.05; just above the femoral head: r = 0.601, p < 0.05) and external rotation (peak: 0.643, p < 0.05; just above the femoral head: r = 0.541, p < 0.05).
In addition, the peak CSA and CSA above the femoral head showed a very strong correlation with volume (peak: r = 0.928, p < 0.05; just above the femoral head: r = 0.926, p < 0.05) (Table 1). The peak CSA and CSA at the lowest end of the sacroiliac joint of the gluteus medius showed abductor muscular strength (peak: r = 0.846, p < 0.05; lowest end of the sacroiliac joint: r = 0.804, p < 0.05 and peak: r = 0.735, p < 0.05; lowest end of the sacroiliac joint: r = 0.686, p < 0.05, respectively). Furthermore, the peak CSA and CSA at the lowest end of the sacroiliac joint showed a very strong correlation with volume (peak: r = 0.959, p < 0.05; just above the femoral head: r = 0.952, p < 0.05) (Table 1).
The peak CSA and CSA right above the femoral head showed a very strong correlation with peak volume (r = 0.928, p < 0.05; just above the femoral head: r = 0.926, p < 0.05). The peak CSA and CSA at the lowest end of the sacroiliac joint showed a very strong correlation with volume (peak: r = 0.959, p < 0.05; just above the femoral head: r = 0.952, p < 0.05) (Table 1).
For the CSA of the gluteus maximus, the CSA just above the femoral head and peak CSA were significantly larger than the CSA measured at the lowest end of the sacroiliac joint (p < 0.05) (Table 2).
Moreover, in the gluteus maximus, the peak CSA and muscle CSA obtained just above the femoral head show no significant difference (Table 2). The peak area of the gluteus medius and CSA obtained at the lowest end of the sacroiliac joint were not significantly different from the CSA of the femoral head (Table 2).
Discussion
As a method of objectively evaluating the muscles, a CSA can be calculated using images obtained by MRI and CT. However, the measurement location of the muscle CSA to be evaluated is unclear. Our finding can be applied to objectively assess simple muscle mass in clinical studies in the field of physical therapy.
Muscle volume, CSA, and muscular strength of the gluteus muscles showed a significant positive correlation. The result that muscle mass evaluation indexes such as the CSA and muscle volume showed a positive correlation with muscular strength support results of previous studies [8, 11]. Moreover, previous studies evaluated and calculated the CSA of the gluteus maximus and medius [1, 9, 14]. However, no reports have verified the correct calculation of the CSA. A novel point of this study was that we verified the muscle CSA to be measured, which has not been elucidated so far. In the present study, muscle CSA was calculated at the lowest end of the sacroiliac joint, just above the femoral head, and at its peak, and the relationship between muscular strength and muscle volume was verified. Each CSA of the gluteus maximus showed a positive correlation with muscular strength, but the muscle CSA calculated just above the femoral head in the gluteus medius showed a weak correlation with muscular strength during abduction. This result suggests that muscular strength may not be reflected sufficiently depending on the part of the CSA measured. The stop portion of the gluteus medius is the greater trochanter, and the muscle CSA calculated just above the femoral head is closer to the greater trochanter, i.e., the stop portion, than that calculated at the lowest end of the sacroiliac joint.
We think that measuring larger areas is more likely to reflect muscular strength and volume. In fact, the gluteus maximus also showed a larger correlation with the CSA measured just above the femoral head, indicating a large CSA. Regarding the CSA of the gluteus maximus, the peak CSA was not significantly different from the CSA of the femoral head as the largest section of the CSA. Therefore, it was suggested that the maximum CSA of the gluteus maximus may exist around the femoral head. For the CSA of the gluteus medius, the peak CSA and CSA at the lowest end of the sacroiliac joint were significantly larger than the CSA measured at the femoral head. Therefore, the maximum CSA of the gluteus maximus could be obtained by measuring it at the lowest end of the sacroiliac joint.
CSA above the femoral head strongly reflects the volume in the gluteus maximus, and CSA of the lowest end of the sacroiliac joint of the gluteus muscle strongly reflects the volume in the gluteus medius. Given that we verified that the CSA reflects muscle volume and muscular strength, we think that we could clarify the most important evaluation index. CSA obtained from the mentioned landmarks that can be used to calculate the CSA of larger muscles showed a significant positive correlation with volume and muscle strength, reflecting muscle volume and performance.
Although we targeted healthy subjects, Flack et al. [3] studied patients with lateral hip pain and the relationship between muscle pain and muscle volume. Flack et al. measured the gluteus medius and tensor of fascia lata. We measured the gluteus medius and can compare our findings with those of Flack et al.
In the previous study by Flack et al., there was no significant difference in the muscle volume between patients with lateral hip pain and the control group. In addition, they reported that the volume of the gluteus medius ranged from 278 to 296 cm3. The volume of the gluteus medius measured in our study in healthy adults was 313 cm3. Further, the average age of the Flack et al.’s case group and control group was 55 years, and since it is older than the age of our study patients, it is necessary to consider the affect of age; the muscle volume of the gluteus medius measured in our study was large. Based on these facts, the muscle volume may change with age. Therefore, it is necessary to clarify volume and muscle function by age and the measurement of each case.
When evaluating a patient, pain may occur during the measurement. Furthermore, it is sometimes difficult to evaluate images after surgery due to halation. Therefore, we believe it is necessary to devise an evaluation method that is not affected by the measurement timing or patient’s physical condition. Considering the relationship between patient’s muscle function, muscle volume, and nutritional status, appropriate prognostic prediction may become possible.
Some limitations of this study should be noted. First, in this study, we assessed only the gluteus maximus and gluteus medius. Therefore, it is necessary to assess the gluteus minimus and tensor fascia of the abductor muscle group in the future. Secondly, this study included healthy subjects and did not include patients. Therefore, it is unclear whether the results obtained from this finding can be generalized to patients. Conducting the same verification even for patients in the future is necessary.
The findings obtained in this study clarify the sites for calculating the CSA of the gluteus maximus and medius. Furthermore, CSAs of the gluteus maximus and gluteus medius reflect the volume and muscle force, so it is possible to objectively evaluate the index reflecting muscle strength and muscle force. This finding will make clinical muscle assessment easier.
References
Ahedi H, Aitken D, Scott D, Blizzard L, Cicuttini F, Jones G (2014) The association between hip muscle cross-sectional area, muscle strength, and bone mineral density. Calcif Tissue Int 95:64–72. https://doi.org/10.1007/s00223-014-9863-6
Bullock-Saxton JE, Wong WJ, Hogan N (2001) The influence of age on weight-bearing joint reposition sense of the knee. Exp Brain Res 136:400–406. https://doi.org/10.1007/s002210000595
Flack NA, Meikle GR, Reddy M, Nicholson HD, Woodley SJ (2012) Hip abductor muscle volume in women with lateral hip pain: a case-controlled study. Surg Radiol Anat 34:847–855. https://doi.org/10.1007/s00276-012-0970-7
Fukunaga T, Miyatani M, Tachi M, Kouzaki M, Kawakami Y, Kanehisa H (2001) Muscle volume is a major determinant of joint torque in humans. Acta Physiol Scand 172:249–255. https://doi.org/10.1046/j.1365-201x.2001.00867.x
Grimaldi A, Richardson C, Durbridge G, Donnelly W, Darnell R, Hides J (2009) The association between degenerative hip joint pathology and size of the gluteus maximus and tensor fascia lata muscles. Man Ther 14:611–617. https://doi.org/10.1016/j.math.2008.11.002
Grimaldi A, Richardson C, Stanton W, Durbridge G, Donnelly W, Hides J (2009) The association between degenerative hip joint pathology and size of the gluteus medius, gluteus minimus and piriformis muscles. Man Ther 14:605–610. https://doi.org/10.1016/j.math.2008.11.002
Hartzman S, Gold RH (1989) MRI atlas of the musculoskeletal system. Martin Dunitz Ltd., London
O’Brien TD, Reeves ND, Baltzopoulos V, Jones DA, Maganaris CN (2009) Strong relationships exist between muscle volume, joint power and whole-body external mechanical power in adults and children. Exp Physiol 94:731–738. https://doi.org/10.1113/expphysiol.2008.045062
Rasch A, Byström AH, Dalen N, Berg HE (2007) Reduced muscle radiological density, cross-sectional area, and strength of major hip and knee muscles in 22 patients with hip osteoarthritis. Acta Orthop 78(4):505–510. https://doi.org/10.1080/17453670710014158
Seeger LL, Lufkin RB (1989) MRI atlas of the musculoskeletal system. Martin Dunitz Ltd., London
Suetta C, Aagaard P, Rosted A, Jakobsen AK, Duus B, Kjaer M, Magnusson SP (2004) Training-induced changes in muscle CSA, muscle strength, EMG, and rate of force development in elderly subjects after long-term unilateral disuse. J Appl Physiol 97:954–1961. https://doi.org/10.1152/japplphysiol.01307.2003
Thorborg K, Petersen J, Magnusson SP, Hölmich P (2010) Clinical assessment of hip strength using a hand-held dynamometer is reliable. Scand J Med Sci Sports 20:493–501. https://doi.org/10.1111/j.1600-0838.2009.00958.x
Tracy BL, Ivey FM, Jeffrey Metter E, Fleg JL, Siegel EL, Hurley BF (2003) A more efficient magnetic resonance imaging-based strategy for measuring quadriceps muscle volume. Med Sci Sports Exerc 35:425–433. https://doi.org/10.1249/01.MSS.0000053722.53302.D6
Uemura K, Takao M, Sakai T, Nishii T, Sugano N (2016) Volume increases of the gluteus maximus, gluteus medius, and thigh muscles after hip arthroplasty. J Arthroplasty 31:906–912. https://doi.org/10.1016/j.arth.2015.10.036
Zacharias A, Pizzari T, English DJ, Kapakoulakis T, Green RA (2016) Hip abductor muscle volume in hip osteoarthritis and matched controls. Osteoarthr Cartil 24:1727–1735. https://doi.org/10.1016/j.joca.2016.05.002
Acknowledgements
DH would like to express his appreciation to his English teacher Mr. Takao Kobayashi, and gratefulness to everyone in the radiology department of the Niigata Bandai Hospital. We would also like to thank Editage (http://www.editage.jp) for English language editing.
Funding
This study did not receive any funding or financial support.
Author information
Authors and Affiliations
Contributions
DH: Data collection or management, analysis, and manuscript writing/editing. IM: Protocol/project development. NI: Manuscript writing/editing. DM: Protocol/project development. YS: Data collection or management. YH: Data analysis. HS: Data analysis. YD: Data collection or management. NE: Protocol/project development.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study was approved by Niigata Bandai Hospital’s ethics committee (Approval number 54). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Rights and permissions
About this article

Cite this article
Homma, D., Minato, I., Imai, N. et al. Investigation on the measurement sites of the cross-sectional areas of the gluteus maximus and gluteus medius. Surg Radiol Anat 41, 109–115 (2019). https://doi.org/10.1007/s00276-018-2099-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00276-018-2099-9