
Abstract
The purpose of this study was to investigate the radiation doses to the lower extremities in interventional radiology suites and evaluate the benefit of installation of protective lead shielding. After an alarmingly increased dose to the lower extremity in a preliminary study, nine interventional radiologists wore thermoluminescent dosimeters (TLDs) just above the ankle, over a 4-week period. Two different interventional suites were used with Siemens undercouch fluoroscopy systems. A range of procedures was carried out including angiography, embolization, venous access, drainages, and biopsies. A second identical 4-week study was then performed after the installation of a 0.25-mm lead curtain on the working side of each interventional table. Equivalent doses for all nine radiologists were calculated. One radiologist exceeded the monthly dose limit for a Category B worker (12.5 mSv) for both lower extremities before lead shield placement but not afterward. The averages of both lower extremities showed a statistically significant dose reduction of 64% (p < 0.004) after shield placement. The left lower extremity received a higher dose than the right, 6.49 vs. 4.57 mSv, an increase by a factor of 1.42. Interventional radiology is here to stay but the benefits of interventional radiology should never distract us from the important issue of radiation protection. All possible measures should be taken to optimize working conditions for staff. This study showed a significant lower limb extremity dose reduction with the use of a protective lead curtain. This curtain should be used routinely on all C-arm interventional radiologic equipment.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
The rapid development of imaging technology has contributed to the growth of interventional radiology (IR). Continuing advances in digital imaging enable new and complex operations, such as vascular and hepatobillary interventional procedures that were impossible in the past. Improvements in catheters, guide wires, and stents have expanded the role of the radiologist, placing them at the forefront of patient treatment. IR accounts for more than 75% of all “minimally invasive” procedures [1]. Reduced hospitalization costs and low risk have contributed to its worldwide popularity and expansion [2, 3].
Most IR procedures are performed under fluoroscopic, CT, or ultrasound guidance. Fluoroscopic techniques, in particular, expose patients and staff to long screening times, from 30 min to up to 4 h, depending on the complexity of the procedure. Flouroscopy dose rates can be in excess of 100 mGy per minute [4]. Thus interventionalists and other staff members work in an environment with the potential for considerable occupational exposure to radiation.
There is growing concern about staff exposure with increasing IR workload. Some radiologists now approach the legal limits for radiation exposure and could be categorized as “classified workers.” These personnel, liable to receive an effective dose of more than 6 mSv per year, are classified as Category A workers [5, 6]. Other staff members at risk include assistants, nurses, and radiographers. Interventionalists, however, receive the highest radiation doses because of their close proximity to the x-ray tube. This consists of scatter and, occasionally, primary beam radiation. The dose received by other staff members is principally caused by scatter.
The ICRP dose limit for extremities for a Category B worker is 150 mSv per year (or 12.5 mSv per month). A number of previous studies conducted at Beaumont Hospital measured doses to different parts of the body and found that the lower extremities received a disproportionately high dose [7]. We conducted this study to further quantify the doses to the legs and measure the dose reduction after effective shielding had been put in place.
Material and Methods
Over a 4-week period, nine interventional radiologists wore LiF-7 thermoluminescent dosimeters (TLDs; NE Technology Limited, Reading, UK) just above the ankle anteriorly on both lower extremities (See Table 1 for dosimeter characteristics). A range of IR procedures was performed including angiography, embolizations. and drainages. Our two main interventional suites were equipped with Siemens Angioskop C-Arm undercouch fluoroscopy systems (Siemens Medical Solutions, Forchheim, Germany). TLDs were collected at the end of the 4-week period and read by GLOSRAD (Medical Physics Department, Gloucestershire Royal Hospital, Gloucester, UK).
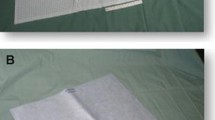
Subsequently, a second similar study was performed with the same radiologists after installation of a 0.25-mm protective lead curtain shield along the working side of the interventional table during all procedures (See Fig. 1). As shown in Fig. 1, the protective lead curtain is hung from the side of the fluoroscopy table to the floor. It is used only on the working side of the table during a procedure but is detachable for use on the opposite side if required. Again, TLDs were collected and read at the end of a 4-week period. All statistical analyses were performed on Jandel SigmaStat statistical software version 2.0. (Jandel GmbH, Erkrath, Germany).

Protective lead curtain along the side of an interventional fluoroscopy table

Table and diagram of equivalent doses (mSv) before and after shield placement
Results
Equivalent doses for all nine radiologists were calculated and are shown in Fig. 2 and Table 2. Before shield placement the mean right lower extremity dose was 4.57 mSv (range: 12.3–0.3 mSv), and the left lower extremity mean was 6.50 mSv (range: 1.7–15.7 mSv). One radiologist exceeded the monthly dose limit for a Category B worker (12.5 mSv) for both lower extremities before lead shield placement but not afterward. After shield placement the right lower extremity mean was 1.64 mSv (range: 0–5.0 mSv), and the left leg mean was 2.31 mSv (range: 6.6–0.3 mSv). The average dose reduction for both legs after shield placement was 3.55 mSv, a reduction factor of 2.8. or 64% (See Fig. 2).
When analyzed separately, using Student’s t-test, the left lower extremity dose reduction was statistically significant (mean, 6.50 vs. 2.31; p < 0.045). The right lower limb reduction was just outside statistical significance (mean, 4.57 vs. 1.64 mSv; p < 0.077). However, when the averages of both lower extremities were analyzed using the Wilcoxon signed rank test there was an overall statistically significant dose reduction between the two groups (p < 0.004).
Discussion
Many recent studies have focused attention on staff radiation doses to the eyes, hands, thyroid, and trunk [8–10]. There are many products available for radiation shielding of these areas for both staff and patients [11, 12]. The dose to the lower extremity, however, has only been covered in the literature by a few articles [13].
Radiologists usually fall into Category B workers and are liable to receive >1 mSv but <6 mSv per year [5, 6]. Any worker receiving more than this must be classified as Category A. The reason for the increased dose is then investigated by the national radiation protection authority and the worker must undergo yearly medical examinations and close radiation dose monitoring. One of the most significant findings of this study was the discovery of alarmingly high doses to the lower limbs, which exceeded the Category B limit of 12.5 mSv per month [14] for one operator. Immediate action was taken to install protective shielding in the interventional suites. A 0.25-mm lead curtain was installed on the working side of the screening table. The additional study, performed after the protective curtain was installed, demonstrated a reduction in lower extremity doses of 64%. All radiologists were well within the Category B limit after placement of the protective curtain.
The results are explained by the distribution of significant scattered radiation by the undercouch x-ray tube on to the radiologist’s legs, which are not usually covered by lead aprons. Doses are higher on the left leg. This is explained by most radiologists’ being right-handed, with the left leg being closer to the x-ray tube during most interventional procedures. It should also be borne in mind that the protective lead curtain is a detachable device which should be moved to the side of the interventional table that the interventionalist is working on. Our results are similar to those of other studies in this area, showing an alarming dose to the lower extremities, which was significantly reduced by the use of a protective shield [13].
IR is here to stay but the benefits of IR should never distract us from the important issue of radiation protection. All possible measures should be taken to optimize working conditions for staff. The ALARA (as low as reasonably achievable) principle must govern all fluoroscopically guided procedures [14, 15]. All staff working with radiation need to be aware of the methods of reduction of staff radiation exposure, which include appropriate radiographic techniques, equipment requirements, personal practices, and protective measures. There is no substitute for individual awareness in minimizing exposure to radiation. Furthermore, familiarity with radiation protection legislation and directives is essential for staff working with ionizing radiation.
The latest piece of Irish radiation legislation is the Statutory Instrument 478 [16], which implemented the 97/43 Euratom Directive [17] and deals with equipment issues such as adequate shielding.
This study has shown the need for increased awareness in the area of radiation protection and the requirement for ongoing staff monitoring to ensure a safe working environment in interventional radiology. It led to a change in practice through the installation of protective curtains on all our fluoroscopy units, with a dose reduction of 64%.
Departments should insist on the inclusion of protective lower extremity lead shielding as a standard part of the angiography table when purchasing fluoroscopy systems.
References
Merland J (1992) Interventional radiology: organising models. Lecture at the Berzelius Symposium, Swedish Society of Medicine, Stockholm
McBride KD, et al. (1997) A comparative analysis of radiological and surgical placement of central venous catheters. CardioVasc Intervent Radiol 20(1):17–22
Noh HM, et al. (1999) Cost comparison of radiologic versus surgical placement of long-term hemodialysis catheters. AJR 172(3):673–675
Marx MV, Ellis JH (1996) Radiation protection of the hand in interventional radiology: Should it fit like a glove? Radiology 200(1):24–25
The Council of the European Union (1996) European Directive 96/29 Euratom
European Communities Medical Ionising Radiation Protection, (2000) S.I. No. 125
Al-Hashimi H, M.L., McGee A, Varghese JC, Lee MJ (1997) Interventional radiology: a case for not putting your best foot forward. 83rd Scientific Assembly and Annual Meeting RSNA
Synowitz M, Kiwit J (2006) Surgeon’s radiation exposure during percutaneous vertebroplasty. J Neurosurg Spine 4(2):106–109
Muller LP, et al. (1998) Radiation exposure to the hands and the thyroid of the surgeon during intramedullary nailing. Injury 29(6):461–468
Tan GA, Van Every B (2005) Staff exposure to ionizing radiation in a major trauma centre. Aust NZ J Surg 75(3):136–137
Colombo P, et al. (2004) Evaluation of the efficacy of a bismuth shield during CT examinations. Radiol Med (Torino) 108(5–6):560–568
Hopper KD, et al. (2001) Radioprotection to the eye during CT scanning. Am J Neuroradiol 22(6):1194–1198
Whitby M, Martin CJ (2003) Radiation doses to the legs of radiologists performing interventional procedures: Are they a cause for concern? Br J Radiol 76(905):321–327
ICRP (1991) Recommendation of the IRCP (Report 26). Pergamon Press, Oxford
Brateman L (1999) Radiation safety considerations for diagnostic radiology personnel. Radiographics 19(4):1037–1055
European Communities Medical Ionising Radiation Protection (2002) S.I. No. 478
The Council of the European Union (1997) European Directive 97/43 Euratom
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Shortt, C.P., Al-Hashimi, H., Malone, L. et al. Staff Radiation Doses to the Lower Extremities in Interventional Radiology. Cardiovasc Intervent Radiol 30, 1206–1209 (2007). https://doi.org/10.1007/s00270-007-9071-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00270-007-9071-0