
Abstract
Purposes
We sought to determine the usefulness and the disadvantages of the navigation in medial opening wedge high tibial osteotomy (MOWHTO) compared to the conventional technique, in terms of target coronal alignment achievement, tibial slope maintenance, radiation exposure and operative time.
Methods
We retrospectively compared 40 knees treated with navigated MOWHTO by one surgeon with 20 knees treated with conventional MOWHTO by another surgeon. Screw length of the plate was predetermined using validated simple algorithms only in the navigation group to facilitate the operation. The acceptable range of the postoperative coronal alignment was defined as 2°–6° of the mechanical tibiofemoral angle (mTFA) and 55 %–70 % of the weight loading line coordinate (WLL). The proportion of the coronal alignment outlier, posterior tibial slope change, fluoroscopy time and operative time were compared.
Results
The coronal alignment outliers were fewer in the navigation group, but the differences were not significant (mTFA outlier 18 % vs. 30 %, p = 0.326; WLL outlier 20 % vs. 30 %, p = 0.519). Tibial slope was maintained in the navigation group (+0.3°, p = 0.732), whereas increased in the conventional group (+3°, p < 0.001). The fluoroscopy time was shorter in the navigation group (10.4 seconds vs. 24.8 seconds, p < 0.001). The operative time was comparable in both groups (41.3 minutes vs. 39.2 minutes, p = 0.232).
Conclusions
The use of navigation can improve tibial slope maintenance and reduce radiation exposure in MOWHTO, without considerable extension of operative time by optimising the surgical technique.
Level of evidence
Level III, retrospective comparative study.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
High tibial osteotomy (HTO), a viable option for younger patients with medial tibiofemoral joint osteoarthritis (OA) with varus malalignment, is a load-shifting procedure that changes lower limb alignment [1]. Consequently, satisfactory outcomes after the procedure require that optimal target alignment is achieved [2]. Notably, several previous studies revealed that poorly corrected alignment was one of the most important reasons for unsatisfactory clinical results after HTO [3–5]. Given the importance of optimal target alignment to the success of HTO, opening wedge HTO has become more popular because it has a definite advantage; alignment can be adjusted during this procedure [1, 6]. Nevertheless, failure to achieve optimal target alignment has been reported for a remarkable fraction of the patients, which are frequently described as outliers [7].
Although the navigation was introduced for HTO to increase the likelihood of achieving target alignment [8, 9], the usefulness of the navigation in HTO has not yet been well established. Most of the previous studies that compared the results of navigated HTO with those after the conventional method reported that the navigated group achieved more accurate coronal alignment with less frequent outliers than the conventional group [10–16]. However, a concerning incidence of outliers is still reported even in navigated HTO, with a wide range, from 0 to 35 % [7, 10, 12, 14–17]. Whether the use of navigation improves sagittal alignment is still controversial [11–13, 18]. In addition, a theoretical advantage of the navigation is the potential to reduce radiation exposure, which has not yet been rigorously investigated [19, 20].
Similar to the experience of the use of navigation in the total knee arthroplasty, longer operative time has been suggested as a typical disadvantage of navigated HTO, owing to tracker fixation registration, compared to the conventional surgery [10, 12, 14]. The authors recently reported a novel method to estimate the length of the proximal screws of the plate, using a pre-operative plain radiograph, which has so far functioned well in our navigated medial opening wedge HTO series [21]. These simple algorithms helped us to predetermine the screw length, without the need for fluoroscopy, so we anecdotally experienced reduced fluoroscopy use and operative time. This improvement in the surgical technique is thought to be able to reduce operative time and radiation exposure.
The purpose of this study was to determine the usefulness of the navigation in medial opening wedge HTO compared to the conventional technique, in terms of target coronal alignment achievement, tibial slope maintenance and reduction of radiation exposure. We also aimed to determine whether the longer operation time, a potential disadvantage of navigated HTO, can be overcome by optimization of surgical technique, such as use of screw length-predicting algorithms which may facilitate the operation.
Patients and methods
Study design and patients allocation
This retrospective comparative study was approved by our Institutional Review Board. For this study, we defined two comparison groups: (1) the navigation group that included patients who underwent navigated HTO by a single surgeon as treatment for symptomatic varus knee OA, and (2) the conventional group that included patients who underwent conventional HTO by another surgeon for treatment of symptomatic varus knee OA. The follow-up period was more than three months. First, we reviewed 44 knees in 38 patients who underwent navigated medial opening wedge HTO in our institute from February 2012 to February 2013, in order to identify members of the navigation group. From these patients, we excluded four knees in four patients that fulfilled at least one of the following exclusion criteria: (1) patients underwent HTO to treat diseases other than primary or secondary osteoarthritis (OA), including ligament injuries (posterolateral corner injury of the knee and anterior cruciate ligament injury), developmental deformity of the knee, or for cosmetic purpose (2 knees); (2) patients whose osteotomy site were fixed with the implants other than TomoFix® (0 knee); and (3) patients whose radiographs were not adequate to measure accurate alignment due to rotation or whose radiographs were taken ≥ three months after surgery were not available (2 knees). Finally, 40 knees (34 patients) that underwent navigated medial opening wedge HTO for symptomatic primary varus knee OA remained. Our general indications for HTO in patients with varus knee OA were (1) moderate (Kellgren–Lawrence grade 3) radiographic medial TF OA with varus malalignment and with intact radiographic joint space at the lateral TF compartment; (2) the major component of the varus limb alignment did not stem from the distal femur but from the proximal tibia; and (3) significant and disabling pain originating from the medial side of the knee that was recalcitrant to conservative measures for > three months. There were 33 women and seven men with a mean age of 55.4 years [standard deviation (SD) = 5.8, range: 43–73] and a mean body mass index (BMI) of 26.9 kg/m2 (SD = 2.6, range: 22.5–32.5) (Table 1) in this group.
To identify a conventional group with half the number of patients of the navigation group, we reviewed cases of conventional medial opening wedge HTO conducted by another surgeon in our institute in a retrograde sequential manner from May 2012, applying the same exclusion criteria as for the navigation group. Among the 33 knees in 30 patients between August 2010 and May 2012, 13 knees in 13 patients were excluded; 20 knees in 17 patients remained after the following exclusions: seven knees for diagnosis other than primary or secondary OA, three knees for other fixation device, and three for inadequate radiographs to measure alignment. There were 11 women and 9 men with a mean age of 50.0 years (SD = 9.5, range: 29–60) and a mean bBMI of 25.3 kg/m2 (SD = 3.1, range: 20.0–29.8) (Table 1). Because the patients were not randomly allocated study groups, we found significant differences in all the demographic parameters except weight.
Surgical techniques
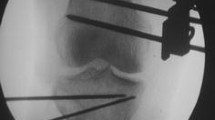
Surgical procedures for navigated HTO were controlled using information provided by the navigation system (OrthoPilot®; B. Braun Aesculap, Tuttlingen, Germany). After longitudinal skin incision on the proximal tibia, the pes anserinus was identified. Then, the superficial medial collateral ligament (MCL) was released while the pes anserinus was protected (Fig. 1a). The osteotomy site was determined by identifying the joint line using an 18-gauge syringe needle and applying a real plate on the proximal tibia (Fig. 1b). A dual osteotomy line, which consisted of horizontal and vertical osteotomy, was drawn on the tibial surface below the position of D screw hole and behind the patellar tendon insertion (Fig. 1c). After femoral and tibial trackers were fixated, kinematic and anatomical registration was performed. Then, initial deformity was evaluated using the navigation system in terms of mechanical tibiofemoral angle (mTFA) and the position of the weight loading line (WLL) coordinate (Fig. 1d). Two guide pins were inserted from the determined osteotomy site, aiming the fibular tip under fluoroscopy guidance (Fig. 1e). Dual osteotomies were performed using a micro-oscillating saw system and completed with 4 thin osteotomes provided by the TomoFix® HTO system (Synthes, Solothurn, Switzerland) (Fig. 1f). Degrees of correction were determined by considering the mTFA and the position of WLL coordinate at the knee joint. The targets for the correction were a mTFA of valgus 3° and a WLL coordinate of 62 %; if both criteria were not met simultaneously, a target avoiding too much correction was chosen, typically a mTFA range of 2°–6° and a WLL coordinate range of 55 %–70 %. Allogenous cancellous bone grafts were used to fill the osteotomy sites while the corrected position was maintained with a bone spreader under navigation control (Fig. 1g, h). After gap filling of the osteotomy site, a TomoFix® plate was applied at the predetermined position (Fig. 1i). Screws selected for holes A, B, C, and D by using the simple algorithms were inserted without the use of fluoroscopy (Fig. 1j) [21]. The algorithms consisted of eight sub-algorithms, which were based on the anteroposterior (AP) length or mediolateral (ML) width measured on the pre-operative radiographs, and two algorithms for each of the four screws (Fig. 2; Table 2). If the two algorithms from the ML and AP dimensions suggested different lengths, a shorter screw was selected to avoid potential neurovascular complications. Once the osteotomy was completed, the procedures were controlled by navigation only and no further fluoroscopy was used except for a single exposure for a final assessment.

The surgical technique of navigated high tibial osteotomy was presented. The superficial medial collateral ligament (MCL, red arrow) was released while the pes anserinus (blue arrow) was protected (a). The osteotomy site was determined by identifying the joint line using an 18-gauge syringe needle and applying a real plate (b). A dual osteotomy line (blue arrows) was drawn on the tibial surface below the position of the D screw hole (red arrow) (c). The navigation system shows the pre-operative deformity in terms of mechanical tibiofemoral angle (red circle) and the position of the weight load line coordinate (dotted red circle) (d). Two guide pins were inserted from the determined osteotomy site with aiming the fibular tip under fluoroscopy guidance (e). Osteotomy was completed by stacking the four thin osteotomes after preliminary osteotomy using micro-oscillating saw (f). A bone spreader (red arrow) was used to achieve targeted correction, and the osteotomy site gap was filled with allogenous cancellous bone graft (blue arrow) (g). Achievement of targeted alignment was confirmed with the help of navigation. (h). While the target alignment was maintained with a bone spreader, a TomoFix® plate preloaded with three drill guides was placed at the predetermined position (i). Screws selected for holes A, B, C, and D using the algorithm were inserted without the use of fluoroscopy (j)

Mediolateral (ML) width and anteroposterior (AP) length of the proximal tibia were measured on a parallel line 1 cm distal from the joint line identified on a standing whole-limb anteroposterior (a) and lateral (b) radiograph of the knee, respectively
The conventional technique had the same targets as the navigated HTO, valgus 3° of mTFA and 62 % of the WLL coordinate. The opening gap of the osteotomy site was planned pre-operatively to determine the amount of correction. With the conventional technique, screw insertion for the TomoFix® plate was done under the control of fluoroscopy. All other surgical procedures and the rehabilitation protocols were same, irrespective of the study group.
Intra-operative measurement
During the operation, two kinds of time-related parameters were recorded, the fluoroscopy time and operative time. The fluoroscopy time was displayed on the fluoroscopy system, so the data were recorded on the case report form during every surgery. The operative time was defined as the time from the skin incision to the point that the plate was completely fixed with eight screws. It was checked by the timer in the operation room and recorded on the case report form in every surgery.
Radiographic evaluations
Radiographic evaluations were performed using double limb standing whole-leg anteroposterior radiographs and the lateral knee view; they were taken pre-operatively and postoperatively. The postoperative radiographs used in the radiographic evaluation were selected from among those obtained at ≥ three months after surgery; the best quality-images, without significant rotation, were selected. All the radiographs were taken on 14 × 51-inch grid cassettes, ensuring that the patella was facing directly anterior. All radiographic images were digitally acquired using a picture archiving communication system (PACS). Radiographic measurements were conducted on a 24-inch monitor (U2412M: Dell, Round Rock, TX, USA) in portrait mode using PACS software (Infinite, Seoul, Korea). This software could detect minimum differences of 0.1° in angle and 0.1 mm in length measurements.
To evaluate the coronal alignment, two parameters were measured; the mTFA and the WLL coordinate. The mTFA was defined as the angle formed by the intersection of the mechanical axes of the femur (the line from the femoral head centre to the femoral intercondylar notch centre) and the tibia (the line from ankle talus centre to the centre of the tibial spine tips) (Fig. 3). A negative value was assigned to the knee in varus alignment. The WLL coordinate (%) was defined as the proportion of the mechanical axis of the limb (the line from the femoral head centre to the ankle talus centre) passing through the knee from the edge of the medial tibial plateau (0 %) to the edge of the lateral tibial plateau (100 %) (Fig. 4). A negative value was assigned to severe varus with the WLL passing through the medial side of the medial edge of the tibial plateau. To evaluate the sagittal alignment, we measured the posterior tibial slope on the lateral view of the knee. This tibial slope was defined as the angle formed between the tangential line of the medial tibial plateau and the posterior cortical line connecting the two points on the posterior cortex of the tibia at 5 and 15 cm distal to the knee joint (Fig. 5) [22]. The tibial slope was expressed as the angle size minus 90°; hence, a negative slope value indicated that the angle is less than 90° and that the tibia slope is tilted anteriorly (reverse slope). The size of the changes in the tibial slope was calculated using the pre-operative and postoperative values of tibial slope, which a positive value indicated an increase in the slope after the HTO.

Radiographs showing the pre-operative (a) and postoperative (b) mechanical tibiofemoral angle (mTFA). mTFA was defined as the angle formed by the intersection between the mechanical axes of the femur (the line from the centre of femoral head to the centre of femoral intercondylar notch) and the tibia (the line from the centre of ankle talus to the center of the tibial spine tips). A negative value was assigned to the knee in varus alignment

Radiographs showing the pre-operative (a) and postoperative (b) weight loading line (WLL) coordinate. The WLL coordinate was defined as the proportion of the mechanical axis of the limb (the line from the femoral head centre to the ankle talus centre) passing through the knee from the edge of the medial tibial plateau (0 %) to the edge of the lateral tibial plateau (100 %)

Radiographs showing the pre-operative (a) and postoperative (b) tibial slope. Tibial slope was defined as the angle formed by the tangential line of the medial tibial plateau and the posterior cortical line connecting the two points on the posterior cortex of the tibia at 5 and 15 cm distal from the knee joint
To determine intra- and inter-observer reliabilities of radiographic assessments, two orthopedic surgeons performed radiographic assessments in 20 randomly selected knees twice within a three week interval. The intra-and inter-observer reliabilities of assessments of all radiographic measurements were evaluated using intra-class correlation coefficients (ICCs). The ICCs of intra- and inter-observer reliabilities of all measurement were > 0.9 (range: 0.902–0.994) representing satisfactory reliabilities in the measurements. Thus, measurements taken by a single investigator were used in the analyses.
Statistical analysis
All the statistical analyses were carried out with SPSS for Windows v.20.0 (IBM, Chicago, IL, USA), and p values < 0.05 were considered significant. To examine differences in coronal limb alignments between the two groups, the mTFA and the WLL coordinate were compared using Student’s t test. To evaluate the difference in the proportion of outliers, which were defined as the proportion of cases that deviated from the target range of valgus 2°–6° of mTFA and 55 %–70 % of WLL coordinate, we compared the two groups using the chi-square test. The pre-operative and postoperative tibial slope was compared in each group using paired t test, and the amount of the changes in the tibial slope was compared between the two groups using Student’s t test. The differences in the fluoroscopy time and operative time were compared between the two groups using the Student’s t test.
Results
The navigation group showed better tibial slope maintenance and less radiation exposure, while the target coronal alignment achievement was not significantly improved compared to the conventional group (Table 2). The mTFA and WLL coordinate had no significant different between the navigation and conventional groups (3.5° vs. 3.3°, p = 0.755 in mTFA; 64.5 % vs. 62.9 %, p = 0.509 in WLL coordinate). The proportion of the coronal alignment outliers was smaller in the navigation group for both the mTFA criteria (18 % in navigation group and 30 % in conventional group, p = 0.326) and the WLL coordinate criteria (20 % in navigation group and 30 % in conventional group, p = 0.519). However, the differences did not reach statistical significance. The tibial slope change was not significant in the navigation group (mean change, +0.3°, p = 0.732), whereas it was increased significantly in the conventional group (mean change, +3.0°, p < 0.001). Consequently, the amount of change of the tibial slope in the conventional group was greater than the navigation group (p = 0.024). The fluoroscopy time was shorter in the navigation group than the conventional group (10.4 s vs. 24.8 s, p < 0.001).
The operative time was comparable between the two groups (Table 3). The operative time was about two minutes longer in the navigation group, but this difference was not statistically significant (41.3 minutes vs. 39.2 minutes, p = 0.232).
Discussion
Navigation was introduced in high tibial osteotomy primarily to achieve more accurate coronal alignment, which is crucial to the successful clinical outcome. However, the reported proportion of outliers in the coronal alignment after navigated HTO varied widely, and the contribution of the navigation to the control of the tibial slope control is still controversial. In addition, reduction of fluoroscopy use is a potential merit of navigated HTO, which is not well established in the literature. On the other hand, longer operative time has been a major criticism of the navigated HTO. We conducted this study to determine whether the use of navigation in HTO is advantageous, in terms of achieving target coronal alignment, maintaining tibial slope and reducing fluoroscopy use. We also aimed to determine whether the longer operation time, a potential drawback of navigated HTO, can be overcome by optimization of surgical technique, such as the use of screw length-predicting algorithms.
Our findings suggest that the use of navigation is beneficial in medial opening wedge HTO, in terms of tibial slope maintenance and reduction of radiation exposure during the surgery. There was an only minimal change in the tibial slope in the navigation group, whereas it increased by 3° in the conventional group. This finding agreed with three of the previous studies [10–12, 18], but did not agree with that of another report [13]. It has generally been accepted that the posterior tibial slope increases after medial opening wedge HTO [23–25], as we observed in our conventional group. However, we thought that the tibial slope could be maintained unchanged in the navigation group by assuring that the degree of the maximal extension remained unchanged throughout the operation using the navigational information, as described in the previous reports [10, 26]. Less radiation exposure was one of the theoretical advantages of the navigated HTO, but there is limited clinical data comparing the radiation exposure between the navigation and conventional techniques for HTO. A cadaveric study found that the fluoroscopic radiation time was shorter in the navigated HTO [19]. The fluoroscopic radiation time was 63.8 seconds in the conventional group and 53.2 seconds in the navigation group, which was considerably different from our data: 24.8 seconds and 10.4 seconds, respectively. These remarkable differences are thought to result primarily from the surgical technique and the fluoroscopy-use habit of the operators. On the other hand, 12 seconds of fluoroscopy use reported by Jackson et al. was very similar to our results [20]. Our findings confirm this theoretical advantage of navigation: fluoroscopic time was reduced to less than one-half the time of the conventional technique.
The advantage of the navigated HTO in the target coronal alignment achievement was not definitely revealed in our study. The mean values of mTFA and WLL coordinate were similar, and the occurrence of the coronal alignment outlier was not significantly different between the two groups, although the navigation group had fewer outliers than the conventional group. Our findings were similar with several previous studies that reported fewer occurrence of coronal alignment outlier in the navigation group than the conventional method, and the proportion of the outliers was in the middle of the reported wide range (Table 4). Using power analysis, we found that a larger sample size was needed for the difference observed in our study to reach significance. Nevertheless, even with the use of navigation, 20 % of patients were outliers in our series. Although this considerable frequency of outliers may reflect the relatively narrow target range, the inherent limitation of the navigation system appears to be the major cause of outliers. Navigated surgery, which is performed with the patient supine, cannot fully reflect the standing position with full weight bearing status [27]. In addition, correction of the coronal alignment may alter the knee adduction moment, which can cause the alignment to deviate from the pre-operatively estimated result. These unpredictable factors are thought to produce discrepancies between navigational information and the alignment measured on the postoperative radiograph. Thus, further studies should be conducted to achieve improved target alignment by reducing the limitations of the current navigation-assisted surgery in HTO.
In terms of the operative time, the use of navigation did not significantly lengthen it in the current study. Our findings agreed with previous studies that reported comparable operation time in both groups [13, 15], although they conflicted with some other articles that reported longer operative times in the navigation group [10, 12, 14]. Furthermore, the additional operation time in navigation group was only about two minutes in our series, which was definitely shorter than previous studies reporting longer operation times ranging from ten to 23 minutes [10, 12, 14]. It is reasonable to predict that the navigation approach would take more time because it requires some additional steps throughout the operation compared to the conventional technique, such as tracker fixation and registration of anatomical landmarks. In our series, the simple algorithm for prior estimation of the proximal screws’ length of the TomoFix® plate was used only in the navigation group, which would eliminate the time required to check the screw length using fluoroscopy. We thought this difference in the surgical technique might have significantly affected the operative time as well the fluoroscopy time. Our findings suggest that the longer operative time, a frequently mentioned disadvantage of the navigation surgery, can be overcome by optimising the surgical procedure.
The current study has several limitations that should be considered during the interpretation of the results. First, the high tibial osteotomies in each group were performed by two different surgeons. Thus, the comparison may be affected by the surgeon factor. However, both surgeons were highly experienced in high tibial osteotomy before the start of this series, as confirmed by the results of the operative time and the target coronal alignment achievement. The operative time in the each group was far shorter than those of other reports, although we did not include about 15–20 minutes of wound closure time in the operation time [10, 13, 15]. The proportion of the coronal alignment outliers was less than those mean values of the previous studies in the literature [10, 12, 14–16]. Thus, the potential bias stemming from the surgeon effect may be limited. Second, the demographic features of the two groups were significantly different from each other, because the patients were not randomly allocated to the groups. The different patient pools of the two surgeons may explain these differences in demographic features. However, we compared accuracy of the alignment, operative time and radiation exposure, not the clinical results, such as functional status, pain or patient satisfaction, outcomes that can be confounded by demographic characteristics. Thus, we believe that the differences in the demographics did not considerably limit the validity of this study. Third, the prior screw length estimation algorithm was used only in the navigation group. This might have distorted parallel comparisons of the fluoroscopy and operative times, but not in the radiologic outcome, between the navigated and conventional HTO groups. However, longer operation time was already reported as a disadvantage of navigated HTO so we did not expect that the navigated HTO could be performed in shorter operation times than conventional HTO [10, 12, 14]. Rather, we wanted to know whether the longer operative time of the navigation surgery could be overcome by improving the surgical procedure, such as the use of our algorithms to predict screw length of the plate. Finally, we did not compare functional outcome owing to the short-term follow-up period. Thus, further study is required to reveal whether there will be differences in the clinical outcome after navigated HTO compared to the conventional technique.
In conclusion, the use of navigation in the medial opening wedge HTO is beneficial for the maintenance of tibial slope and reduction of the radiation exposure when compared to the conventional technique. The longer operation time, a typical potential disadvantage of navigation, can be overcome by optimizing the surgical procedure. Therefore, we recommend the use of navigation in the medial opening wedge HTO, for more precise sagittal alignment control and radiation safety of the patients and the surgeons, without considerable extension of operative time.
References
Amendola A, Bonasia DE (2010) Results of high tibial osteotomy: review of the literature. Int Orthop 34:155–160
El-Azab HM, Morgenstern M, Ahrens P, Schuster T, Imhoff AB, Lorenz SG (2011) Limb alignment after open-wedge high tibial osteotomy and its effect on the clinical outcome. Orthopedics 34:e622–e628
Dugdale TW, Noyes FR, Styer D (1992) Preoperative planning for high tibial osteotomy. The effect of lateral tibiofemoral separation and tibiofemoral length. Clin Orthop Relat Res:248–264
Hernigou P, Medevielle D, Debeyre J, Goutallier D (1987) Proximal tibial osteotomy for osteoarthritis with varus deformity. A ten to thirteen-year follow-up study. J Bone Joint Surg Am 69:332–354
Coventry MB (1973) Osteotomy about the knee for degenerative and rheumatoid arthritis. J Bone Joint Surg Am 55:23–48
Gaasbeek RD, Nicolaas L, Rijnberg WJ, van Loon CJ, van Kampen A (2010) Correction accuracy and collateral laxity in open versus closed wedge high tibial osteotomy. A one-year randomised controlled study. Int Orthop 34:201–207
Song EK, Seon JK, Park SJ, Seo HY (2008) Navigated open wedge high tibial osteotomy. Sports Med Arthrosc 16:84–90
Wang G, Zheng G, Keppler P, Gebhard F, Staubli A, Mueller U, Schmucki D, Fluetsch S, Nolte LP (2005) Implementation, accuracy evaluation, and preliminary clinical trial of a CT-free navigation system for high tibial opening wedge osteotomy. Comput Aided Surg 10:73–85
Keppler P, Gebhard F, Grutzner PA, Wang G, Zheng G, Hufner T, Hankemeier S, Nolte LP (2004) Computer aided high tibial open wedge osteotomy. Injury 35(Suppl 1):S-A68–S-A78
Akamatsu Y, Mitsugi N, Mochida Y, Taki N, Kobayashi H, Takeuchi R, Saito T (2012) Navigated opening wedge high tibial osteotomy improves intraoperative correction angle compared with conventional method. Knee Surg Sports Traumatol Arthrosc 20:586–593
Bae DK, Song SJ, Yoon KH (2009) Closed-wedge high tibial osteotomy using computer-assisted surgery compared to the conventional technique. J Bone Joint Surg (Br) 91:1164–1171
Iorio R, Pagnottelli M, Vadala A, Giannetti S, Di Sette P, Papandrea P, Conteduca F, Ferretti A (2013) Open-wedge high tibial osteotomy: comparison between manual and computer-assisted techniques. Knee Surg Sports Traumatol Arthrosc 21:113–119
Kim SJ, Koh YG, Chun YM, Kim YC, Park YS, Sung CH (2009) Medial opening wedge high-tibial osteotomy using a kinematic navigation system versus a conventional method: a 1-year retrospective, comparative study. Knee Surg Sports Traumatol Arthrosc 17:128–134
Maurer F, Wassmer G (2006) High tibial osteotomy: does navigation improve results? Orthopedics 29:S130–S132
Reising K, Strohm PC, Hauschild O, Schmal H, Khattab M, Sudkamp NP, Niemeyer P (2013) Computer-assisted navigation for the intraoperative assessment of lower limb alignment in high tibial osteotomy can avoid outliers compared with the conventional technique. Knee Surg Sports Traumatol Arthrosc 21:181–188
Saragaglia D, Roberts J (2005) Navigated osteotomies around the knee in 170 patients with osteoarthritis secondary to genu varum. Orthopedics 28:s1269–s1274
Saragaglia D, Blaysat M, Mercier N, Grimaldi M (2012) Results of forty two computer-assisted double level osteotomies for severe genu varum deformity. Int Orthop 36:999–1003
Ribeiro C, Severino N, de Barros M, Fucs P (2014) Opening wedge high tibial osteotomy: navigation system compared to the conventional technique in a controlled clinical study. Int Orthop 38:1627–1631
Hankemeier S, Hufner T, Wang G, Kendoff D, Zeichen J, Zheng G, Krettek C (2006) Navigated open-wedge high tibial osteotomy: advantages and disadvantages compared to the conventional technique in a cadaver study. Knee Surg Sports Traumatol Arthrosc 14:917–921
Jackson DW, Warkentine B (2007) Technical aspects of computer-assisted opening wedge high tibial osteotomy. J Knee Surg 20:134–141
Kim TK, Chang CB, Lee KH, Cho HJ, Je MS, Won HH, Kang YG (2012) Use of simple algorithms to predict screw length facilitates navigation-controlled medial opening-wedge osteotomy using the TomoFix HTO system. Orthopedics 35:22–28
Yoo JH, Chang CB, Shin KS, Seong SC, Kim TK (2008) Anatomical references to assess the posterior tibial slope in total knee arthroplasty: a comparison of 5 anatomical axes. J Arthroplasty 23:586–592
Brouwer RW, Bierma-Zeinstra SM, van Koeveringe AJ, Verhaar JA (2005) Patellar height and the inclination of the tibial plateau after high tibial osteotomy. The open versus the closed-wedge technique. J Bone Joint Surg Br 87:1227–1232
El-Azab H, Halawa A, Anetzberger H, Imhoff AB, Hinterwimmer S (2008) The effect of closed- and open-wedge high tibial osteotomy on tibial slope: a retrospective radiological review of 120 cases. J Bone Joint Surg (Br) 90:1193–1197
Marti CB, Gautier E, Wachtl SW, Jakob RP (2004) Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 20:366–372
Song EK, Seon JK, Park SJ (2007) How to avoid unintended increase of posterior slope in navigation-assisted open-wedge high tibial osteotomy. Orthopedics 30:S127–S131
Ribeiro CH, Severino NR, Fucs PM (2013) Preoperative surgical planning versus navigation system in valgus tibial osteotomy: a cross-sectional study. Int Orthop 37:1483–1486
Acknowledgments
Each author certifies that his or her institution has approved the human protocol for this investigation, and that all investigations were conducted in conformity with ethical principles of research, and that informed consent was obtained. This work was performed at the Joint Reconstruction Center, Seoul National University Bundang Hospital.
Funding
No financial support was provided for this study.
Conflict of interest
Dr. Kim received research funding from Smith & Nephew and B.Braun Aesculap, and is a design consultant for Smith & Nephew and B.Braun Aesculap. None of the other authors (YGN, SHE, SJK, MJC) have relevant conflicts of interest to declare.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Na, Y.G., Eom, S.H., Kim, S.J. et al. The use of navigation in medial opening wedge high tibial osteotomy can improve tibial slope maintenance and reduce radiation exposure. International Orthopaedics (SICOT) 40, 499–507 (2016). https://doi.org/10.1007/s00264-015-2880-x
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2880-x