
Abstract
Purpose
The objective of this study was to verify whether the correction obtained using a navigation system (NS) corresponds to the wedge calculated by the Dugdale method (DM) in high tibial osteotomy (HTO).
Methods
We included 17 patients with primary varus and HTO indication, consecutively admitted to a public university hospital. All patients underwent panoramic radiography with bipedal load for the wedge calculation by DM. They underwent HTO with an opening wedge, fixed with an HTO plate and monitored by the OrthoPilot NS. Bone grafts were used in every case. The wedge opening obtained by the NS was compared to that calculated in the radiographs.
Results
The mean opening by DM was 9.53° and by the NS 11.8° (p < 0.045).
Conclusions
There was a significant difference in the calculation of the wedge opening between the DM and NS. HTO without the aid of the NS could theoretically lead to undercorrection of the deformity.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Tibial osteotomy with an opening wedge fixed with a medial plate is an established procedure for the treatment of medial unicompartmental osteoarthritis associated with genu varum, especially in young or very active patients [1–3]. This procedure became popular in the 1990s, with the emergence of the Puddu plate, which gave a stable fixation of the osteotomy and allowed early mobilisation of the joint [3, 4]. Since then, other osteotomy plates for medial fixation have been developed, always seeking to add stability to the opening wedge.
The stability of the fixation is essential, but it is not, on its own, sufficient for the successful outcome of surgery [2, 5]. It is well established that correction of misalignment must be accurate, because over- and undercorrections lead to unsatisfactory results from a clinical point of view [6, 7]. If the leg axis is undercorrected, the transfer of weight from the medial to the lateral compartment is incomplete, the patient experiences pain and the gonarthritis progresses. If it is overcorrected (too much valgus), the knee may become unstable and the arthritis progresses faster in the lateral compartment [7].
It is extremely difficult for the surgeon to check the alignment of the limb during surgery, since the lower limb is covered by sterile drapes and has a tourniquet [8]. In order to guide the opening of the wedge a good surgical plan is mandatory. Based on clinical and radiographic evaluation of the patient, the surgeon begins the procedure already knowing how many degrees the opening should reach. Among the planning methods so far proposed, one should be noted: the method of Dugdale et al. [9]. According to these authors, the goal of osteotomy is to transfer the load to the limb with varus deformity to the lateral compartment of the knee, a region that corresponds to 62 % of the joint surface. The final result is considered acceptable when the mechanical axis presents 2–6° of valgus [7, 9, 10]. Good and very good results have been reported using this planning [10]. However, the frequency of over- and undercorrections found in the literature is still considerable [1, 3]. Moreover, it is known that any long-term clinical improvement obtained will be lost [3, 6].
In this decade, a new tool has been developed to control intra-operative alignment of the leg. This is a navigation system that is positioned at strategic points on the femur and the tibia and, according to the measurements made by the software, to demonstrate, on the computer screen, the alignment of the limb in real time [11–13]. It is expected that the navigation system will provide a more accurate alignment correction of the limb and possibly improve the long-term results. However, we are still looking for a correlation between the correction proposed by the preoperative planning method, on radiographs, and the one produced during the operation by the navigation system. Therefore, the objective of this study was to verify whether the correction angles indicated by the navigation system correspond to the degree of opening wedge calculated by the method of Dugdale et al. [9].
Patients and methods
Design and patient selection
This prospective study, which was carried out with approval from the local Institutional Ethics Review Board and the written informed consent of the patients, included all consecutive patients admitted to the knee surgery division of a public university hospital for high tibial osteotomy (HTO) from August 2010 to May 2011. The inclusion criteria were: knee pain for at least one year, radiographs showing varus deformity not exceeding 20° and medial compartment osteoarthritis, preserved range of motion, with flexion of at least 90°, extension deficit of less than 15° and a stable knee. Patients were excluded if they had undergone previous knee surgery, if Ahlbäck grade 4 or 5 osteoarthritis was present [14] and if they had patellofemoral pain or a diagnosis of rheumatoid arthritis. In the study period, 20 patients were admitted, but three did not fulfil the inclusion criteria, leaving 17 patients for this study.
Preoperative evaluation and planning
Before surgery, all patients were clinically and radiographically evaluated. Digital radiographs were taken in the anteroposterior (AP) view, bilaterally, 30° profile, with a standing flexion position, axial profile of the patella in 30° and panoramic view with bipedal load. In the latter, patients stood with their feet parallel, barefoot and no rotation. These views allowed the classification of arthritis according to Ahlbäck [14] criteria and also the measurement of varus deformity.
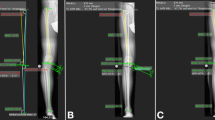
Preoperative planning was based on the Dugdale et al. [9] method, based on the panoramic view. According to this method, the objective of the osteotomy is to transfer the load from the medial region to the lateral plateau, in a position corresponding to 62 % of the tibial joint surface. On the AP radiograph, a line is drawn on the X-ray on the tibial joint surface, setting a point “P” in the lateral compartment at the site corresponding to 62 % of that area from medial to lateral. A second line is then traced from the centre of the femoral head to point P and another line from the centre of the ankle to point P. The acute angle α formed by the intersection of these two lines determines the angle correction (Fig. 1).

Calculation of the angle for the preoperative planning as proposed by Dugdale et al. [9]
Surgical procedure and navigation
All patients underwent HTO by the same team, under spinal anaesthesia, in the dorsal decubitus position. The procedure began with arthroscopy for the treatment of meniscal injuries, chondral lesions or loose bodies. Once arthroscopy was completed, navigation guides were positioned and fixed with Steinmann pins on the distal femur, proximal tibia and distal tibia, respectively. Minimally invasive reference array units were mounted, ideally, in the medial cortex of the tibia and ventral medial or ventral lateral side of the femur. The registration automatically starts with the definition of the centre of the femoral head, which is found by pivoting the leg at the hip joint. When a precision margin of less than two millimetres is achieved, the software automatically proceeds to the next step. Anatomical landmarks, to calculate the centre of the knee and ankle, are registered percutaneously with a pointer. The first landmark is the medial malleolus followed by the lateral malleolus. The medial tibial plateau border is registered as well as the lateral tibial plateau border. The AP direction is then defined. The last points to be digitalised are the medial and lateral epicondyles. At this point, the surgeon has all the information on the mechanical leg axis, the degree of flexion and the relative rotation of the tibia against the femur. On the screen of the navigation system, the leg is shown with the alignment parameters. The sequence of data collection was determined by the navigation system (OrthoPilot HTO v. 1.5, Aesculap, Tuttlingen, Germany).
After the initial navigation reading, the wedge was opened with the objective of obtaining a mechanical axis of 30–40° from the lateral tibial plateau surface (Fujisawa et al. [15] line). Fixation was made with the HTO plate (Aesculap, Tuttlingen, Germany) and the wedge was filled with preformatted artificial graft.
Post-operative care and data analyses
Patients remained in hospital for one night with suction drains and received prophylactic antibiotic (intravenous cefazolin, 1 g, eight hourly for up to 48 hours). After drainage removal, passive movement on the operated knee was allowed. Partial weight bearing was allowed six weeks after surgery, with full weight-bearing at 12 weeks. By this time, radiographs were taken to measure the mechanical axis, according to the Dugdale et al. [9] method, and to assess the bone healing.
Mean preoperative mechanical axis measurements by the Dugdale et al. [9] method were compared to the navigation system measurement using Student’s t and Kruskal-Wallis tests. Statistical Analysis System (SAS) software was used and a p value of 0.05 was adopted as significant.
Results
Among the 17 patients included, the right knee was affected in 8 and the left knee in 9. There was only one woman in the sample. The mean age of patients was 45.7 years (24–59 years).
Preoperative mechanical axis in the radiographs was 7.47° in varus and the navigation system measurement was 6.73° in varus (ranges are presented in Table 1), with no statistically significant differences between them (p = 0.5823 by Student’s t test and 0.6919 by Kruskal-Wallis test).
The mean opening obtained, calculated by the Dugdale et al. method, was 9.53° and 11.8° by the navigation system measurement. This difference was statistically significant (p = 0.0359 by Student’s t test and p = 0.045 by Kruskal-Wallis test).
Discussion
It is known that long-term satisfactory results of tibial osteotomies are directly related to the final correction obtained [6, 7]. The preoperative planning described by Dugdale et al. [9] is an established method for calculating the opening wedge osteotomy, seeking a final mechanical axis 3–6° [9]. However, the frequency of over- and especially undercorrections using of this method is still high [1, 3]. It is known that each step in the implementation of the method may interfere with the calculation of the wedge. The positioning of the patient at the time of the panoramic radiograph is of extreme importance: the patient must stand with the feet parallel to each other and barefoot, to prevent internal or external rotation of the limbs. Mistakes in measurements with a ruler and pencil may also occur; therefore, it is preferable to use digital radiography, as this enables more accurate measurements [8, 16].
The navigation system has been used in tibial osteotomies for almost a decade and provides information about the alignment, the load axis, varus and valgus stress, speed, range of motion, limb length and slope. Despite the increased surgical time and the fact that it has a longer learning curve, navigation is considered a promising adjunct for intraoperative use to avoid under- and overcorrections [7, 11–13, 17–19].
Other studies have already investigated the navigation system accuracy in comparison with preoperative planning based on radiographs [20–22], one of them using cadavers [21]. However, this is the first study to compare the navigator to the Dugdale et al. [9] method of preoperative planning.
According to our study, the initial mechanical axis obtained by the navigation system was the same calculated by a carefully taken panoramic digital radiograph. However, navigation indicated an opening of the wedge that was larger than that indicated by the Dugdale et al. [9] method. This would avoid some cases of undercorrection. However, it is essential to examine why this occurred. The reason is not clear, but we speculate that the method of measurement in the navigation system may be involved. The system uses the Fujisawa et al. [15] method to calculate the final mechanical axis. According to these authors, the mechanical axis must be transferred to a region corresponding to 30–40 % of the lateral joint surface from the centre of the knee. On the other hand, Dugdale et al. propose that the load axis be transferred to 62 % laterally from the medial face of the tibia [9]. Considering a knee where the medial and lateral compartments are symmetrical, the point set by Dugdale et al. [9] would correspond to 24 % of the lateral compartment. This difference can account for the larger wedge indicated by the navigation system. It should also be noted that the navigation system allows a 3D evaluation of the limb, while radiographs provide only 2D images, and the wedge in osteotomy, trapezoidal in shape, has an anterior angle that is smaller than the posterior one.
Dugdale et al. [9] also propose that for each one millimetre of wedge opening, one degree of deformity should be corrected. However, this does not take into consideration the size of the tibia of each patient, while the navigation system measures and considers the tibia size.
Finally, the panoramic radiograph used in the Dugdale et al. [9] method is made with the patient in the standing position, with load and tensioning of ligaments and muscles, which would increase varus deformity. In the navigation system, the measurement is made with the limb in a relaxed position.
The two methods calculated different wedge openings, but the real significance of this finding, in the long term, still needs to be evaluated from the perspective of cost-benefit analysis: besides increasing surgical time, the navigation system has higher costs and higher risks of femoral and tibial fractures [23–26]. Studies, which are currently being carried out by our team, will investigate the final results of the osteotomy with the correction calculated by the Dugdale et al. [9] method and by the navigation system after surgery.
This study has shown a significant difference in the calculation of the wedge opening between the methods of Dugdale et al. [9] and that provided by the navigation system. If we believe that the navigation system is a more precise calculation method, then HTO without the aid of the system could theoretically lead to undercorrection of the deformity.
References
Marti CB, Gautier E, Wachtl SW, Jakob RP (2004) Accuracy of frontal and sagittal plane correction in open-wedge high tibial osteotomy. Arthroscopy 20(4):366–372
Esenkaya I, Elmali N (2006) Proximal tibia medial open-wedge osteotomy using plates with wedges: early results in 58 cases. Knee Surg Sports Traumatol Arthrosc 14(10):955–961
Insall JN, Joseph DM, Msika C (1984) High tibial osteotomy for varus gonarthrosis. A long-term follow-up study. J Bone Joint Surg Am 66(7):1040–1048
Puddu G, Franco V (2000) Femoral antivalgus opening wedge osteotomy. Oper Tech Sports Med 8(1):56–60
Lobenhoffer P, Agneskirchner JD (2003) Improvements in surgical technique of valgus high tibial osteotomy. Knee Surg Sports Traumatol Arthrosc 11(3):132–138
Amendola A (2003) Unicompartmental osteoarthritis in the active patient: the role of high tibial osteotomy. Arthroscopy 19(Suppl 1):109–116
Gebhard F, Krettek C, Hüfner T, Grützner PA, Stöckle U, Imhoff AB et al (2011) Reliability of computer-assisted surgery as an intraoperative ruler in navigated high tibial osteotomy. Arch Orthop Trauma Surg 131(3):297–302
Kendoff D, Citak M, Pearle A, Gardner MJ, Hankemeier S, Krettek C et al (2007) Influence of lower limb rotation in navigated alignment analysis: implications for high tibial osteotomies. Knee Surg Sports Traumatol Arthrosc 15(8):1003–1008
Dugdale TW, Noyes FR, Styer D (1992) Preoperative planning for high tibial osteotomy. The effect of lateral tibiofemoral separation and tibiofemoral length. Clin Orthop Relat Res 274:248–264
Ribeiro CH, Severino NR, Cury Rde P, de Oliveira VM, Avakian R, Ayhara T et al (2009) A new fixation material for open-wedge tibial osteotomy for genu varum. Knee 16(5):366–370
Lo WN, Cheung KW, Yung SH, Chiu KH (2009) Arthroscopy-assisted computer navigation in high tibial osteotomy for varus knee deformity. J Orthop Surg (Hong Kong) 17(1):51–55
Iorio R, Vadalà A, Giannetti S, Pagnottelli M, Di Sette P, Conteduca F et al (2010) Computer-assisted high tibial osteotomy: preliminary results. Orthopedics 33(10 Suppl):82–86
Saragaglia D, Mercier N, Colle PE (2010) Computer-assisted osteotomies for genu varum deformity: which osteotomy for which varus? Int Orthop 34(2):185–190
Ahlbäck S (1968) Osteoarthrosis of the knee. A radiographic investigation. Acta Radiol Diagn (Stockh) Suppl 277:7–72
Fujisawa Y, Masuhara K, Shiomi S (1979) The effect of high tibial osteotomy on osteoarthritis of the knee. An arthroscopic study of 54 knee joints. Orthop Clin North Am 10(3):585–608
Liodakis E, Kenawey M, Liodaki E, Mommsen P, Krettek C, Hankemeier S (2010) The axis-board: an alternative to the cable technique for intraoperative assessment of lower limb alignment. Technol Health Care 18(3):165–171
Goleski P, Warkentine B, Lo D, Gyuricza C, Kendoff D, Pearle AD (2008) Reliability of navigated lower limb alignment in high tibial osteotomies. Am J Sports Med 36(11):2179–2186
Lützner J, Gross AF, Günther KP, Kirschner S (2009) Reliability of limb alignment measurement for high tibial osteotomy with a navigation system. Eur J Med Res 14(10):447–450
Demange MK, Camanho GL, Pécora JR, Gobbi RG, Tirico LE, da Mota e Albuquerque RF (2011) Simultaneous anterior cruciate ligament reconstruction and computer-assisted open-wedge high tibial osteotomy: a report of eight cases. Knee 18(6):387–391
Kim SJ, Koh YG, Chun YM, Kim YC, Park YS, Sung CH (2009) Medial opening wedge high-tibial osteotomy using a kinematic navigation system versus a conventional method: a 1-year retrospective, comparative study. Knee Surg Sports Traumatol Arthrosc 17(2):128–134
Lützner J, Gross AF, Günther KP, Kirschner S (2010) Precision of navigated and conventional open-wedge high tibial osteotomy in a cadaver study. Eur J Med Res 15(3):117–120
Akamatsu Y, Mitsugi N, Mochida Y, Taki N, Kobayashi H, Takeuchi R et al (2012) Navigated opening wedge high tibial osteotomy improves intraoperative correction angle compared with conventional method. Knee Surg Sports Traumatol Arthrosc 20(3):586–593
Noyes FR, Goebel SX, West J (2005) Opening wedge tibial osteotomy: the 3-triangle method to correct axial alignment and tibial slope. Am J Sports Med 33(3):378–387
Hankemeier S, Hufner T, Wang G, Kendoff D, Zeichen J, Zheng G et al (2006) Navigated open-wedge high tibial osteotomy: advantages and disadvantages compared to the conventional technique in a cadaver study. Knee Surg Sports Traumatol Arthrosc 14(10):917–921
Maurer F, Wassmer G (2006) High tibial osteotomy: does navigation improve results? Orthopedics 29(10 Suppl):S130–S132
Song EK, Seon JK, Park SJ (2007) How to avoid unintended increase of posterior slope in navigation-assisted open-wedge high tibial osteotomy. Orthopedics 30(10 Suppl):S127–S131
Conflict of interest
The authors declare that they have no conflict of interest. No benefits in any form have been received or will be received from any commercial party related directly or indirectly to the subject of this article.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Ribeiro, C.H., Severino, N.R. & de Moraes Barros Fucs, P.M. Preoperative surgical planning versus navigation system in valgus tibial osteotomy: a cross-sectional study. International Orthopaedics (SICOT) 37, 1483–1486 (2013). https://doi.org/10.1007/s00264-013-1960-z
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-013-1960-z