
Abstract
Purpose
While the use of bone marrow concentrate (BMC) has been described in the treatment of rotator cuff tears, the impact of a rotator cuff injury on the mesenchymal stem cells (MSCs) content present in the human shoulder has not been determined, especially with regard to changes in the levels of MSCs at the tendon–bone interface. With the hypothesis that there was a decreased level of MSCs at the tendon–bone interface tuberosity in patients with rotator cuff tear, we assessed the level of MSCs in the tuberosity of the shoulder of patients undergoing a rotator cuff repair.
Methods
We analysed the data of 125 patients with symptomatic rotator cuff tears and of 75 control patients without rotator cuff injury. We recorded the following data: size of tear, number of torn tendons, aetiology of the tear, lag time between onset of shoulder symptoms/injury and repair, and also fatty infiltration of muscles. Mesenchymal stem cell content at the tendon–bone interface tuberosity was evaluated by bone marrow aspiration collected in the humeral tuberosities of patients at the beginning of surgery.
Results
A significant reduction in MSC content (from moderate, 30–50 %, to severe >70 %) at the tendon–bone interface tuberosity relative to the MSC content of the control was observed in all rotator cuff repair study patients. Severity of the decrease was statistically correlated to a number of factors, including the delay between onset of symptoms and surgery, number of involved tendons, fatty infiltration stage and increasing patient age.
Conclusion
This study demonstrates that the level of MSCs present in the greater tuberosity of patients with a rotator cuff tear decreases as a function of a number of clinical factors, including lag time from tear onset to treatment, tear size, number of tears and stage of fatty infiltration, among others. This information may help the practices in using biologic augmentation of a rotator cuff repair.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
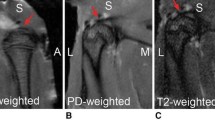
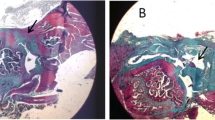
The site of the rotator cuff insertion is composed of four zones that include tendon, unmineralized fibrocartilage, mineralized fibrocartilage, and bone. In humans, the rotator cuff often ruptures at the fibrocartilage zone. The tendon-to-bone junction is slow to heal because of the relative avascularity of the fibrocartilage zone and some bone loss at the site of injury [11, 14, 20] . In human’s rotator cuff, the native biologic and histologic structure of the interface is not recapitulated during a healing process involving a fibrovascular scar tissue interface, thereby resulting in a mechanically and structurally decreased interfacial area (i.e., at the footprint). The poor healing response of the rotator cuff healing is most likely multifactorial [3, 4, 19, 22], and may include an insufficient number of MSCs at the healing tendon–bone interface. Mesenchymal stem cells are defined as being derived from mesenchymal tissue and having the functional capacity to self-renew and generate a number of differentiated progeny. These cells participate in tissue homoeostasis, remodeling, and repair by paracrine mechanisms [15, 28], as well as demonstrating an ability to differentiate into mature tissue cells that are lost during the course of physiological turnover, senescence, injury, or disease. A few papers [8, 16] have provided clinical evidence of improved healing of RTC tears with MSC augmentation.
Despite the current literature on MSCs and rotator cuff tears [7, 13], little is known about the MSC content in the greater tuberosity [25, 26] of the human shoulder. More importantly, the impact of a rotator cuff injury on the MSC content present in the human shoulder has not been determined, especially with regard to changes in the levels of MSCs at the tendon–bone interface after the onset of the RC injury.
With the hypothesis that there is a decreased level of MSCs at the tendon–bone interface tuberosity in patients with rotator cuff tear, the goals of this study are: (1) to evaluate the number of MSCs at the tendon–bone interface tuberosity of control patients (group 1) without RC injury, (2) to evaluate the number of MSCs at the tendon–bone interface tuberosity of study patients (group 2) with rotator cuff injury, and (3) to compare the index ratios for the two population groups and identify factors related to their variation in patients with rotator cuff injury.
Material and methods
Study design
Based on a power analysis, we analysed the data of 200 patients (a study group of 125 patients with symptomatic rotator cuff tears and a control group of 75 patients without rotator cuff injury). Those with a rotator cuff injury underwent open or arthroscopic tendon repair for a full thickness tendon rupture between 2000 and 2010. The rationale for the investigation and the accompanying risks were discussed with each patient, and an informed consent form approved by the University Hospital was signed. All 200 patients in the study received general anaesthetic and gave their informed consent to allow for aspiration of bone marrow during their procedure from the greater tuberosity of the proximal humerus. The average age of the patients at the time of imaging and surgery was 61.2 years (range, 45–75 years). Men represented 62 % of cases (124/200), while 67 % (134/200) involved the dominant side.
Patients
The control group (group 1) consisted of 45 males and 30 females with a mean age of 59.4 years (range 45–73). None of the control group patients had any evidence of rotator cuff tear, but required a surgical procedure involving the shoulder. The study group (group 2) consisted of patients with rotator cuff injuries with a mean age of 62.3 years (range, 46–75).
Evaluation of the rotator cuff tears
Each patient underwent an evaluation of the rotator cuff, as well as an analysis of the number of MSCs in aspirate samples from the greater tuberosity and the iliac crest. All patients (even those without shoulder symptoms) had an MRI. Group 1 patients had a normal rotator cuff on their MRI (an asymptomatic rotator cuff injury was a cause of exclusion of the study) with muscles graded stage 0–1 for fatty infiltration.
We identified and characterized the rotator cuff tears [23, 27, 29] based upon pre-operative CT arthrogram or MRI, or both when available. Rotator cuff tears (Table 1) were identified on pre-operative images and confirmed intra-operatively and ranged from isolated single tendon tears to massive multiple tendon tears. Patients with full thickness tears of at least one tendon were included in this study. The rotator cuff tears (Table 1) involved one tendon in 54 shoulders, two tendons in 35, three tendons in 20 shoulders and four tendons in 16 shoulders. The supraspinatus was involved in 94 % of cases (118/125), the subscapularis in 44 % (55/125), the infraspinatus in 50 % (62/125), and the teres minor in 13 % (16/125).
The aetiology of the rotator cuff tear was classified as traumatic (those patients who recalled a specific traumatic event), degenerative (those who did not recall a single incident), or acute on chronic. The acute on chronic type was defined as a patient with chronic shoulder symptoms who experienced an acute traumatic event that exacerbated the chronic symptoms and motivated the patient to seek formal treatment. The aetiology of the rotator cuff tear was traumatic in 42 of the 125 cases (34 %), degenerative in 50 (40 %), and acute on chronic in 33 (26 %). Disease onset was considered to be the traumatic event when the aetiology was traumatic or the beginning of pain when the aetiology was degenerative. In the case of acute on chronic shoulders, we considered two onsets, with the first as degenerative, and the second as “trauma-like”.
We graded only fatty infiltration of the supraspinatus (tear present in 94 % of the shoulders) using either the CT arthrogram (soft-tissue sequences) and the classification of Goutallier et al. [12] or MRI (T1 sequences) and the classification developed by Fuchs et al. [9].
Evaluation of the number of MSCs with bone marrow aspiration
Bone marrow was collected from the humeral head of patients at the beginning of surgery, just before skin incision through a transdeltoid approach under general anaesthesia. Bone-marrow punctures were carried out under fluoroscopic control in the tuberosity at the level of the rotator cuff tears or rotator cuff insertion (in control patients). The number of mononucleated cells was determined by counting marrow smears on a hemocytometer and then normalizing the counts to the volume of marrow aspirated. The number of colony-forming unit fibroblasts (CFU-F) was determined as an indication of the number of mesenchymal stem cells present in the bone marrow. The assay was done as previously described [17, 18].
Statistical analysis
Each experiment was performed in triplicate. Data are reported as mean ± standard deviation. The non-parametric Mann-Whitney U test and the Spearman rank correlation coefficient were used to measure the relationship between variables. The chi square test was used to identify trends with categorical variables.
We used multiple regression analysis to determine the influence of several factors on the decrease of mesenchymal stem cells at the tendon–bone interface tuberosity, including increasing patient age, delay between onset of symptoms and diagnosis, aetiology, size of the tear, number of involved tendons, and severity of fatty infiltration. MSC content at the tendon–bone interface tuberosity was analysed by comparing shoulders with moderate decrease to shoulders with major and severe decrease, respectively, with chi square of the maximum likelihood test for qualitative variables. Major and severe amounts of decrease of mesenchymal stem cells at the tendon–bone interface tuberosity also were compared to each other. Levels of MSCs at the tendon–bone interface tuberosity were analysed with two-by-two and multivariate logistic regression to determine the influence of the same factors on the speed of appearance and progression of this phenomenon.
Results
(1) Control group without rotator cuff tears
In the absence of rotator cuff rupture, the concentration of MSCs per 1.0 mL of bone marrow aspirates in the tuberosity averaged 564 ± 216 MSCs/mL (range 745–378) with approximately a 50 % reduction over the 30 years separating the youngest and the oldest patients. Other factors, like side of pathology (dominant or not), gender, or the type of pathology treated were not significant.
(2) Study group with rotator cuff tears
In patients with a rotator cuff injury a significant decrease of mesenchymal stem cells at the tendon–bone interface tuberosity was observed in all patients. A significant decrease (214 ± 128 MSCs/mL; range 18–310) was observed for the MSC content in the tuberosities. A significant, but moderate decrease of the index ratio between the study group and the control group was considered when the index ratio was between 0.25 and 0.35, which corresponds to a decrease from 30 % to 50 % of the concentration of MSCs expected in the tuberosity of a patient of the same age without a rotator cuff tear. Similarly, a major decrease was considered when the index dropped down to between 0.15 and 0.25 (decrease from 50 % to 70 %), while a severe decrease was considered when the index was <0.15 (decrease higher than 70 %). A significant, but moderate decrease was present in 56 shoulders, which corresponds to a decrease from 30 % to 50 % of the concentration of MSCs expected in the tuberosity of a patient of the same age without a rotator cuff tear. Similarly, a major decrease (40 shoulders) was considered when there was a decrease from 50 % to 70 %, while a severe decrease (29 shoulders) was considered for a decrease higher than 70 %.
Temporally, the degree of the decrease of MSCs at the tendon–bone interface tuberosity correlated with the increase time from onset of rotator cuff symptoms in terms of severity. MSCs at the tendon–bone interface tuberosity decreased (p < 0.01) as more time elapsed between the onset of symptoms and surgery of rotator cuff tear for all types of ruptures (traumatic, acute on chronic and degenerative; Table 2). On average, a moderate decrease occurred within one year (11.9 ± 4.8 months) after the onset of symptoms, a major decrease occurred between one and two years (19.7 ± 7.8 months) after the onset of symptoms, and a severe decrease occurred after two years (30.3 ± 14 months) from the onset of symptoms. In traumatic tears, where the delay can be theoretically precisely determined, a moderate decrease of MSCs at the tendon–bone interface tuberosity occurred on average within four months (3.2 ± 2.8 months) after onset of symptoms, a major decrease occurred with an average of eight months (8.4 ± 4.7 months) and a severe decrease with an average of 12 months (12.2 ± 5.7 months) after the onset of injury. Consequently, the severity of MSC loss in traumatic injury appeared to progress significantly more quickly than after degenerative tears (Table 3). However, when traumatic and acute on chronic shoulders were compared, the progression was similar when the “trauma like” onset was selected, which means that the rate of MSC decrease in degenerative tears becomes significant only after the occurrence of the rupture and not during the painful period with tendinitis.
Significant (p < 0.01) variations also were observed in the severity MSC content loss according to the number of tendons torn (Table 3), such that the MSC content loss was rated as moderate for ruptures of one tendon, while the MSC content loss was severe in patients with massive rotator cuff tears involving three or four tendons. The level of MSC decrease at the tendon–bone interface tuberosity was more severe in tears with higher stages of fatty infiltration (Table 4). The average age of patients (Table 5) with a severe decrease was 68 years (range, 60–75 years), which was higher (p < 0.01) than in patients with a major decrease at 61 years (range, 52–73 years) or moderate decrease at 54 years (range, 45–67 years). One of the more important predictors for the rate of loss of MSCs was determined to be the time between onset of symptoms and surgery, even when compared to factors like the number of involved tendons or age or fatty infiltration.
Overall, the majority of tears with less than six months after the onset of injury before treatment, with one tendon rupture, with a tear size < 1 cm, and with a fatty degeneration stage 0 or 1 had a moderate decrease in the MSC content at the tendon–bone interface tuberosity, in contrast with tears treated after more than two years following injury onset, or with three tendons ruptured, or with a tear size > 3 cm, or with a fatty degeneration stage 3 or 4, which all had a severe decrease.
Discussion
Despite the current literature [1, 6, 10, 21] describing the importance of biologic abnormalities in RCT and the biologic strategies [2, 5, 30–33] to improve tendon to bone healing, the association between biological abnormalities and RCT has not been investigated previously and is poorly defined. In this study, we evaluated the MSC content in the tuberosities of the humeral head of patients with and without rotator cuff tear. Understanding the relationship of the number of MSCs and rotator cuff muscle tears, as well as clinical and temporal factors that might influence the MSC levels in the greater tuberosity of affected shoulders, may help physicians to better understand outcomes or provide patients with better prognostic information. The goals of our study were, therefore, to determine the status of MSC content in patients with and without rotator cuff tears, identify factors related to the changes in the level of MSCs after rotator cuff injury, determine the speed of appearance and progression of this phenomenon, and assess the role of a variety of factors in contributing to the levels of MSCs in the tuberosity of RCT patients, including assessing the role of the size of the tear, the number of tendon tears, the fatty infiltration and the age of patients, since all of these factors are considered as pejorative for healing.
We demonstrated that after a rotator cuff tear there is a significant decrease in the level of MSCs in the bone marrow of the proximal humerus at the tendon–bone interface tuberosity. Overall, the lag time between the onset of rotator cuff symptoms and rotator cuff repair plays a major role in the decrease of MSCs in the affected tuberosity. For traumatic tears, the time of onset of symptoms is easier to determine than in other types (degenerative or acute on chronic). In the case of traumatic tears, we observed that the level of MSC decrease was moderate in patients with small tears that were diagnosed and treated early after the onset of symptoms. A severe decrease in the level of MSCs developed in patients for whom one year or more had elapsed between the initial incident/onset of symptoms and surgery, and was particularly important in patients with several tendon tears and who were older [24].
Our study has some limitations, namely, our choice of symptoms onset corresponding with the occurrence of pain in degenerative tears may limit the study because some tears are asymptomatic and the decrease of MSCs may precede the symptom onset. However, as demonstrated by Yamaguchi et al. [33], asymptomatic tears are usually small, becoming symptomatic as their size increases. If the decrease of MSCs is moderate in small symptomatic tears, we can presume that it is moderate or absent in asymptomatic small tears. Second, we analysed several tear patterns but only in the case of full thickness tears. Obviously, application of the current systems of classification can result in an oversimplification of the factors of tear morphology and retraction. In addition, some variables are a function of the time of rotator cuff tear onset, so that tear size and fatty degeneration will vary over time. However, the approaches we have taken allow assessing factors that surgeons could consider in their evaluation of level of MSCs at the tendon–bone interface tuberosity.
Overall, the findings in this study provide a context for surgeons who use biologic augmentation [1–8, 27–33] in treating rotator cuff tears. Since MSCs found in bone marrow concentrate have been demonstrated to provide therapeutic benefit in a wide range of orthopaedic pathologies, it is important to understand the strategy for their use in treating rotator cuff tears. In particular, this study has shown that the level of MSCs present in the greater tuberosity of patients with a rotator cuff tear decreases as a function of a number of clinical factors, including lag time from tear onset to treatment, tear size, number of tears and stage of fatty infiltration, among others. Understanding the influence of age and number of tendons torn, as well as the time interval between the onset of rotator cuff symptoms and treatment on the loss of MSCs in the affected shoulder could serve as a guide to define patient expectations, and improve the best practices in using biologic augmentation of a rotator cuff repair. As a first result of this observation, it is potentially counterproductive to remove bone marrow from a patient’s injured shoulder and instead supports aspirating bone marrow from the patient’s iliac crest as a source of bone marrow-derived MSCs. Future studies will help to confirm the findings of this study and their usefulness in clinical practice.
References
Awad HA, Butler DL, Boivin GP, Smith FN, Malaviya P, Huibregtse B et al (1999) Autologous mesenchymal stem cell-mediated repair of tendon. Tissue Eng 5:267–77
Barber FA, Hrnack SA, Snyder SJ, Hapa O (2011) Rotator cuff repair healing influenced by platelet-rich plasma construct augmentation. Arthroscopy 27:1029–35
Bigliani LU, Cordasco FA, McIlveen SJ, Musso ES (1992) Operative treatment of failed repairs of the rotator cuff. J Bone Joint Surg Am 74:1505–1515
Boileau P, Brassart N, Watkinson DJ, Carles M, Hatzidakis AM, Krishnan SG (2005) Arthroscopic repair of full-thickness tears of the supraspinatus: does the tendon really heal? J Bone Joint Surg Am 87:1229–1240
Chang CH, Chen C, Su C, Liu H, Yu C (2009) Rotator cuff repair with periosteum for enhancing tendon–bone healing: a biomechanical and histological study in rabbits. Knee Surg Sports Traumatol Arthrosc 17:1447–1453
Chen JM, Willers C, Xu J, Wang A, Zheng MH (2007) Autologous tenocyte therapy using porcine-derived bioscaffolds for massive rotator cuff defect in rabbits. Tissue Eng 13:1479–91
Dines JS, Grande DA, Dines DM (2007) Tissue engineering and rotator cuff tendon healing. J Shoulder Elb Surg 16(5):S204–S207
Ellera Gomes JL, da Silva RC, Silla LM, Abreu MR, Pellanda R (2011) Conventional rotator cuff repair complemented by the aid of mononuclear autologous stem cells. Knee Surg Sports Traumatol Arthrosc 1607–9
Fuchs B, Weishaupt D, Zanetti M, Hodler J, Gerber C (1999) Fatty degeneration of the muscles of the rotator cuff: assessment by computed tomography versus magnetic resonance imaging. J Shoulder Elb Surg 8:599–605
Funakoshi T, Majima T, Iwasaki N, Suenaga N, Sawaguchi N, Shimode K et al (2005) Application of tissue engineering techniques for rotator cuff regeneration using a chitosan-based hyaluronan hybrid fiber scaffold. Am J Sports Med 33:1193–201
Galatz LM, Ball CM, Teefey SA, Middleton WD, Yamaguchi K (2004) The outcome and repair integrity of completely arthroscopically repaired large and massive rotator cuff tears. J Bone Joint Surg Am 86-A:219–224
Goutallier D, Postel JM, Lavau L, Voisin MC (1994) Fatty muscle degeneration in cuff ruptures. Pre and postoperative evaluation by CT scan. Clin Orthop Relat Res 304:78–83
Gulotta LV, Kovacevic D, Ehteshami JR, Dagher E, Packer JD, Rodeo SA (2009) Application of bone marrow-derived mesenchymal stem cells in a rotator cuff repair model. Am J Sports Med 37:2126–2133
Harryman DT II, Mack LA, Wang KY, Jackins SE, Richardson ML, Masten FA (1991) Repairs of the rotator cuff. Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am 73:982–989
Hernigou P, Flouzat-Lachaniette CH, Delambre J, Poignard A, Allain J, Chevallier N, Rouard H (2015) Osteonecrosis repair with bone marrow cell therapies: state of the clinical art. Bone 70:102–9
Hernigou P, Flouzat Lachaniette CH, Delambre J, Zilber S, Duffiet P, Chevallier N, Rouard H (2014) Biologic augmentation of rotator cuff repair with mesenchymal stem cells during arthroscopy improves healing and prevents further tears: a case-controlled study. Int Orthop 38(9):1811–8
Hernigou P, Homma Y, Flouzat-Lachaniette CH, Poignard A, Chevallier N, Rouard H (2013) Cancer risk is not increased in patients treated for orthopaedic diseases with autologous bone marrow cell concentrate. J Bone Joint Surg Am 95(24):2215–21
Hernigou P, Poignard A, Beaujean F, Rouard H (2005) Percutaneous autologous bone-marrow grafting for nonunions. Influence of the number and concentration of progenitor cells. J Bone Joint Surg Am 87:1430–7
Isaac C, Gharaibeh B, Witt M, Wright VJ, Huard J (2012) Biologic approaches to enhance rotator cuff healing after injury. J Shoulder Elb Surg 21:181–190
Jost B, Zumstein M, Pfirrmann C, Gerber C (2006) Long-term outcome after structural failure of rotator cuff repairs. J Bone Joint Surg Am 88:472–479
Kobayashi M, Itoi E, Minagawa H, Miyakoshi N, Takahashi S, Tuoheti Y et al (2006) Expression of growth factors in the early phase of supraspinatus tendon healing in rabbits. J Shoulder Elb Surg 15:371–7
Kovacevic D, Rodeo S (2008) Biological augmentation of rotator cuff tendon repair. Clin Orthop Relat Res 466:622–633
Liem D, Lichtenberg S, Magosch P, Habermeyer P (2007) Magnetic resonance imaging of arthroscopic supraspinatus tendon repair. J Bone Joint Surg Am 89:1770–1776
Maijenburg MW, Kleijer M, Vermeul K, Mul EP, van Alphen FP, van der Schoot CE, Voermans C (2012) The composition of the mesenchymal stromal cell compartment in human bone marrow changes during development and aging. Haematologica 97(2):179–83
Mazzocca AD, McCarthy MB, Chowaniec DM, Cote MP, Arciero RA, Drissi H (2010) Rapid isolation of human stem cells (connective tissue progenitor cells) from the proximal humerus during arthroscopic rotator cuff surgery. Am J Sports Med 38(7):1438–47
Mazzocca AD, McCarthy MB, Chowaniec D, Cote MP, Judson CH, Apostolakos J, Solovyova O, Beitzel K, Arciero RA (2011) Bone marrow-derived mesenchymal stem cells obtained during arthroscopic rotator cuff repair surgery show potential for tendon cell differentiation after treatment with insulin. Arthroscopy 27(11):1459–71
Mellado JM, Calmet J, Olona M, Esteve C, Camins A, Perez Del Palomar L, Gine J, Sauri A (2005) Surgically repaired massive rotator cuff tears: MRI of tendon integrity, muscle fatty degeneration, and muscle atrophy correlated with intraoperative and clinical findings. Am J Roentgenol 184:1456–1463
Murphy MB, Moncivais K, Caplan AI (2013) Mesenchymal stem cells: environmentally responsive therapeutics for regenerative medicine. Exp Mol Med 45:e54. doi:10.1038/emm.2013.94
Nakagaki K, Ozaki J, Tomita Y, Tamai S (1994) Alterations in the supraspinatus muscle belly with rotator cuff tearing: Evaluation with magnetic resonance imaging. J Shoulder Elb Surg 3:88–93
Rodeo SA, Potter HG, Kawamura S, Turner AS, Kim HJ, Atkinson BL (2007) Biologic augmentation of rotator cuff tendon healing with use of a mixture of osteoinductive growth factors. J Bone Joint Surg Am 89:2485–2497
Seeherman HJ, Archambault JM, Rodeo SA, Turner AS, Zekas L, D’Augusta D et al (2008) rhBMP-12 accelerates healing of rotator cuff repairs in a sheep model. J Bone Joint Surg Am 90:2206–19
Seeherman HJ, Archambault JM, Rodeo SA, Turner AS, D’Augusta D, Li XJ, Smith E, Wozney JM (2008) rhBMP-12 accelerates healing of rotator cuff repairs in a sheep model. J Bone Joint Surg Am 90:2206–2219
Yamaguchi K, Ditsios K, Middleton WD, Hildebolt CF, Galatz LM, Teefey SA (2006) The demographic and morphological features of rotator cuff disease. A comparison of asymptomatic and symptomatic shoulders. J Bone Joint Surg Am 88:1699–1704
Acknowledgments
We thank Ted Sand and Richard Suzuki and the other members of Celling Biosciences for the review of the final manuscript, and their help in translation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Hernigou, P., Merouse, G., Duffiet, P. et al. Reduced levels of mesenchymal stem cells at the tendon–bone interface tuberosity in patients with symptomatic rotator cuff tear. International Orthopaedics (SICOT) 39, 1219–1225 (2015). https://doi.org/10.1007/s00264-015-2724-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-015-2724-8