
Abstract
Purpose
A new intraoperative filtered salvaged blood re-transfusion system has been developed for primary total hip arthroplasty (THA) that filters and re-transfuses the blood that is lost during THA. This system is intended to increase postoperative haemoglobin (Hb) levels, reduce perioperative net blood loss and reduce the need for allogeneic transfusions. It supposedly does not have the disadvantages of intraoperative cell-washing/separating re-transfusion systems, such as extensive procedure, high costs and need for specialised personnel. To re-transfuse as much as blood as possible, postoperatively drained blood was also re-transfused.
Methods
A randomised, controlled, blinded, single-centre trial was conducted in which 118 THA patients were randomised to an intraoperative autologous blood re-transfusion (ABT) filter system combined with a postoperative ABT filter unit or high-vacuum closed-suction drainage.
Results
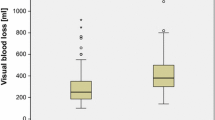
On average, 577 ml of blood was re-transfused in the ABT group: 323 ml collected intraoperatively and 254 ml collected postoperatively. Hb level was higher in the ABT vs the high-vacuum drainage group: 11.4 vs. 10.8 g/dl, p = 0.02 on day one (primary endpoint) and 11.0 vs. 10.4 g/dl, p = 0.007 on day three. Total blood loss was less in the autotransfusion group: 1472 vs. 1678 ml, p = 0.03. Allogeneic transfusions were needed in 3.6 % of patients in the ABT group and 6.5 % in the drainage group, p = 0.68.
Conclusion
The use of a new intraoperative ABT filter system combined with a postoperative ABT unit resulted in higher postoperative Hb levels and less total blood loss compared with a high-vacuum drain following THA.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Total hip arthroplasty (THA) is associated with a mean total blood loss of 1,500 ml and a postoperative decline in haemoglobin (Hb) levels of 3.0 g/dl [1]. It is important in THA to reduce perioperative net blood loss, to maintain higher postoperative Hb levels and to avoid the use of allogeneic blood transfusions as much as possible [2, 3]. One measure by which to try to achieve these goals is to implement autologous re-transfusion of blood lost during and after surgery. An advantage of intra- and postoperative autologous blood re-transfusion (ABT) is the good quality and direct contribution of the re-transfused red blood cells to oxygen transport and consumption and reduction of allogeneic blood transfusion requirement [4–9]. Postoperative ABT filter systems for re-transfusion of filtered drained blood are often used in primary THA. However, intraoperative cell-saver devices currently used in revision hip surgery are not used in primary THA because it is an extensive procedure with high costs. With these cell-saver devices, the blood is filtered and consecutively washed, the different cell types are separated and the red blood cells are subsequently re-transfused. Consequently, the 500 ml of blood, and thus suitable red blood cells that are directly available for autotransfusion, is lost during THA [4, 6–9]. Therefore, a new system has been developed for use during primary THA that filters the intraoperatively collected blood in the same manner as commonly used for postoperative blood loss. Subsequently, intraoperative filtered blood can be re-transfused. This system is intended to increase postoperative Hb levels, reduce the need for allogeneic blood transfusions and be less expensive and easier to handle than intraoperative cell-washing/separating devices and therefore suitable for general use in primary THA.
Combined intra- and postoperative re-transfusion delivers the maximum re-transfusion of autologous red blood cells lost during THA. We therefore conducted a prospective randomised controlled trial to evaluate the effects of this new intraoperative autologous filtered salvaged blood re-transfusion system combined with a postoperative ABT filter unit and compare it with a closed-suction high-vacuum drainage system following primary THA.
Materials and methods
This is an open, double-blind, randomised controlled single-centre study. Approval of our institutional medical ethics committee was obtained for this study in which 118 patients scheduled for primary THA were randomised to either the intraoperative and postoperative autologous transfusion group (Sangvia, intraoperative and postoperative autologous blood-salvage unit, low vacuum, 100–150 mmHg, Astratech, Mölndal, Sweden) or to the high-vacuum closed-suction drainage group (Redon, Medinorm AG, Quierschied, Germany). In the ABT, intraoperatively suctioned blood and postoperatively drained blood was re-transfused after filtering through 200-, 80- and 40-μm filters consecutively. Patients were enrolled based on the following inclusion criteria: provision of written informed consent and undergoing primary THA. Exclusion criteria were coagulation disorders, including deep venous thrombosis and pulmonary embolism; malignancy; ongoing infections; untreated hypertension; unstable angina pectoris; myocardial infarction within the past 12 months; coronary bypass surgery within the past 12 months; renal dysfunction; anticoagulant intake or participation in other clinical trials dealing with any drugs that affect blood loss.
Formal randomisation and concealed allocation took place prior to the operation. Sealed and numbered opaque envelopes containing pre-randomised cards to either the autologous transfusion group or the drainage group were available in the operating room. Intraoperatively lost blood was suctioned and collected for all 118 patients. The surgeons were blinded to group allocation until the end of surgery, just before wound closure, at which time the envelope was opened and the patient’s allocation group was disclosed.
In the ABT group, blood collected during the operation was subsequently re-transfused, and a drain with a postoperative re-transfusion unit was inserted. Postoperatively drained blood was re-transfused within six hours of surgery. A closed-suction high-vacuum drain was inserted in the control (drain) group; intraoperatively suctioned blood was not re-transfused in this group. In both groups, the drains were removed 24 hours postoperatively.
All patients were operated at Isala Clinics, Zwolle, The Netherlands. Cemented hip prostheses (SP-2 stem, Fal cup, Link, Hamburg, Germany), uncemented prostheses [Bimetric stem, Recap cup, Biomet, Warsaw (IN), USA] and hybrid prostheses of these components were used in the study. Surgeons used either the posterolateral or anterolateral approach.
Measurements were taken when patients attended the clinic preoperatively, during hospital stay and six weeks and three months postoperatively. The primary endpoint of this study was Hb level on the first postoperative day. Secondary endpoints were Hb levels on the second and third postoperative days, the lowest postoperative Hb level, blood loss during surgery, volume of intraoperatively suctioned and re-transfused blood, volume of re-transfused drained wound blood, allogeneic blood transfusions, postoperative pain, hospital stay, adverse events and total blood loss. Total blood loss was calculated according to Gross based on the maximum perioperative decrease in Hb level and the patient’s preoperative blood volume: blood loss = preoperative blood volume x (Hb preoperative – Hb lowest)/Hb average. Preoperative blood volume was calculated as 65 ml/kg. Hb average is average of preoperative Hb level and lowest postoperative Hb level [10].
Operation time, surgical approach, type of anaesthesia and patient’s temperature at the end of surgery were assessed because of their potential effects on blood loss. Creatinine levels and estimated glomerular filtration rate (eGFR) according to the Modification of Diet in Renal Disease (MDRD) formula were recorded because of the possible negative effect on kidney function of free Hb in high concentrations. A preoperative creatinine level greater than 125 μmol/L was the exclusion criterion for renal dysfunction. Pain at rest and during exercise was scored on a visual analogue scale (VAS). Adverse events were registered during hospital stay and the first three months postoperatively. The physicians who performed postoperative examinations at the outpatient clinic were blinded to group allocation. A standardised blood management protocol was implemented for this study, as follows:
-
Venous thromboembolism prophylaxis was carried out using fondaparinux (Arixtra®, 2.5 mg/0.5 ml) subcutaneously once daily. The first dose was administered on the evening of the day of surgery and was continued for five weeks.
-
Administration of nonselective nonsteroidal anti-inflammatory drugs (NSAID)s was stopped one day before surgery. The COX-2-selective NSAID meloxicam 15 mg once daily was used in all patients.
-
Additional allogeneic blood transfusions were given based on the Dutch allogeneic blood transfusion guidelines [11]. The trigger for allogeneic transfusions was an Hb level of 6.4 g/dl in patients with American Society of Anaesthesiologists (ASA) physical classification 1, 8.0 g/dl in ASA classifications 2 and 3, and 9.6 g/dl in ASA classification 4, as well as in those whose cardiac output failed to increase to compensate for dilution [11].
Statistical analysis
Based on a clinically relevant difference in Hb level on the first postoperative day of 0.8 g/dl [10.2 g/dl vs. 11.0 g/dl, standard deviation (SD)] 1.4 [12], alpha of 0.05 and power of 80.8 %, a sample size of 115 patients (50 per group plus 15 %) was required for this study. Study data were collected using customised case report forms and entered into a computerised database that allowed unbiased and reliable data management. Categorical data were expressed as percentages. Continuous data were expressed as means and SD. Based on an intention-to-treat analysis, differences were analysed using chi-squared tests for categorical data and Student’s t tests for continuous data. The Levene test was used to check for test assumptions. A two-sided p < 0.05 was considered statistically significant.
Results
Patients were operated upon between August 2008 and May 2009. The study had an enrolment of 118 patients: 56 in the ABT group and 62 in the drain group without re-transfusion. The groups were statistically homogeneous with respect to gender, age, body mass index, medical history, Charnley osteoarthritis classification and indication for operation (Table 1). With the exception of operation time, which was six minutes longer in the drain group (p = 0.04), there were no significant differences between groups regarding anaesthetic or surgical parameters that could affect blood loss, such as type of anaesthesia, body temperature, surgeon, surgical approach or prosthetic fixation.
Perioperative blood loss, autologous transfusion, Hb levels
Total intraoperatively suctioned blood loss was similar in both groups: 537 ml in the ABT group and 555 ml in the drain group (Table 1). Of this blood loss, approximately 415 ml was collected with the re-transfusion suction unit and approximately 130 ml with a different suction unit. On average, 323 ml of the 415 ml intraoperatively collected blood in the ABT group was re-transfused. In one patient in the ABT group, intraoperatively collected blood was not re-transfused. In the ABT group, on average, 254 ml of postoperatively drained blood was re-transfused within six hours of surgery and was re-transfused in 46 patients (82 %). In eight patients, only a small volume of wound blood was collected, which was not sufficient to be re-transfused. In two patients, a technical failure of the system occurred. In the ATB group, a mean of 577 ml of intraoperatively and postoperatively lost blood was re-transfused. The maximum re-transfusion of intraoperatively collected blood was 850 ml, the maximum re-transfusion of postoperatively collected blood was 960 ml and the maximum total re-transfused blood in a patient was 1,260 ml.
The Hb level on the first postoperative day, primary endpoint of the study, was significantly higher in the ABT than in the drain group, as it was also on the third postoperative day (Table 2). The mean lowest postoperative Hb level was also significantly different. The decline in Hb level from preoperatively to the first and third postoperative days was also less in the ABT group, i.e. −2.8 ± 0.9 vs. −3.3 ± 0.9 (p = 0.007) and −3.2 ± 1.2 vs. −3.7 ± 1.1 (p = 0.01). Allogeneic blood transfusions were needed in 3.6 % (two patients) in the ABT group and 6.5 % (four patients) in the drain group (p = 0.68.) In the ABT group, the four allogeneic transfusions were given on the second postoperative day. In the drain group, seven allogeneic transfusions were given in three patients postoperatively on the day of surgery, and two were given in one patient on the second postoperative day. Total blood loss was less in the ABT group compared with the drain group (Table 2).
Pain scores, hospital stay
Pain scores were similar for both groups preoperatively, during hospital stay, and six weeks and three months postoperatively (Table 2). Length of hospital stay was also similar in both groups: 4.5 ± 1.2 days in the ABT group and 4.3 ± 1.0 days in the drain group, p = 0.48. Most patients were discharged on a predetermined discharge date.
Adverse events
Adverse events during hospital stay and afterwards up to three months postoperatively were similar between groups (Table 3). One patient with a preoperative high creatinine level, 164 μmol/L, was included. Moreover, 17 patients with suboptimal GFR, MDRD <60, were included: six in the ABT group and 11 in the drain group. No statistically significant differences were noted in creatinine levels, or GFR MDRD preoperatively or during hospital stay.
Discussion
In this study, the use of a new intraoperative ABT filter system combined with a postoperative ABT filter unit resulted in higher Hb levels on both the first (primary endpoint) and third postoperative days and in less total blood loss compared with the commonly used high-vacuum drainage system following primary THA. Higher pre- and postoperative Hb levels are correlated with better early functional recovery, higher patient satisfaction and shorter hospital stay following THA [2, 3]—although not substantiated in every study [13]—and with a reduced allogeneic blood transfusion rate [2, 3, 13, 14]. Allogeneic blood transfusions are related with poorer outcomes following THA, such as a higher postoperative infection rate, delayed wound healing and prolonged hospital stay. An advantage of autologous re-transfusion is the direct contribution of the re-transfused red blood cells to oxygen consumption in the patient [4, 6–9]. This is in contrast to red blood cells in allogeneic transfusions from a blood bank in which optimal contribution to oxygen consumption may take several hours because of so-called storage lesions [15, 16] .
Many surgeons prefer to use a drain following THA to reduce the risk of haematoma. In THA, the use of a postoperative ABT system only significantly reduced allogeneic blood transfusions in one study when compared with a closed-suction drainage system, but this was not so in another study, and not when compared with no drainage system [12, 17, 18]. One randomised controlled trial was published on the comparison of the same intra- and postoperative ABT system used in this study compared with no drain after primary THA. The study showed less perioperative blood loss and less decrease in maximum postoperative Hb but no significant difference in Hb levels on days one, two and three [19].
Studies on intraoperative cell salvage with intraoperative cell-washing/separating ABT show that this system is not cost effective in primary THA [20, 21]. Moreover, it is an extensive procedure that needs personnel from the anaesthesia department. Therefore, these intraoperative cell-washing/separating devices are currently not used in primary THA despite the 500-ml blood with red blood cells of good quality that is suitable for autotransfusion. To re-transfuse as much of the perioperatively lost blood as possible in THA, intraoperatively and postoperatively collected blood was re-transfused in our study. The intraoperative filter system used in this study is assumed to be less expensive and can be used without an extensive training programme. Costs of the combined intra- and postoperative ABT filter system used in this study were around $180: approximately $140 for the intraoperative unit and approximately $40 for the postoperative unit. The ABT system comprises disposable components; there is no need to purchase a cell-saver machine, and there are no maintenance costs. However, this study was not set up as a cost-effectiveness analysis.
In this study, approximately 550 ml of blood was lost and collected during surgery. Not all available intraoperatively lost blood was suctioned with the re-transfusion system and autotransfused. This was partly due to unfamiliarity with the re-transfusion system and partly on purpose: e.g. a different suction unit was used while cementing the prosthesis. In the autotransfusion group, a mean of 323 ml of intraoperative blood loss and 254 ml of postoperative blood loss, totalling 577 ml, was re-transfused, resulting in less net total blood loss and higher postoperative Hb levels. There was no significant difference in allogeneic blood transfusions that may be affected by the strict Dutch transfusion trigger. Restrictive transfusion triggers seem to be safe for most surgical patients when appropriately implemented [22]. The introduction of a strict transfusion trigger, such as the Dutch allogeneic blood transfusion guidelines, has decreased the postoperative allogeneic blood transfusion rate by 20–50 % [11, 23–26]. Other larger studies powered on allogeneic transfusion rate are needed. Moreover, functional scores might be addressed in these studies.
Adverse events during hospital stay and during the first three months postoperatively were similar in both groups. Free Hb, which is released into the wound during surgery, may be harmful to the kidneys in high concentrations. Special attention was therefore paid to renal function, and patients with a history of renal dysfunction were not included in the study. One patient with a preoperatively high creatinine level was unintentionally included. Moreover, 17 patients with suboptimal kidney clearance were included. Despite this, kidney clearance did not deteriorate after surgery in either group. This study showed no statistically significant differences in creatinine levels, or GFR between groups. However, the study was not powered to detect differences in adverse events.
The strength of the study is its prospective randomised controlled design. Furthermore, surgeons were blinded to patient group allocation until the end of surgery, as were the research physicians during follow-up. Moreover, the primary endpoint was based on blinded laboratory analysis. Other perioperative factors that might affect blood loss were examined also, and no differences were seen in these factors between groups. The limitation of the study is that not all available intraoperatively suctioned blood suitable for re-transfusion was autotransfused.
In conclusion, the use of a new intraoperative autologous filtered salvaged blood re-transfusion system combined with a postoperative ABT unit resulted in higher postoperative Hb levels and less total blood loss compared with a high-vacuum closed-suction drain following primary THA.
References
Sehat KR, Evans RL, Newman JH (2004) Hidden blood loss following hip and knee arthroplasty. Correct management of blood loss should take hidden loss into account. J Bone Joint Surg Br 86:561–565
Conlon NP, Bale EP, Herbison GP, McCarroll M (2008) Postoperative anemia and quality of life after primary hip arthroplasty in patients over 65 years old. Anesth Analg 106:1056–61, table
Husted H, Holm G, Jacobsen S (2008) Predictors of length of stay and patient satisfaction after hip and knee replacement surgery: fast-track experience in 712 patients. Acta Orthop 79:168–173
Colwell CW Jr, Beutler E, West C, Hardwick ME, Morris BA (2002) Erythrocyte viability in blood salvaged during total joint arthroplasty with cement. J Bone Joint Surg Am 84-A:23–25
Carless, PA, Henry, DA, Moxey, AJ, O'Connell, D, Brown, T, and Fergusson, DA (2010) Cell salvage for minimising perioperative allogeneic blood transfusion. Cochrane Database Syst Rev CD001888-
Stachura A, Krol R, Poplawski T, Michalik D, Pomianowski S, Jacobsson M, Aberg M, Bengtsson A (2011) Transfusion of intra-operative autologous whole blood: influence on complement activation and interleukin formation. Vox Sang 100:239–246
Elawad AA, Ohlin AK, Berntorp E, Nilsson IM, Fredin H (1991) Intraoperative autotransfusion in primary hip arthroplasty. A randomized comparison with homologous blood. Acta Orthop Scand 62:557–562
Gharehbaghian A, Haque KM, Truman C, Evans R, Morse R, Newman J, Bannister G, Rogers C, Bradley BA (2004) Effect of autologous salvaged blood on postoperative natural killer cell precursor frequency. Lancet 363:1025–1030
Sinardi D, Marino A, Chillemi S, Irrera M, Labruto G, Mondello E (2005) Composition of the blood sampled from surgical drainage after joint arthroplasty: quality of return. Transfusion 45:202–207
Gross JB (1983) Estimating allowable blood loss: corrected for dilution. Anesthesiology 58:277–280
The Dutch Institute for Healthcare Improvement (CBO) (Allogenic Blood Transfusion Guideline. http://www.cbo.nl/Downloads/96/bloedrl2004.pdf. p109
Strumper D, Weber EW, Gielen-Wijffels S, Van DR, Bulstra S, Slappendel R, Durieux ME, Marcus MA (2004) Clinical efficacy of postoperative autologous transfusion of filtered shed blood in hip and knee arthroplasty. Transfusion 44:1567–1571
Vuille-Lessard E, Boudreault D, Girard F, Ruel M, Chagnon M, Hardy JF (2012) Postoperative anemia does not impede functional outcome and quality of life early after hip and knee arthroplasties. Transfusion 52:261–270
Saleh E, McClelland DB, Hay A, Semple D, Walsh TS (2007) Prevalence of anaemia before major joint arthroplasty and the potential impact of preoperative investigation and correction on perioperative blood transfusions. Br J Anaesth 99:801–808
Sparrow RL (2010) Red blood cell storage and transfusion-related immunomodulation. Blood Transfus 8(Suppl 3):s26–s30
Johnson BA, Weil MH (1991) Redefining ischemia due to circulatory failure as dual defects of oxygen deficits and of carbon dioxide excesses. Crit Care Med 19:1432–1438
Moonen AF, Knoors NT, van Os JJ, Verburg AD, Pilot P (2007) Re-transfusion of filtered shed blood in primary total hip and knee arthroplasty: a prospective randomized clinical trial. Transfusion 47:379–384
Horstmann WG, Kuipers BM, Slappendel R, Castelein RM, Kollen BJ, Verheyen CC (2012) Postoperative autologous blood transfusion drain or no drain in primary total hip arthroplasty? A randomised controlled trial. Int Orthop 36:2033–2039
Horstmann WG, Swierstra MJ, Ohanis D, Castelein RM, Kollen BJ, Verheyen CC (2013) Reduction of blood loss with the use of a new combined intra-operative and post-operative autologous blood transfusion system compared with no drainage in primary total hip replacement. Bone Joint J 95-B:616–622
Guerra JJ, Cuckler JM (1995) Cost effectiveness of intraoperative autotransfusion in total hip arthroplasty surgery. Clin Orthop Relat Res 212–222
Shulman G, Grecula MJ, Hadjipavlou AG (2002) Intraoperative autotransfusion in hip arthroplasty. Clin Orthop Relat Res 119–130
Muñoz M, Leal-Noval SR (2013) Restrictive transfusion triggers in major orthopaedic surgery: effective and safe? Blood Transfus 11:169–171
Carless, PA, Henry, DA, Carson, JL, Hebert, PP, McClelland, B, and Ker, K (2010) Transfusion thresholds and other strategies for guiding allogeneic red blood cell transfusion. Cochrane Database Syst Rev CD002042-
Grover M, Talwalkar S, Casbard A, Boralessa H, Contreras M, Boralessa H, Brett S, Goldhill DR, Soni N (2006) Silent myocardial ischaemia and haemoglobin concentration: a randomized controlled trial of transfusion strategy in lower limb arthroplasty. Vox Sang 90:105–112
Young SW, Marsh DJ, Akhavani MA, Walker CG, Skinner JA (2008) Attitudes to blood transfusion post arthroplasty surgery in the United Kingdom: a national survey. Int Orthop 32:325–329
Weber EWG, Slappendel R, Van der Schaaf DB, Oosting JD (2000) [Fifty percent reduction in packed cells by transfusion trigger protocol] Halvering van de toediening van packed cells bij geprotocolleerde indicatie stelling. Nederlands Tijdschrift voor Orthopedie 7:10–12
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Horstmann, W.G., Swierstra, M.J., Ohanis, D. et al. Favourable results of a new intraoperative and postoperative filtered autologous blood re-transfusion system in total hip arthroplasty: a randomised controlled trial. International Orthopaedics (SICOT) 38, 13–18 (2014). https://doi.org/10.1007/s00264-013-2084-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00264-013-2084-1