
Abstract
Purpose
The objective of this study was to evaluate the role of 68Ga-DOTATOC positron emission tomography (PET)/CT scan in patients with suspected pulmonary carcinoid tumour and to compare its results with 18F-fluorodeoxyglucose (FDG) PET/CT scan.
Methods
In this prospective study, 32 patients (age 34.22 ± 12.03 years; 53.1 % female) with clinical suspicion of bronchopulmonary carcinoid were evaluated with 68Ga-DOTATOC PET/CT and 18F-FDG PET/CT. The two imaging modalities were compared, considering the tissue diagnosis as the reference standard.
Results
Based on the reference standard 26 cases were carcinoid tumours [21 typical carcinoids (TC) and 5 atypical carcinoids (AC)] and 6 cases were non-carcinoid tumours. The sensitivity, specificity and accuracy of 68Ga-DOTATOC PET/CT in the diagnosis of pulmonary carcinoid tumour were 96.15, 100 and 96.87 % respectively, whereas those of 18F-FDG PET/CT were 78.26, 11.1 and 59.37 % respectively. The maximum standardised uptake value (SUVmax) of TC on 68Ga-DOTATOC PET/CT scan ranged from 3.58 to 55, while that of AC ranged from 1.1 to 32.5. 18F-FDG PET/CT was true-positive in all cases of AC and false-negative in eight cases of TC (sensitivity for TC 61.9 % and for AC 100 %).
Conclusion
68Ga-DOTATOC PET/CT is a useful imaging investigation for the evaluation of pulmonary carcinoids. 18F-FDG PET/CT scan suffers from low sensitivity and specificity in differentiating the pulmonary carcinoids from other tumours.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Bronchopulmonary neuroendocrine tumours (NETs) are a subset of bronchopulmonary neoplasms that share a distinctive basic microscopic appearance, resembling NETs found elsewhere in the body [1]. Bronchopulmonary NETs, representing 2 % of all lung tumours, are endobronchial in location in 90 % of the cases. They were classified as typical carcinoids (TC), atypical carcinoids (AC), large cell neuroendocrine carcinoma (LCNEC) and small cell neuroendocrine carcinoma (SCNEC) based on a number of features such as number of mitoses per high power field and the presence or absence of necrosis, nuclear pleomorphism, nuclear cytoplasmic ratio and many more [2]. Bronchial NETs account for approximately 24.5 % of well-differentiated NETs [3]. However, recent analysis of Surveillance, Epidemiology, and End Results (SEER) data put it as the most common site accounting for almost 32 % [4]. Among the carcinoids, TC are more common, constituting 65–90 %, with the remaining 10–35 % being AC [5–7].
The diagnosis of pulmonary carcinoid tumours can be made based on a number of biochemical investigations and imaging techniques. The imaging techniques include structural imaging with plain chest radiograph, computed tomography (CT), magnetic resonance imaging (MRI), functional imaging with somatostatin receptor scintigraphy (SRS), radioiodinated metaiodobenzylguanidine (MIBG) scan and positron emission tomography (PET) scan. However, there are no findings on conventional imaging that are specific for carcinoids [8]. They cannot assess the functional status of the tumour and cannot provide much information on tumour biology and degree of differentiation. Although various methods have been described for evaluation of carcinoid tumours, the gold standard is histopathological examination.
Carcinoid tumours are known to express somatostatin receptor (SSR) types 2 and 5. Functional imaging techniques like SRS, aimed at localising these receptors, suffers from low tumour to background contrast, low resolution for very small tumours and from the lack of accurate spatial resolution. 2-[18F]Fluoro-2-deoxy-D-glucose (FDG) PET/CT identifies the tumours based on their glucose metabolism. 18F-FDG PET/CT has low uptake in carcinoids because of their low metabolic activity and thus cannot accurately identify the nature of the lesion. 1, 4,7,10-Tetraazacyclododecane-N,N′,N″,N′″-tetraacetic acid-D-Phe1-Tyr3-octreotide (68Ga-DOTATOC) PET/CT scan offers the best possibility of detecting these tumours, with very high sensitivity and specificity rates with high spatial resolution. The usefulness of 68Ga-DOTATOC PET scan has been reported in assessing abdominal NETs [9]. However, there is only scant literature available addressing the role of 68Ga-DOTANOC PET/CT scan in the evaluation of pulmonary carcinoids [10].
The present study was planned to prospectively evaluate the role of 68Ga-DOTATOC PET/CT scan for suspected pulmonary carcinoids and compare its results with those of 18F-FDG PET/CT scan, using tissue diagnosis obtained at biopsy or surgery as the gold standard.
Materials and methods
This prospective analytical study was conducted after obtaining the approval of the Institutional Review Board. This study was conducted at the Department of Surgical Disciplines in collaboration with the Departments of Nuclear Medicine and Pulmonary Medicine at our institution. Written informed consent was obtained from all patients. Patients were recruited into the study during a span of 1 year and 10 months (February 2010 to November 2011).
Patients
A total of 32 patients with clinical suspicion of pulmonary carcinoid, presenting to the surgical and medical outpatient clinic, were included as the study group. Inclusion criteria were all patients with clinical suspicion of pulmonary carcinoid tumour based on history, examination or radiological findings. Children < 15 years of age, pregnant women, uncontrolled diabetics with blood sugar level of more than 140 mg/dl and patients who refused to give consent for the study were excluded from the study population.
The patients were included in the study, after having signed the informed written consent, underwent complete workup with an in-depth history taking, thorough clinical examination and complete routine blood investigations, chest radiograph and chest CT with bronchoscopy and biopsy whenever feasible. In those patients who underwent biopsy PET/CT scan was performed after a period of 6 weeks to avoid false-positive results. All patients underwent 18F-FDG PET/CT scan and 68Ga-DOTATOC PET/CT scan.
18F-FDG PET/CT imaging
PET scans were performed on a dedicated PET/CT scanner present in our institute (Siemens Biograph 64) as already reported [11]. After fasting for at least 4 h, verifying the serum glucose level (that should be below 140 mg/dl) and with patients in a resting state, in a quiet room, a dose of 370 MBq of 18F-FDG was injected intravenously. After a 45- to 60-min uptake period, patients were placed in the scanner. In the PET/CT system, non-contrast CT scan acquisition was performed on spiral dual slice CT with a slice thickness of 4 mm and a pitch of 1. After CT, 3-D PET acquisition was done from the skull to mid-thighs with 3–5 min per bed position. CT-based attenuation correction of the emission images was employed. PET images were reconstructed by the iterative method ordered subset expectation maximisation (2 iterations and 8 subsets) with a filter of 5 mm. After completion of PET acquisition, the reconstructed attenuation-corrected PET images, CT images and fused images of matching pairs of PET and CT images were available for review in axial, coronal and sagittal planes and in maximum intensity projections, 3-D cine mode.
68Ga-DOTATOC PET/CT imaging
68Ga-DOTATOC DOTA0-D-Phe1-Tyr3-octreotide was synthesised with a 1,110–1,850 MBq 68Ge/68Ga generator as previously reported [11]. 68Ga-DOTATOC PET/CT scan was obtained 45–60 min after intravenous injection of 74–111 MBq of the radiotracer. During the PET/CT acquisition all PET/CT parameters were kept the same as during 18F-FDG PET/CT scan, except 3-D PET acquisition timing, which was 5–8 min per bed position instead of 3–5 min per bed position in 18F-FDG PET/CT scan.
Interpretation of images
The PET/CT images were evaluated independently by two experienced nuclear medicine physicians. They were blinded to the clinical and structural imaging findings. Their findings were concordant in all cases. PET images were assessed for area of increased radiotracer uptake. Corresponding areas in the CT images and fused PET/CT images were corroborated. Any non-physiological focal area of increased 68Ga-DOTATOC or 18F-FDG uptake was looked for, keeping physiological tracer distribution in perspective. For 68Ga-DOTATOC PET/CT any non-physiological uptake more than surrounding tissue was taken as positive. Positive findings on 68Ga-DOTATOC and 18F-FDG PET were localised to anatomic images from the non-enhanced CT. For semi-quantitative analysis, a region of interest (ROI) was carefully drawn around the site of the abnormal 18F-FDG uptake in the consequent four to six PET/CT scan slices. The slice with a maximal 18F-FDG uptake in the ROI was chosen for semi-quantitative measurement of metabolic activity of the tracer [standardised uptake value (SUV)]. From these ROIs, the SUVmax was calculated. 68Ga-DOTATOC PET/CT images were also interpreted similarly. An ROI was drawn surrounding the uptake area and the SUVmax was calculated.
Reference standard
The sensitivity and specificity of 68Ga-DOTATOC PET/CT scan and 18F-FDG PET/CT scan were calculated considering tissue diagnosis (preoperative or post-operative) as gold standard.
Statistical analysis
The statistical package Stata 8.0 (StataCorp., College Station, TX, USA) and SPSS 16.0 (SPSS Inc., Chicago, IL, USA) were used for all statistical analyses. The data were expressed as mean wherever applicable. The sensitivity, specificity, positive and negative predictive values, false-positive rate, false-negative rate and accuracy of 18F-FDG PET/CT scan and 68Ga-DOTATOC PET/CT scan in evaluating pulmonary carcinoids were calculated.
Results
Patient characteristics
A total of 32 patients with a mean age of 34.22 (±12.03) years and age range of 16–71 years were evaluated. There were 15 men and 17 women. The overall demographic profile of all 32 patients, with their histological diagnosis, is described in Table 1. The incidence of TC was higher in the group aged 20–30 years, while AC were common in the groups aged 30–50 years. Cases of mucoepidermoid carcinoma (MEC) occurred in patients below 30 years of age, while cases of squamous cell carcinoma were found in those above 40 years of age.
Clinical presentation
The patients in our study group presented with a wide range of clinical manifestations, from being asymptomatic, to having overt chest symptoms and endocrine symptoms. The common clinical presenting symptoms in our patients have been summed up in Table 2. The duration of symptoms ranged from 1 month to as long as 4 years. One patient in our study was asymptomatic and was incidentally discovered to have a mass on a routine X-ray.
Radiological evaluation
All patients initially underwent a chest radiograph and later on contrast-enhanced CT of the chest was performed to further characterise the lesion. The chest radiograph was unremarkable in 5 patients, while in 15 cases it showed the presence of some hilar opacity, and in another 6 there was evidence of hilar opacity associated with collapse of the distal lung and significant loss of lung volume. In five cases there was evidence of parenchymal lesion, while in one patient a mass in the trachea could be visualised. On contrast CT of the chest, a well-defined enhancing mass along the bronchial tree was seen in 25 cases, of which 15 cases had associated collapse of the distal lung parenchyma and 3 had bronchiectatic changes in the distal parenchyma. There were five parenchymal lesions—three being a solitary pulmonary nodule and two being a lower lobe mass lesion (one right and one left). Two of the patients had lesions in the trachea with intratracheal and significant extraluminal extension. Thus according to the CT there were 27 central tracheobronchial lesions and 5 peripheral parenchymal lesions.
Bronchoscopy
The patients with central lesions underwent bronchoscopy, along with biopsy whenever feasible. Bronchoscopic evaluation was performed in 27 patients. The most common finding on bronchoscopy was a smooth walled vascular polypoidal lesion, often bleeding on touch. On the whole the right sided lesions were more common than left sided lesions. Location wise, the bronchus intermedius was the commonest site. It was seen that most of the carcinoid tumours were located within 2.5–3.5 cm from the carina.
Preoperative tissue diagnosis
Bronchoscopic biopsy could be taken in 25/27 patients in whom bronchoscopic evaluation was performed, while in the remaining 2 patients the attempt to obtain a bronchoscopic biopsy was abandoned due to bleeding. Five patients had a parenchymal lesion, where percutaneous transthoracic biopsy was attempted with image guidance (CT guidance) in three, while in two other patients, biopsy was not possible because of the small size of the lesion (~1 × 1 cm in size). In total 28 of 32 patients had a preoperative biopsy (bronchoscopic or image-guided biopsy). On retrospective analysis, these were compared with the histopathology of the operative specimen. It was seen that the preoperative tissue biopsy was concordant with post-operative biopsy in 17 patients (60.71 %), while it was discordant in 3 (10.71 %) and inconclusive in 3. Of the remaining five patients with a preoperative biopsy, one had undergone endobronchial resection only, one patient was inoperable and three more patients are yet to be operated, so there were no post-operative samples to compare and so the preoperative biopsy was taken as final. Among patients with carcinoid tumours 22/26 had a preoperative tissue diagnosis, of which 14 (63.6 %) were consistent with the post-operative histology, 3 were discordant (13.6 %), 2 were inconclusive and 3 more patients are yet to be operated as mentioned above. Of the three discordant reports two were reported as small cell carcinoma (post-operative biopsy was TC and AC).
Treatment analysis
Of the 32 patients enrolled in the study, 27 underwent surgical treatment. Of these 20 underwent parenchymal resection procedures (pneumonectomy, lobectomy, bilobectomy and wedge resection) while 5 underwent parenchyma-preserving surgeries (4 sleeve lobectomies and one sleeve bronchectomy) and the 2 tracheal tumours underwent resection and end-to-end anastomosis of the trachea. One of the patients (a case of MEC) underwent endobronchial resection for a mass in the left main bronchus, became asymptomatic post resection and is doing well at follow-up of 15 months. Surgical management remained the same irrespective of a typical or atypical nature of the carcinoids. Lymph node dissection was done routinely in all cases of carcinoid tumours, and lymph node metastasis was found in only one case, an AC.
Functional imaging
Evaluation of the tumours with 18F-FDG PET/CT scans
All 32 patients included in the study underwent 18F-FDG PET/CT scan as per the standard protocol described above. The range of SUVmax on 18F-FDG PET/CT scan for various types of tumours with their size is summarised in Table 3. 18F-FDG PET/CT was true-positive in 18/26 carcinoids. It was false-negative in eight cases of TC (Fig. 1) and true-positive in all cases of AC (Fig. 2). The sensitivity for TC and AC was 61.9 and 100 % respectively. AC revealed significantly higher uptake values on 18F-FDG PET/CT compared with the TC (p = 0.002) (Table 3). Among the non-carcinoid tumours included in the study, 18F-FDG PET/CT was positive in all cases except for one case of MEC.

Transaxial PET (a), CT (b) and PET/CT (c) images in a patient with TC inthe right lower lobe showing intense uptake on 68Ga-DOTATOC PET/CT scan (SUVmax 6.20). PET (d), CT (e) and PET/CT (f) images of the same patient showing no uptake on 18F-FDG PET/CT scan (SUVmax 0.74)

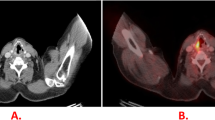
Transaxial PET (a), CT (b) and PET/CT (c) images in a patient with AC tumour of the right main bronchus showing intense uptake on 68Ga-DOTATOC PET/CT scan (SUVmax 32.5). PET (d), CT (e) and PET/CT (f) images of the same patient showing intense uptake on 18F-FDG PET/CT scan (SUVmax 8.45)
Evaluation of tumours by 68Ga-DOTATOC PET/CT scans
All 32 patients underwent 68Ga-DOTATOC PET/CT scan as per the standard protocol described earlier. The findings in different tumours along with the tumour size and tumour uptake (SUVmax) have been summed up in Table 3. Both TC (Fig. 1) and AC (Fig. 2) showed intense uptake on 68Ga-DOTATOC PET/CT against the background; however, there was one case of AC which failed to show uptake on 68Ga-DOTATOC PET/CT. None of the non-carcinoid tumours included in the study showed any uptake on 68Ga-DOTATOC PET/CT. Also of note is that 68Ga-DOTATOC PET/CT helped in identifying the presence of tumour metastasis to a mediastinal lymph node in the case of an AC. No other metastatic lesions were found in any of the other patients with bronchial carcinoids. TC revealed significantly higher uptake values on 68Ga-DOTATOC PET/CT compared with the AC (p = 0.003).
Based on the findings on 18F-FDG PET/CT scan and 68Ga-DOTATOC PET/CT, sensitivity, specificity, positive and negative predictive values, and accuracy were calculated for the diagnosis of pulmonary carcinoids (Table 4). It can be seen that 68Ga-DOTATOC PET/CT had a higher sensitivity and specificity than 18F-FDG PET/CT in the diagnosis of pulmonary carcinoid tumour especially in the TC tumours.
Discussion
The mean age of patients with TC was 31.24 ± 8.78 years, while that of those with AC was 39.60 ± 8.84 years. This was in keeping with the literature, wherein the patients with AC tend to be older than those with TC [7, 12]. Our study showed a higher prevalence of TC in comparison to AC as stated in the literature (4:1 ratio) [13]. In our study the most common presenting symptom among patients with carcinoid tumour was cough (80.76 %), which was also the commonest symptom reported by many other major studies [6, 14]. Most of the tumours were centrally located (~80 %) as reported in various studies [6, 15] and were more common on the right side (69.23 %). The predilection of carcinoids to affect the right lung is well described in the literature [6, 7]. Among patients with carcinoid tumours with a preoperative tissue diagnosis, three were discordant (13.6 %) of which two were reported as small cell carcinoma (post-operative biopsy was TC and AC). The literature also reports on carcinoids being misdiagnosed as small cell carcinoma in the preoperative biopsies [16].
Carcinoid tumours are rich in SSRs, so they typically show high uptake on 68Ga-DOTATOC PET/CT scan which targets these receptors. There have been various studies in the literature that have demonstrated the utility of 68Ga-DOTATOC PET/CT scan in the evaluation of various NETs, but data regarding its utility in pulmonary carcinoids are essentially less frequently reported [9, 17–23]. In our study, 68Ga-DOTATOC PET/CT scan successfully detected almost all of the patients with carcinoid tumours (sensitivity 96.15 % and specificity 100 %). The positive predictive value was 100 %, while the negative predictive value was 85.71 %. There was no false-positive case. One AC did not show any uptake (false-negative) on 68Ga-DOTATOC PET/CT scan. In one patient, 68Ga-DOTATOC PET/CT scan helped in demonstrating additional lesions in mediastinal lymph nodes which was confirmed on final histopathological examination, whereas 18F-FDG PET/CT scan was negative in that patient. The SUVmax of TC on 68Ga-DOTATOC PET/CT scan ranged from 3.58 to 55 (mean SUVmax 21.50), while that of AC ranged from 1.1 to 32.5 (mean SUVmax 15.43). The TC showed higher uptake values on 68Ga-DOTATOC PET/CT scan which may be because of their higher degree of differentiation and SSR expression than the AC.
The high sensitivity observed in our study with 68Ga-DOTATOC PET/CT scan was similar to the observations in other studies. Koukouraki et al. reported an overall sensitivity of 90.47 % in evaluation of carcinoid tumours (n = 15) by 68Ga-DOTATOC PET [19]. Gabriel et al. evaluated 84 cases of NET (5 bronchial carcinoids) using 68Ga-DOTATOC PET scan and reported a higher sensitivity for tumour detection by 68Ga-DOTATOC PET as compared to single photon emission computed tomography (SPECT) or CT. The overall sensitivity of 68Ga-DOTATOC PET scan was 97 %, specificity 92 % and overall accuracy 96 % [20]. Ambrosini et al. evaluated 11 patients with pulmonary carcinoids and found 100 % sensitivity, with no false-positive findings on 68Ga-DOTANOC PET scan. It also detected a higher number of lesions as compared to CT scan (37 vs 21) [10]. Our results are in concordance with these reports in the literature.
In our study, 18F-FDG PET/CT had an overall sensitivity of 78.26 % for detection of pulmonary carcinoids, but the specificity was as low as 11.1 % as many non-carcinoid tumours also revealed uptake on 18F-FDG PET/CT scan. The positive predictive value was 69.23 %, while the negative predictive value was 16.6 %. The accuracy of 18F-FDG PET/CT scan for the diagnosis of pulmonary carcinoids was 59.37 %. In our study, 18F-FDG PET/CT was true-positive in 18/26 carcinoids. It was true-positive in all cases of AC and false-negative in eight cases of TC (sensitivity for TC 61.9 % and for AC 100 %). This is in consensus with the study by Daniels et al. who demonstrated a trend toward higher FDG PET sensitivity for AC tumours (80 %) compared to TC tumours (72.7 %) [24]. Erasmus et al. reported that only one of seven carcinoids evaluated by 18F-FDG PET scan was positive [25], but Marom et al. reported a higher sensitivity for carcinoids: five of six patients with pulmonary carcinoids were visually positive on 18F-FDG PET scan [26].
It was seen in our study that the mean SUVmax for AC was considerably higher than that for TC (4.37 vs 2.88). This is in consensus with a few studies that have shown AC to have higher SUVmax than TC on 18F-FDG PET scan. Wartski et al. reported AC showing increased uptake on FDG PET/CT (SUVmax 10.6) in comparison to TC (SUVmax 4.87) [27]. Chong et al. also showed that AC had a higher uptake in comparison with TC (SUVmax range 3.3–7.1 vs 3.2–3.4) [28].
In comparing the two functional imaging modalities, we found that 68Ga-DOTATOC PET/CT scan had a higher utility in the evaluation of suspected bronchial carcinoids (sensitivity 96.15 % and specificity 100 %) in comparison with 18F-FDG PET/CT (sensitivity 78.26 % and specificity 11.1 %). Also seen was that the two types of carcinoid (typical and atypical) showed differential uptakes in the two functional scans and thus a combination of the two functional scans may help in predicting the tumour histology prior to surgery.
Although only a few studies were available with respect to 68Ga-DOTATOC PET/CT in pulmonary NETs, our finding was similar to that reported in other studies when considering NETs in general. Koukouraki et al. comparing 68Ga-DOTATOC PET scan and 18F-FDG PET in evaluation of 15 carcinoids found 68Ga-DOTATOC PET scan to have higher sensitivity (90.47 %) than 18F-FDG PET (sensitivity 68.2 %) [19]. Kayani et al. compared the utility of 68Ga-DOTATATE PET scan and 18F-FDG PET in evaluating 38 cases of NET and found the former to have a higher sensitivity (82 vs 66 %) [21]. Ambrosini et al. and Haug et al. in their studies evaluating the utility of 68Ga-somatostatin analogue PET scan and 3,4-dihydroxy-6-[18F]fluorophenylalanine (18F-FDOPA) PET scan found that 68Ga-somatostatin analogue PET scan was more sensitive than 18F-DOPA PET in detecting NET (sensitivity 96 vs 56 %) [10, 29]. Jindal et al. comparing 68Ga-DOTATOC PET scan and 18F-FDG PET scan in the evaluation of bronchial carcinoids found that TC showed higher uptake on 68Ga-DOTATOC PET scan than AC, while the latter showed an increased uptake on 18F-FDG PET/CT. The ratio of SUVmax of 68Ga-DOTATOC PET scan to that of 18F-FDG PET was significantly higher in TC than in AC (p < 0.001) [30]. One of the limitations in our study is that we had a low number of AC, due to which the overall accuracy of 18F-FDG PET/CT in the patient population of this study is low. Further studies evaluating the accuracy of both methods in a higher number of patients with AC are warranted. Also, another limitation concerns the accuracy of preoperative pathological assessment in three patients, which was not optimal because no post-operative sample was available to compare with the preoperative biopsy.
We had two cases of MEC in our study (both female patients) with a mean age of 19.50 years. In both cases of MEC, preoperative bronchoscopic biopsy was possible and was confirmatory for MEC. In the functional imaging with 18F-FDG PET/CT, one case was positive, while another showed no uptake (SUVmax 4.5 and 1.2 respectively) (Fig. 3). The reported experience of functional imaging in MECs is limited [31, 32]. Both patients with MECs were negative on 68Ga-DOTATOC PET/CT scan (SUVmax range 1.17–1.40).

Transaxial PET (a), CT (b) and PET/CT (c) images in a patient with MEC of left main bronchus showing no uptake on 68Ga-DOTATOC PET/CT scan (SUVmax 1.17). PET (d), CT (e) and PET/CT (f) images of the same patient showing no uptake on 18F-FDG PET/CT scan (SUVmax 1.22)
Two of the patients included in our study had a long duration of symptoms (cough, haemoptysis with dyspnoea) raising the suspicion of bronchial carcinoids and were found to have tracheal tumours. One of the patients had schwannoma and the other had adenoid cystic carcinoma of the trachea. Nakamura et al. reported a case of bronchial schwannoma with high uptake on 18F-FDG PET scan [33]. The schwannoma included in our study group also showed increased uptake on 18F-FDG PET/CT (SUVmax 2.1). Schwannomas do not have somatostatin receptors and are negative on 68Ga-DOTATOC PET/CT scan. In our study the schwannoma also had no uptake on 68Ga-DOTATOC PET/CT scan (SUVmax 0.80). Adenoid cystic carcinoma of the tracheobronchial tree is known to show variable uptake on 18F-FDG PET scan depending on the degree of differentiation [34]. In our study the tumour was positive on 18F-FDG PET/CT scan (SUVmax 2.80). 68Ga-DOTATOC PET/CT scan was negative (SUVmax 0.70) in this patient, as these tumours lack somatostatin receptors (Fig. 4).

Transaxial PET (a), CT (b) and PET/CT (c) images in a patient with adenoid cystic carcinoma of the trachea showing no uptake on 68Ga-DOTATOC PET/CT scan (SUVmax 0.70). PET (d), CT (e) and PET/CT (f) images of the same patient showing uptake on 18F-FDG PET/CT scan (SUVmax 2.8)
Two cases in our study suspected of being bronchial carcinoids turned out to be squamous cell carcinomas. Squamous cell carcinomas of the tracheobronchial tree are known to show intense uptake on 18F-FDG PET scan due to their increased metabolic activity [34]. A similar pattern of uptake was observed in our study with squamous cell carcinomas on 18F-FDG PET scan, with both showing positive uptake (SUVmax 2.6–9). One patient was found to have a metastatic lesion in the ribs. Both cases were negative on 68Ga-DOTATOC PET/CT scan.
Conclusion
68Ga-DOTATOC PET/CT scan is an effective investigation for the initial evaluation of pulmonary carcinoids. 68Ga-DOTATOC PET/CT but not 18F-FDG PET/CT helps to predict histology in suspected bronchopulmonary carcinoids. A negative 68Ga-DOTATOC PET/CT scan potentially rules out the presence of typical pulmonary carcinoid tumour. 18F-FDG PET/CT scan suffers from low sensitivity and specificity in differentiating the pulmonary carcinoids from other tumours. Further evaluation and validation of the above findings with a larger number of patients are required to substantiate our results. In future, prospective studies comparing 68Ga-DOTATOC PET/CT with 18F-FDOPA PET/CT performance in pulmonary carcinoids would be of interest.
References
Klöppel G. Tumour biology and histopathology of neuroendocrine tumours. Best Pract Res Clin Endocrinol Metab 2007;21:15–31.
Beasley MB, Brambilla E, Travis WD. The 2004 World Health Organization classification of lung tumors. Semin Roentgenol 2005;40:90–7.
Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer 2003;97:934–59.
Hauso O, Gustafsson BI, Kidd M, Waldum HL, Drozdov I, Chan AK, et al. Neuroendocrine tumor epidemiology: contrasting Norway and North America. Cancer 2008;113:2655–64.
Cooper WA, Thourani VH, Gal AA, Lee RB, Mansour KA, Miller JI. The surgical spectrum of pulmonary neuroendocrine neoplasms. Chest 2001;119:14–8.
Fink G, Krelbaum T, Yellin A, Bendayan D, Saute M, Glazer M, et al. Pulmonary carcinoid: presentation, diagnosis, and outcome in 142 cases in Israel and review of 640 cases from the literature. Chest 2001;119:1647–51.
Filosso PL, Rena O, Donati G, Casadio C, Ruffini E, Papalia E, et al. Bronchial carcinoid tumors: surgical management and long-term outcome. J Thorac Cardiovasc Surg 2002;123:303–9.
Jeung MY, Gasser B, Gangi A, Charneau D, Ducroq X, Kessler R, et al. Bronchial carcinoid tumors of the thorax: spectrum of radiologic findings. Radiographics 2002;22:351–65.
Ambrosini V, Tomassetti P, Castellucci P, Campana D, Montini G, Rubello D, et al. Comparison between 68Ga-DOTA-NOC and 18F-DOPA PET for the detection of gastro-entero-pancreatic and lung neuro-endocrine tumours. Eur J Nucl Med Mol Imaging 2008;35:1431–8.
Ambrosini V, Castellucci P, Rubello D, Nanni C, Musto A, Allegri V, et al. 68Ga-DOTA-NOC: a new PET tracer for evaluating patients with bronchial carcinoid. Nucl Med Commun 2009;30:281–6.
Kumar R, Sharma P, Garg P, Karunanithi S, Naswa N, Sharma R, et al. Role of (68)Ga-DOTATOC PET-CT in the diagnosis and staging of pancreatic neuroendocrine tumors. Eur Radiol 2011;21:2408–16.
El Jamal M, Nicholson AG, Goldstraw P. The feasibility of conservative resection for carcinoid tumours: is pneumonectomy ever necessary for uncomplicated cases? Eur J Cardiothorac Surg 2000;18:301–6.
McCaughan BC, Martini N, Bains MS. Bronchial carcinoids. Review of 124 cases. J Thorac Cardiovasc Surg 1985;89:8–17.
Beasley MB, Thunnissen FB, Brambilla E, Hasleton P, Steele R, Hammar SP, et al. Pulmonary atypical carcinoid: predictors of survival in 106 cases. Hum Pathol 2000;31:1255–65.
Rosado de Christenson ML, Abbott GF, Kirejczyk WM, Galvin JR, Travis WD. Thoracic carcinoids: radiologic-pathologic correlation. Radiographics 1999;19:707–36.
Pelosi G, Rodriguez J, Viale G, Rosai J. Typical and atypical pulmonary carcinoid tumor overdiagnosed as small-cell carcinoma on biopsy specimens: a major pitfall in the management of lung cancer patients. Am J Surg Pathol 2005;29:179–87.
Hofmann M, Maecke H, Börner R, Weckesser E, Schöffski P, Oei L, et al. Biokinetics and imaging with the somatostatin receptor PET radioligand (68)Ga-DOTATOC: preliminary data. Eur J Nucl Med 2001;28:1751–7.
Kowalski J, Henze M, Schuhmacher J, Mäcke HR, Hofmann M, Haberkorn U. Evaluation of positron emission tomography imaging using [68Ga]-DOTA-D Phe(1)-Tyr(3)-Octreotide in comparison to [111In]-DTPAOC SPECT. First results in patients with neuroendocrine tumors. Mol Imaging Biol 2003;5:42–8.
Koukouraki S, Strauss LG, Georgoulias V, Eisenhut M, Haberkorn U, Dimitrakopoulou-Strauss A. Comparison of the pharmacokinetics of 68Ga-DOTATOC and [18F]FDG in patients with metastatic neuroendocrine tumours scheduled for 90Y-DOTATOC therapy. Eur J Nucl Med Mol Imaging 2006;33:1115–22.
Gabriel M, Decristoforo C, Kendler D, Dobrozemsky G, Heute D, Uprimny C, et al. 68Ga-DOTA-Tyr3-octreotide PET in neuroendocrine tumors: comparison with somatostatin receptor scintigraphy and CT. J Nucl Med 2007;48:508–18.
Kayani I, Bomanji JB, Groves A, Conway G, Gacinovic S, Win T, et al. Functional imaging of neuroendocrine tumors with combined PET/CT using 68Ga-DOTATATE (DOTA-DPhe1, Tyr3-octreotate) and 18F-FDG. Cancer 2008;112:2447–55.
Miederer M, Seidl S, Buck A, Scheidhauer K, Wester HJ, Schwaiger M, et al. Correlation of immunohistopathological expression of somatostatin receptor 2 with standardised uptake values in 68Ga-DOTATOC PET/CT. Eur J Nucl Med Mol Imaging 2009;36:48–52.
Treglia G, Castaldi P, Rindi G, Giordano A, Rufini V. Diagnostic performance of gallium-68 somatostatin receptor PET and PET/CT in patients with thoracic and gastroenteropancreatic neuroendocrine tumours: a meta-analysis. Endocrine 2012;42:80–7.
Daniels CE, Lowe VJ, Aubry M-C, Allen MS, Jett JR. The utility of fluorodeoxyglucose positron emission tomography in the evaluation of carcinoid tumors presenting as pulmonary nodules. Chest 2007;131:255–60.
Erasmus JJ, McAdams HP, Patz Jr EF, Coleman RE, Ahuja V, Goodman PC. Evaluation of primary pulmonary carcinoid tumors using FDG PET. AJR Am J Roentgenol 1998;170:1369–73.
Marom EM, Sarvis S, Herndon 2nd JE, Patz Jr EF. T1 lung cancers: sensitivity of diagnosis with fluorodeoxyglucose PET. Radiology 2002;223:453–9.
Wartski M, Alberini JL, Leroy-Ladurie F, De Montpreville V, Nguyen C, Corone C, et al. Typical and atypical bronchopulmonary carcinoid tumors on FDG PET/CT imaging. Clin Nucl Med 2004;29:752–3.
Chong S, Lee KS, Kim BT, Choi JY, Yi CA, Chung MJ, et al. Integrated PET/CT of pulmonary neuroendocrine tumors: diagnostic and prognostic implications. AJR Am J Roentgenol 2007;188:1223–31.
Haug A, Auernhammer CJ, Wängler B, Tiling R, Schmidt G, Göke B, et al. Intraindividual comparison of 68Ga-DOTA-TATE and 18F-DOPA PET in patients with well-differentiated metastatic neuroendocrine tumours. Eur J Nucl Med Mol Imaging 2009;36:765–70.
Jindal T, Kumar A, Venkitaraman B, Meena M, Kumar R, Malhotra A, et al. Evaluation of the role of [18F]FDG-PET/CT and [68Ga]DOTATOC-PET/CT in differentiating typical and atypical pulmonary carcinoids. Cancer Imaging 2011;11:70–5.
Lee EY, Vargas SO, Sawicki GS, Boyer D, Grant FD, Voss SD. Mucoepidermoid carcinoma of bronchus in a pediatric patient: (18)F-FDG PET findings. Pediatr Radiol 2007;37:1278–82.
Ishizumi T, Tateishi U, Watanabe S-I, Maeda T, Arai Y. F-18 FDG PET/CT imaging of low-grade mucoepidermoid carcinoma of the bronchus. Ann Nucl Med 2007;21:299–302.
Nakamura R, Ishikawa S, Sakai M, Goto Y, Minami Y. Increased fluorodeoxyglucose-uptake in positron emission tomography with an endobronchial schwannoma occluding the left main stem bronchus. J Thorac Oncol 2009;4:1183–4.
Park CM, Goo JM, Lee HJ, Kim MA, Lee CH, Kang MJ. Tumors in the tracheobronchial tree: CT and FDG PET features. Radiographics 2009;29:55–71.
Funding
No financial assistance/grant was received for this study.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Venkitaraman, B., Karunanithi, S., Kumar, A. et al. Role of 68Ga-DOTATOC PET/CT in initial evaluation of patients with suspected bronchopulmonary carcinoid. Eur J Nucl Med Mol Imaging 41, 856–864 (2014). https://doi.org/10.1007/s00259-013-2659-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00259-013-2659-5