
Abstract
This brief review discusses copper transport in humans, with an emphasis on knowledge learned from one of the simplest model organisms, yeast. There is a further focus on copper transport in Alzheimer’s Disease (AD). Copper homeostasis is essential for the well-being of all organisms, from bacteria to yeast to humans: survival depends on maintaining the required supply of copper for the many enzymes, dependent on copper for activity, while ensuring that there is no excess free copper, which would cause toxicity. A virtual orchestra of proteins are required to achieve copper homeostasis. For copper uptake, Cu(II) is first reduced to Cu(I) via a membrane-bound reductase. The reduced copper can then be internalised by a copper transporter where it is transferred to copper chaperones for transport and specific delivery to various organelles. Of significance are internal copper transporters, ATP7A and ATP7B, notable for their role in disorders of copper deficiency and toxicity, Menkes and Wilson’s disease, respectively. Metallothioneins and Cu/Zn superoxide dismutase can protect against excess copper in cells. It is clear too, increasing age, environmental and lifestyle factors impact on brain copper. Studies on AD suggest an important role for copper in the brain, with some AD therapies focusing on mobilising copper in AD brains. The transport of copper into the brain is complex and involves numerous players, including amyloid precursor protein, Aβ peptide and cholesterol.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Survival of an organism depends on maintaining the proper balance of copper within all cells. Excess free copper is toxic but a deficiency of copper will also incapacitate proper functions, since copper is essential for numerous copper enzymes including cytochrome oxidase (EC 1.9.3.1), superoxide dismutase (EC 1.13.11.11), tryptophan-2,3-dioxygenase (EC 1.13.11.11), lysine oxidase (EC 1.4.3.12), monoamine oxidase (EC 1.4.3.4), tyrosinase (EC 1.14.18.1) and dopamine-β-hydroxylase (EC 1.14.17.1). In humans, these metalloenzymes are required in various organs or sites, and indeed some are essential in all cells. Thus, it can be seen that there is a need for correct transport of copper to organs distant from the site of copper absorption, as well as to cells and cellular components within those organs.
The purpose of this review is to discuss the mechanisms of copper transport and homeostasis throughout the body, and in addition, to discuss strategies to alter copper transport and homeostasis in the brain, which may affect outcomes of neurological disease. There is an orchestra of proteins involved in copper metabolism in humans and these proteins almost always have a counterpart in yeast, as shown in Table 1. Therefore, the study of copper metabolism in yeast, specifically Saccharomyces cerevisiae, has had a major impact on the knowledge we now possess. Throughout this review frequent reference will be made to these yeast studies (Fig. 1).

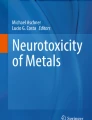
Simplified schematic diagram of copper homeostasis in eukaryotic organisms. Light shaded boxes represent the classes of proteins described in Table 1. Cu(II) is first reduced by a copper reductase. Cu(I) can then be transported into the cell by a membrane-spanning copper transporter. Cu(I) is then carried by various chaperones to specific locations, including to Sod1, the mitochondrion and the trans-Golgi network. Another copper transporter is employed to deliver intracellular copper to late endosomes (E) and lysosomes (L) in mammals, or vacuoles (V) in yeast. Excess copper can be removed by efflux pumps, or can be sequestered into metallothionein. The synthesis of copper apothionein is controlled by a copper-sensing transcription factor that is itself a copper apothionein. Arrows indicate the passage of copper from one protein to the next
Distribution of copper from the diet to serum
It is estimated that a 70 kg adult contains 110 mg of copper, most of which is in the skeleton (46 mg) and skeletal muscle (26 mg). The liver (10 mg), brain (7 mg) and blood (6 mg) contain most of the remaining copper. There is a continual turnover of copper, with most of it being recycled. Each day more than 4 mg is excreted into the bile but most is reabsorbed in the intestines. Daily diets have around 0.6–1.6 mg of copper, about half of which is absorbed. The end result is for the organism to maintain copper homeostasis, with no net change in copper levels.
The uptake of copper from the diet has been reviewed by (Linder and Hazegh-Azam 1996). Absorption of copper occurs primarily (or solely) via the brush border cells of the small intestine into interstitial fluid and blood where copper then binds albumin (Linder and Hazegh-Azam 1996). Monitoring the distribution of injected radiolabelled copper sulfate from serum (Weiss and Linder 1985), showed that labelled copper disappeared from plasma within 2 h, with 40% of it being localised in the liver after 6 h. After that time there was significant redistribution to the plasma and to other organs, with levels in plasma, heart brain, muscle and kidney peaking after one to 3 days. Although albumin can accommodate ∼40 mg copper per litre of blood, it normally carries <1% of this amount. The major copper binding in blood is ceruloplasmin, which is synthesised in the liver where it binds copper. Ceruloplasmin binds most of the serum copper but is not necessary for copper transport; it is used in the iron transport system. Ceruloplasmin functions as a multicopper oxidase, oxidizing Fe2+ to Fe3+. The Fe3+ is then bound by transferrin for transport. The equivalent protein in yeast is Fet3, a protein that also functions as a multicopper oxidase (Table 1) (Askwith et al. 1994; de Silva et al. 1997; De Silva et al. 1995; Yuan et al. 1995). People with a total deficiency of ceruloplasmin have an iron metabolism disorder and mid-life dementia (Harris et al. 1995).
Cellular uptake of copper
Copper transport is dependent on the oxidation state of the copper. Only reduced copper can be transported, yet oxidative environments result in copper frequently occurring as the oxidised copper, Cu(II). Reduction occurs through copper reductases. In yeast the copper transporters, Ctr1 and Ctr2, utilise the same metalloreductase, Fre1 (Rees and Thiele 2007) which is also a ferric reductase. Another ferric reductase, Fre2, appears to have an equivalent role to Fre1. The human counterparts of Fre1, the Steap proteins, function as both cupric and ferric reductases (Ohgami et al. 2006).
In yeast the transport of reduced copper at the plasma membrane takes place through a high affinity copper transporter Ctr1 (Dancis et al. 1994a, b). Ctr3 also shares this function but is inactivated by a Ty2 element insertion in some lab strains (Knight et al. 1996). The human equivalent of Ctr1, hCtr1, was identified by complementation in yeast (Zhou and Gitschier 1997). The yeast ctr1 mutant exhibited defects in respiratory growth, iron transport and Sod1p, all of which were rescued by the hCtr1, while overproduction of hCtr1 led to copper overload (Zhou and Gitschier 1997). An additional gene, hCtr2, found by a similarity search (Zhou and Gitschier 1997), was recently shown to be expressed in late endosomes and lysosomes where it facilitated cellular copper uptake (van den Berghe et al. 2007). In yeast an equivalent copper transporter, Ctr2, is found exclusively on the vacuolar membrane where it controls vacuolar copper levels (Kampfenkel et al. 1995; Rees et al. 2004). Ctr2 appears to be a non-essential vacuolar copper transporter (Portnoy et al. 2001).
Copper chaperones
Yeast studies provided the first functional identification of the copper chaperones, or metallochaperones. These are intracellular proteins that receive copper and deliver it to specific locations. Because of the various pathways to the ultimate destinations, there are a series of pathway-specific chaperones. The chaperone Ccs1 delivers copper to Cu/Zn superoxide dismutase (Sod1) in the cytosol (Culotta et al. 1997). Cox17 delivers copper to the mitochondrion for incorporation into subunits of cytochrome oxidase (Amaravadi et al. 1997; Glerum et al. 1996), via both Sco1, and Cox11 (Horng et al. 2004). Atx1 is involved in delivery of copper to the secretory pathway for copper enzymes at the cell surface or for release (Klomp et al. 1997; Lin et al. 1997; Pufahl et al. 1997). In the Golgi, this copper is utilised by the copper–transporting ATPases, ATP7A and ATP7B, that are described below.
Internal copper transporters
The two major inherited disorders of copper metabolism, Menkes disease and Wilson’s disease, provide insights on cellular copper efflux. Menkes disease has been shown to result from mutations in the MNK transporter, ATP7A, a P-type ATPase. ATP7A is produced in mucosal cells of the intestine and used for systemic absorption of copper. At normal or low copper ATP7A delivers intracellular copper to enzymes in the trans-Golgi network (Yamaguchi-Iwai et al. 1996). At high copper levels ATP7A moves to the plasma membrane and performs copper efflux (Petris et al. 1996). Menkes disease is effectively a copper deficiency disease that causes growth failure, skeletal defects, degeneration of the central nervous system, and early death (Danks 1995).
Wilson’s disease is a result of defects in the WND transporter, ATP7B, which has 54% sequence identity with ATP7A. At normal or low copper ATP7B is found only in the liver where it delivers intracellular copper to apoceruloplasmin in the trans-Golgi network (Yamaguchi et al. 1996). At high copper levels ATP7B moves copper to vesicles for delivery to the biliary caniliculus, performing copper efflux into the bile for excretion (Petris et al. 1996). ATP7B mutations result in copper accumulation in the liver and brain leading to liver disease and neurological problems including behavioural disturbances and movement disorders. Menkes and Wilson’s disease are similar in that they utilise a similar pump, but they use it in different tissues. Yeast cells have an equivalent pump, Ccc2, which facilitates cation transport, including copper, in trans Golgi vesicles (Yuan et al. 1995).
Copper sequestration
Excess and free copper are toxic to cells so it is essential that mechanisms exist to sequester free intracellular copper. In healthy yeast cells free copper levels are incredibly low (less than one free ion per cell) (Rae et al. 1999). Metallothionein is a cellular copper binding protein that provides significant protection against elevated copper levels. Yeast metallothionein (Karin et al. 1984; Winge et al. 1985) is highly regulated by Ace1, a constitutively produced transcriptional activator of the yeast metallothionein gene (Buchman et al. 1989; Szczypka and Thiele 1989). In the presence of copper Ace1 binds copper, and activates transcription. In the absence of metallothionein, superoxide dismutase can play a major protective role against copper toxicity. It is significant that some cases of amyotrophic lateral sclerosis (ALS) have defects in Cu/Zn superoxide dismutase, suggesting some linkage between this form of motor neurone disease and copper metabolism.
Alzheimer’s disease and copper transport
Links have been established between copper metabolism and late onset neurological diseases, however, much work still needs to be done to fully understand the relationships. In Parkinson’s Disease, α-synuclein oligomerisation is affected by copper (Paik et al. 1999) and dopamine may be affected by copper to become toxic (Paris et al. 2001; Snyder and Friedman 1998; Spencer et al. 1994). Human prions have also been found to have copper binding sites (Brown et al. 1997; Hornshaw et al. 1995). The remainder of this review will focus on Alzheimer’s Disease (AD) where the amyloid precursor protein (APP) and the Aβ peptide derived from APP are strongly implicated in copper metabolism.
Amyloid precursor protein is the most important protein in AD and may be a copper transporter that is unique to mammals. It has two copper binding sites, including one in the Aβ peptide sequence (Atwood et al. 1998; Hesse et al. 1994). Overexpression of APP in transgenic mice appears to reduce levels of copper in brains (Bayer et al. 2003; Maynard et al. 2002; Phinney et al. 2003) leading to suggestions that APP may be a copper transporter (White et al. 1998). Even though APP has no yeast equivalent, it can cause copper efflux in yeast (Treiber et al. 2004) as it does in brains. Proteins of similar structure, Aplp1 and Aplp2, have copper binding domains and may similarly function in copper efflux (Hesse et al. 1994; White et al. 1998, 1999a, b). APP is unique among this family because it is processed by the proteases BACE (Vassar et al. 1999) and γ secretase, to produce the Aβ peptide, or β amyloid, a causative agent in AD. Aβ exhibits neurotoxicity, and is a major component of the extracellular Aβ plaques associated with AD. These plaques are a reservoir for a number of metals, including copper, and it is has been considered that the copper in these plaques may be available for the production of reactive oxygen species which could cause neuronal loss and brain damage (Bush 2000). However, in view of the overall decline in copper levels as brains age, the alternate possibility, that build up of Aβ causes a copper shortfall, should also be considered.
Can neuronal copper levels be manipulated? If so this could be an avenue to the treatment of neurological diseases (although the latter will not be discussed here at any length). One of the most promising drugs that have been trialled is clioquinol, a metal protein attenuating compound. Clioquinol reduces plaque in mouse AD models and it would appear to alter copper levels (Cherny et al. 2001). In a treatment of APP 750SL transgenic mice, clioquinol was shown to improve survival (Schafer et al. 2007). While clioquinol reduced serum copper levels from around 800 μg/l to around 500 μg/l, even with added copper in the diet, brain copper significantly increased, from 3.9 to 4.2 μg/g with added dietary copper. The treated mice also exhibited normal survival and improved memory, suggesting that clioquinol enabled brain copper levels to increase, and this in turn gave the positive benefit. Interestingly clioquinol has also been shown to cause increased copper levels in yeast producing APP (Treiber et al. 2004).
A combination of copper with high dietary cholesterol has been linked to increased deposits of Alzheimer’s Aβ brain plaque in rabbits (Sparks and Schreurs 2003). Plaques were induced at levels of 0.12 ppm copper, much lower than the levels of 1.3 ppm permitted by water supply agencies. Conversely could lower cholesterol levels lead to lower copper levels, reducing Aβ plaques? Studies of cholesterol-lowering drugs, known as statins, may provide answers to this question.
Statins inhibit HMG-CoA reductase, leading to reduced cholesterol levels as well as lower levels of several other products dependent on HMG-CoA reductase (Fig. 2). Many consider these blockbuster drugs to be the best drugs to lower the incidence of AD. However, there has been a lack of concordance in some studies leading to significant confusion. A recent study by (Wolozin et al. 2007) has now shown that simvastatin is unique with respect to reducing AD. Unlike many other statins, simvastatin is lipophilic and crosses the blood brain barrier (BBB), so it may be expected that simvastatin would reduce cholesterol synthesis in the brain.

Biochemical pathway affected by statins
A major question now is how does simvastatin reduce the incidence of AD? As predicted from the cholesterol-fed rabbit model for AD, simvastatin may decrease Aβ deposition in the brain by reducing brain cholesterol levels. A second possibility, is that statins reduce protein prenylation decreasing BACE activity, thereby leading to lower levels of Aβ (see Fig. 2); cell culture studies support this possibility (Cole et al. 2005). A third possibility is that statins can reduce mitochondrial respiratory function through decreased haem synthesis, coenzyme Q10 production (see Fig. 2) (Macreadie et al. 2006; Satoh et al. 1994; Westermeyer and Macreadie 2007) or reduced mtDNA levels (Westermeyer and Macreadie 2007). This could in turn lead to lower levels of reactive oxygen species, possibly reducing the threshold for Aβ-induced damage (Tabner et al. 2001). The idea that statins reduce AD through anti-inflammatory properties could be dismissed with the knowledge that simvastatin but not atorvastatin reduces the incidence of AD. Understanding exactly how simvastatin affects the brain will now be an even higher priority area of research.
Finally, vaccine approaches may have some merit in animal models of AD by clearing Aβ plaque. Whether this affects brain copper has not been considered but presumably metals associated with the plaque would be removed along with plaque.
It is clear that much is now known about copper homeostasis, but there is still some way to go before we conquer neurological diseases that involve copper. It is likely that an increased understanding of copper homeostasis may help in unravelling the many important neurological diseases involving copper metabolism.
References
Amaravadi R, Glerum DM, Tzagoloff A (1997) Isolation of a cDNA encoding the human homolog of COX17, a yeast gene essential for mitochondrial copper recruitment. Hum Genet 99:329–333
Askwith C, Eide D, Van Ho A, Bernard PS, Li L, Davis-Kaplan S, Sipe DM, Kaplan J (1994) The FET3 gene of S. cerevisiae encodes a multicopper oxidase required for ferrous iron uptake. Cell 76:403–410
Atwood CS, Moir RD, Huang X, Scarpa RC, Bacarra NM, Romano DM, Hartshorn MA, Tanzi RE, Bush AI (1998) Dramatic aggregation of Alzheimer Aβ by Cu(II) is induced by conditions representing physiological acidosis. J Biol Chem 273:12817–12826
Bayer TA, Schafer S, Simons A, Kemmling A, Kamer T, Tepest R, Eckert A, Schussel K, Eikenberg O, Sturchler-Pierrat C, Abramowski D, Staufenbiel M, Multhaup G (2003) Dietary Cu stabilizes brain superoxide dismutase 1 activity and reduces amyloid Aβ production in APP23 transgenic mice. Proc Natl Acad Sci USA 100:14187–14192
Brown DR, Qin K, Herms JW, Madlung A, Manson J, Strome R, Fraser PE, Kruck T, von Bohlen A, Schulz-Schaeffer W, Giese A, Westaway D, Kretzschmar H (1997) The cellular prion protein binds copper in vivo. Nature 390:684–687
Buchman C, Skroch P, Welch J, Fogel S, Karin M (1989) The CUP2 gene product, regulator of yeast metallothionein expression, is a copper-activated DNA-binding protein. Mol Cell Biol 9:4091–4095
Bush AI (2000) Metals and neuroscience. Curr Opin Chem Biol 4:184–191
Cherny RA, Atwood CS, Xilinas ME, Gray DN, Jones WD, McLean CA, Barnham KJ, Volitakis I, Fraser FW, Kim Y, Huang X, Goldstein LE, Moir RD, Lim JT, Beyreuther K, Zheng H, Tanzi RE, Masters CL, Bush AI (2001) Treatment with a copper-zinc chelator markedly and rapidly inhibits β-amyloid accumulation in Alzheimer’s disease transgenic mice. Neuron 30:665–676
Cole SL, Grudzien A, Manhart IO, Kelly BL, Oakley H, Vassar R (2005) Statins cause intracellular accumulation of amyloid precursor protein, β-secretase-cleaved fragments, and amyloid β-peptide via an isoprenoid-dependent mechanism. J Biol Chem 280:18755–18770
Culotta VC, Klomp LW, Strain J, Casareno RL, Krems B, Gitlin JD (1997) The copper chaperone for superoxide dismutase. J Biol Chem 272:23469–23472
Danks DM (1995) Disorders of copper transport. In: Scriver CR, Beaudet AL, Sly WM, Valle D (eds) The metabolic and molecular basis of inherited disease. McGraw-Hill, New York, pp 2211–2235
Dancis A, Haile D, Yuan DS, Klausner RD (1994a) The Saccharomyces cerevisiae copper transport protein (Ctr1p). Biochemical characterization, regulation by copper, and physiologic role in copper uptake. J Biol Chem 269:25660–25667
Dancis A, Yuan DS, Haile D, Askwith C, Eide D, Moehle C, Kaplan J, Klausner RD (1994b) Molecular characterization of a copper transport protein in S. cerevisiae: an unexpected role for copper in iron transport. Cell 76:393–402
de Silva D, Davis-Kaplan S, Fergestad J, Kaplan J (1997) Purification and characterization of Fet3 protein, a yeast homologue of ceruloplasmin. J Biol Chem 272:14208–14213
De Silva DM, Askwith CC, Eide D, Kaplan J (1995) The FET3 gene product required for high affinity iron transport in yeast is a cell surface ferroxidase. J Biol Chem 270:1098–1101
Glerum DM, Shtanko A, Tzagoloff A (1996) Characterization of COX17, a yeast gene involved in copper metabolism and assembly of cytochrome oxidase. J Biol Chem 271:14504–14509
Harris ZL, Takahashi Y, Miyajima H, Serizawa M, MacGillivray RT, Gitlin JD (1995) Aceruloplasminemia: molecular characterization of this disorder of iron metabolism. Proc Natl Acad Sci USA 92:2539–2543
Hesse L, Beher D, Masters CL, Multhaup G (1994) The β A4 amyloid precursor protein binding to copper. FEBS Lett 349:109–116
Horng YC, Cobine PA, Maxfield AB, Carr HS, Winge DR (2004) Specific copper transfer from the Cox17 metallochaperone to both Sco1 and Cox11 in the assembly of yeast cytochrome C oxidase. J Biol Chem 279:35334–35340
Hornshaw MP, McDermott JR, Candy JM (1995) Copper binding to the N-terminal tandem repeat regions of mammalian and avian prion protein. Biochem Biophys Res Commun 207:621–629
Kampfenkel K, Kushnir S, Babiychuk E, Inze D, Van Montagu M (1995) Molecular characterization of a putative Arabidopsis thaliana copper transporter and its yeast homologue. J Biol Chem 270:28479–28486
Karin M, Najarian R, Haslinger A, Valenzuela P, Welch J, Fogel S (1984) Primary structure and transcription of an amplified genetic locus: the CUP1 locus of yeast. Proc Natl Acad Sci USA 81:337–341
Klomp LW, Lin SJ, Yuan DS, Klausner RD, Culotta VC, Gitlin JD (1997) Identification and functional expression of HAH1, a novel human gene involved in copper homeostasis. J Biol Chem 272:9221–9226
Knight SA, Labbe S, Kwon LF, Kosman DJ, Thiele DJ (1996) A widespread transposable element masks expression of a yeast copper transport gene. Genes Dev 10:1917–1929
Lin SJ, Pufahl RA, Dancis A, O’Halloran TV, Culotta VC (1997) A role for the Saccharomyces cerevisiae ATX1 gene in copper trafficking and iron transport. J Biol Chem 272:9215–9220
Linder MC, Hazegh-Azam M (1996) Copper biochemistry and molecular biology. Am J Clin Nutr 63:797S–811S
Macreadie IG, Johnson G, Schlosser T, Macreadie PI (2006) Growth inhibition of Candida species and Aspergillus fumigatus by statins. FEMS Microbiol Lett 262:9–13
Maynard CJ, Cappai R, Volitakis I, Cherny RA, White AR, Beyreuther K, Masters CL, Bush AI, Li QX (2002) Overexpression of Alzheimer’s disease amyloid- β opposes the age-dependent elevations of brain copper and iron. J Biol Chem 277:44670–44676
Ohgami RS, Campagna DR, McDonald A, Fleming MD (2006) The steap proteins are metalloreductases. Blood 108:1388–1394
Paik SR, Shin HJ, Lee JH, Chang CS, Kim J (1999) Copper(II)-induced self-oligomerization of alpha-synuclein. Biochem J 340:821–828
Paris I, Dagnino-Subiabre A, Marcelain K, Bennett LB, Caviedes P, Caviedes R, Azar CO, Segura-Aguilar J (2001) Copper neurotoxicity is dependent on dopamine-mediated copper uptake and one-electron reduction of aminochrome in a rat substantia nigra neuronal cell line. J Neurochem 77:519–529
Petris MJ, Mercer JF, Culvenor JG, Lockhart P, Gleeson PA, Camakaris J (1996) Ligand-regulated transport of the Menkes copper P-type ATPase efflux pump from the Golgi apparatus to the plasma membrane: a novel mechanism of regulated trafficking. EMBO J 15:6084–6095
Phinney AL, Drisaldi B, Schmidt SD, Lugowski S, Coronado V, Liang Y, Horne P, Yang J, Sekoulidis J, Coomaraswamy J, Chishti MA, Cox DW, Mathews PM, Nixon RA, Carlson GA, St George-Hyslop P, Westaway D (2003) In vivo reduction of amyloid-β by a mutant copper transporter. Proc Natl Acad Sci USA 100:14193–14198
Portnoy ME, Schmidt PJ, Rogers RS, Culotta VC (2001) Metal transporters that contribute copper to metallochaperones in Saccharomyces cerevisiae. Mol Genet Genomics 265:873–882
Pufahl RA, Singer CP, Peariso KL, Lin SJ, Schmidt PJ, Fahrni CJ, Culotta VC, Penner-Hahn JE, O’Halloran TV (1997) Metal ion chaperone function of the soluble Cu(I) receptor Atx1. Science 278:853–856
Rae TD, Schmidt PJ, Pufahl RA, Culotta VC, O’Halloran TV (1999) Undetectable intracellular free copper: the requirement of a copper chaperone for superoxide dismutase. Science 284:805–808
Rees EM, Lee J, Thiele DJ (2004) Mobilization of intracellular copper stores by the ctr2 vacuolar copper transporter. J Biol Chem 279:54221–54229
Rees EM, Thiele DJ (2007) Identification of a Vacuole-associated metalloreductase and its role in Ctr2-mediated intracellular copper mobilization. J Biol Chem 282:21629–21638
Satoh K, Nakai T, Ichihara K (1994) Influence of 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitors on mitochondrial respiration in rat liver during ischemia. Eur J Pharmacol 270:365–369
Schafer S, Pajonk FG, Multhaup G, Bayer TA (2007) Copper and clioquinol treatment in young APP transgenic and wild-type mice: effects on life expectancy, body weight, and metal-ion levels. J Mol Med 85:405–413
Snyder RD, Friedman MB (1998) Enhancement of cytotoxicity and clastogenicity of l-DOPA and dopamine by manganese and copper. Mutat Res 405:1–8
Sparks DL, Schreurs BG (2003) Trace amounts of copper in water induce β-amyloid plaques and learning deficits in a rabbit model of Alzheimer’s disease. Proc Natl Acad Sci USA 100:11065–11069
Spencer JP, Jenner A, Aruoma OI, Evans PJ, Kaur H, Dexter DT, Jenner P, Lees AJ, Marsden DC, Halliwell B (1994) Intense oxidative DNA damage promoted by L-dopa and its metabolites. Implications for neurodegenerative disease. FEBS Lett 353:246–250
Szczypka MS, Thiele DJ (1989) A cysteine-rich nuclear protein activates yeast metallothionein gene transcription. Mol Cell Biol 9:421–429
Tabner BJ, Turnbull S, El-Agnaf O, Allsop D (2001) Production of reactive oxygen species from aggregating proteins implicated in Alzheimer’s disease, Parkinson’s disease and other neurodegenerative diseases. Curr Top Med Chem 1:507–517
Treiber C, Simons A, Strauss M, Hafner M, Cappai R, Bayer TA, Multhaup G (2004) Clioquinol mediates copper uptake and counteracts copper efflux activities of the amyloid precursor protein of Alzheimer’s disease. J Biol Chem 279:51958–51964
van den Berghe PV, Folmer DE, Malingre HE, van Beurden E, Klomp AE, van de Sluis B, Merkx M, Berger R, Klomp LW (2007) Human copper transporter 2 is localized in late endosomes and lysosomes and facilitates cellular copper uptake. Biochem J 407:49–59
Vassar R, Bennett BD, Babu-Khan S, Kahn S, Mendiaz EA, Denis P, Teplow DB, Ross S, Amarante P, Loeloff R, Luo Y, Fisher S, Fuller J, Edenson S, Lile J, Jarosinski MA, Biere AL, Curran E, Burgess T, Louis JC, Collins F, Treanor J, Rogers G, Citron M (1999) β-secretase cleavage of Alzheimer’s amyloid precursor protein by the transmembrane aspartic protease BACE. Science 286:735–741
Weiss KC, Linder MC (1985) Copper transport in rats involving a new plasma protein. Am J Physiol 249:E77–E88
Westermeyer C, Macreadie IG (2007) Simvastatin reduces ergosterol levels, inhibits growth and causes loss of mtDNA in Candida glabrata. FEMS Yeast Res 7:436–441
White AR, Multhaup G, Maher F, Bellingham S, Camakaris J, Zheng H, Bush AI, Beyreuther K, Masters CL, Cappai R (1999a) The Alzheimer’s disease amyloid precursor protein modulates copper-induced toxicity and oxidative stress in primary neuronal cultures. J Neurosci 19:9170–9179
White AR, Reyes R, Mercer JF, Camakaris J, Zheng H, Bush AI, Multhaup G, Beyreuther K, Masters CL, Cappai R (1999b) Copper levels are increased in the cerebral cortex and liver of APP and APLP2 knockout mice. Brain Res 842:439–444
White AR, Zheng H, Galatis D, Maher F, Hesse L, Multhaup G, Beyreuther K, Masters CL, Cappai R (1998) Survival of cultured neurons from amyloid precursor protein knock-out mice against Alzheimer’s amyloid-β toxicity and oxidative stress. J Neurosci 18:6207–6217
Winge DR, Nielson KB, Gray WR, Hamer DH (1985) Yeast metallothionein. Sequence and metal-binding properties. J Biol Chem 260:14464–14470
Wolozin B, Wang SW, Li N-C, Lee A, Lee TA, Kazis LE (2007) Simvastatin is associated with a reduced incidence of dementia and Parkinson’s disease. BMC Med 5:20. doi:10.1186/1741-7015-5-20
Yamaguchi-Iwai Y, Stearman R, Dancis A, Klausner RD (1996) Iron-regulated DNA binding by the AFT1 protein controls the iron regulon in yeast. EMBO J 15:3377–3384
Yuan DS, Stearman R, Dancis A, Dunn T, Beeler T, Klausner RD (1995) The Menkes/Wilson disease gene homologue in yeast provides copper to a ceruloplasmin-like oxidase required for iron uptake. Proc Natl Acad Sci USA 92:2632–2636
Zhou B, Gitschier J (1997) hCTR1: a human gene for copper uptake identified by complementation in yeast. Proc Natl Acad Sci USA 94:7481–7486
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Macreadie, I.G. Copper transport and Alzheimer’s disease. Eur Biophys J 37, 295–300 (2008). https://doi.org/10.1007/s00249-007-0235-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00249-007-0235-2