
Abstract
This study aimed at evaluating the protective effects of a herbal medication (Tutukon) on the hyperoxaluria induced apoptotic changes and crystal deposition in renal tubular epithelium in rat model. 60 male wistar rats were divided into three different groups (each group n: 20). In Group I severe hyperoxaluria was induced by ethylene glycol (EG) (0.75 %) administration for 28 days. In Group II, in addition to hyperoxaluria induction, animals were treated with Tutukon for 28 days. Group III animals constituted the controls without any specific medication and/or intervention. While the presence and degree of crystal deposition in the tubular lumen were examined histopathologically under light microscopy, tubular apoptotic changes were evaluated using immunohistochemical staining for cysteine-aspartic acid protease-3 (Caspase-3) and tumor necrosis factor alpha (TNF-α) positivity on days 14 and 28, respectively. Evaluation of apoptotic changes by Caspase-3 positivity showed that while the majority of animals undergoing EG only showed evident apoptotic changes (n: 9), Tutukon application demonstrated a significant limitation with limited or no apoptosis (n: 7) in these animals. Similar data were noted for TNF alpha expression; while apoptotic changes were evident in 8 (80 %) in Group I animals, limited changes were noted in Tutukon Group (n: 2). Regarding crystal deposition despite evident changes in Group I (9 animals), like apoptotic alterations, it was again significantly limited in animals receiving Tutukon (4 animals). Renal tubular crystal deposition and apoptotic changes induced by hyperoxaluria play a role in the pathogenesis of urolithiasis and the limitation of these changes might be instituted by Tutukon as a result of its antioxidant and antiinflammatory effects.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Hyperoxaluria is the main risk factor for human idiopathic calcium oxalate (CaOx) stone formation, and the induction of hyperoxaluria is a powerful driving force in stone formation and the development of CaOx urolithiasis [1]. Both clinical and experimental studies suggest that renal tubular epithelium is the major target for oxalate-induced injury and sustained hyperoxaluria, along with crystal–cell interaction may result in injury to the renal tubular cells [2, 3]. Recent studies on LLC-PK1 cells have shown well that a high oxalate concentration together with CaOx crystal formation/deposition may induce renal tubular cell damage and/or dysfunction producing a variety of changes in renal tubular cell morphology and function, including increased cellular proliferation and, at elevated concentrations which may express as cell apoptosis [4–6].
The etiopathogenesis of cell injury during hyperoxaluric diet involves induced lipid peroxidation in tubular cells, which usually leads to the functional impairment of cellular components by reactive oxygen species (ROS) formation due to oxidative stress [4, 7, 8]. Apart from possible hyperoxaluria-induced tubular ischemia, which gives rise to ROS production as a result of lipid peroxidation, studies have clearly demonstrated that oxalate ions themselves may also be responsible tubular alterations as a result of their direct toxic effects [4, 5, 9, 10].
Taking the injurious effects of hyperoxaluria causing crystal deposition in renal parenchyma and apoptotic changes in renal tubular epithelium (as a result of ROS production) into account, it may be useful to apply protective agents in an attempt to prevent or at least limit the extent of the pathologic alterations. While verapamil and nifedipine (calcium channel blocking agents) were found to limit the histologic changes as well as crystal deposition induced by certain renal trauma [8, 11, 12], potassium citrate was found to limit stone recurrence after extracorporeal shockwave lithotripsy [7], and allopurinol as well as vitamin E has been used as antioxidant agents to minimize the effects of free oxygen radical formation in certain tissues [11, 13, 14].
In addition to the use of these medical agents; recent data clearly demonstrated that as a promising and effective alternative, herbal medicine has gained an increasing importance in the prevention and metaphylaxis of renal stones [22, 23] as well as to improve the results of lithotripsy [24]. Related with this subject, Tutukon is a medication composed of different herbal ingredients demonstrating certain biological traits among which the antioxidant potential is one of the most important characteristics of these ingredients.
In this present animal study, taking the effective antioxidant potential into account; we aimed to evaluate the possible protective effect of Tutukon on the presence and degree of apoptotic changes as well as crystal formation in renal tubular epithelial cells induced by hyperoxaluric diet in a rat model.
Materials and methods
A total of 60 male wistar white rats, each weighing 250–300 g/each, were included into the study program. Ethical committee approval was obtained from the animal laboratory of the Pendik animal research laboratory. All animals were fed standard chow and kept under normal room conditions, and following a complete physical examination, biochemical evaluation including blood and urine analyses and stool examination was performed in all of them.
Animals were then divided into three different groups (n = 20). While the animals in Group I were given hyperoxaluria-inducing diet of 0.75 % ethylene glycol (EG) in distilled drinking water from day 0 to day 28, animals in Group II received a protective agent (Tutukon—see drug characteristics below) in addition to the induction of hyperoxaluria via a feeding catheter (5 ml/BW–20 ml/day—three times in a day in divided doses) for 28 days during the study program. Last, Group III included control animals receiving only distilled drinking water during all study phases. During the experimental period, all animals were provided regular rat chow ad libitum. Following a 2-week hyperoxaluric diet in Group I and additional protective agent in Group II and a normal diet in Group III, ten animals in each group were killed on days 14 and 28 after which a bilateral flank incision was performed and the kidneys removed for histopathologic evaluation.
Drug characteristics
Pharmacological group: plant-based fixed-dose combination,
Dosage form: 45 ml three times/daily.
Active plant ingredients: Essential oils, flavonoids-quercetin, polysaccharides, rosmarinic acid, boldin, flavone glycosides.
Pathological processing
The kidneys were fixed with 10 % formalin solution, embedded in paraffin blocks, sliced to 4–6 μm thickness, and stained with hematoxylin–eosin (H&E), Periodic acid–Schiff stain (PAS) (Bio-Optica, Milano), and Masson’s trichrome stain (MTK) (Bio-Optica, Milano). Immunohistochemical studies were performed using the Bond polymer refine detection method (Leica Biosystems Newcastle Ltd., Newcastle) with diaminobenzidine as the chromogen and hematoxylin as the nuclear counterstain. All immunohistochemical processes were performed using the Leica BOND-MAX automated system (Leica Biosystems, Melbourne). Included antibodies were anti-TNF-alpha antibody (Polyclonal, 1:500 dilution; Novus Biologicals, UK), anti-Caspase-3 antibody (clone JHM62, 1:400 dilution; Leica Biosystems Newcastle Ltd., Newcastle). All antibodies were diluted with Lab Vision™ Antibody Diluent (TA-125-AD, Thermo Scientific™, CA).
Caspase and TNF-α positive immunostaining was graded using a three-point scale: none, score 0; faint immunoreactivity or single positive cell, score 1; scattered moderately intense immunoreactivity or numerous positive cells, score 2; and dense intense immunoreactivity or clusters of positive cells, score 3. By utilizing a specific grading system, tubules demonstrating granular crystallization and/or calcification were evaluated and scored under light microscopy with polarized filter in hematoxylin eosin stain with in double-blinded fashion. The extent of the crystallization was graded as follows: none: score 0, Minimal: single crystal formation in one focus: score 1, Moderate: scattered crystal formations in more than one focus: score 2, Severe: dense crystal formations—numerous crystal clusters: score 3.
Statistical analysis
For statistical analysis of the obtained data NCSS (Number Cruncher Statistical System) 2007&PASS (Power Analysis and Sample Size) 2008 Statistical Software (Utah, USA) program was used. While evaluating the obtained data, in addition to definitive statistical methods (Mean, Standard deviation, Median, Frequency, Ratio) Mann–Whitney U test was utilized to evaluate the parameters demonstrating abnormal distribution for comparison of the three groups. However, if the number of groups demonstrating abnormal distribution was more than 3, Kruskal–Wallis test was used and last, Mann–Whitney U test was used to identify the group causing difference among the groups. Statistical significance was defined as p < 0.01 and p < 0.05 levels.
Results
A total of four rats died during the study program due to infection in two and resistance to feeding in the other two animals. Evaluation of tubular apoptotic changes as demonstrated by immuno-histochemical staining of TNF-alpha and Caspase-3 and crystal deposition in renal parenchyma during early as well as late follow-up period demonstrated the following findings.
Evaluation of tubular apoptotic changes
Apoptotic changes were found to be more prominent in tubular cells surrounding the crystals; however, some degree of apoptotic changes could also be found in tubular cells, even when no crystal formation was seen. On the other hand, apoptotic changes were prominent in distal tubular as well as collecting duct cells. Evaluation of apoptotic changes in renal tubular cells with respect to Caspase-3 positivity during early phase (14 days) showed that while number of animals demonstrating moderate to severe apoptotic changes was meaningfully lower in control group, a considerable number of animals undergoing EG only showed moderate to severe degree of apoptotic changes (n: 9, 90 %) (Fig. 1). Tutukon application in these animals, however, demonstrated an evident limitation of apoptotic changes with limited (n: 7, 70 %) degree of changes observed in the majority of the animals (Fig. 2). The mean percentage of apoptotic cells stained by Caspase-3 was higher in Group 1 animals (2.30 ± 0.67) than in animals in Group 2 (1.50 ± 1.08) during this period. The same findings were noted in favor of Tutukon application during late-phase (28 days) evaluation. Mean percentage values were (2.25 ± 0.71) and (1.22 ± 0.83) (p = 0.021) in both groups, respectively this period (Table 1). Thus our results indicate that Tutukon application seemed to prevent or at least limit the formation of apoptotic changes in renal tubular epithelium during both the early (day 14) and late period (day 28). However, while the significance was meaningful during late evaluation period (p = 0.021), it was near to statistical significance but not meaningfully significant during early-phase evaluation (p = 0.079).

Evident Caspase-3 expression with immunohistochemistry staining in an animal undergoing hyperoxaluria induction without any protective agent. (Caspase-3, original magnification ×400)

Minimal Caspase-3 expression with immunohistochemistry staining in an animal undergoing hyperoxaluria induction along with Tutukon application. (Caspase-3, original magnification ×400)
On the other hand again, TNF alpha expression after hyperoxaluria induction in study group animals showed evident apoptotic chances during early phase (14 days) with moderate to severe apoptotic changes in 8 (80 %) animals (Fig. 3). But these changes were found to be limited again in both control group (n: 1, 10 %) and in animals receiving Tutukon (n: 2, 20 %) (Fig. 4) (Table 2). The mean scores of apoptotic cells stained by TNF-alpha during this period was significantly higher in Group 1 animals (2.10 ± 0.74) than in animals in Group 2 (1.00 ± 0.67) (p = 0.005) during 14-day evaluation. The same findings were again obtained during late-phase (28 days) evaluation (Table 2).

Evident TNF- alpha expression with immunohistochemistry staining in an animal undergoing hyperoxaluria induction without any protective agent. (TNF-alpha, original magnification ×400)

Minimal TNF-alpha expression with immunohistochemistry staining in an animal undergoing hyperoxaluria induction along with Tutukon application. (TNF-alpha, original magnification ×400)
Evaluation of crystal deposition
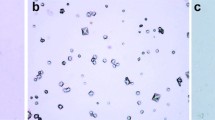
Examination of renal parenchymal tissue specimens from rats on an hyperoxaluric diet for 14 days revealed various degrees of crystal deposition, mainly in the tubular lumen. Apart from a slight degree of crystal deposition, no notable histologic alteration could be demonstrated in the interstitial areas. Crystal deposition was widespread in these animals both during early and late follow-up examination (Fig. 5). While severe crystal deposition was observed in 3 (30 %) rats, moderate and minimal deposition have been observed in 6 (60 %) and 1 (10 %) animals, respectively, during early phase (14 days). The overall mean crystal deposition value was 2.20 ± 0.63 in this group. Evaluation of the animals receiving Tutukon after hyperoxaluria induction, however, demonstrated the protective effect of this medication on the presence as well as severity of crystal formation. While severe crystal deposition was noted in 1 (10 %) rat, moderate and minimal deposition of crystal were present in 3 (30 %) and 6 (60 %) (Fig. 6) rats, respectively. Again, the mean value of crystal deposition was significantly lower in this group when compared with animals receiving EG only 1.50 ± 0.71 (p = 0.031). Last but not least, no evident crystal deposition has been observed in control group animals as expected (with a mean value for crystal deposition of 0.10 ± 0.32 (Table 3). The same findings were noted during late (28 days) evaluation indicating the limitation of crystal deposition by Tutukon after hyperoxaluria induction (p = 0.001). The degree of crystal deposition in all groups is given in Table 3.

Evident crystal formation (multiple areas with dense deposition) in an animal undergoing hyperoxaluria induction without any protective agent. (H&E, olympus polarizer filter, original magnification ×400)

Limited crystal deposition in an animal undergoing hyperoxaluria induction along with Tutukon application. (H&E, olympus polarizer filter, original magnification ×400)
Discussion
Experimental studies have well demonstrated that both CaOx crystals and/or oxalate ions forming after hyperoxaluric diet may play a critical role in the formation of urinary stones. Induction of hyperoxaluria has been found to be associated with cellular injury and necrosis in renal tubular epithelial cells [1, 3, 15]. Demonstration of enzymuria, proteinuria as well as membranuria, following an hyperoxaluric diet in animal models also supports this hypothesis to a meaningful extent [2]. Observation of tubular injury even in the absence of crystalluria suggests that the damage is not solely produced by CaOx crystals, but oxalate ions themselves may also be toxic to the renal tubular cells [16].
Regarding the mechanism of tubular cell injury, in addition to the original study performed by Khan et al. [15], other groups were also able to demonstrate the functional impairment of cellular components originates from oxidative stress which causes ROS formation [4, 7, 8]. Scheid et al. [6] demonstrated that among the various mono-and dicarboxylates examined in their study, high urinary oxalate level was the most common causative factor for increased free radical production and subsequent cell death. Results of some well-conducted animal studies led the authors to propose that the interaction of oxalate ions with renal epithelial cells may initiate a programmed sequence of events which may in turn lead to cell proliferation or cell death [4, 5, 9, 10]. Last but not least, Koul et al. [4] were able to show that there may be a causal link between the oxalate-induced increase in C-myc gene expression and oxalate-induced increase in cellular proliferation. All these observations indicate that, as a distinctive form of cell death, apoptosis could also be responsible for renal tubular injury induced by hyperoxaluria. To support this proposal, we were able to demonstrate renal tubular cell apoptotic changes in rabbit model where the degree and extent of apoptosis were found to be time dependent [17]. After observing the injurious effects of hyperoxaluria causing crystal deposition and apoptotic changes in renal tubular epithelium, physicians began to search for agents to prevent or at least minimize the extent of these pathologic alterations [18].
Among the agents used so far, verapamil and nifedipine (calcium channel blockers) were found to limit histologic changes and crystal deposition to a certain extent [12, 19, 20]. Potassium citrate again was found to limit stone recurrence after extracorporeal shockwave lithotripsy [7], and as highly potent antioxidant agents, allopurinol and vitamin E have been used to minimize free oxygen radical-induced alterations in certain tissues by inhibiting ROS formation [11, 13, 14, 21].
On the other hand, in addition to the use of these medical agents, recently published data clearly demonstrated that as a promising and effective alternative, herbal medicine may have a certain role in the prevention and metaphylaxis of renal stones [22, 23]. Phytotherapy applied in a complementary fashion for the conservative treatment of urolithiasis has been found to improve the results of lithotripsy and increase the efficacy of metaphylactic management of urinary tract stones [24]. Evaluation of the available data in the literature so far did show that majority of these phytotherapeutic agents have diuretic, anti-inflammatory, antioxidant, vasodilating, and spasmolytic effects [25, 26].
The active ingredients responsible for such specific effects have been found to be essential oils, flavonoids, saponins, xanthine derivatives and glycosides [25, 27–29]. Among the phytotherapeutic agents applied so far, Phyllanthus niruri has been found to be promising in the prevention of stone formation [25, 30] due to its potentially active compounds of genus Phyllanthus, alkaloids, flavonoids, lactones, steroids, terpenoids, lignans, and tannins. In addition to its well-demonstrated antispasmodic [26] and analgesic effects [25], this herbal agent has also been shown to inhibit CaOx endocytosis by renal tubular cells. Supporting this hypothesis again in a small clinical trial this agent appeared to reduce urinary calcium excretion amongst hypercalciuric stone formers [31]. Among the other herbal agents used to limit crystal formation and eventual stone formation, a Moroccan herb Hernaria hirsuta and green tea [22, 30] have also been found to be promising in the limitation of CaOx crystallization.
Taking the reported effects of such antioxidant as well as anti-inflammatory agents in the prevention of ischemia-induced renal tubular epithelial injury into account, in this present study we aimed to evaluate the possible limitation of tubular apoptotic changes and eventual crystal formation resulting from hyperoxaluric state using a potent antioxidant and anti-inflammatory herbal agent (Tutukon) in rat model.
Tutukon (Grand Medical, Spain) is a medication composed of different herbal ingredients demonstrating certain biological effects in different tissues (Fig. 1). Among these effects, the antioxidant potential is one of the most important characteristics of this drug due to its active ingredients. Published data show that among the 8 different ingredients of this herbal agent, alkaloids, rosmarinic acid, flavonoids [27], apigenin, luteolin [28], ekvizetonin saponin [29], and essential oils [32] are well known for their potent antioxidant as well as anti-inflammatory effects. Regarding the mechanism of action, studies have clearly shown that the above-mentioned active ingredients may reduce the permeability of kidney capillaries, dilate kidney blood vessels and ureters, restore the tubular epithelial function, induce an osmotic effect, inhibit synthesis and activation of inflammatory mediators, and thus prevent inflammatory alterations as well as crystal formation and growth [22, 24–26, 33].
Our results clearly demonstrated significant crystal formation/deposition together with apparent renal tubular cell apoptosis in animals undergoing hyperoxaluria induction by EG during the early phase of hyperoxaluric state (day 14). Quantitative examination of the cell apoptosis and crystal deposition indicated a significant difference between these animals and the ones receiving the preventive agent (Tutukon). As mentioned above, ischemia-induced oxidative stress in renal tubules and the inflammatory changes are the major underlying causes for tubular cell apoptosis and subsequent crystal formation/deposition. Our results again demonstrated that Tutukon with its potent ingredients: alkaloids, rosmarinic acid, flavonoids [27] apigenin, luteolin [28], ekvizetonin, saponin [29], and essential oils [32], may be protective enough in the limitation of such alterations causing crystal formation at least in experimental animal models. Treatment of the animals with Tutukon provided a significant protection from calcium oxalate deposition and apoptosis in tubular cells. However, it is clear that the dosage of the herbal agent used in rat model in this study does not match those used clinically in humans.
Conclusions
In the light of our findings and the reported literature data, it is clear that both hyperoxaluria itself and CaOx crystal formation are injurious to renal epithelial cells. Tubular cell apoptosis as a result of free radical formation causing lipid peroxidation is the main causative factor for these alterations. As a potent antioxidant medication, Tutukon was found to limit both crystal deposition and apoptotic changes in this present study indicating that the clinical application of such antioxidant and anti-inflammatory agents might limit the formation of urinary calculi, particularly in recurrent stone formers. However, we believe that further clinical and research studies are certainly needed to support the above-mentioned preventive effects of this drug in CaOx crystal formation.
References
Hackett RL, Shevock PN, Khan SR (1990) Cell injury associated with calcium oxalate crystalluria. J Urol 144:1535
Khan SR, Shevock PN, Hackett RL (1989) Urinary enzymes and calcium oxalate urolithiasis. J Urol 142:846
Lieske JC, Norris R, Swift H, Toback FG (1997) Adhesion, internalization and metabolism of calcium oxalate monohydrate crystals by renal epithelial cells. Kidney Int 52:1291
Koul H, Kennington L, Nair G, Honeyman T, Menon M, Scheid C (1994) Oxalate-induced initiation of DNA synthesis in LLC-PK1 cells, a line of renal epithelial cells. Biochem Biophys Res Commun 205:1632
Scheid CR, Koul H, Hill WA, Luber-Narod J, Jonassen J, Honeyman T, Kennington L, Kohli R, Hodapp J, Ayvazian P, Menon M (1996) Oxalate toxicity in in LLC-PK1 cells, a line of renal epithelial cells. J Urol 155:1112
Scheid CR, Koul H, Kennington L, Hill WA, Luber-Narod J, Jonassen J, Honeyman T, Menon M (1995) Oxalate-induced damage to renal tubular cells. Scanning Microsc 9:1097
Selvam R, Bijikurien T (1992) Effect of citrate feeding on free radical induced changes in experimental urolithiasis. Indian J Exp Biol 30:705
Strohmaier WL, Bichler KH, Koch J, Balk KN, Wilbert DM (1993) Protective effect of verapamil on shock wave-induced renal tubular dysfunction. J Urol 150:27
Sarıca K, Kupeli B, Budak M, Kosar A, Kavukcu M, Durak I, Gogus O (1997) Influence of experimental spermatic cord torsion on the contralateral testes in rats: evaluation of tissue free oxygen scavenger enzyme levels. Urol Int 58:208
Scheid C, Koul H, Hill WA, Luber-Narod J, Kennington L, Honeyman T, Jonassen J, Menon M (1996) Oxalate toxicity in LLC-PK1 cells: role of free radicals. Kidney Int 49:413
Benyi L, Weilherg Z, Puyun L (1995) Protective effects of nifedipine and allopurinol on high energy shock wave induced acute changes of renal function. J Urol 153:596
Sarıca K, Bakır K, Yagcı F, Topcu O, Akbay C, Sayın N, Korkmaz C (1999) Limitation of possible enhanced crystal deposition by verapamil in renal parenchyma after shock wave application in rabbit model. J Endourol 13:343
Cohen PJ (1992) Allopurinol administered prior to hepatic ischemia in the rat prevents chemiluminescence following restoration of circulation. Can J Anesth 39:1090
Parekh MH, Lobel R, O’Connor L, Leggett RE, Levin RM (2001) Protective effect of Vitamin E on the response of the rabbit bladder to partial outlet obstruction. J Urol 166:341
Khan SR (1995) Calcium oxalate crystal interaction with renaltubular epithelium, mechanism of crystal adhesion and its impact on stone development. Urol Res 23:71
Khan SR, Shevock PN, Hackett RL (1992) Acute hyperoxaluria, renal injury and calcium oxalate urolithiasis. J Urol 147:226
Sarıca K, Yagcı F, Bakır K, Erturhan S, Ucak R (2001) Renal tubular injury induced by hyperoxaluria: evaluation of apoptotic changes. Urol Res 29:34
Ogawa Y, Yamaguchi K, Morozumi M (1990) Effects of magnesium salts in preventing experimental oxalate urolithiasis. J Urol 144:385
Sarıca K, Bakır K, Yagcı F, Erbagcı A, Topcu O, Uysal O (2000) Unilateral testicular torsion; protective effect of verapamil on contralateral testicular histology. Urol Int 62:159
Sarıca K, Ozer G, Soygur T, Yaman O, Ozer E, Ustun H, Yaman LS, Gogus O (1997) Preservation of shock-wave-induced renal histologic changes by Dermatan sulphate. Urology 49:145
Sarıca K, Kosar A, Yaman O, Beduk Y, Durak I, Gogus O, Kavukcu M (1996) Evaluation of ischemia after ESWL: detection of free oxygen radical scavenger enzymes in renal parenchyma subjected to high energy shock waves. Urol Int 57:221
Itoh Y, Yasui T, Okada A, Tozawa K, Hayashi Y, Kohri K (2005) Preventive effects of green tea on renal stone formation and the role of oxidative stress in nephrolithiasis. J Urol 173(1):271–275
Cho Hyuk Jin, Bae Woong Jin, Kim Su Jin, Hong Sung Hoo, Lee Ji Youl, Hwang Tae-Kon, Choi Yeong Jin, Hwang Sung Yeoun, Kim Sae Woong (2014) The inhibitory effect of an ethanol extract of the spores of Lygodium japonicum on ethylene glycol-induced kidney calculi in rats. Urolithiasis 42(4):309–315
Butterweck V, Khan SR (2009) Herbal medicines in the management of urolithiasis: alternative or complementary? Planta Med 75(10):1095–1103
Calixto JB, Santos AR, Cechinel Filho V et al (1998) A review of the plants of the genus Phyllanthus: their chemistry, pharmacology, and therapeutic potential. Med Res Rev 18:225
Calixto JB, Yunes RA, Neto AS et al (1984) Antispasmodic effects of an alkaloid extracted from Phyllanthus sellowianus: a comparative study with papaverine. Braz J Med Biol Res 17:313
Zadra M, Piana M, Brum TF, Boligon AA, Freitas RB, Machado MM, Stefanello ST, Soares FA, Athayde ML (2012) Antioxidant Activity and phytochemical composition of the leaves of Solanum guaraniticum A. St.-Hil. Molecules 17(11):12560–12574
Wang H, Yang L, Zu Y, Zhao X (2014) Microwave-assisted simultaneous extraction of luteolin and apigenin from tree peony pod and evaluation of its antioxidant activity. Sci World J 2014:506971
Xi M, Hai C, Tang H, Chen M, Fang K, Liang X (2008) Antioxidant and antiglycation properties of total saponins extracted from traditional Chinese medicine used to treat diabetes mellitus. Phytother Res 22(2):228–237
Atmani F, Slimani Y, Mimouni M et al (2004) Effect of aqueous extract from Herniaria hirsuta L. On experimentally nephrolithiasic rats. J Ethnopharmacol 95:87
Nishiura JL, Campos AH, Boim MA et al (2004) Phyllanthus niruri normalizes elevated urinary calcium levels in calcium stone forming (CSF) patients. Urol Res 32:362
Ariffin A, Rahman NA, Yehye WA, Alhadi AA (2014) Kadir FA:PASS-assisted design, synthesis and antioxidant evaluation of new butylated hydroxytoluene derivatives. Eur J Med Chem 2(87C):564–577
Bodakhe KS, Namdeo KP, Patra KC, Machwal L, Pareta SK (2013) A polyherbal formulation attenuates hyperoxaluria-induced oxidative stress and prevents subsequent deposition of calcium oxalate crystals and renal cell injury in rat kidneys. Chin J Nat Med 11(5):466–471
Conflict of interest
We have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Sahin, C., Sarikaya, S., Basak, K. et al. Limitation of apoptotic changes and crystal deposition by Tutukon following hyperoxaluria-induced tubular cell injury in rat model. Urolithiasis 43, 313–322 (2015). https://doi.org/10.1007/s00240-015-0777-1
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00240-015-0777-1