
Abstract
Introduction
Spectral shaping aims to narrow the X-ray spectrum of clinical CT. The aim of this study was to determine the image quality and the extent of radiation dose reduction that can be achieved by tin prefiltration for parasinus CT.
Methods
All scans were performed with a third generation dual-source CT scanner. A study protocol was designed using 100 kV tube voltage with tin prefiltration (200 mAs) that provides image noise levels comparable to a low-dose reference protocol using 100 kV without spectral shaping (25 mAs). One hundred consecutive patients were prospectively enrolled and randomly assigned to the study or control group. All patients signed written informed consent. The study protocol was approved by the local Institutional Review Board and applies to the HIPAA. Subjective and objective image quality (attenuation values, image noise, and contrast-to-noise ratio (CNR)) were assessed. Radiation exposure was assessed as volumetric CT dose index, and effective dose was estimated. Mann-Whitney U test was performed for radiation exposure and for image noise comparison.
Results
All scans were of diagnostic image quality. Image noise in air, in the retrobulbar fat, and in the eye globe was comparable between both groups (all p > 0.05). CNReye globe/air did not differ significantly between both groups (p = 0.7). Radiation exposure (1.7 vs. 2.1 mGy, p < 0.01) and effective dose (0.055 vs. 0.066 mSv, p < 0.01) were significantly reduced in the study group.
Conclusion
Radiation dose can be further reduced by 17% for low-dose parasinus CT by tin prefiltration maintaining diagnostic image quality.
Similar content being viewed by others

Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Multidetector helical computed tomography (CT) enables visualizing of small bony details individual anatomic variants and thickening of the mucosal surfaces. Three dimensional reconstructions are used for surgery planning and ease image-guided navigation as well as robotic surgery. However, the drawback of CT is its radiation burden. Patients referred for imaging are often of young age, and radiation sensitive organs like eye lenses and thyroid gland are directly or indirectly affected by X-rays during the examination. This is especially of concern when repetitive examinations are required. Magnetic resonance imaging visualizes sinonasal mucosal disease avoiding any radiation exposure, but is limited in delineating fine bony structures and is rather time consuming and expensive compared to CT. According to the ALARA principle (“as low as reasonably achievable”), radiation dose should be reduced as much as possible without impairing the diagnostic value. Different approaches to decrease the radiation exposure have been proposed including direct shielding, judicious adjustments of the tube settings, and iterative image reconstructions [1].
The radiation dose to the eye lenses can be significantly reduced by direct bismuth shielding of the orbits with the drawback of reduced image quality in the protected region [2]. Reducing the tube current leads to an increase in image noise, which is acceptable to a certain degree for the paranasal sinuses. Diagnostic accuracy can be preserved due to the high contrast between air, mucosa, and the bony walls [3–5]. Reducing the tube voltage represents another popular approach to decrease the radiation dose, even below the lower radiation exposure limits of the conventional technique using 120 kV. Another recently introduced approach to decrease the radiation dose below the lower edge of technically applicable radiation dose at 120 kV is spectral shaping. Third generation dual-source CT systems are equipped with additional tin prefiltration that removes the primarily low energy photons in the X-ray beam, which contribute little to image quality but increase the radiation dose. Thus, diagnostic image quality can be maintained at a reduced radiation dose [6, 7].
The aim of this comparative noninferiority study was to assess the effect of tin prefiltration on image quality and radiation dose at 100 kV compared to a standard CT protocol at 100 kV without tin filtration at equal image noise levels using the same CT unit.
Materials and methods
The study complies with the Declaration of Helsinki and the HIPAA and was performed with local ethics committee approval. Informed patient consent was obtained. Data acquisition was performed between October 2014 and June 2015. All scans were performed using a third generation dual-source CT system (Somatom Force, Siemens, Forchheim, Germany) in a single source mode with the following parameters: 0.5-s gantry rotation time, 192 × 0.6 mm collimation using a z-flying focal spot, tube current modulation switched off. Since tin prefiltration is only available at 100 and 150 kV, with higher diagnostic dose efficiency at 100 kV [6], the lower kV setting was used for this study. The lowest mAs setting at 100 kV without tin prefiltration is 25 mAs, which served as reference protocol. Phantom measurements (Gammex 464, Middleton, WI, USA) were performed to identify the tube current settings with tin prefiltration to reach a comparable image noise level. Line pair resolution was additionally assessed for both protocols as an objective quality measure. For clinical evaluation, 100 consecutive patients scheduled for paranasal sinus CT for inflammatory disease were randomized to the study or control group.
Patient position was supine with a slight reclination of the head aligning the upper jaw to the gantry in order to minimize artifacts from dental hardware in both groups. The scan range included the roof of the frontal sinuses to the maxillary alveolar process. Image reconstruction from the raw data set was performed in a 2-mm axial, 2-mm coronal, and 2-mm sagittal orientation using the same bone (Br64) and soft tissue kernels (Bf36). Additionally, thin overlapping slices in an axial orientation (0.6 mm slice thickness, 0.5 mm increment) were reconstructed using the same kernels for MPR evaluation and transferred to a 3D workstation (SyngoVia VA30A, Siemens Healthcare GmbH, Forchheim, Germany). For dose distribution, additional Monte Carlo simulations were performed with the study and reference protocol and a ROI with a size of 5 × 5 pixels were measured in the left eye lense.
Objective image quality
To obtain and to compare objective parameters between the two acquisition protocols, regions of interest (ROIs) were placed on axial 2-mm soft tissue reconstructions in both eye globes, in the retrobulbar fat and in the air within the maxillary sinuses. ROIs with at least an area of 2 mm2 were measured to obtain attenuation values (AV). Image noise (N) was considered as the standard deviation of the measurement in the eye globes. Attenuation differences between eye globe and air (A) as well as eye globe and retrobulbar fat (B) divided by image noise were used for calculation of contrast to noise ratios (CNR A or CNR B) according to the following equation:
In order to compare the CNR values independently of radiation dose, each obtained CNR value was dose normalized [8].
To account for anatomic differences between patients, the ROIs were chosen as large and as similar as possible, while carefully avoiding image artifacts and adjacent structures in order to prevent partial volume effects.
Subjective image quality
Subjective parameters were evaluated independently by two radiologists as proposed in the European Guidelines on Quality Criteria for CT. Both readers were blinded to all clinical data. “Entirely acquired volume from the apical edge of the frontal sinus to the palate and visually sharp reproduction of anatomic structures” (cortical and trabecular bone structures, frontal sinuses, sphenoid sinuses, orbitae, optic nerve and orbital muscles, ethmoid, maxilla and its sinuses, nasal cavity, and rhinopharynx) were evaluated on a dichotomous scale (1 yes; 2 no) image noise and spatial resolution were assessed on a 3-point scale (1 too much; 2 optimum; 3 too little), and the overall diagnostic image quality on a 4-point Likert scale (1 fully acceptable; 2 probably acceptable; 3 only acceptable under limited conditions; 4 unacceptable).
Radiation dose
The radiation exposure was assessed as volumetric CT dose index (CTDIvol) and dose-length product (DLP) provided by the scanner. For the control group, calculation of an effective dose (ED) associated with the CT examinations was based on multiplication of the DLP with a previously published conversion factor for the head region (0.0019 mSv × mGy−1 × cm−1) that is referenced to the 16-cm CTDI-phantom [9].
CTDIvol values from the study group, which are referenced to a 32-cm CTDI-phantom in the patient protocol, had to be converted to match the 16-cm reference CTDI-phantom from the patient protocol of the control group [9]. Therefore, an additional conversion factor of 2.5 was introduced [6]. As currently no energy spectra specific (100 kV + tin prefiltration) conversion factor is available, we extrapolated the conversion factor to calculate the DLP for the study group based on the publication from Deak et al. [9]. The extrapolation was done using a linear regression between the mean effective energies of the known tube spectra (80–140 kV) and the corresponding (known) conversion factors. We chose to prefer a linear regression over a more complex (polynomial) extrapolation because the conversion factors were too close (0.0018 and 0.0019 for all tube voltages) to identify a true trend of the conversion factor for higher effective energies. Assuming there is a small trend, we extrapolated a conversion factor of 0.00197 mSv × mGy−1 × cm−1.
Statistical analysis
Values are given as mean ± standard deviation if normal distribution was assumed by Kolmogorow-Smirnov tests and as median and range if normal distribution was not assumed. Sample size calculation was performed following a noninferiority hypothesis with a desired statistical power of 0.9 using the standard deviation of image noise from the ex ante trial (3 HU) and a noninferiority limit of 2 HU. All statistical tests were two-tailed and performed for the entire group size. Mann-Whitney U test was performed for radiation exposure, image noise, and CNR comparison between both groups. Nonparametric Wilcoxon signed-rank test was used for comparison of subjective image quality. Interrater agreement was assessed using Cohen’s kappa test, and values >0.61 were interpreted as substantial and >0.81 as almost perfect agreement according to Landis and Koch [10]. Significance levels of 0.05 were assumed. Test statistics are provided as standardized values. Statistical analysis was performed using a dedicated software package (SPSS Statistics, Version 19, SPSS Inc./IBM, Chicago, IL).
Results
Patient characteristics
Sample size calculation concluded that 39 patients are required per group to be 90% sure that the lower limit of a one-sided 95% confidence interval will be above the noninferiority limit of −2. We included a total of 100 patients that were randomized to the study (n = 50) and the control group (n = 50). In the study group, the population consisted of 21 female and 29 male patients with a mean age of 52 ± 16 years. In the control group, 24 female and 26 male patients were included with a mean age of 51 ± 16 years. Acute paranasal sinusitis was found in 29 patients (n = 18 in the study group and n = 11 in the control group) and chronic paranasal sinusitis in 10 patients (n = 4 in the study group and n = 6 in the control group). In 14 patients (n = 10 in the study and n = 4 in the control group), complete obstruction of the maxillary sinus was present.
Radiation exposure
Radiation exposure was very low in both groups, but significantly lower in the study group (CTDIvol 1.7 mGy vs. 2.1 mGy, p < 0.01). The mean ED using the study protocol with tin filtration was 0.055 mSv and 0.066 mSv in the control group (p < 0.01) which corresponds to 17% dose reduction. Detailed results are displayed in Table 1.
According to the Monte Carlo simulation, mean radiation dose for the left eye lense was μ: 7.1 mGy/Sigma: 4.4 for the study protocol and μ: 10.8 mGy/Sigma: 16.6 for the reference protocol which corresponds to 35% dose reduction (see Fig. 1).

Monte Carlo simulation with the reference and study protocol
Objective image quality
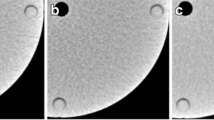
Both protocols were able to discriminate 10 line pairs per centimeter with slight subjective advantages in edge sharpness for the study protocol (Fig. 2).

Comparable resolution of 10 line pairs per centimeter is attained by the study (a) and the reference protocol (b) with slight subjective advantages in edge sharpness for the images with spectral shaping
Attenuation values in air (−979 ± 11 HU vs. −963 ± 12, p < 0.01), in the eye globe (5 ± 3 vs. 9 ± 5, p < 0.01), and in the retrobulbar fat (−81 ± 8 vs. -84 ± 11, p < 0.01) were significantly different between the study and the control group. Image noise in the eye globe (15.9 ± 2.4 vs. 15.8 ± 2.5, p = 0.70), in air (14.4 ± 3.0 vs. 14.7 ± 2.6, p = 0.08), and in the retrobulbar fat (17.3 ± 2.8 vs. 17.7 ± 2.6, p = 0.16) was comparable without statistically significant differences. CNR calculations for air and soft tissue of the eye globes were comparable between both groups (63.2 ± 10.5 vs. 62.9 ± 10.1, p = 0.7). Attenuation differences of the soft tissue measurements resulted in small but statistically significant decrease in CNR when calculated for the soft tissues of the eye bulbs and the retrobulbar fat (5.5 ± 1 vs. 6.2 ± 1.2, p < 0.01). However, CNR normalized to unit dose was higher for the study protocol (5.5/1.7 mGy = 3.2 mGy−1) compared to the reference (6.2/2.1 mGy = 3.0 mGy−1). Detailed results are displayed in Table 2.
Subjective image quality
All scans included the roof of the frontal sinus to the palate, and the evaluated anatomic structures were clearly discernible in all patients. All scans were fully acceptable. Subjective image noise and spatial resolution were rated optimal in both groups. Interrater agreement was perfect (kappa value = 1). Typical images of the study and control group are shown in Figs. 3, 4, and 5.

Image quality attained by the study (a/b) and the reference protocol (c/d), 2-mm slice thickness in a coronal (a/c), and an axial plane (b/d). Images are displayed with a soft tissue window of W:300, C:40. Patients were addressed to rule out sinusitis. Even thin bony structures like the lamina papyracea are clearly discernible in both groups

Image quality in patients with pansinusitis using the study (a/b) and the reference protocol (c/d), 2-mm slice thickness in coronal planes using a sharp (a/c), and a soft convolution kernel (b/d). Images are displayed with a bone window of W:3000, C: 1000 and soft tissue window of W:300, C:40. Extensive obstruction of the ethmoid cells and the maxillary sinus with clear delineation of the lamina papyracea and comparable image noise in the orbital soft tissues. Both protocols provide sufficient image quality to rule out orbital complications

Images of the study (a/b) and the reference protocol (c/d), 2-mm slice thickness in an axial (a/c), and coronal plane (b/d) using a soft convolution kernel. Images are displayed with a soft tissue window of W:300, C:40. Image noise is comparable in the retrobulbar fat, the eye globe and air
Discussion
We could demonstrate that equivalent image noise levels can be achieved at substantially reduced radiation exposure by spectral shaping using additional tin prefiltration in low-dose CT examinations of the paranasal sinuses. All evaluated anatomic landmarks were sufficiently visualized, and diagnostic confidence was maintained.
Different approaches to reduce the radiation dose in CT of the paranasal sinuses have been evaluated. Lowering of the tube current significantly reduces the exposure with the backside of increased image noise levels. With iterative reconstruction technique, image noise can be reduced as shown for other regions. Hoxworth et al. recently published a study comparing high dose parasinus CT (120 kV, 210 mA, and 31.6 mGy) with a low-dose parasinus CT (120 kV, 20 mA, and 2.9 mGy), performed back-to-back in 20 patients [11]. They concluded that iterative reconstruction algorithms (VEO, GE Healthcare) significantly improved image quality in the soft tissues, but negatively affected the detailed delineation of bony structures. Moreover, the lower limit of radiation exposure is limited by the minimum tube output in this approach with CTDIvol around 2.9–3.6 mGy using 120 kV, depending on the type of scanner [6, 11].
High pitch scan mode was proposed by other groups to combine the advantages of low dose and minimal motion artifacts due to the fast scan speed. However, dose distribution along the z-axis is less homogeneous using this approach and overranging is higher compared to conventional pitch modes [12].
Another alternative to further reduce radiation dose is low kV scanning. Bodelle et al. evaluated the diagnostic image quality and radiation dose of low-dose parasinus CT at 70 kV/75 mAs (2.3 mGy, n = 44) in comparison to 100 kV/40 mAs (4.0 mGy, n = 42) and 120 kV/40 mAs (6.3 mGy, n = 41). The attenuation of organ structures was increased, and the diagnostic confidence maintained using the 70 kV protocol, but they also concluded that the strong increase in image noise limits the potential for radiation dose reduction and yielded to a reduced subjective image quality [13].
Due to the high contrast of the relevant structures in parasinus CT—bone vs. mucosal soft tissue vs air—diagnostic image quality is much more limited by the image noise than the image contrast. Higher photon energies can decrease the image noise measured in the detector because of reduced absorption in the patient. Tin filtration narrows and shifts the X-ray spectra towards higher keV levels. Hence, radiation dose can be reduced while the obtained image noise is equivalent compared to a reference by absorbing the vast majority of low energy photons emitted from the X-ray tube.
Tin filtration was recently evaluated for the parasinus region in a cadaveric phantom study using different tube voltages, tube currents, pitch values, and rotation times to optimize image quality and radiation exposure on a third generation dual-source CT [6]. The best tradeoff between radiation dose and image quality was figured out for a low-dose protocol using 100 kV tube voltage and tin filtration (150 mAs, 1.2 mGy). However, the exact radiation dose reduction by means of tin prefiltration at equivalent noise levels was not yet assessed.
We could demonstrate that tin prefiltration substantially reduces radiation dose by an average of 17% with an even higher dose reduction of 35% for the eye lense while image noise, CNR for air and soft tissue, subjective image quality, and diagnostic confidence are maintained. Even when CNR for soft tissues like the eye bulb and the retrobulbar fatty tissue were statistically decreased using the study protocol, its CNR normalized to unit dose was higher. Thus, protocols using tin prefiltration might also provide dose efficient image quality if the clinical focus is on soft tissue structures, like ruling out orbital complications in symptomatic patients.
Some limitations of our study merit consideration. First, tin prefiltration is not available on the vast majority of CT systems at this moment. Second, we adapted the tube current setting in the study protocol to the image noise level obtained by the lowest applicable radiation dose using 100 kV without tin filter (25 mAs, 2.1 mGy) for comparative reasons. Thus, the radiation dose level used in this study (200m As, 1.7 mGy) was slightly higher than the optimum dose level found in the cadaveric phantom study (150 mAs, 1.2 mGy). Third, this study only compares protocols using 100 kV tube voltages. The radiation dose reduction by tin filtration at different tube voltages remains unclear and should be evaluated in further studies. Fourth, image quality of the proposed protocol was considered to be sufficient to detect or rule out sinusitis, to provide relevant anatomic information for surgery and allow 3D surgical navigation. Patients with other indications, like trauma or leakage of cerebrospinal fluid where additional soft tissue evaluation is necessary, were not included.
As a conclusion, we can summarize that spectral shaping by tin prefiltration allows for an average dose reduction of 17% without impairing the diagnostic image quality in low-dose parasinus CT using 100-kV tube voltages.
References
Lell MM, Wildberger JE, Alkadhi H, Damilakis J, Kachelriess M (2015) Evolution in computed tomography: the battle for speed and dose. Investig Radiol 50(9):629–644
Raissaki M, Perisinakis K, Damilakis J, Gourtsoyiannis N (2010) Eye-lens bismuth shielding in paediatric head CT: artefact evaluation and reduction. Pediatr Radiol 40(11):1748–1754
Brem MH, Zamani AA, Riva R et al (2007) Multidetector CT of the paranasal sinus: potential for radiation dose reduction. Radiology 243:847–852
Hagtvedt T, Aalokken TM, Notthellen J, Kolbenstvedt A (2003) A new low-dose CT examination compared with standard-dose CT in the diagnosis of acute sinusitis. Eur Radiol 13:976–980
Hojreh A, Czerny C, Kainberger F (2005) Dose classification scheme for computed tomography of the paranasal sinuses. Eur J Radiol 56:31–37
Lell MM, May MS, Brand M et al (2015) Imaging the parasinus region with a third-generation dual-source CT and the effect of tin filtration on image quality and radiation dose. AJNR Am J Neuroradiol 36(7):1225–1230
Wuest W, May M, Saake M et al (2016) Low-dose CT of the paranasal sinuses: minimizing X-ray exposure with spectral shaping. Eur Radiol 26(11):4155–4161
Buls N, Van Gompel G, Van Cauteren T et al (2015) Contrast agent and radiation dose reduction in abdominal CT by a combination of low tube voltage and advanced image reconstruction algorithms. Eur Radiol 25:1023–1031
Deak PD, Smal Y, Kalender WA (2010) Multisection CT protocols: sex- and age-specific conversion factors used to determine effective dose from dose-length product. Radiology 257:158–166
Landis JR, Koch GG (1977) The measurement of observer agreement for categorical data. Biometrics 33:159–174
Hoxworth JM, Lal D, Fletcher GP et al (2014) Radiation dose reduction in paranasal sinus CT using model-based iterative reconstruction. AJNR Am J Neuroradiol 35(4):644–649
Lell MM, May M, Deak P et al (2011) High-pitch spiral computed tomography: effect on image quality and radiation dose in pediatric chest computed tomography. Investig Radiol 46:116–123
Bodelle B, Wichmann JL, Klotz N et al (2015) Seventy kilovolt ultra-low dose CT of the paranasal sinus: first clinical results. Clin Radiol 70(7):711–715
Acknowledgements
We thank Petra Ruse and Katharina Roth for excellent patient management and Marie-Louise Haider for assistance in data management. This study was supported by the German government, Bundesministerium für Bildung und Forschung (01EX1012B, Spitzencluster Medical Valley).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
We declare that all human and animal studies have been approved by the ethics committee and have therefore been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments. We declare that all patients gave informed consent prior to inclusion in this study
Conflict of interest
MM is part of Siemens Speakers’ Bureau; ML is part of Siemens and Bayer Speakers’ Bureau, has grants from Siemens and Bayer and consults for Bracco;
MB is part of Siemens Speakers’ Bureau; MU is part of Siemens, Bayer, Bracco and Medtronic Speakers’ Bureau; and WW is part of Siemens Speakers’ Bureau.
No financial support for this study was received from any company listed above.
Rights and permissions
About this article

Cite this article
May, M.S., Brand, M., Lell, M.M. et al. Radiation dose reduction in parasinus CT by spectral shaping. Neuroradiology 59, 169–176 (2017). https://doi.org/10.1007/s00234-016-1780-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-016-1780-0