
Abstract
Introduction
The aim of this study was to determine the effect of different volumes of contrast material with and without a saline chaser on tissue enhancement in multidetector row CT (MDCT) of the head and neck.
Methods
In a blind prospective fashion, 120 patients were randomized into the following four groups: group 1, 80 ml contrast material administered at a flow rate of 2.0 ml/s; group 2, 80 ml followed by 40 ml saline at 2.0 ml/s; group 3, 60 ml at 1.5 ml/s; and group 4, 60 ml followed by 30 ml saline at 1.5 ml/s. The attenuation values of the carotid artery, internal jugular vein, and muscle were measured at an interval of 1.5 s in each patient. The degree of perivenous artifacts was subjectively assessed.
Results
Mean attenuation values in the carotid artery and internal jugular vein were significantly higher in groups 1 and 2 than in groups 3 and 4. The width of the diagnostic window (both carotid and jugular enhancement >150 HU) were significantly longer in groups 1 and 2 than in groups 3 and 4. The addition of a saline chaser did not result in improved vascular enhancement or a wider diagnostic window, but reduced perivenous artifacts, compared with using contrast material alone.
Conclusion
Reduction of contrast material from 80 to 60 ml results in insufficient enhancement of neck vessels. In addition, the benefit of a saline chaser technique is not obvious except for its ability to reduce perivenous artifacts.
Similar content being viewed by others
Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
With the introduction of spiral CT scanners, scanning time has gradually decreased in CT studies of the head and neck during the last decade. This allows optimized use of contrast materials and can reduce the dose of contrast material required. This decrease in contrast material has several potential benefits. The most obvious advantage is cost saving as a result of the increasing number of CT examinations. Another advantage of reduction in contrast material dose is the potential decrease in the likelihood of subsequent nephrotoxicity [1, 2]. Although there is still controversy concerning the volume of contrast material necessary for spiral CT of the head and neck, volumes of 90–120 ml are regarded as the standard recommended doses [3–8].
Several groups of investigators have reported the use of a saline chaser in contrast material dose reduction in thoracic CT [9–11], abdominal CT [12, 13], and CT angiography [14–17]. To our knowledge, however, the potential of a saline chaser in contrast material dose reduction has not been evaluated for CT of the head and neck. In addition, there are few reports regarding the effect of contrast material volume on vascular enhancement in the head and neck using multidetector row spiral CT (MDCT).
Thus, the purpose of this study was to investigate the effect of different volumes of contrast material with and without a saline chaser on tissue enhancement in MDCT of the head and neck.
Materials and methods
Patient population
Between February and May 2006, 125 consecutive patients who were scheduled to undergo CT of the head and neck were prospectively examined. The majority of the patients were referred for assessment of a palpable neck mass, for staging of pharyngeal or laryngeal tumor, or for imaging follow-up after tumor therapy. Five patients were excluded from the evaluation because of technical errors in scanning (n=3) or extravasation of contrast material (n=2). None of the patients included in the study had a medical history of cardiac output failure. Thus, a total of 120 patients (72 men and 48 women) were finally included for assessment. Their mean age was 47.8±16.0 years, their mean weight 61.5±10.7 kg, their mean height 164.4±8.8 cm, and their mean body mass index (BMI) 22.7±3.2 kg/m2. BMI was calculated as body weight/height2 (kg/m2).
The 120 patients were randomly assigned to the following four groups: group 1 (n=30), 80 ml contrast material administered at a flow rate of 2.0 ml/s; group 2 (n=30), 80 ml contrast material followed by 40 ml saline at 2.0 ml/s; group 3 (n=30), 60 ml contrast material at 1.5 ml/s; and group 4 (n=30), 60 ml contrast material followed by 30 ml saline at 1.5 ml/s. Table 1 shows the characteristics of the patients in each group. Analysis of variance (ANOVA) revealed no significant differences between the four patient groups regarding age (P=0.56), sex (P=0.27), body weight (P=0.57), height (P=0.53), or BMI (P=0.17).
This clinical study received the approval of our institutional review board, and all patients gave written informed consent before enrollment in the study.
CT protocol and contrast material infusion
The contrast material used in all patients was iohexol (Omnipaque 300; Amersham Health, Cork, Republic of Ireland) with an iodine concentration of 300 mg/ml. In each group with different contrast protocols, the bolus of contrast material with or without subsequent saline solution was injected into a right arm vein in 15 patients, while a left arm vein was used in the remaining 15 patients.
In this study, flushing with saline solution was performed using a single power injector (CT9000ADV; Liebel-Flarsheim, Cincinnati, Ohio) in which the saline solution was loaded on top of the contrast material. The mixing of contrast material and saline after loading into the injector could be considered negligible because the density of saline is less than that of the contrast material. Thus, the contrast material was injected first, followed by the saline chaser. The saline chaser technique with a single injector has been described in detail in previously [9, 13].
All CT scans were obtained using a 16 detector-row CT scanner (MX8000 Infinite Detector Technology; Philips, Haifa, Israel) with the following parameters: section thickness 3 mm, table feed per rotation 4.5 mm, pitch 1.5, gantry rotation time 0.75 s, collimation 4×1.5 mm, 120 kV and 200 mAs, and scan delay 40 s. The scanning range was planned in a craniocaudal direction from the level of the skull base to the tracheal bifurcation (mean coverage 250 mm, range 230–270 mm). Axial images were reconstructed at 3-mm increments on a 512×512 matrix.
Data collection and analysis
All CT scans were transferred to a picture archiving and communication system workstation (Pi-ViewStar, INFINITT, Seoul, Korea) for analysis.
Quantitative evaluation of contrast enhancement was performed by a radiologist (S.Y.Y, with 2 years of experience in CT of the head and neck), who was unaware of the injection protocol. The attenuation values (in Hounsfield units, HUs) were measured in six regions: the right and left carotid arteries (CAs), the right and left internal jugular veins (IJVs), and muscles (sternocleidomastoid or temporalis) in the right and left neck. All measurements were performed at an interval of 1.5 s (every fifth section) along the z-axis, using a circular region-of-interest (ROI). If a vessel of interest was occluded, obscured by artifact, or surgically missing, the attenuation values of the referred vessel at that scanning level were not measured.
After data acquisition, the mean attenuation value was calculated for each patient by averaging all the attenuation values. In addition, time-attenuation curves were generated based on the averaged attenuations of the CA, IJV, and muscle in each slice (Figs. 1, 2 and 3). From these graphs, the diagnostic window defined as the time during which the attenuation of both CA and IJV simultaneously exceeded 150 HU was determined for each patient.

Mean time-attenuation curves obtained in the carotid artery with four different contrast material injection protocols. Contrast material injections of 80 ml and 80 ml followed by saline chaser (groups 1 and 2) resulted in higher attenuation, and a reliably wide diagnostic window (over 150 HU). Regardless of protocol, the maximum attenuation was reached approximately 50 s after contrast material injection

Mean time-attenuation curves obtained in the internal jugular vein with four different contrast material injection protocols. Contrast material injection of 60 ml with or without saline chaser (groups 3 and 4) resulted in lower attenuation and narrower diagnostic window (over 150 HU) than injection of 80 ml with or without saline chaser (groups 1 and 2). The maximum attenuation was reached approximately 50 s after contrast material injection in all four groups
Two radiologists (D.Y.Y. and S.K.C., with 11 and 4 years of experience in CT of the head and neck, respectively), who were unaware of the injection protocol used, graded by consensus perivenous artifacts adjacent to the subclavian or brachiocephalic vein. They were asked to subjectively evaluate perivenous artifacts using the following four-point scale: grade 1 corresponded to minimal artifacts and very sharp vessel edges; grade 2 corresponded to mild artifacts (maximum extension of beam hardening artifacts ≤10 mm); grade 3 corresponded to moderate artifacts (>10 mm), but evaluation of perivascular structures still possible; and grade 4 corresponded to pronounced artifacts completely obscuring the anatomic detail of perivascular structures.
In addition, differences in vascular enhancement and perivenous artifacts between patients receiving contrast material injection via the right arm (n=60) and left arm (n=60) were also assessed.
Statistical analysis
Mean attenuation values obtained from the CA, IJV, and muscle were compared using one-way ANOVA. If a significant difference was found, a pair-wise comparison with Student’s t-test was performed. In addition, the relationships between mean attenuation and intrinsic parameters (age, sex, body weight, height, and BMI) of the patient were analyzed with a linear regression model. Perivenous artifacts was compared with the Kruskal-Wallis nonparametric rankF-test. If a significant difference was found, a pair-wise comparison with the Mann-Whitney U-test was performed. In addition, differences in attenuation and perivenous artifacts between patients with right and left arm injection were assessed with the unpaired Student’s t-test and the χ2 test.
P values <0.05 were considered to indicate a statistically significant difference. All statistical analyses were performed with commercially available software (SPSS 10.0 for Windows; SPSS, Chicago, Ill.).
Results
The attenuation values in the CA, IJV, and muscle for the four protocols are summarized in Table 2. The groups that received 60 ml of contrast material (groups 3 and 4) had significantly lower arterial and venous attenuations than the groups that received 80 ml of contrast material (groups 1 and 2; P<0.05 or <0.01). The addition of a saline chaser resulted in a slight decrease in attenuation values of both the CA and IJV, regardless of injection volume, although the differences were not significant (group 1 vs 2 and group 3 vs 4).
Figures 1 and 2 show the mean time-attenuation curves of the CA and IJV for each group, respectively. The attenuation profiles of the CA and IJV were similar in all groups, showing an increase of attenuation to a maximum and a decrease of attenuation to the end of the scan. The time point when the mean attenuation values of both the CA and IJV ROIs reached their maximum were 50.5 s after injection of contrast material in all groups. The mean (±SD) times during the diagnostic window when both the CA and IJV simultaneously exceeded the 150 HU level were 15.8±3.6 s in group 1, 14.6±4.9 s in group 2, 11.8±4.7 s in group 3, and 9.8±5.7 s in group 4. The widths of the diagnostic window were significantly narrower for groups that received 60 ml of contrast material (groups 3 and 4) than for groups that received 80 ml of contrast material (groups 1 and 2; P<0.001).
In all groups, there were weak inverse correlations between weight and the mean attenuation values of the vessel (slope −1.2 to about −2.2; P<0.001; r 2=0.16 to about 0.18) and between height and the mean attenuation values of the vessel (slope −1.9 to about −3.7; P<0.001; r 2=0.16 to about 0.19). Linear regression analysis showed no correlation between the mean attenuation values of the vessel and age (r 2=0.05), sex (r 2=0.03), and BMI (r 2=0.02). The adjusted mean attenuation values of the vessel for age, sex, body weight, height, and BMI in a regression model showed the same significant differences between the groups.
The attenuation values of the muscle were not significantly different between the four groups. The time-attenuation curves for muscle (Fig. 3) showed no single strong peak of contrast enhancement, regardless of the protocol, with no differences between the groups.

Mean time-attenuation curves obtained in muscle with four different contrast injection protocols. Regardless of protocol, the curves show no single strong peak of contrast enhancement. There were no significant differences between the groups
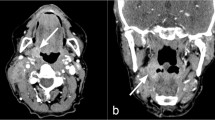
The qualitative grading results for perivenous artifacts are summarized in Table 3. The calculated mean values (±SD) for the perivenous artifacts graded on the four-point scale were 2.66±0.92 for group 1, 1.90±0.80 for group 2, 2.63±0.93 for group 3, and 1.93±0.74 for group 4. A comparison between groups with the same dose (group 1 vs 2 and group 3 vs 4) showed that the use of saline chaser significantly reduced perivenous beam-hardening artifacts (P<0.01 for both comparisons; Figs. 4 and 5). However, there were no significant differences in the visual assessment of perivenous artifacts for the comparisons group 1 vs 3 and group 2 vs 4.

CT scan of the neck obtained after administration of 60 ml contrast material in a 61-year-old woman shows dense contrast within the right subclavian vein resulting in pronounced beam hardening artifacts (arrows). Perivenous artifacts were graded as 4

CT scan of neck obtained after administration of 80 ml contrast material followed by 40 ml saline in an 81-year-old woman shows homogeneous enhancement and a sharp edge through the right subclavian vein (arrows). Perivenous artifacts were graded as 1
The baseline characteristics were not significantly different between patients with right and left arm injection in the combined evaluation of all groups (data not shown). Combined data from all 120 patients revealed no significant differences between patients with right and left arm injection in any of the contrast enhancements of the CA, IJV, and muscle (Table 4). In addition, the mean (±SD) values for perivenous artifacts were 2.40±0.93 for patients with left arm injection and 2.20±1.00 for patients with right arm injection (P>0.05).
Discussion
The recent development of MDCT scanners may further reduce the volume of contrast material as shorter scanning times are possible compared with single-detector row CT scanners [18]. In this study using 16-channel MDCT scanners, we evaluated the possibility of reducing the volume of contrast material from 80 to 60 ml, because 80 ml of contrast material has been the standard dose for CT of the head and neck in our department.
Our study clearly showed that 60 ml of contrast material resulted in a significantly lower mean attenuation in comparison to 80 ml of contrast material and, thus, unacceptable vessel contrast. These results are similar to those of Keberle et al. [8], who studied the effects of reducing the contrast material to 90 ml (300 mg/ml of iodine) and found no significant decrease in vessel and tumor enhancement in four-channel MDCT of the neck. However, a further reduction in volume of contrast material (i.e. to 70 ml) resulted in a significant decrease in vessel enhancement in their study. Although the mean body weight of the subjects was not mentioned in their study, our study group (mean body weight 61.5 kg) seems to be comparable to that in their study in a Western population.
In most studies of contrast media a fixed volume of contrast material was used regardless of individual differences in age, sex, and body weight. The last of these factors (body weight) appears to be the most important patient-related factor affecting the magnitude of tissue enhancement [19–21]. In our study, there was a weak correlation between increasing patient weight and decreasing attenuation value of the vessel. Therefore, weight-adjusted dose of contrast material appears to be desirable in order to achieve adequate contrast enhancement, particularly in populations with higher body weights. The 80 ml of contrast material used in our study corresponds to 1.3 ml/kg of contrast material with an iodine concentration of 300 mg/ml. Finally, there was also a weak inverse correlation between vascular enhancement and height of the patient. However, this correlation was considered to be attributable to the body weight.
Theoretically, a saline chaser technique has several potential benefits: clearing the intravenous catheter with a connecting tube of contrast material, keeping the bolus of contrast material more compact on its course from the peripheral vein to the heart with minimal mixing with blood, and avoidance of pooled contrast material in the arm veins [9–17]. It has been reported in the other anatomic territories studied that the use of a saline chaser can reduce the volume of contrast material without a decrease in vascular enhancement [9–11, 14, 15], can prolong the period of the phase of adequate vascular enhancement [11, 12], and can lessen perivenous streak artifacts [9, 10, 12].
The results of the present study confirmed that the use of a saline chaser substantially reduces perivenous artifacts, which may obscure supraclavicular or mediastinal lesions. However, our study did not show any significant difference in attenuation of the neck vessels with a saline chaser technique. Moreover, we observed slightly lower attenuation values for both the CA and IJV in groups 2 and 4 (with saline chaser) than in groups 1 and 3 (without saline chaser). Previous studies have not revealed such a decrease in attenuation after the additional infusion of a saline chaser. This discrepancy could partly be explained by the relatively small amounts of contrast material (60 and 80 ml) and low flow rates (1.5 and 2.0 ml/s). Although not directly proven, it can be assumed that the saline solution itself dilutes the administered contrast material at the peripheral vein then decreases the iodine concentration if small volumes of contrast material are administered at low injection rates. The benefit of a saline chaser may be more obvious with larger amounts of contrast material and higher flow rates than were used in the present study.
In accordance with the results of a consensus conference [5], we consider attenuation values of cervical vessels of more than 150 HU to be sufficient for CT of the head and neck. We believe that vascular attenuation of more than 200 HU is actually not necessary for differentiation from lymph nodes. Most parts of the mean arterial and venous time-attenuation curves of the patients examined with the 80 ml at 2.0 ml/s protocol (group 1) ran above the 150 HU level (Figs. 1 and 2), therefore indicating adequate vascular enhancement. However, a reduction in volume and flow rate to 60 ml at 1.5 ml/s (group 3) resulted in consistently lower attenuation values, and thus a significantly narrower diagnostic window. On the other hand, as shown by comparison of the mean time-attenuation curves of group 1 vs 2 and group 3 vs 4, the application of a saline chaser did not provide a wider window of adequate vascular enhancement.
Several authors have proposed the preferential use of a right arm vein for intravenous administration of contrast material in CT of the different anatomic territories [17, 22–24]. They have suggested that left arm injection may provide lower image quality than right arm injection because of the longer path of the contrast material through the venous system in the left arm [17] or physiological narrowing in the left brachiocephalic vein [25]. In this study, however, there was no significant difference in the mean attenuation values between patients with right and left arm injection. Further study with larger groups of patients is needed to determine the influence of right versus left arm injection of contrast material on image quality.
There are several limitations to our study. First, the overall scan time in this study (mean 23.5 s) with a 16-channel CT scanner was not substantially shorter than with previous four-channel scanners. The 16-channel CT scanner has the capability of scanning the entire neck from the skull base to the thoracic inlet within 15 s. However, we chose to use our standardized CT protocol with a combination of a 3-mm section thickness, a pitch of 1.5, and a 0.75-s gantry rotation time, considering the heat limitations of the tube and tube-cooling delay. Further study using a higher-performance scanner with a shorter scanning period is needed. Second, the small number of patients with primary neck tumors in our study did not allow reliable comparisons between the contrast protocols for tumor enhancement. For further assessment of diagnostic efficacy, larger numbers of patients with a proven solid tumor would need to be examined in each group.
In conclusion, reducing the contrast material from 80 to 60 ml resulted in insufficient enhancement of neck vessels. Furthermore, our study also indicated that the benefit of a saline chaser is not obvious, except in reducing perivenous artifacts, when 80 or 60 ml of contrast material is administered for MDCT of the head and neck.
References
Lasser EC, Lyon SG, Berry ML (1997) Reports on contrast media reactions: analysis of data from reports to the U.S. Food and drug administration. Radiology 203:605–610
Tublin ME, Murphy ME, Tessler FN (1998) Current concepts in contrast media-induced nephropathy. AJR Am J Roentgenol 171:933–939
Spreer J, Krahe T, Jung G, Lackner K (1995) Spiral versus conventional CT in routine examinations of the neck. J Comput Assist Tomogr 19:905–910
Harris EW, LaMarca AJ, Kondroski EM, Murtagh FR, Clark RA (1996) Enhanced CT of the neck: improved visualization of lesions with delayed imaging. AJR Am J Roentgenol 167:1057–1058
Feuerbach S, Lorenz W, Klose KJ, et al (1996) Administration of contrast medium in spiral computed tomography: results of a consensus conference. Rofo 164:158–165
Sakai O, Nakashima N, Shibayama C, Shinozaki T, Furuse M (1997) Asymmetrical or heterogeneous enhancement of the internal jugular veins in contrast-enhanced CT of the head and neck. Neuroradiology 39:292–295
Groell R, Willfurth P, Schaffler GJ, et al (1999) Contrast-enhanced spiral CT of the head and neck: comparison of contrast material injection rates. AJNR Am J Neuroradiol 20:1732–1736
Keberle M, Tschammler A, Hahn D (2002) Single-bolus technique for spiral CT of laryngopharyngeal squamous cell carcinoma: comparison of different contrast material volumes, flow rates, and start delays. Radiology 224:171–176
Hopper KD, Mosher TJ, Kasales CJ, et al (1997) Thoracic spiral CT: delivery of contrast material pushed with injectable saline solution in a power injector. Radiology 205:269–271
Haage P, Schmitz-Rode T, Hubner D, et al (2000) Reduction of contrast material dose and artifacts by a saline flush using a double power injector in helical CT of the thorax. AJR Am J Roentgenol 174:1049–1053
Irie T, Kajitani M, Yamaguchi M, et al (2002) Contrast-enhanced CT with saline flush technique using two automated injectors: how much contrast medium does it save? J Comput Assist Tomogr 26:287–291
Sadick M, Lehmann KJ, Diehl SJ, et al (1997) Bolus tracking and NaCl bolus in biphasic spiral CT of the abdomen (in German). Rofo 167:371–376
Dorio PJ, Lee FT, Henseler KP, et al (2003) Using a saline chaser to decrease contrast media in abdominal CT. AJR Am J Roentgenol 180:929–934
Cademartiri F, van der Lugt A, Luccichenti G, Pavone P, Krestin GP (2002) Parameters affecting bolus geometry in CTA: a review. J Comput Assist Tomogr 26:598–607
Cademartiri F, Mollet N, van der Lugt A, et al (2004) Non-invasive 16-row multislice CT coronary angiography: usefulness of saline chaser. Eur Radiol 14:178–183
Schoellnast H, Tillich M, Deutschmann MJ, Deutschmann HA, Schaffler GJ, Portugaller HR (2004) Aortoiliac enhancement during computed tomography angiography with reduced contrast material dose and saline solution flush: influence on magnitude and uniformity of the contrast column. Invest Radiol 39:20–26
de Monyé C, Cademartiri F, de Weert TT, Siepman DAM, Dippel DWJ, van Der Lugt A (2005) Sixteen-detector row CT angiography of carotid arteries: comparison of different volumes of contrast material with and without a bolus chaser. Radiology 237:555–562
Rubin GD, Shiau MC, Leung AN, Kee ST, Logan LJ, Sofilos MC (2000) Aorta and iliac arteries: single versus multiple detector-row helical CT angiography. Radiology 215:670–676
Platt JF, Reige KA, Ellis JH (1999) Aortic enhancement during abdominal CT angiography: correlation with test injections, flow rates, and patient demographics. AJR Am J Roentgenol 172:53–56
Macari M, Israel GM, Berman P, et al (2001) Infrarenal abdominal aortic aneurysm at multi-detector row CT angiography: intravascular enhancement without a timing acquisition. Radiology 220:519–523
Ho LM, Nelson RC, Thomas J, Gimenez EI, DeLong DM (2004) Abdominal aortic aneurysms at multi-detector row helical CT: optimization with interactive determination of scanning delay and contrast medium dose. Radiology 232:854–859
Suzuki H, Oshima H, Shiraki N, Ikeya C, Shibamoto Y (2004) Comparison of two contrast materials with different iodine concentrations in enhancing the density of the aorta, portal vein and liver at multi-detector row CT: a randomized study. Eur Radiol 14:2099–2104
Ertl-Wagner BB, Hoffmann RT, Bruning R, et al (2004) Multi-detector row CT angiography of the brain at various kilovoltage settings. Radiology 231:528–535
Ertl-Wagner BB, Bruning R, Blume J, et al (2005) Prospective, multireader evaluation of image quality and vascular delineation of multislice CT angiography of the brain. Eur Radiol 15:1051–1059
Tanaka T, Uemura K, Takahashi M, et al (1993) Compression of the left brachiocephalic vein: cause of high signal intensity of the left sigmoid sinus and internal jugular vein on MR images. Radiology 188:355–361
Conflict of interest statement
We declare that we have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Yoon, D.Y., You, S.Y., Choi, C.S. et al. Multi-detector row CT of the head and neck: comparison of different volumes of contrast material with and without a saline chaser. Neuroradiology 48, 935–942 (2006). https://doi.org/10.1007/s00234-006-0146-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00234-006-0146-4