
Abstract
Background
The safety and efficacy of tirofiban for patients with acute ischemic stroke (AIS) remains controversial. We therefore conducted a systematic review and meta-analysis.
Methods
We searched PubMed, EMBASE, Cochrane Library, Web of Science, and related international clinical trials registries through March 31, 2019, using the terms “tirofiban” and “stroke”. All apparently unconfounded randomized controlled trials (RCTs) and cohort studies with two arms comparing treatment with and without tirofiban for AIS were included in this review. Primary outcomes included symptomatic intracranial hemorrhage (sICH), fatal ICH, mortality, and modified Rankin Scale (mRS 0–2) at 3 months.
Results
Seventeen studies including 2914 AIS patients were identified. Pooled results showed that tirofiban treatment in AIS did not increase the risk of sICH (OR, 0.95; 95% CI, 0.71–1.28; p = 0.75) or mortality (OR, 0.80; 95% CI; 0.64–1.02; p = 0.07). However, fatal ICH increased significantly in the tirofiban treatment group (OR, 2.84; 95% CI, 1.38–5.85; p = 0.005), and subgroup analysis showed that tirofiban via intra-arterial (IA) administration was associated with increased risk of fatal ICH (OR, 2.90; 95% CI, 1.12–7.55; p = 0.03), while intravenous (IV) administration was not (OR, 2.75; 95% CI, 0.92–8.20; p = 0.07). In addition, tirofiban showed no obvious improvement in functional outcome (mRS 0–2) (OR, 1.29; 95% CI, 0.97–1.71; p = 0.08).
Conclusion
Tirofiban seems to be safe in systemic treatment and may represent a potential choice for management of AIS. However, intra-arterial administration requires further adequately controlled studies in order to develop an appropriate protocol, similar to that in cardiology.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Tirofiban is a highly selective, fast-acting non-peptide glycoprotein IIb/IIIa (Gp IIb/IIIa) platelet receptor antagonist with a short half-life. It has been approved for the treatment of acute coronary syndromes and has been proven effective and safe in numerous studies [1]. Extending to acute cerebrovascular occlusion, tirofiban also appears to be a feasible treatment, as demonstrated by several preliminary studies from different stroke centers [2,3,4,5]. The rapid technological advancements in endovascular therapy have further encouraged the administration of tirofiban in acute ischemic stroke (AIS) [6,7,8]. However, its efficacy post-endovascular therapy has raised concerns due to an association with increased risk of fatal intracranial hemorrhage (ICH) and poor outcomes in patients with ischemia [9]. A recent prospective cohort study also suggests that tirofiban treatment increases the risk of fatal ICH in ischemic stroke patients receiving endovascular thrombectomy [10]. Since no consensus has been achieved on the clinical use of tirofiban in AIS patients [11], we aimed to conduct a meta-analysis of cohort studies to compare the safety and efficacy of a tirofiban versus no-tirofiban regimen for AIS treatment.
Methods
We conducted this study following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [12]. All analyses in this meta-analysis are based on previously published studies, and thus no ethical approval or patient consent were required.
Search strategy
We searched PubMed, EMBASE, Cochrane Library, and Web of Science through March 31, 2019, using the search terms “tirofiban” and “stroke”. A similar search strategy was applied in international clinical trial registries, including the Stroke Trials Registry (www.strokecenter.org/trials), ClinicalTrials.gov (www.clinicaltrials.gov/), EU Clinical Trials Register (www.clinicaltrialsregister.eu), Current Controlled Trials (www.controlled-trials.com), and World Health Organization International Clinical Trials Registry Platform (http://apps.who.int/trialsearch/). In addition, references from relevant published original articles were retrieved manually, and the corresponding author was contacted when necessary. Studies were limited to clinical subjects, and no language restrictions were imposed.
Selection criteria
Randomized controlled trials (RCTs) and cohort studies incorporating tirofiban treatment alone or in combination with other conventional therapies were selected for review if they met the following criteria: (1) included patients with confirmed AIS; (2) compared the efficacy and/or safety between treatment with and without tirofiban; and (3) reported outcomes including at least one of the following: symptomatic intracranial hemorrhage (sICH), fatal ICH, any ICH, systemic hemorrhage, mortality, modified Rankin Scale (mRS) at 3 months, or recanalization rate (Thrombolysis in Cerebral Infarction [TICI] 2b/3).
Exclusion criteria
The following were excluded: (1) studies with duplicate or overlapping data; (2) those with no reporting of specified outcomes; (3) single-arm studies; (4) studies in which both arms included tirofiban treatment; and (5) those with fewer than 10 patients in either group.
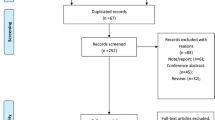
It should be mentioned that no restriction was applied in the group receiving tirofiban with regard to route of administration, dosage, or treatment course. The specific process of study selection is shown in Fig. 1.

Flowchart of study selection process
Data extraction and management
Two investigators (J.H.G. and J.J.S.) retrieved potential studies by title and abstract, and then reviewed the full article to identify the appropriate studies according to the inclusion and exclusion criteria. The data were extracted independently by the same two investigators. The tabulated data included first author, publication year, country, study design and period, number of patients, basic characteristics of patients, intervention strategy, tirofiban dosage regimen, and outcomes measurement. When the two investigators could not reach a consensus or had any potential doubt, resolution was achieved by discussion, or turned over to a third investigator (H.Y.) for decision.
Assessment of quality and risk of bias
The Cochrane risk-of-bias assessment tool was used to evaluate the potential sources of bias in the included RCTs [13], and the quality of the cohort studies was assessed using the Newcastle–Ottawa Scale [14]. Quality control and bias identification were performed independently by two investigators (J.H.G. and J.J.S.), and any disagreements were resolved by a third investigator (H.Y.).
Outcomes definition
Primary outcomes considered were sICH, fatal ICH, mortality, and functional outcome (mRS 0–2) [15] at 3 months. Secondary outcomes considered were any ICH, systemic hemorrhage, functional outcome (mRS 0–1) [16] at 3 months, and recanalization rate (TICI 2b/3) [17]. Outcomes were defined according to the definitions used in the individual studies.
Data synthesis and statistical analysis
The meta-analysis was conducted using Review Manager (RevMan) version 5.3 (The Cochrane Collaboration 2014, Nordic Cochrane Centre, Copenhagen, Denmark). For all outcomes, pooled odds ratios (OR) and 95% confidence intervals (CIs) were calculated according to the Mantel–Haenszel method with a fixed-effects or random-effects model according to the heterogeneity among all included studies. The I2 statistic by the χ2 test for heterogeneity was quantified to measure inconsistency across studies. A value of I2 greater than 50% was considered as indicative of substantial heterogeneity, and the random-effects model was used. Otherwise, a fixed-effects model according to the Mantel–Haenszel method was adopted. When substantial heterogeneity was confirmed, subgroup analyses (stratified by administration route, dosage) and forest plots were conducted to probe the source of heterogeneity as far as possible. In addition, subgroup analyses were performed by administration route for all primary outcomes. Publication bias was estimated qualitatively by funnel plots for primary outcomes.
Results
Study selection and study characteristics
From 545 studies retrieved from the literature, 17 studies [2,3,4,5,6,7,8,9,10, 18,19,20,21,22,23,24,25] were included in our final analysis (Fig. 1). A total of 2914 individuals were enrolled, with 1241 in the tirofiban group and 1673 in the control group. Participants were derived from two RCTs [2, 3], eight prospective cohort studies [5, 6, 9, 10, 19,20,21, 24], and seven retrospective cohort studies [4, 7, 8, 18, 22, 23, 25] (Table I in Electronic Supplementary Material [ESM]).
Among the 17studies selected, eight were from European countries (four in Germany, three in Italy, one in Switzerland) and nine were from Asian countries (eight in China, one in Korea). All studies similarly compared a regimen of tirofiban versus no tirofiban with other treatments, with the exception of two studies that compared tirofiban with intravenous (IV) aspirin [3, 8]. No significant differences were found in age, National Institutes of Health Stroke Scale (NIHSS) on administration, time from onset to treatment (OTT), or occlusion site between the tirofiban and comparative group in most of the included studies. However, the route of administration and dosage of tirofiban differed among studies, with intra-arterial (IA) administration in six studies and IV administration in the other 11 studies.
Study quality and publication bias
Of the two included RCTs, one [3] had a low risk of all evaluated types of bias, and the other [2] had low risk of selection, detection, reporting, and other potential bias, but had a high risk of performance bias because of its open-label design, and its attrition bias was unclear, as the study did not address in detail the four patients who were lost to follow-up (Table II in the ESM).
Risk of bias among the cohort studies was assessed using the Newcastle–Ottawa Scale (Table III in ESM). The risk of selection, comparability, and outcome bias was found to be low in all the studies. More specifically, patients in the control group were recruited from a different center in two studies [4, 21], recombinant tissue plasminogen activator (rt-PA) dosage was lower in the tirofiban group than in the control group in one study [4], onset to treatment time (OTT) was significantly longer in the tirofiban group than in the control group in one study [24], and no proper description of patients lost to follow-up was available in one study [24]. The overall score of the Newcastle–Ottawa Scale was 130/135 (96.3%), which is considered to represent an overall high quality. Funnel plot inspection revealed no evidence of publication bias among studies regarding primary outcomes (Figure I in ESM).
Primary safety outcomes
Tirofiban did not increase the risk of sICH in patients with AIS (17 studies [2,3,4,5,6,7,8,9,10, 18,19,20,21,22,23,24,25]; OR, 0.95; 95% CI, 0.71–1.28; p = 0.75), and subgroup analysis by route of administration showed that neither IV nor IA increased the risk of sICH (OR, 0.88; 95% CI, 0.55–1.40; p = 0.58 and OR, 1.01; 95% CI, 0.69–1.46; p = 0.97, respectively) (Fig. 2). Tirofiban significantly increased the risk of fatal ICH (5 studies [4, 7,8,9,10]; OR, 2.84; 95% CI, 1.38–5.85; p = 0.005); subgroup analysis showed that tirofiban administered by IA significantly increased the risk of fatal ICH (OR, 2.90; 95% CI, 1.12–7.55; p = 0.03), but no significant difference was found in the IV subgroup (OR, 2.75; 95% CI, 0.92–8.20; p = 0.07) (Fig. 3). Tirofiban did not increase the risk of mortality at 3 months (15 studies [2,3,4,5, 7, 8, 10, 18,19,20,21,22,23,24,25]; OR, 0.80; 95% CI, 0.64–1.02; p = 0.07); subgroup analysis showed that neither IV nor IA increased the risk of mortality (OR, 0.80; 95% CI, 0.53–1.20; p = 0.28 and OR, 0.81; 95% CI, 0.60–1.08; p = 0.15, respectively) (Fig. II in ESM).

Odds ratio with 95% confidence interval (CI) estimates for symptomatic intracranial hemorrhage (sICH) (tirofiban vs. control) by individual study and pooled results (IV: intravenous, IA: intra-arterial)

Odds ratio with 95% confidence interval (CI) estimates for fatal intracranial hemorrhage (fatal ICH) (tirofiban vs. control) by individual study and pooled results (IV: intravenous, IA: intra-arterial)
Primary efficacy outcome
Tirofiban showed no significant improvement in functional outcome (mRS 0–2) (10 studies [6,7,8,9, 18, 21,22,23,24,25]; OR, 1.29; 95% CI, 0.97–1.71; p = 0.08) for AIS patients, and the result was unchanged in subgroup analysis stratified by route of administration (IV: OR, 1.35; 95% CI, 0.74–2.49; p = 0.33 and IA: OR, 1.23; 95% CI, 0.94–1.62; p = 0.12, respectively) (Fig. III in ESM).
Secondary outcomes
Tirofiban did not increase the risk of either ICH (17 studies [2,3,4,5,6,7,8,9,10, 18,19,20,21,22,23,24,25]; OR, 1.02; 95% CI, 0.70–1.48; p = 0.93; Fig. IV in ESM) or systemic hemorrhage (6 studies [3, 4, 19, 20, 23, 25]; OR, 0.77; 95% CI, 0.41–1.45; p = 0.41; Fig. V in ESM) in AIS patients. No difference in good outcome (mRS 0–1) (9 studies [3, 7,8,9,10, 19, 20, 22, 25]; OR, 1.10; 95% CI, 0.87–1.39; p = 0.44; Fig. VI in ESM) or recanalization (TICI 2b/3) rate (8 studies [8,9,10, 21, 22, 24, 25]; OR, 1.00; 95% CI, 0.74–1.34; p = 0.98; Fig. VII in ESM) was observed between the tirofiban and control groups.
Discussion
Tirofiban is highly selective for inhibiting GPIIb/IIIa receptors, and it is rapidly eliminated after cessation of infusion due to its short half-life of about 2 h; thus it is widely used in the treatment of ischemic heart disease, including unstable angina pectoris, myocardial infarction (MI), and percutaneous transluminal coronary angioplasty (PTCA). By analogy, it is also considered as a potential alternative for AIS, and has been extensively evaluated in ischemic stroke, alone or as adjunctive therapy with intravenous thrombolysis and endovascular therapy [26]. As early as 2001, Junghans et al. [5] performed a baseline-matched prospective cohort study and demonstrated no additional increased risk of cerebral bleeding with the use of tirofiban in AIS. Similarly, a double-blind randomized trial found no association with increased risk of sICH compared with intravenous administration of aspirin [3]. The placebo-controlled phase II Safety of Tirofiban in AIS (SaTIS) trial also found no increased risk of cerebral hemorrhage with tirofiban treatment in acute stroke [2]. However, Kellert et al. [9] reported that tirofiban was associated with increased risk of fatal ICH in endovascular therapy for AIS.
The current meta-analysis of 17 studies with a total of 2914 AIS patients indicated that tirofiban carried no increased risk of sICH, any ICH, systemic hemorrhage, or mortality, but it revealed a probability of increased risk of fatal ICH. Subgroup analysis showed that intravenous infusion of tirofiban was safe, but intra-arterial administration was associated with an increased risk of fatal ICH. Additionally, subgroup analysis stratified by anterior circulation stroke (ACS) and posterior circulation stroke (PCS) was conducted in several of the studies reviewed [7, 9, 10]. Kellert et al. [9] reported that fatal ICH occurred more frequently in tirofiban-treated patients with ACS (13.3% vs. 3.1%; p = 0.05), and Wu et al. [10] also noted an increased risk of fatal ICH in an ACS subgroup (10.3% vs. 1.9%, p = 0.015). However, Zhao et al. [7] suggested that tirofiban introduced no difference in fatal ICH for patients with ACS (3.8% vs. 4.6%, p = 1.000). Pooled analysis showed that tirofiban seemed to increase the risk of fatal ICH in ACS (OR, 2.73; 95% CI, 1.16–6.45; p = 0.02) but not in PCS (OR, 4.35; 95% CI, 0.74–25.56; p = 0.10) (Fig. VIII in ESM).
In view of the dose-dependent inhibitory effects on platelet aggregation [27], the proper dosage regimen is a key point for tirofiban administration. The most commonly adopted protocol included intravenously administered tirofiban with a 30-min loading infusion at a rate of 0.4 μg/kg/min followed by continuous infusion of 0.1 μg/kg/min for 12 to 48 h according to the PRISM-PLUS protocol for acute coronary syndrome [27]. However, a high dose of 0.6 μg/kg/min for 30 min followed by an infusion of 0.15 μg/kg/min for 72 h was administered in the study by Torgano et al. [3]. Sensitivity analysis to exclude this study yielded no change in the results (sICH: OR, 0.92; 95% CI, 0.57–1.49; p = 0.74). For intra-arterial application, a bolus of tirofiban was administered at a dose ranging from 0.25 to 1.0 mg [7, 8, 10, 21, 22, 25], which varied among different studies. Intravenous thrombolysis (IVT) with rt-PA was administered in 10 studies [4, 7,8,9,10, 19, 21,22,23,24], typically in a standard dose of 0.9 mg/kg. A reduced dose of rt-PA (0.6 mg/kg) was used in both the ACS and PCS groups in the study by Kellert et al. [9], and IVT plus tirofiban was found to be safe and feasible for both groups with optimized dosing.
Several limitations should be taken into consideration when interpreting the results of this meta-analysis, especially for fatal ICH. First, dosage regimens among included studies were not completely consistent, especially for intra-arterial administration. A precise dosage regimen for intra-arterial administration of tirofiban is an important issue requiring clarification. Second, types of vessel occlusion (large vessel or arterioles) were not specified in most of the included studies, the exception being the study by Kang et al. [21], in which only patients with large vessel occlusion (LVO) were enrolled, and results suggested that intra-arterial infusion of tirofiban was effective and safe in the treatment of acute stroke patients with emergent LVO. The selection of suitable patients for tirofiban treatment according to occlusion site might improve outcomes in AIS. Third, aside from tirofiban, treatments such as unfractionated heparin, endovascular therapy, and IVT varied among studies. The heterogeneity of endovascular treatment devices used among different research institutions should also be considered. Fourth, the definition of sICH varied among studies, including NINDS [28], ECASSII [29], ECASS III [16], SITS-MOST [15], and Heidelberg Bleeding Classification [30]. Additionally, only a few studies reported on fatal ICH, which might introduce additional bias to this outcome. These considerations highlight the need for future well-controlled studies to assess the risk of fatal ICH with tirofiban administration in patients with AIS, especially for those undergoing endovascular therapy.
In conclusion, tirofiban appears to be associated with low risk when administered systemically during the management of acute stroke, and thus warrants further clinical studies. Intra-arterial administration seems to carry a higher risk, and a protocol and registry similar to that for cardiology should be developed for the neuroradiological community.
References
Baxter Healthcare Corporation. AGGRASTAT® (tirofiban hydrochloride) injection, for intravenous use. Available at: https://www.accessdatafdagov/drugsatfda_docs/label/2019/020912s027,020913s026lblpdf. Accessed 28 May 2019
Siebler M, Hennerici MG, Schneider D, von Reutern GM, Seitz RJ, Rother J, Witte OW, Hamann G, Junghans U, Villringer A, Fiebach JB (2011) Safety of tirofiban in acute ischemic stroke: the SaTIS trial. Stroke 42(9):2388–2392. https://doi.org/10.1161/strokeaha.110.599662
Torgano G, Zecca B, Monzani V, Maestroni A, Rossi P, Cazzaniga M, Manganaro D, Boiti C, Zilioli E, Borutti G, Falaschi F, Mandelli C (2010) Effect of intravenous tirofiban and aspirin in reducing short-term and long-term neurologic deficit in patients with ischemic stroke: a double-blind randomized trial. Cerebrovasc Dis 29(3):275–281. https://doi.org/10.1159/000275503
Seitz RJ, Hamzavi M, Junghans U, Ringleb PA, Schranz C, Siebler M (2003) Thrombolysis with recombinant tissue plasminogen activator and tirofiban in stroke: preliminary observations. Stroke 34(8):1932–1935. https://doi.org/10.1161/01.Str.0000080535.61188.A6
Junghans U, Seitz RJ, Aulich A, Freund HJ, Siebler M (2001) Bleeding risk of tirofiban, a nonpeptide GPIIb/IIIa platelet receptor antagonist in progressive stroke: an open pilot study. Cerebrovasc Dis 12(4):308–312. https://doi.org/10.1159/000047726
Palumbo V, Saia V, Nappini S, Romani I, Nencini P, Inzitari D, Mangiafico S (2010) Preliminary evaluation of hemorrhagic risk of systemic tirofiban in acute stroke patients treated with endovascular approach. Cerebrovasc Dis 29(suppl 2):206. https://doi.org/10.1159/000321266
Zhao W, Che R, Shang S, Wu C, Li C, Wu L, Chen J, Duan J, Song H, Zhang H, Ling F, Wang Y, Liebeskind D, Feng W, Ji X (2017) Low-dose tirofiban improves functional outcome in acute ischemic stroke patients treated with endovascular thrombectomy. Stroke 48(12):3289–3294. https://doi.org/10.1161/strokeaha.117.019193
Gruber P, Hlavica M, Berberat J, Victor Ineichen B, Diepers M, Nedeltchev K, Kahles T, Remonda L (2018) Acute administration of tirofiban versus aspirin in emergent carotid artery stenting. Interv Neuroradiol. https://doi.org/10.1177/1591019918808777
Kellert L, Hametner C, Rohde S, Bendszus M, Hacke W, Ringleb P, Stampfl S (2013) Endovascular stroke therapy: tirofiban is associated with risk of fatal intracerebral hemorrhage and poor outcome. Stroke 44(5):1453–1455. https://doi.org/10.1161/strokeaha.111.000502
Wu Y, Yin C, Yang J, Jiang L, Parsons MW, Lin L (2018) Endovascular thrombectomy: tirofiban increases bleeding risk in acute stroke patients. Stroke 49(11):2783–2785. https://doi.org/10.1161/strokeaha.118.022919
Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, Biller J, Brown M, Demaerschalk BM, Hoh B, Jauch EC, Kidwell CS, Leslie-Mazwi TM, Ovbiagele B, Scott PA, Sheth KN, Southerland AM, Summers DV, Tirschwell DL (2018) 2018 guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 49(3):e46–e110. https://doi.org/10.1161/str.0000000000000158
Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, Shekelle P, Stewart LA (2015) Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst Rev 4:1. https://doi.org/10.1186/2046-4053-4-1
Higgins JP, Altman DG, Gotzsche PC, Juni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA (2011) The Cochrane Collaboration's tool for assessing risk of bias in randomised trials. BMJ (Clinical Research Ed) 343:d5928. https://doi.org/10.1136/bmj.d5928
Stang A (2010) Critical evaluation of the Newcastle-Ottawa scale for the assessment of the quality of nonrandomized studies in meta-analyses. Eur J Epidemiol 25(9):603–605. https://doi.org/10.1007/s10654-010-9491-z
Wahlgren N, Ahmed N, Davalos A, Ford GA, Grond M, Hacke W, Hennerici MG, Kaste M, Kuelkens S, Larrue V, Lees KR, Roine RO, Soinne L, Toni D, Vanhooren G (2007) Thrombolysis with alteplase for acute ischaemic stroke in the safe implementation of thrombolysis in stroke-monitoring study (SITS-MOST): an observational study. Lancet 369(9558):275–282. https://doi.org/10.1016/s0140-6736(07)60149-4
Hacke W, Kaste M, Bluhmki E, Brozman M, Davalos A, Guidetti D, Larrue V, Lees KR, Medeghri Z, Machnig T, Schneider D, von Kummer R, Wahlgren N, Toni D (2008) Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med 359(13):1317–1329. https://doi.org/10.1056/NEJMoa0804656
Higashida RT, Furlan AJ, Roberts H, Tomsick T, Connors B, Barr J, Dillon W, Warach S, Broderick J, Tilley B, Sacks D (2003) Trial design and reporting standards for intra-arterial cerebral thrombolysis for acute ischemic stroke. Stroke 34(8):e109–e137. https://doi.org/10.1161/01.Str.0000082721.62796.09
Renieri L, Consoli A, Rosi A, Chiarotti I, Vignoli C, Lanzetta C, Limbucci N, Nappini S, Nencini P, Inzitari D, Mangiafico S (2014) Safety and clinical outcome in patients treated with GP IIbIIIa inhibitors (Tirofiban) in endovascular treatment of acute ischemic stroke: a single centre experience. Cerebrovasc Dis 37(Suppl 1):652
Li W, Lin L, Zhang M, Wu Y, Liu C, Li X, Huang S, Liang C, Wang Y, Chen J, Feng W (2016) Safety and preliminary efficacy of early tirofiban treatment after alteplase in acute ischemic stroke patients. Stroke 47(10):2649–2651. https://doi.org/10.1161/strokeaha.116.014413
Lin L, Li W, Liu CC, Wu Y, Huang SH, Li XS, Liang CR, Wang H, Zhang LL, Xu ZQ, Wang YJ, Feng W, Zhang M (2017) Safety and preliminary efficacy of intravenous tirofiban in acute ischemic stroke patient without arterial occlusion on neurovascular imaging studies. J Neurol Sci 383:175–179. https://doi.org/10.1016/j.jns.2017.10.041
Kang DH, Yoon W, Kim SK, Baek BH, Lee YY, Kim YW, Kim YS, Hwang YH, Kim JT, Park MS (2018) Endovascular treatment for emergent large vessel occlusion due to severe intracranial atherosclerotic stenosis. J Neurosurg 1–8. https://doi.org/10.3171/2018.1.Jns172350
Yu T, Lin Y, Jin A, Zhang P, Zhou X, Fang M, Liu X (2018) Safety and efficiency of low dose intra-arterial tirofiban in mechanical thrombectomy during acute ischemic stroke. Curr Neurovasc Res 15(2):145–150. https://doi.org/10.2174/1567202615666180605104931
Liu J, Shi Q, Sun Y, He J, Yang B, Zhang C, Guo R (2019) Efficacy of tirofiban administered at different time points after intravenous thrombolytic therapy with alteplase in patients with acute ischemic stroke. J Stroke Cerebrovasc Dis. https://doi.org/10.1016/j.jstrokecerebrovasdis.2018.12.044
Pan X, Zheng D, Zheng Y, Chan PWL, Lin Y, Zou J, Zhou J, Yang J (2019) Safety and efficacy of tirofiban combined with endovascular treatment in acute ischemic stroke. Eur J Neurol. https://doi.org/10.1111/ene.13946
Zhang S, Hao Y, Tian X, Zi W, Wang H, Yang D, Zhang M, Zhang X, Bai Y, Li Z, Sun B, Li S, Fan X, Liu X, Xu G (2019) Safety of intra-arterial tirofiban administration in ischemic stroke patients after unsuccessful mechanical thrombectomy. J Vasc Interv Radiol 30(2):141–147.e141. https://doi.org/10.1016/j.jvir.2018.08.021
Yang M, Huo X, Miao Z, Wang Y (2019) Platelet glycoprotein IIb/IIIa receptor inhibitor tirofiban in acute ischemic stroke. Drugs. https://doi.org/10.1007/s40265-019-01078-0
Platelet Receptor Inhibition in Ischemic Syndrome Management in Patients Limited by Unstable Signs and Symptoms (PRISM-PLUS) Study Investigators (1998) Inhibition of the platelet glycoprotein IIb/IIIa receptor with tirofiban in unstable angina and non–Q-wave myocardial infarction. N Engl J Med 338(21):1488–1497. https://doi.org/10.1056/nejm199805213382102
National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group (1995) Tissue plasminogen activator for acute ischemic stroke. N Engl J Med 333(24):1581–1588. https://doi.org/10.1056/nejm199512143332401
Hacke W, Kaste M, Fieschi C, von Kummer R, Davalos A, Meier D, Larrue V, Bluhmki E, Davis S, Donnan G, Schneider D, Diez-Tejedor E, Trouillas P (1998) Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Second European-Australasian acute stroke study investigators. Lancet 352(9136):1245–1251. https://doi.org/10.1016/S0140-6736(98)08020-9
von Kummer R, Broderick JP, Campbell BC, Demchuk A, Goyal M, Hill MD, Treurniet KM, Majoie CB, Marquering HA, Mazya MV, San Roman L, Saver JL, Strbian D, Whiteley W, Hacke W (2015) The Heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke 46(10):2981–2986. https://doi.org/10.1161/strokeaha.115.010049
Funding
This work was supported by Changzhou Science and Technology Program (Grant No.CE20195048; CJ20190034), the Science and Technology Development Foundation of Nanjing Medical University (Grant No. NMUB2018061) and Natural Science Foundation of Jiangsu Province (Grant No.BK20191157) .
Author information
Authors and Affiliations
Contributions
J.H.G., Q.Z.S., and G.J.L. conceptualized and designed the study, and J.H.G. and J.J.S. selected studies and planned the analysis. J.H.G., J.J.S., and H.Y. contributed to the development of the selection criteria, the assessment strategy for the risk of bias, and the data extraction criteria. Z.Q.S. and Q.W. provided statistical expertise. J.H.G. drafted the manuscript, and D.S., Z.Q.S., and G.J.L. participated in critical revision of the manuscript. All authors read, provided feedback, and approved the final manuscript as submitted.
Corresponding authors
Ethics declarations
Conflict of interest
All authors declare that they do not have a conflict of interest.
Additional information
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
ESM 1
(DOC 239 kb)
Rights and permissions
About this article

Cite this article
Gong, J., Shang, J., Yu, H. et al. Tirofiban for acute ischemic stroke: systematic review and meta-analysis. Eur J Clin Pharmacol 76, 475–481 (2020). https://doi.org/10.1007/s00228-019-02817-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-019-02817-8