
Abstract
Familial Hypocalciuric Hypercalcaemia (FHH) Type 1 is caused by an inactivating mutation in the calcium-sensing receptor (CASR) gene resulting in elevated plasma calcium levels. We investigated whether FHH is associated with change in bone density and structure. We compared 50 FHH patients with age- and gender-matched population-based controls (mean age 56 years, 69 % females). We assessed areal BMD (aBMD) by DXA-scans and total, cortical, and trabecular volumetric BMD (vBMD) as well as bone geometry by quantitative computed tomography (QCT) and High-Resolution peripheral-QCT (HR-pQCT). Compared with controls, FHH females had a higher total and trabecular hip vBMD and a lower cortical vBMD and hip bone volume. Areal BMD and HRpQCT indices did not differ except an increased trabecular thickness and an increased vBMD at the transition zone between cancellous and cortical bone in of the tibia in FHH. Finite element analyses showed no differences in bone strength. Multiple regression analyses revealed correlations between vBMD and P-Ca2+ levels but not with P-PTH. Overall, bone health does not seem to be impaired in patients with FHH. In FHH females, bone volume is decreased, with a lower trabecular volume but a higher vBMD, whereas cortical vBMD is decreased in the hip. This may be due to either an impaired endosteal resorption or corticalization of trabecular bone. The smaller total bone volume suggests an impaired periosteal accrual, but bone strength is not impaired. The findings of more pronounced changes in females may suggest an interaction between sex hormones and the activity of the CaSR on bone.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Familial Hypocalciuric Hypercalcemia (FHH) is a rare autosomal dominant inherited calcium metabolic disorder. The condition is most often due to an inactivating variant in the calcium-sensing receptor (CASR) gene (FHH Type 1) causing lifelong mild to moderate hypercalcemia with inappropriately high-normal or elevated PTH levels [1]. Recently, similar phenotypes have been shown to be attributable to mutations in the G-protein subunit a11 (GNA11) gene (FHH type 2) and adaptor protein 2 sigma 1 (AP2S1) gene (FHH Type 3) with loci placed on chromosome 19p and 19q, respectively [2, 3]. In most studies, patients with FHH have been reported to have only few or no symptoms [4, 5].
Physiologically, calcium homeostasis and bone remodeling are closely related hence the importance of studying the skeleton in FHH in detail. A study in knockout mice has shown that CaSR has a critical role for skeleton development [6]. Previously, three minor cross-sectional studies did not demonstrate changes in areal bone mineral density (aBMD) as assessed by dual- energy X-ray absorptiometry (DXA) scans in patients with FHH [7–9], although a slightly increased bone turnover in FHH has been reported by some investigators [8, 10]. In the previous cross-sectional study from our group, aBMD was normal in FHH patients as assessed by z scores calculated according to a reference population. Nevertheless, an enhanced phenotypic expression of the studied CASR variants in terms of increasing hypercalcemia was associated with higher aBMD at the lumbar spine and hip [11]. This finding is in accordance with data reported by Theman et al. [12] on patients with an activating mutation in the CASR (autosomal dominant hypocalcemia [ADH]) in whom bone mineralization may be reduced. However, a meta-analysis of genome wide association data did not link the CASR to aBMD or risk of osteoporotic fractures [13].
The hyperparathyroid hypercalcemia in patients with FHH is similar to the biochemical characteristics in patients with mild primary hyperparathyroidism (PHPT) [14]. In PHPT, aBMD is decreased at multiple sites with predominance at the forearm as measured by DXA [15]. Furthermore Hansen et al. [16] recently reported that female patients with PHPT have negative alteration of geometry, volumetric density, and microarchitecture in radius, but not in tibia as measured by high-resolution peripheral quantitative computed tomography (HR-pQCT) scans. In the case of FHH, parathyroidectomy is inappropriate, as it does not cure FHH-associated hypercalcemia [14]. Since we have no treatment for FHH, it is important to assess whether this life-long inherited disorder has any skeletal consequences for the patients. To the best of our knowledge, no data are available on volumetric BMD (vBMD) or bone structure in FHH. In order to investigate possible effects of the CaSR on bone, we performed DXA and 3-dimensional (3-D) scanning techniques (QCT- and HR-pQCT-scans) in patients diagnosed with FHH.
Subjects and Methods
Design and Participants
In a cross-sectional study, we compared 50 FHH patients with 51 gender- and aged-matched population-based controls aged 18–85 years. All studied subjects were Caucasians. The design of the study has previously been reported [5]. In brief, we excluded patients and controls with major medical or social problems suspected to influence study outcome including: impaired renal function (plasma creatinine >125 μmol/l), malignancies, untreated intestinal malabsorption (including active pancreatitis), chronic disabling disease, or prior hospital admission due to chronic drug or alcohol abuse. In addition, we excluded pregnant women and patients treated with drugs known to affect the CaSR (lithium, strontium, or cinacalcet) as well as subjects diagnosed with calcium metabolic diseases except osteoporosis.
Patients
At the out-patient clinic of our hospital, we had information on 82 patients with genetically verified FHH in terms of inactivating mutations in CASR (FHH type 1). The diagnosis was supported by documented hypercalcemia, low renal calcium excretion, inappropriately high PTH, and verified parents or offspring with hypercalcemia when available. One patient had hypercalcemia, elevated PTH, and an offspring with hypercalcemia, but mutation analysis only showed a p.R990G variant in the CASR gene, which is now considered to be a common variant not associated with FHH [17, 18]. The patient has not yet been studied for mutations in other possible genes. Sixty-six were known by earlier studies by our group, whereas 16 had been identified since our last work-up on FHH [11]. Two had died, and one had emigrated, leaving 79 potential patients to be recruited among whom 50 patients with FHH were included in the present study.
Controls
From the Danish Civil Registrations System, we retrieved a list of randomly selected control subjects aged 18–85 and residing in the county of Aarhus, Denmark. For each FHH patient, an invitation was sent to between five and ten gender-matched controls of similar age (±2 years). In parts of the investigations, we were forced to exclude results for specific reasons such as motion infarcts in HRpQCT-scans. In those instances, we match two controls for one FHH but still according to the matching criteria.
All participants gave verbal and written informed consent. We asked participants to fill in a questionnaire concerning their state of health. Variables covered by the questionnaire are shown in Table 1. We assessed daily total calcium intake according to reported dietary intakes of milk, cheese, milk products, and use of calcium supplements [19]. We measured height and body weight in light indoor clothing using the same equipment for each participant (Seca, Sa-med, Kvistgaard, Denmark). We conducted the study according to the Declaration of Helsinki II. The study was approved by The Central Denmark Region Committees on Health Research Ethics (#M-2010-0296) and notified to The Danish Data Protection Agency (#2011-41-5733).
Biochemistry
Blood samples were collected in the morning after an overnight fast and following 1 h of bed-rest. In addition, participants collected a 24-h urine sample. Samples were analyzed or stored at −80° C until analysis. We measured plasma and urinary levels of calcium, creatinine, phosphate, magnesium, and albumin by standard laboratory methods using Roche/Hitachi Cobas c-systems (Cobas c 501). To reduce analytical variation, we analyzed plasma levels of PTH and 25-hydroxyvitamin D (25OHD) from patients and controls in a single batch. Plasma total calcium (P-Ca) was corrected for individual variations in plasma albumin according to the equation: adjusted P-Ca (mmol/l) = 1.14 × (0.700 – plasma albumin (mmol/l)) + P-Ca (mmol/l) [20]. Plasma 25OHD was analyzed by isotope dilution liquid chromatography-tandem mass spectrometry (LC-MS/MC) [21]. This method quantifies both 25(OH)-D2 and 25(OH)-D3. Calibrators traceable to NIST SRM 972 (Chromsystems, Münich, Germany) were used. Coefficients of Variance (CV) values (%) for 25(OH)D3 were 6.4 and 9.1 % at levels of 66.5 and 21.1 nmol/L, respectively, and for 25(OH)D2, the CV values were 8.8 and 9.4 % at levels of 41.2 and 25.3 nmol/L, respectively. We measured plasma intact PTH by a 2o-generation assay using Cobas e601 immunoassay analyzers (Roche Diagnostics, Basel, Switzerland). The lower limit of detection of the assay is 0.127 pmol/L, with a total imprecision (CV, %) of 3.3 and 2.7 % at PTH levels of 3.7 and 26.6 pmol/L, respectively.
Genetics
FHH patients were characterized by molecular genetic analysis of the CASR gene as previously described [18, 22]. Sequences were aligned to GenBank reference sequence NM_000388.2. Findings were confirmed in the second analysis on separately drawn blood. The nomenclature of the sequence variants follows the current guidelines [23].
DXA
We performed Dual-energy X-ray Absorptiometry (DXA) using a Hologic Discovery scanner (Hologic, Inc., Waltham MA, USA) assessing areal BMD (aBMD) at the lumbar spine (L1–L4), the total hip, the forearm, and whole body. The coefficient of variation (CV %) was 1.5 % for the lumbar spine, 2.1 % for the femoral neck, and for the ultradistal radius 1.9 % [24].
QCT
Bone volume and density were measured by a quantitative computed tomography (QCT) scan performed at the lumbar spine (L1 to L2) and hip. The scans were performed using a spiral CT scanner (Philips Brilliance 40 multidetector helical CT scanner, Phillips, Eindhoven, Netherlands). Scans were performed using a dose modulation tool (Z-DOM, Phillips) at voltage 120 kV with an effective radiation dose of approximately 0.6 to 1 milli Sievert (mSv) for the lumbar spine and 1.8–2.3 mSv for the hip. Rotation time was 1 second at the spine and 0.5 s at the hip. Field of view was 400 mm, and collimation was 64 × 0.625. Thickness and spacing of slices were both 3 mm. We determined volumetric bone mineral density (vBMD) at the lumbar spine (L1 to L2) and at the hip analyzing data with QCT PRO 3D Volumetric Spine and Hip BMD CTXA System using Bone Investigational Tool (BIT)-kit (Mindways Software Inc, Austin, Texas, USA) compared to a solid state CT calibration phantom (Model 3, Mindways Software) which was scanned together with the participants. Size and position were determined by software algorithms except scans with inaccurate positioning in which manual handling was performed [25].
HR-pQCT
We assessed volumetric BMD (vBMD) and bone geometry using a high-resolution peripheral quantitative computed tomography (HR-pQCT) scanner (Scanco Medical AG, Bruüttisellen, Switzerland). The scans were performed at the nondominant forearm (distal radius) and the ipsilateral distal tibia. If a participant had a previous fracture corresponding to the nondominant side, we performed the scans on the opposite side. Scans were conducted as manufacturer’s default protocol for in vivo imaging implying 110 slices with an isotropic resolution of 82 μm beginning 9.5 mm and 22.5 mm from the endplate at the distal radius and distal tibia, respectively. Scans were performed in proximal direction ending with a 9.02 mm axial 3D representation of the bone. The quality of all scans was inspected visually by two independent investigators (NFBJ and LRe). Scans with severe or extreme motion artifacts were excluded [26, 27]. The analyses consisted of segmentation in cortical and trabecular regions [28, 29]. In a few scans, it was necessary to correct manually. Architectural parameters (Cortical Thickness (Ct.Th [mm]), Trabecular Thickness (Tb.Th [mm]) Number of Trabeculae (Tb.N [mm−1]), Trabecular separation (Tb.Sp [mm]), Trabecular Bone Volume fraction (Tb BV/TV [%]), and Standard Deviation of Trabecular Number (Tb.N.SD [mm]) were assessed with an automated segmentation algorithm based on a dual threshold method [30–33]. Bone strength in terms of bone Stiffness [kN/mm] and Failure load [N] was analyzed using a finite element analysis (FEA) [34]. In brief, voxels representing bone were converted into equally-sized eight-node brick elements resulting in models with approximately 2 and 5 million elements for radius and tibia models, respectively. All bone materials were given a Young’s modulus of 10 GPa and a Poisson’s ratio of 0.3. Boundary conditions represent a high friction compression test. From the models, estimated stiffness was calculated along with an estimate of failure load, based on the assumption that bone failure occurs if >2 % of the elements are strained beyond 0.7 % strain. Model solving was performed with Scanco FEA software v1.15 using unmatched images.
Statistically Approaches
We assessed differences between groups using χ 2 test for categorical variables and a two-sample t test or Mann-Whitney U test for continuous variables, as appropriate after testing for normal distributions. General linear regression model was used to adjust for differences between groups. Correlations between variables were tested by bivariate correlation analysis (Pearson’s or Spearman’s correlation coefficients, as appropriate) and by multiple linear regression analysis calculating partial correlation coefficients (r p). Results are reported as mean ± SD or as median with interquartile range (25 and 75 % percentiles) as appropriate according to the distribution of data. A p value <0.05 was considered statistically significant. Statistical analyses were performed using the Statistical Package for Social Sciences (SPSS 20.0) for Windows (IBM, Armonk, NY, USA).
Results
Characteristics and Biochemistry
Characteristics of the FHH patients and their matched controls are shown in Table 1. Our participants had a mean age of 56 years. Sixty-nine percent was females. The groups did not differ in height (p = 0.43), weight (p = 0.66), or BMI (p = 0.84). Use of calcium supplement was borderline significantly more common among controls than in the FHH group (p = 0.09), but total intake of calcium did not differ between groups (Table 1).
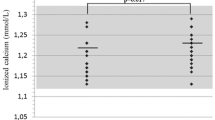
Compared with the controls, patients with FHH had significant higher plasma levels of calcium, magnesium, and PTH, whereas calcium/creatinine clearance ratio (CCCL) and plasma phosphate levels were lower (Table 2). Hypophosphatemia was more frequent in FHH males (n = 7 [44 %]) than control male (n = 1 [6 %]; p = 0.04) but not in female (Table 2). Renal tubular maximum reabsorption rate of phosphate to glomerular filtration rate (TmP/GRF) was lower in FHH subjects (p < 0.001). Plasma 25OHD levels did not differ between groups (Table 2).
Areal Bone Mineral Density (aBMD) and Body Composition by DXA Scanning (Table 3)
Comparing the FHH group with the controls, aBMD and body composition did not differ between groups. Exclusion of participants on treatment with anti-osteoporotic drugs (n = 4 in both groups) did not change results. Neither did stratification by gender reveal significant differences between group, although aBMD at the trochanter was borderline significantly higher in FHH females (0.681 ± 0.099 g/cm2) compared with their controls (0.635 ± 0.102 g/cm2; p = 0.07). After excluding female who used anti-osteoporotic drugs, the difference became statistical significant (0.690 ± 0.095 g/cm2 vs. 0.639 ± 0.104 g/cm2, p < 0.05). Bone area as assessed by DXA did not differ between groups although there was a tendency towards a smaller bone area in trochanter and radius in FHH patients (data not shown). Stratification by gender revealed that FHH females had a significantly smaller bone area at the trochanter (11.0 ± 0.9 cm2 vs. 11.5 ± 1.3 cm2, p = 0.04).
Within the entire group of participants, plasma ionized calcium (P-Ca2+) levels were correlated with aBMD at the total hip (r = 0.206, p = 0.04) and at the trochanteric region (r = 0.299, p < 0.01). This was not changed by adjusting for P-PTH, 25OHD, BMI, gender, and age (data not shown). Plasma PTH was correlated with aBMD at the trochanteric region (r = 0.234, p = 0.02). However, after adjustments for P-Ca2+, 25OHD, BMI, gender, and age, this was no longer significant (p = 0.74).
Hip and Spine Volumetric BMD (vBMD) by QCT Scanning (Table 4)
Analyses at the entire group showed only minor differences between group except that FHH patients had a significantly higher trabecular vBMD (p < 0.01) and a lower trabecular bone volume (p = 0.03) at the total hip. Stratification by gender showed no differences between FHH males and their matched controls, whereas FHH females differed significantly from their controls in a large number of measurements. Accordingly, FHH females had a significantly higher vBMD with a lower bone volume at the total hip (Table 4) as well as at the different sub-regions of the hip (data not shown). Stratification by bone compartments showed a significantly lower cortical vBMD, whereas trabecular vBMD was significantly higher at the hip in females with FHH compared with the controls. Cortical bone volume did not differ between groups, but trabecular bone volume was lower in FHH females. Stratification by menopausal status showed a similar pattern in both pre- and postmenopausal females (data not shown). The results were unchanged after excluding those who were on treatment with anti-osteoporotic drugs.
Significant correlations between P-Ca2+ and vBMD were found at the total hip (r = 0.259, p = 0.02), the trochanteric (r = 0.324, p < 0.01), and at the intertrochanteric region (r = 0.217, p < 0.05), but not at the femoral neck (r = 0.164, p = 0.14), or at the lumbar spine (r = 0.86, p = 0.43). After adjusting for P-PTH, 25OHD, BMI, gender, and age, the association was only significant at the trochanteric region (r p = 0.242, p = 0.04). P-PTH was correlated with vBMD at the trochanteric region (r = 0.242, p = 0.03). However, after adjusting for P-Ca2+, 25OHD, BMI, gender, and age, the association was no longer significant (r p = 0.033, p = 0.78).
Tibia and Radius Structural Analysis by HR-pQCT (Table 5)
Due to motion artifacts causing poor quality, 13 scans (11 FHH patients) of the radius and two scans of tibia (one FHH) were excluded. One control was excluded due to a cyst in the scanned field. After those exclusions, it was not possible to match all participants leaving two (one FHH) not included in analysis.
At the distal tibia, both the total area and the trabecular area were reduced in FHH compared with controls (p = 0.03). The difference was only significant in females, although a similar tendency was present in males. Tb.Th was higher in the FHH group (p = 0.04), but other variables of volumetric density and indices of bone geometry did not differ significantly between groups. If patients receiving anti-osteoporotic drugs were excluded from analyses, Tb.Th no longer differed significantly between groups (p = 0.08), whereas other results were unchanged (data not shown).
At the distal radius, vBMD was higher in FHH subjects in trabecular bone (p = 0.04) and at the transition zone between cortical and trabecular bone (meta-trabecular bone) (p = 0.01). Analysis of microarchitecture showed that FHH subjects had increased Tb.Th (p = 0.03) and Tb BV/TV (p = 0.04). After exclusion of patients receiving anti-osteoporotic drugs, the differences in trabecular vBMD and Tb BV/TV no longer reached statistical significance (p = 0.06) (data not shown). Stratification by gender showed that FHH male had increased Tb.Th (p = 0.03), and FHH female had higher vBMD at meta-trabecular bone (p = 0.02). Furthermore, similar to the findings at the tibia, both total area and trabecular area at the radius tended to be lower in the FHH group compared with controls although only statistical significant in females (p = 0.04). Those results were unchanged after exclusion of patients receiving anti-osteoporotic drugs except that average vBMD at the distal radius in FHH female was higher (p < 0.05) (data not shown). There were no differences between males regarding bone area or vBMD.
Estimated bone strength in terms of stiffness and failure load did not differ significantly either at the radius or the tibia.
In radius, P-Ca2+ levels were correlated significantly with meta-trabecular vBMD (r = 0,236, p = 0.04) and borderline with trabecular vBMD (r = 0,192, p = 0.09). This was not changed by adjusting for P-PTH, 25OHD, BMI, gender, and age (r p = 0.256, p < 0.03) (r p = 0,226, p = 0.05), respectively. However, there were no significant correlations with P-PTH. In tibia, no significant correlations were found either with P-Ca2+ or P-PTH.
Discussion
In accordance with the previous studies, aBMD as assessed by DXA did not differ between FHH patients and their matched controls, except a higher aBMD at the trochanteric region in female with FHH [9, 11]. Moreover, 3-dimensional scanning techniques revealed distinct characteristics in female patients with FHH, including a smaller hip bone volume as assessed by QCT scans and a smaller cross-sectional bone area as assessed by HR-pQCT scans. At the hip, the total vBMD was higher in FHH females compared with controls, which was attributable to a higher trabecular vBMD, whereas cortical vBMD tended to be lower. No differences were encountered between males with FHH and their matched controls.
The findings of higher vBMD at trabecular bone and at the transition zone between cortical and trabecular bone in the distal radius may point towards an explanation of the findings at the hip. QCT scans of the hip are performed at a lower resolution than HR-pQCT scans, and the separation between cortical and trabecular bone is based on a threshold value differentiating the two bone compartments from one another. Due to a higher density of trabecular bone, the transition zone between cortical and trabecular bone may be calculated as cortical bone when measurements are performed by QCT scans. Accordingly, our results do not necessarily imply altered bone geometry in terms of an altered relative distribution of cortical and trabecular bone in females with FHH.
Since FHH is a life-long condition, our findings of a smaller bone area, smaller trabecular bone volume, without differences in cortical bone volume may be a result of changed bone remodeling due to impaired periosteal apposition with reduced trabecularization of cortical bone and reduced endocortical expansion [35]. In this situation, the result will be smaller bone area and smaller trabecular area as we found.
Alternatively, our findings may be explained by a corticalization of trabecular bone, i.e., that the trabecular bone close to cortical bone is apportioned as cortical bone when analyzing the QCT scans. This may also explain our findings of a lower cortical density in female with FHH. Although the trabecular bone accounted for as cortical bone is relatively dense, it is less dense than the rest of the cortical compartment, and cortical bone density may on averages seems to be decreased. Nevertheless, an alternative explanation for the lower cortical density in FHH females is their increased PTH levels, as PTH is known to increase cortical porosity [36]. Our data do not exclude such physiological effects of PTH of cortical bone in FHH even though the correlations between PTH and bone indices were marginal. Micro-CT scans and histomorphometric analyses of bone biopsies are needed to further improve our understanding of bone indices in patients with FHH.
FHH and PHPT have biochemical similarities in terms of hypercalcemia and elevated PTH levels. PHPT is associated with deleterious effects on bone. In addition to a decreased aBMD, HR-pQCT scans of patients with PHPT have shown altered bone geometry in trabecular and cortical bone at the radius [16]. In PHPT, cortical area and thickness are reduced along with a reduced volumetric density. Moreover, trabecular density and number are reduced, whereas trabecular spacing is increased. In contrast, we found higher Tb.Th and higher trabecular vBMD in the distal radius in FHH patients compared to matched healthy controls. This may point towards a physiological effect of the CaSR on bone. In FHH, the relative insensitivity of the CaSR to P-Ca2+ levels may prevent potential harmful effects on bone of hyperparathyroid hypercalcemia. In multiple regression analyses, we studied whether P-Ca2+ correlated to vBMD, as P-Ca2+ was considered as a proxy for the insensitivity of the CaSR to calcium levels. We found that positive correlations between P-Ca2+ and vBMD suggesting an inverse association between the sensitivity of the CaSR and bone density. However, both osteoblasts and osteoclasts express the CaSR [37]. Hence, inactivating variants in the CASR may affect bone remodeling and bone growth per se, independent of concomitant changes P-PTH.
The CaSR is expressed by the long bone’s growth plate, and the CaSR has been shown to be involved in the growth of bone. CASR knockout mice have been shown to exhibit growth retardation, whereas activation of CaSR in the growth plate accelerates bone growth [38, 39]. Our findings of a smaller bone volume at the hip as well as a smaller bone area at the distal extremities support the interaction of the CaSR on bone growth. It may be of interest to investigate whether bone volume is increased in patients with a CASR activating mutation.
Similarly to the state of FHH, the calcium “set-point” may be increased by treatment with lithium, causing a state of mild hyperparathyroid hypercalcemia with a reduced renal calcium excretion [40]. Apparently, lithium acts as calcilytic drug rendering the CaSR to be less sensitive to calcium concentrations, i.e., an effect similar to the state of FHH [41]. In contrast to patients with hyperparathyroid hypercalcemia due to PHPT, lithium therapy does not seem to compromise bone health, as an increased aBMD and a decreased risk of fractures have been reported in patients on treatment with lithium [42, 43]. Interestingly, in a cross-sectional study, comparing patients on treatment with lithium with matched controls, an increased aBMD was found only in females but not in males [42]. In this study, female on treatment with lithium had higher estradiol levels compared with their matched controls. Moreover, lithium was shown to cause hyperestrogenism in female rats, whereas androgen levels were decreased in male rats [44]. In our study, alterations in bone density and geometry were more pronounced in females than males. The CaSR is widely expressed by different tissues, including ovary cells, suggesting that the CaSR protein may affect secretion and function of sex hormones [45]. Experiments performed in the MCF-7 breast cancer cell line indicate that CaSR has a modulating effect of the estrogen receptor alpha [46, 47]. Further studies should aim to determine whether FHH is associated with alteration in the levels of sex hormones and potential interactions between sex hormones and CASR variants.
Our findings of lower plasma phosphate levels in FHH patients compared with their matched controls are in agreement with the well-known effect of CaSR on renal phosphate handling [48]. In the proximal tubule, the CaSR is known to inhibit PTH stimulated phosphate reabsorption, and FHH is accordingly associated with lower plasma levels of phosphate.
Strengths and Limitations to Study
The strength of the present study is the uniform program applied to all participants. Furthermore, the participants are well-matched regarding gender, age, and ethnicity. A further strength is that our controls were recruited randomly from the general background population. In most circumstances, patient and controls were investigated within 3 weeks avoiding seasonal variations in 25-OHD. All investigations were carried out by trained personnel.
Regarding FHH patients, all except one had genetically verified variants in the CASR gene explaining their hypercalcemia. The controls may contribute some uncertainty because recruitment of volunteer causes selection bias. In our population, few were on treatment with anti-osteoporotic drugs, but excluding those did not alter our findings to any major degree. Some of our results showed only borderline significant differences. We are not able to determine whether this is due to lack of statistical power due to a relatively small sample size or should be interpreted in terms of a lack of physiological effects of the inactivating mutation on measured indices. Moreover, we cannot exclude that some borderline p values might have occur by chance due to numerous tests performed. However, it has to be acknowledged that FHH is a rare condition. Accordingly, an appropriate sample size for all measured indices is difficult to obtain. Our cohort of FHH patients is probably one of the largest available, but further studies in similar cohorts are warranted in order to substantiate our findings. Unfortunately, we did not measure estrogen- and androgen-status or biochemical markers of bone turnover, and our study does, therefore, not allow for conclusions on effects of FHH on bone turnover or potential interactions between levels of sex hormones and mutations in the CaSR.
Conclusion
In conclusion, our data showed discrete effects of an inactivating mutation in the CASR gene in female FHH subjects in terms of a smaller bone volume with an increased trabecular bone density at the hip and at the distal radius. Differences were not present in males, suggesting an interaction between sex hormones and the activity of the CaSR on bone. Finite element analyses did not show changes in estimated bone strength. Overall, our findings support that bone health does not seem to be impaired in patients with FHH.
References
Ward BK, Magno AL, Walsh JP, Ratajczak T (2012) The role of the calcium-sensing receptor in human disease. Clin Biochem 45(12):943–953
Nesbit MA, Hannan FM, Howles SA, Reed AA, Cranston T, Thakker CE, Gregory L, Rimmer AJ, Rust N, Graham U, Morrison PJ, Hunter SJ, Whyte MP, McVean G, Buck D, Thakker RV (2013) Mutations in AP2S1 cause familial hypocalciuric hypercalcemia type 3. Nat Genet 45:93–97
Nesbit MA, Hannan FM, Howles SA, Babinsky VN, Head RA, Cranston T, Rust N, Hobbs MR, Heath H 3rd, Thakker RV (2013) Mutations affecting G-protein subunit alpha11 in hypercalcemia and hypocalcemia. N Engl J Med 368:2476–2478
Christensen SE, Nissen PH, Vestergaard P, Mosekilde L (2011) Familial hypocalciuric hypercalcaemia: a review. Curr Opin Endocrinol Diabete Obes 18:359–370
Jakobsen NF, Rolighed L, Nissen PH, Mosekilde L, Rejnmark L (2013) Muscle function and quality of life is not impaired in familial hypocalciuric hypercalcemia (FHH): a cross-sectional study on physiological effects of inactivating variants in the calcium sensing receptor gene (CaSR). Eur J Endocrinol 169(3):349–357
Chang W, Tu C, Chen TH, Bikle D, Shoback D (2008) The extracellular calcium-sensing receptor (CaSR) is a critical modulator of skeletal development. Sci Signal 1:ra1
Law WM Jr, Wahner HW, Heath H 3rd (1984) Bone mineral density and skeletal fractures in familial benign hypercalcemia (hypocalciuric hypercalcemia). Mayo Clin Proc 59:811–815
Kristiansen JH, Rodbro P, Christiansen C, Johansen J, Jensen JT (1987) Familial hypocalciuric hypercalcaemia. III: bone mineral metabolism. Clin Endocrinol (Oxf) 26:713–716
Abugassa S, Nordenstrom J, Jarhult J (1992) Bone mineral density in patients with familial hypocalciuric hypercalcaemia (FHH). Eur J Surg 158:397–402
Menko FH, Bijvoet OL, Fronen JL, Sandler LM, Adami S, O’Riordan JL, Schopman W, Heynen G (1983) Familial benign hypercalcaemia. Study of a large family. Q J Med 52:120–124
Christensen SE, Nissen PH, Vestergaard P, Heickendorff L, Rejnmark L, Brixen K, Mosekilde L (2009) Skeletal consequences of familial hypocalciuric hypercalcaemia versus primary hyperparathyroidism. Clin Endocrinol (Oxf) 71:798–807
Theman TA, Collins MT, Dempster DW, Zhou H, Reynolds JC, Brahim JS, Roschger P, Klaushofer K, Winer KK (2009) PTH(1-34) replacement therapy in a child with hypoparathyroidism caused by a sporadic calcium receptor mutation. J Bone Miner Res 24:964–973
Richards JB, Kavvoura FK, Rivadeneira F, Styrkarsdottir U, Estrada K, Halldorsson BV, Hsu YH, Zillikens MC, Wilson SG, Mullin BH, Amin N, Aulchenko YS, Cupples LA, Deloukas P, Demissie S, Hofman A, Kong A, Karasik D, van Meurs JB, Oostra BA, Pols HA, Sigurdsson G, Thorsteinsdottir U, Soranzo N, Williams FM, Zhou Y, Ralston SH, Thorleifsson G, van Duijn CM, Kiel DP, Stefansson K, Uitterlinden AG, Ioannidis JP, Spector TD, Genetic Factors for Osteoporosis Consortium (2009) Collaborative meta-analysis: associations of 150 candidate genes with osteoporosis and osteoporotic fracture. Ann Intern Med 151:528–537
Christensen SE, Nissen PH, Vestergaard P, Heickendorff L, Brixen K, Mosekilde L (2008) Discriminative power of three indices of renal calcium excretion for the distinction between familial hypocalciuric hypercalcaemia and primary hyperparathyroidism: a follow-up study on methods. Clin Endocrinol (Oxf) 69:713–720
Isaksen T, Nielsen CS, Christensen SE, Nissen PH, Heickendorff L, Mosekilde L (2011) Forearm bone mineral density in familial hypocalciuric hypercalcemia and primary hyperparathyroidism: a comparative study. Calcif Tissue Int 89:285–294
Hansen S, Beck Jensen JE, Rasmussen L, Hauge EM, Brixen K (2010) Effects on bone geometry, density, and microarchitecture in the distal radius but not the tibia in women with primary hyperparathyroidism: a case-control study using HR-pQCT. J Bone Miner Res 25:1941–1947
Harding B, Curley AJ, Hannan FM, Christie PT, Bowl MR, Turner JJ, Barber M, Gillham-Nasenya I, Hampson G, Spector TD, Thakker RV (2006) Functional characterization of calcium sensing receptor polymorphisms and absence of association with indices of calcium homeostasis and bone mineral density. Clin Endocrinol (Oxf) 65:598–605
Nissen PH, Christensen SE, Heickendorff L, Brixen K, Mosekilde L (2007) Molecular genetic analysis of the calcium sensing receptor gene in patients clinically suspected to have familial hypocalciuric hypercalcemia: phenotypic variation and mutation spectrum in a Danish population. J Clin Endocrinol Metab 92:4373–4379
Hermann AP, Thomsen J, Vestergaard P, Mosekilde L, Charles P (1999) Assessment of calcium intake. A quick method comparerd to a 7 days food diary. Calcif Tissue Int 64(suppl 1):S82
Rejnmark L, Vestergaard P, Heickendorff L, Mosekilde L (2011) Determinants of plasma PTH and their implication for defining a reference interval. Clin Endocrinol (Oxf) 74:37–43
Hojskov CS, Heickendorff L, Moller HJ (2010) High-throughput liquid-liquid extraction and LCMSMS assay for determination of circulating 25(OH) vitamin D3 and D2 in the routine clinical laboratory. Clin Chim Acta 411:114–116
Nissen PH, Christensen SE, Ladefoged SA, Brixen K, Heickendorff L, Mosekilde L (2012) Identification of rare and frequent variants of the CASR gene by high-resolution melting. Clin Chim Acta 413:605–611
den Dunnen JT, Antonarakis SE (2001) Nomenclature for the description of human sequence variations. Hum Genet 109:121–124
Abrahamsen B, Gram J, Hansen TB, Beck-Nielsen H (1995) Cross calibration of QDR-2000 and QDR-1000 dual-energy X-ray densitometers for bone mineral and soft-tissue measurements. Bone 16:385–390
Sikjaer T, Rejnmark L, Thomsen JS, Tietze A, Bruel A, Andersen G, Mosekilde L (2012) Changes in 3-dimensional bone structure indices in hypoparathyroid patients treated with PTH(1-84): a randomized controlled study. J Bone Miner Res 27:781–788
Sode M, Burghardt AJ, Pialat JB, Link TM, Majumdar S (2011) Quantitative characterization of subject motion in HR-pQCT images of the distal radius and tibia. Bone 48:1291–1297
Pialat JB, Burghardt AJ, Sode M, Link TM, Majumdar S (2012) Visual grading of motion induced image degradation in high resolution peripheral computed tomography: impact of image quality on measures of bone density and micro-architecture. Bone 50:111–118
Laib A, Hildebrand T, Hauselmann HJ, Ruegsegger P (1997) Ridge number density: a new parameter for in vivo bone structure analysis. Bone 21:541–546
Laib A, Ruegsegger P (1999) Calibration of trabecular bone structure measurements of in vivo three-dimensional peripheral quantitative computed tomography with 28-microm-resolution microcomputed tomography. Bone 24:35–39
Hansen S, Hauge EM, Rasmussen L, Jensen JE, Brixen K (2012) Parathyroidectomy improves bone geometry and microarchitecture in female patients with primary hyperparathyroidism: a one-year prospective controlled study using high-resolution peripheral quantitative computed tomography. J Bone Miner Res 27:1150–1158
Buie HR, Campbell GM, Klinck RJ, MacNeil JA, Boyd SK (2007) Automatic segmentation of cortical and trabecular compartments based on a dual threshold technique for in vivo micro-CT bone analysis. Bone 41:1–505
Nishiyama KK, Macdonald HM, Buie HR, Hanley DA, Boyd SK (2010) Postmenopausal women with osteopenia have higher cortical porosity and thinner cortices at the distal radius and tibia than women with normal aBMD: an in vivo HR-pQCT study. J Bone Miner Res 25:882–890
Burghardt AJ, Kazakia GJ, Ramachandran S, Link TM, Majumdar S (2010) Age- and gender-related differences in the geometric properties and biomechanical significance of intracortical porosity in the distal radius and tibia. J Bone Miner Res 25:983–989
Pistoia W, van Rietbergen B, Lochmuller EM, Lill CA, Eckstein F, Ruegsegger P (2002) Estimation of distal radius failure load with micro-finite element analysis models based on three-dimensional peripheral quantitative computed tomography images. Bone 30:842–848
Seeman E (2003) Periosteal bone formation—a neglected determinant of bone strength. N Engl J Med 349:320–323
Lotinun S, Evans GL, Bronk JT, Bolander ME, Wronski TJ, Ritman EL, Turner RT (2004) Continuous parathyroid hormone induces cortical porosity in the rat: effects on bone turnover and mechanical properties. J Bone Miner Res 19:1165–1171
Marie PJ (2010) The calcium-sensing receptor in bone cells: a potential therapeutic target in osteoporosis. Bone 46:571–576
Wu S, Palese T, Mishra OP, Delivoria-Papadopoulos M, De Luca F (2004) Effects of Ca2+ sensing receptor activation in the growth plate. FASEB J 18:143–145
Brown EM (2013) Role of the calcium-sensing receptor in extracellular calcium homeostasis. Best Pract Res Clin Endocrinol Metab 27:333–334
Broome JT, Solorzano CC (2011) Lithium use and primary hyperparathyroidism. Endocr Pract 17(Suppl 1):31–35
Brown EM (1981) Lithium induces abnormal calcium-regulated PTH release in dispersed bovine parathyroid cells. J Clin Endocrinol Metab 52:1046–1048
Zamani A, Omrani GR, Nasab MM (2009) Lithium’s effect on bone mineral density. Bone 44:331–334
Vestergaard P, Rejnmark L, Mosekilde L (2005) Reduced relative risk of fractures among users of lithium. Calcif Tissue Int 77:1–8
Allagui MS, Hfaiedh N, Croute F, Guermazi F, Vincent C, Soleilhavoup JP, El Feki A (2005) Side effects of low serum lithium concentrations on renal, thyroid, and sexual functions in male and female rats. C R Biol 328:900–911
Hobson SA, McNeil SE, Lee F, Rodland KD (2000) Signal transduction mechanisms linking increased extracellular calcium to proliferation in ovarian surface epithelial cells. Exp Cell Res 258:1–11
Journe F, Dumon JC, Kheddoumi N, Fox J, Laios I, Leclercq G, Body JJ (2004) Extracellular calcium downregulates estrogen receptor alpha and increases its transcriptional activity through calcium-sensing receptor in breast cancer cells. Bone 35:479–488
Leclercq G (2012) Calcium-induced activation of estrogen receptor alpha—new insight. Steroids 77:924–927
Ba J, Brown D, Friedman PA (2003) Calcium-sensing receptor regulation of PTH-inhibitable proximal tubule phosphate transport. Am J Physiol Renal Physiol 285:F1233–F1243
Acknowledgements
This work was supported by a Grant (#10-094047) from The Danish Council for independent Research in Medical Sciences (FSS). The study was conducted at The Osteoporosis Clinic, Aarhus University Hospital, and we hereby thank all the staff for support during the investigations.
Conflict of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Jakobsen, N.F.B., Rolighed, L., Moser, E. et al. Increased Trabecular Volumetric Bone Mass Density in Familial Hypocalciuric Hypercalcemia (FHH) Type 1: A Cross-Sectional Study. Calcif Tissue Int 95, 141–152 (2014). https://doi.org/10.1007/s00223-014-9877-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00223-014-9877-0