
Abstract
The purpose of the present study was twofold. Our first purpose was to test whether joint position sense is similar under instructions to memorize hand position and instructions to memorize shoulder and elbow angles. We hypothesized that instructions to memorize hand position would produce smaller errors due to evidence suggesting that the CNS directly determines hand position but indirectly determines joint angles from proprioceptive information. Our second purpose was to assess biases in joint position sense at various joint angles in a sagittal workspace. We hypothesized that akin to previous single-joint investigations, the shoulder and elbow would demonstrate better joint position sense as joint angles approached 90° during our multi-joint task. Sixteen healthy and right-hand-dominant subjects participated in the present investigation. Subjects were required to actively position their right upper extremity to one of three targets for a memorization period. After returning to the rest position, subjects then actively repositioned back into the target. We did not find evidence of a substantial difference in joint position sense between instructions to memorize the hand position or joint angle. This finding, when considered in conjunction with other evidence, suggests that studies employing either a joint angle protocol or a hand estimation protocol likely produce results that are similar enough to be compared. Proprioception has been shown to be non-uniform across a two-dimensional horizontal workspace. The present investigation provides evidence that proprioception is also non-uniform across a two-dimensional sagittal workspace. Specifically, angular errors decrease as upper extremity joint angles approach 90° of flexion and endpoint errors decrease as targets are located increasingly closer to the head.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Proprioception is the ability to sense both limb position and movement in the absence of vision. Numerous receptors contribute to proprioception including muscle spindles, golgi tendon organs, cutaneous afferents, and joint afferents. The signaling mechanisms behind these receptors are well investigated. Muscle spindles, golgi tendon organs, and cutaneous afferents have been shown to increase their discharge rates in response to muscle lengthening, increased load and stretch, respectively, for a review see Proske and Gandevia (2009). Joint afferents have been shown to differ from other sensory receptors in that their information may only be important when a joint nears the end ranges of motion (Ferrell et al. 1987). Despite a robust breadth of knowledge about proprioception at the receptor level, there is only a modest understanding about how the CNS integrates the signals it receives. Questions such as, ‘how well can the CNS localize its position?’ and ‘what do proprioceptive afferents encode?’ remain challenging to answer.
A number of researchers have suggested that proprioceptive signals are integrated in the CNS to encode joint angles (Soechting 1982; Darling and Gilchrist 1991; Gandevia and Phegan 1999; Gooey et al. 2000). Under this rational, the CNS would need to combine joint angle estimates with information about fixed segment length to determine hand position. This is the same strategy employed in robotics to determine the location of the endpoint effector. An alternative postulate held by other researchers is that proprioceptive signals are integrated to directly encode endpoint position (Wei et al. 1986; van Beers et al. 1998; Fuentes and Bastian 2010) with the CNS bypassing the intermediate step of calculating joint angles. In the case of the upper extremity, the endpoint would be the hand. Although still a debated topic, more evidence points toward an endpoint integration strategy compared to a joint angle integration strategy. A neural network model of the proprioceptive cortex has demonstrated that three-dimensional hand position can be directly determined from muscle spindle afferents (Cho and Reggia 1994), the primary contributors to proprioception (Proske and Gandevia 2009). In this model, the intermediate calculation of joint angles was not required to localize three-dimensional hand position. Recordings from the somatosensory cortex and dorsal spinocerebellar tract suggest that more neurons are tuned to movement direction and endpoint position compared to individual joint angles (Kalaska et al. 1990; Prud’homme and Kalaska 1994; Tillery et al. 1996; Bosco et al. 2000). Furthermore, research by Roll et al. has shown that muscle and cutaneous afferents provide a neuronal population vector that encodes a particular position, suggesting that endpoint position may integrated as early as the peripheral level (Aimonetti et al. 2007).
The output of proprioceptive integration is compartmentalized into the sub-modalities of joint position sense, the ability to identify position of a limb, and kinesthesia, the ability to detect limb movement. Joint position sense can be assessed by either requiring a subject to reproduce the angle made at a specific joint (Soechting 1982; Worringham and Stelmach 1985; Clark et al. 1995; Suprak et al. 2006; Gritsenko et al. 2007) or requiring a subject to reproduce the three-dimensional spatial location of his/her hand (Adamovich et al. 1998; van Beers et al. 1998; Rincon-Gonzalez et al. 2011). While the differences between a protocol utilizing verbal or visual cues to reposition a joint angle versus a protocol utilizing verbal or visual cues to reposition the hand may appear subtle, the data obtained under these differing protocols may not be comparable. If the CNS directly determines endpoint position as more evidence supports, utilizing a hand estimation protocol has an advantage over a joint position protocol. Under a hand estimation protocol, the required task is defined in the same frame of reference as the CNS output. While under a joint angle protocol, the required task is defined in a different frame of reference as the CNS, necessitating a transformation process not present in the hand estimation protocol. For these reasons, researchers have hypothesized that joint position sense under a hand positioning protocol would be better than joint position sense under a joint angle protocol (van Beers et al. 1998; Fuentes and Bastian 2010). Despite the relative ease of presenting the same target under both a hand repositioning and joint repositioning protocol, to our knowledge, only one study has employed such a design (Fuentes and Bastian 2010), finding small but significant improvements under the hand positioning task. Therefore, it remains to be determined whether investigations employing hand repositioning protocols and joint angle protocols produce equivalent results. Currently data obtained under joint repositioning protocols and hand repositioning protocols are assumed to be comparable. If the magnitude of joint position sense errors differs by protocol, it is necessary to consider endpoint perception and joint angle perception as distinct expressions of proprioception.
Since the responses of muscle spindles, golgi tendon organs, cutaneous afferents, and joint afferents vary depending upon stretch and muscle length, it follows that proprioception should vary depending upon joint angles. In a horizontal workspace, a great number of investigations have observed improved proprioception at the midranges of joint motion compared to highly flexed or extended joint angles (Poulton 1979; Dassonville 1995; Wolpert et al. 1995; Lonn et al. 2000; Ariff et al. 2002; Gritsenko et al. 2007; Poulton 2011). Furthermore, Gooey et al. (2000) found that proprioception was best when the arms were positioned in front of the body compared to an abducted position. Proprioceptive differences across joint angles in a sagittal workspace have been less commonly assessed. However, recent investigations suggest that similar to a horizontal workspace, proprioception is best at the midranges of joint motion in sagittal workspace (Suprak et al. 2006, 2007; Chapman et al. 2009; Hung and Darling 2012; King et al. 2013) as well. Specifically, joint position sense at both the shoulder and elbow is best when the shoulder or elbow is positioned at 90° with respect to the distal segment (Suprak et al. 2006, 2007; Chapman et al. 2009; King et al. 2013), with errors increasing linearly as the joint (shoulder/elbow) is positioned further from 90° (Suprak et al. 2006; King et al. 2013). Original theories credited increased muscle activation for the improvements to joint position sense at angles approaching 90°. However, this pattern has been observed despite perturbations to external torque (Suprak et al. 2007) and trunk orientation (Chapman et al. 2009), effectively eliminating muscle activation as the main mechanism. Perhaps neural population vectors are more finally tuned when the hand is in a position corresponding to 90° of shoulder or elbow flexion. One limitation to the aforementioned sagittal workspace investigations is that each employed a single-joint protocol. Therefore, it remains to be determined how joint position sense at the shoulder and elbow behaves across various joint angles during a multi-joint task.
The purpose of the present study was twofold. Our first purpose was to test whether the accuracy and precision of joint position sense are similar under instructions to memorize hand position and instructions to memorize shoulder and elbow angles. Based on the evidence suggesting that the CNS directly integrates proprioceptive information for hand position (Kalaska et al. 1990; Prud’homme and Kalaska 1994; Tillery et al. 1996; Bosco et al. 2000), we hypothesized that instructions to memorize hand position would produce smaller joint position sense errors compared to instructions to memorize joint angles. Our second purpose was to assess biases in joint position sense at various joint angles in a sagittal workspace. Specifically, we wanted to test whether joint position sense at the shoulder and elbow improves as these joints approach 90° of flexion during a multi-joint task. We hypothesized that akin to single-joint tasks (Suprak et al. 2006, 2007; Chapman et al. 2009; King et al. 2013), the shoulder and elbow would demonstrate better joint position sense as joint angles approached 90° of flexion in a multi-joint reaching task.
Methods
Subjects
Sixteen healthy adults (nine females, seven males) with a mean age of 20 ± 3 years, a mean height of 172 ± 12 cm, and a mean body mass of 73 ± 14 kg participated in this study. Prior to testing, all subjects signed an informed consent form approved by the Institutional Review Board. Only right-hand-dominant subjects were included, and dominance was determined by asking subjects which arm they would use to throw a ball. Exclusion criteria included a history of injury to the right shoulder or elbow or participation in a repetitive overhead activity.
Instrumentation
Kinematic data were collected with an electromagnetic tracking system (Fastrak®, Polhemus, Colchester, VT). The unit consists of a transmitter, three receivers, and a digitizer. The first receiver was taped to the border of the left latissimus dorsi and further held in place with the use of an elastic strap and custom orthoplast device. The second receiver was placed on the dorsal side of the right wrist with elastic tape. The third receiver was fastened to the right scapula with a previously validated tracking jig (Karduna et al. 2001). We chose not to affix a humeral receiver due to the potential for large errors associated with skin motion artifact (Lin and Karduna 2013). During the attachment of receivers, digitization, and testing procedures, subjects sat on an ergonomically designed kneeling chair (Better Posture Kneeling Chairs, Jobri®, Konawa, Ok) to control for posture.
Following the attachment of the receivers, anatomical landmarks were digitized in order to establish anatomical coordinate systems for the thorax, humerus, and forearm in accordance with the standards proposed by the International Society of Biomechanics (Wu et al. 2005). The sternal notch, xiphoid process, cervical vertebra seven, and thoracic vertebra eight were used to establish the thoracic coordinate system. The center of the humeral head, elbow joint center, and ulnar styloid process were used to establish the humeral coordinate system. The ulnar styloid process, radial styloid process, and midpoint between the medial and lateral epicondyles were used to establish the forearm coordinate system. The center of the humeral head was defined at the point that moves the least when the shoulder was moved through a series of short arc motions with the elbow in full extension (Karduna et al. 2001). True anatomical rotation at the elbow does not coincide with the midpoint between the medial and lateral epicondyles of the humerus (Veeger et al. 1997). Therefore, we determined the center of the elbow joint using a passive elbow flexion trial that was previously validated (Lin and Karduna 2013).
Kinematic data were represented using standard Euler angle sequences (Wu et al. 2005). For the shoulder, this was (a) plane of elevation, (b) amount of elevation, and (c) external rotation. For the elbow, this was (a) flexion, (b) supination, and (c) carrying angle. However, only the data for shoulder elevation (which we termed shoulder flexion) and elbow flexion were analyzed. The three-dimensional coordinates of the hand (defined by the coordinates of the ulnar styloid process) were determined in relation to the thorax.
Protocol
All testing was performed in a single session. Subjects completed a standardized warm-up on the right limb prior to testing in order to provide a consistent muscle state. The warm-up consisted of ten repetitions of biceps curls, triceps extensions, and Codman’s pendulum exercises (clockwise rotations, counter-clockwise rotations, and sagittal plane motion) while standing and holding a two pound weight. Upon the completion of the warm-up, subjects removed their shirts (females wore sports bras) to minimize tactile cues. Metal objects or jewelry were also removed to avoid interference with the electromagnetic tracking system. After the warm-up, subjects were transferred from a standing position to a seated position in the kneeling chair to attach receivers and digitize bony landmarks (as described above).
After the digitization process, subjects were told that they would be performing a series of reaching movements (with the assistance from a computer program) to targets preselected by the researcher. The subject was then read one of two sets of randomized instructions. Under one set of instructions, subjects were told that after reaching the target, they needed to maintain this posture for 3 s in order to ‘memorize the location of your hand so that you can place your hand in this location again.’ Under the other set of instructions, subjects were told that after reaching the target, they needed to maintain this posture for 3 s in order to ‘memorize the angles made at your shoulder and elbow so that you can recreate these angles again.’ We will call the former set of instructions hand instructions and the later joint angle instructions. After receiving instructions, subjects performed several practice trials (typically 5–7 trials) in order to become acquainted with the protocol. The number of practice trials varied by subject and was determined by the researcher based on the subject’s competency with the protocol. Throughout the practice session, the researcher reread the instructions to the subject. Once the subject displayed competency with the practice trials, the first block of testing began. At the end of the first testing block, subjects were given a 5-min rest period with receivers remaining affixed. After the rest period, subjects were read the second set of instructions and required to perform several practice trials (typically 3–4 trials). Throughout this second practice session, the researcher reread the instructions to the subject. Once the subject verbally indicated they had adjusted to the new set of instructions, the second block of testing began.
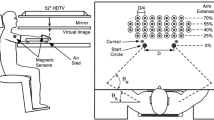
Both practice and test trials consisted of two phases: the positioning phase and repositioning phase. At the beginning of a trial, the subject viewed a blank monitor while the right arm was relaxed at the side with the elbow in extension and the forearm in a neutral pronation/supination position. The positioning phase began when two red bars appeared on the monitor and an automated voice command prompted the subject to ‘find target.’ The subject then made a reaching movement in the sagittal plane requiring both shoulder and elbow flexion. Feedback about the subject’s position relative to the target was provided to the subject via the location of the red bars (see Fig. 1 for greater detail) on the monitor. The subject’s movement and adjustment time typically took 1 to 2 s. When the subject’s shoulder was flexed within 3° of the desired target angle and their elbow was flexed within 3° of the desired target angle, the monitor again became blank. The subject maintained this position for 3 s in order to memorize the target (utilizing one of the two sets of previously mentioned instructions). A 3 s memorization time was chosen in order to be consistent with other joint position sense investigations (Goble and Brown 2008; Anderson and Wee 2011; Hung and Darling 2012; King et al. 2013). Memorization times of 1 (Suprak et al. 2007), 2 (Adamovich et al. 1998; Goble et al. 2012), 4 (Zuckerman et al. 1999), and 5 s (Chapman et al. 2009; Rincon-Gonzalez et al. 2011) have also been used. After the 3 s memorization period, an automated voice command instructed the subject to ‘relax,’ at which time the subject returned the arm to the starting position. In the event the subject did not fully relax their arm into the starting position, the program indicated this with a buzz. After 2 s in the relaxed position and with the monitor remaining blank, the repositioning phase began with an automated voice command instructing the subject to ‘find target.’ The subject (without feedback) repositioned himself into the target and depressed a wireless remote (Libra P5, Ione, Fremont, CA) held in left hand when he believed he had returned to the target presented in the positioning phase. Upon depression of the remote, subjects were prompted to return to the starting position by an automated voice command of ‘relax.’ There was a 5 s rest interval between each trial.

Side view of the positioning phase of a practice trial. Shown is a point in time in which the subject needs to move the hand superior and anterior from its current position (as indicated by the red bars) in order to reach the target. When the target is achieved, the screen becomes blank (color figure online)
Three test targets were used: 45°/45°, 60°/60°, and 75°/75° corresponding to shoulder and elbow flexion angles, respectively. While targets for this study were defined by shoulder and elbow flexion angles, subjects were not given feedback about their joint angles during the positioning phase. Instead subjects received feedback about the anterior–posterior (x) and superior–inferior (y) position of their hand relative to the target (Fig. 1). The translation of angular targets into x and y coordinates was possible due to the fact that the movement was restricted to the sagittal plane, enabling a unique set of x and y coordinates for each angular target.
In order to become familiar with the protocol, subjects viewed an external monitor aligned in the sagittal plane for the first few practice trials. This setup required subjects to rotate their head to the left approximately 45°. After subjects demonstrated proficiency with the protocol using an external monitor, a few more practice trials were performed using a head mounted monitor (Z800, eMagine, Bellevue, WA). It is important to note that the head mounted monitor occluded all external vision and was worn for the duration of testing. The external monitor was only worn for practice trials but did allow subjects to view their upper extremity. Therefore, to control for visual learning, practice targets were different from test targets. The same practice targets were used for all subjects and corresponded to 30°/30°, 30°/90°, 90°/30°, and 90°/90° of shoulder and elbow flexion angles, respectively. During each block of instructions, the three test targets were presented six times, resulting in a total of eighteen test trials per instruction block.
Error score calculations
Accuracy, frequently calculated by constant error, represents an individual’s average directional bias but does not provide information about the consistency of his/her performance. Conversely, precision, frequently calculated by variable error, represents an individual’s consistency during performance but does not provide information about his/her average directional bias. In order to calculate how accurately and precisely the shoulder and elbow joints reproduced the target angles, we used equations proposed by Schmidt and Lee (1999). The following conventions were used: θ i is the angular error in degrees on trial, and n is the number of trials performed.
In order to calculate the repositioning accuracy and precision of the hand, we first calculated the linear error in the anterior–posterior (x) and superior–inferior (y) directions independently. We then combined these one-dimensional error scores to obtain an overall measure of hand accuracy and precision. For hand accuracy, we used a centroid calculation proposed by Hancock et al. (1995), while for hand precision, we used a calculation employed by King et al. (2013). The following conventions were used: n is the number of trials performed, x i is the repositioning error in millimeters in the anterior–posterior direction for trial i, \(\overline{x}\) is the centroid of errors in the anterior–posterior direction, and x p is the precision of repositioning errors in the anterior–posterior direction. The same conventions apply for y (the superior–inferior direction).
Statistical analysis
SPSS version 20.0 (IBM, Chicago IL) was used for statistical analysis. We performed a total of six two-way repeated measures analysis of variance (2 instructions × 3 targets) with shoulder accuracy, shoulder precision, elbow accuracy, elbow precision, endpoint accuracy, and endpoint precision serving as the dependent variables. Family-wise type I error was set to α < 0.05, and pairwise comparisons were made where significant interactions and main effects were found using a Bonferroni correction. We followed conventional analysis of variance logic and did not look at main effects where significant interactions were found. We also performed a series of post hoc dependent t tests at each target to compare endpoint accuracy and precision in the anterior–posterior direction to endpoint accuracy and precision in the superior–inferior direction. For each dependent t test, α was set to <0.05.
Results
Joint accuracy
For shoulder accuracy, there was no significant interaction between instruction and target (p = 0.05), nor was there a main effect of instruction (p = 0.42). The shoulder consistently overshoot each target by ~4° resulting in no significant influence of target on shoulder accuracy (p = 0.61).
For elbow accuracy, there was no significant interaction between instruction and target (p = 0.24), nor was there a main effect of instruction (p = 0.66) (Fig. 2a). Unlike the shoulder, elbow accuracy was found to significantly vary by target (p = 0.01). Pairwise comparisons revealed that errors at 45°/45° (M = 2.3°) were significantly different from errors at 60°/60° (M = −1.2°) and 75°/75° (M = −4.5°) (Fig. 2a).

a Joint accuracy and b endpoint accuracy at the three targets: 45°/45°, 60°/60°, and 75°/75°. Errors were collapsed by instruction, and larger values indicate larger repositioning errors
Hand accuracy
For all targets, subjects generally demonstrated a repositioning bias that was anterior and superior to the presented target (Fig. 3). Furthermore, repositioning accuracy at the hand was significantly better in the anterior–posterior direction compared to the superior–inferior direction at targets 45°/45° (p < 0.01) and 60°/60° (p < 0.01). At target 75°/75°, there was no significant difference (p = 0.20) in the repositioning accuracy of the hand in anterior–posterior and superior–inferior directions.

Scatterplot demonstrating the two-dimensional repositioning errors of every subject at every target. Point (0,0) represents perfect repositioning, while points further from (0, 0) indicate larger errors. Positive x values represent an anterior repositioning (in mm) relative to the target, and positive y values represent a superior repositioning (in mm) relative to the target. Most subjects repositioned their hand anterior and superior to the target
For overall hand accuracy, there was no significant interaction between instruction and target (p = 0.41), nor was there a main effect of instruction (p = 0.23). Target (p = 0.02) did significantly influence hand accuracy, and pairwise comparisons revealed that estimates at 45°/45° (M = 57.9 mm), 60°/60° (M = 45.5 mm), and 75°/75° (M = 33.3 mm) were all significantly different from each other (Fig. 2b).
Joint precision
For shoulder precision, there was no significant interaction between instruction and target (p = 0.08), nor was there a main effect of target (p = 0.48). Instruction (p = 0.01) did significantly influence shoulder precision, and errors under endpoint instruction (M = 3.1°) were smaller than errors under joint angle instruction (M = 3.6°) (Fig. 4a).

a Joint precision and b endpoint precision collapsed across target and instruction. Larger values indicate larger repositioning errors
For elbow precision, there was a significant interaction between instruction and target (p = 0.03); however, pairwise comparisons failed to reveal any differences.
Hand precision
Repositioning precision at the hand was significantly better in the anterior–posterior direction compared to the superior–inferior direction for targets 45°/45° (p < 0.01), 60°/60° (p < 0.01), and 75°/75° (p < 0.01).
For overall hand precision, there was no significant interaction between instruction and target (p = 0.38), nor was there a main effect of target (p = 0.42). A main effect of instruction was found for overall hand precision (p = 0.01), with smaller errors under endpoint instruction (M = 29.3 mm) than joint angle instruction (M = 33.1 mm) (Fig. 4b).
Discussion
Estimation errors across instructions
The first aim of the present study was to test our hypothesis that instructions to memorize hand position would produce smaller joint position sense errors than instructions to memorize joint angles. Contrary to our hypothesis, accuracy at the shoulder, elbow and hand were unaffected by type of instruction in the present study. However, the present study did find that hand positioning instructions produced small (~0.5°) but statistically significant improvements in precision at the shoulder. This in turn led to small (~3.8 mm) but statistically significant improvements in endpoint precision under hand positioning instructions. The results of the present study are similar to those obtained by Fuentes and Bastian (2010) during a single-joint elbow task. Like the present study, subjects displayed small improvements in joint angle precision (~1.4°) but not accuracy when estimating the location of their hand instead of their elbow angle. Although both the current study and the study by Fuentes and Bastian (2010) found precision to be significantly better during a hand positioning task versus a joint angle task, the observed benefit (0.5°–1.4°) is probably too small to be of importance.
To our knowledge, the present study and the study by Fuentes and Bastian (2010) are the only studies that have directly compared joint position sense under a hand repositioning protocol to joint position sense under a joint repositioning protocol. While the present study used verbal instructions to prompt subjects to reproduce hand position or joint angle, Fuentes and Bastian (2010) used visual prompts. Specifically, subjects encountered an interface that required them to either rotate an electronically projected line over their forearm or move an electronically projected cursor over their finger. Taken together, these two studies help to clarify that both verbal and visual cues to reproduce hand position versus joint angle seem to have no influence over joint position sense. This suggests that investigations utilizing either a hand estimation or joint estimation protocol produce results that are similar enough to be compared.
Some researchers have hypothesized that if proprioceptive input is directly integrated for endpoint position, then joint position sense under a hand positioning protocol should be better than joint position sense under a joint angle protocol (van Beers et al. 1998; Fuentes and Bastian 2010). While results of the present study as well as the study by Fuentes and Bastian (2010) do not support the aforementioned hypothesis, the lack of differences found between the two protocols could indicate that subjects are generally employing an endpoint strategy. An endpoint strategy could easily be adopted despite verbal cues to memorize joint angels by focusing on hand position, and an endpoint strategy could easily be adopted despite visual cues to align a cursor over a body segment by aligning the tip of the cursor over the hand. In everyday life, it is rarely meaningful to estimate joint angles since successful interactions with the environment require efficient hand estimation. Therefore, it may be impossible to manipulate a subconscious endpoint strategy into a joint angle strategy through verbal or visual cues.
Estimation errors across targets
The second aim of the present study was to test our hypothesis that joint position sense at the shoulder and elbow joints would become better as targets approached 90° of flexion. Contrary to our hypothesis, accuracy at the shoulder was unaffected by joint angle with the shoulder consistently overshooting each target by ~4°. Accuracy at the elbow was also found to be contrary to our hypothesis. Unlike the shoulder, joint position sense at the elbow was influenced by joint angle. However, the elbow was most accurate at the 60°/60° target not the predicted 75°/75° target (Fig. 4a). Surprisingly, endpoint accuracy matched our hypothesis with smaller errors at the hand as targets required increased flexion (Fig. 4b). This trend can be explained by better counterbalancing of errors between shoulder and elbow joints as targets approached 90°. At the 45°/45° target, both the shoulder and elbow overshot the target, while at the 75°/75° target, the shoulder overshoot the target and the elbow undershoot the target, resulting in errors that compensated for each other.
The results of the present study demonstrate that the accuracy of joint position sense is not stable across a two-dimensional sagittal workspace. Specifically, endpoint estimation errors decrease as targets are located increasingly closer to the head. This finding compliments previous findings about estimation errors across a two-dimensional horizontal workspace, with smaller errors occurring at targets located closer to the shoulder (Tillery et al. 1994; van Beers et al. 1998, 2002; Graziano et al. 2004; Fuentes and Bastian 2010; Wilson et al. 2010; Rincon-Gonzalez et al. 2011). In a horizontal workspace, subjects demonstrate a consistent bias with lateral overestimates to medial targets and medial overestimates to lateral targets (Poulton 1979; Sanes 1986; Dassonville 1995; Wolpert et al. 1995; Lonn et al. 2000; Ariff et al. 2002; Graziano et al. 2004; Gritsenko et al. 2007; Poulton 2011). This trend has been has explained as a ‘range effect,’ where a subject’s errors are biased in the direction of the middle target (Poulton 1979; Poulton 2011). Under the ‘range effect’ theory, a subject would be expected to be best at a 40° target, overshoot a 30° target, and undershoot a 50° target (assuming 30°, 40°, and 50° are the only targets being presented). However, a recent reaching study by Gritsenko et al. (2007) found that estimation errors are best and biased toward the midline of the body even when targets are presented in groups exclusively in medial or lateral positions. This finding refutes the ‘range effect’ theory, and Gritsenko et al. (2007) propose that the bias toward the midline of the body may be due to the CNS employing a Bayesian inference process. Bayesian networks are often employed in machine learning since the output variable is estimated by combining current observations with prior experience. In terms of the CNS, this would mean that estimates of hand position are obtained by combining current proprioceptive signals with prior proprioceptive experiences accumulated over a lifetime of arm movements. Therefore, if the CNS is utilizing Bayesian processing, estimates of hand position should be biased toward those positions that have frequently been used during the lifetime.
In non-human primates, Graziano et al. (2002) found that stimulation of approximately 50 % of the neurons in the precentral gyrus resulted in hand placement in a region located in front of the chest and mouth. Interestingly, in a follow-up study on spontaneous behavior, Graziano et al. (2004) observed that a non-human primate hand spends approximately 50 % of its time performing tasks near the chest and mouth. Thus, if the proprioceptive system of non-human primates utilizes Bayesian inference, a repositioning bias for the mouth and chest would be expected. In the present study, subjects demonstrated a superior repositioning bias to all targets with the magnitude of this bias decreasing as targets required greater joint flexion. Using calibration data and anthropometric tables provided by Winter (2009), we determined that targets 45°/45°, 60°/60°, and 75°/75° were located at the same superior–inferior position as the xiphoid process, jugular notch, and chin, respectively. Together, the large superior bias found when the hand was near the xiphoid process, moderate superior bias when the hand was near the jugular notch, and small superior bias when the hand was near the chin suggest that subjects were biased toward the head. Based on the previously mentioned research by Graziano et al. (2002, 2004), the bias found in the present study is similar to the bias that would be expected in non-human primates utilizing Bayesian inference. A limitation to the current study is that none of our targets were located superior to the mouth. An inferior bias to targets located superior to the mouth would provide more evidence for the human CNS employing a Bayesian inference process. Another limitation to the current study is that target 60°/60° was located near the jugular notch, while target 75°/75° was located near the chin. Both of these targets fall into the region most non-human primate hands spend their time performing tasks in Graziano et al. (2002, 2004).
The present study assessed joint position sense by requiring subjects to memorize and reproduce a target with the same limb. It is important to point out that joint position sense can be measured in a number of other ways, including matching a held position with a pointer or matching a held position with the contralateral limb. Therefore, the superior repositioning bias found in the present study may not be present under another form of measurement. We chose not to use a contralateral matching task since asymmetries in proprioceptive processing are known to exist for the right and left limbs (Adamo and Martin 2009). Therefore, it would have been difficult to determine whether biases across a sagittal workspace were arising from the reference or matching arm. We chose not to use a task requiring the manipulation of a pointer due to the involvement of vision. The integration of proprioceptive and visual information is sensitive to movement direction (van Beers et al. 2002). When movements are made in a superior–inferior direction, visual information is weighted higher than proprioceptive information, and when movements are made in an anterior–posterior direction, proprioceptive information is weighted higher than visual information (van Beers et al. 2002). The present study found that in the absence of vision, repositioning accuracy and precision is worse in the superior–inferior direction compared to the anterior–posterior direction. These findings are in agreement with a study conducted by van Beers et al. (1998) that found repositioning precision to a visually presented target is worse in the superior–inferior direction than in the anterior–posterior direction. The higher weighing of visual information during superior–inferior movements may be due to the poor superior–inferior proprioceptive abilities of CNS observed in the present study and the study by van Beers et al. (1998). In fact, a greater number of somatosensory neurons are tuned to upper extremity movements in the anterior–posterior direction than the vertical direction (Tillery et al. 1996).
Limitations
The volunteer participants in this study were recruited from a university setting and therefore represented a young population (subject age range 18–26 years). Proprioceptive acuity is associated with age (Adamo et al. 2009); therefore, the results obtained from this sample of convenience may not be applicable to an older population. Many activities of daily living require active reaching movements at the upper extremity. For these reasons, the present study employed an active versus passive protocol. Nonetheless, an active protocol allows the CNS to estimate hand position from both peripheral afferent information and efference copy. The relative contribution of efference copy cannot be determined from this study design.
Conclusions
The present study did not find evidence of a substantial difference in joint position sense between instructions to memorize the hand position or joint angle. This finding, when considered in conjunction with other evidence, suggests that studies employing either a joint angle protocol or a hand estimation protocol likely produce results that are similar enough to be compared. Proprioception has been shown to be non-uniform across a two-dimensional horizontal workspace. The present study provides evidence that proprioception is also non-uniform across a two-dimensional sagittal workspace, such that endpoint errors decrease as targets are located increasingly closer to the head.
References
Adamo DE, Martin BJ (2009) Position sense asymmetry. Exp Brain Res 192:87–95. doi:10.1007/s00221-008-1560-0
Adamo DE, Alexander NB, Brown SH (2009) The influence of age and physical activity on upper limb proprioceptive ability. J Aging Phys Act 17:272–293
Adamovich SV, Berkinblit MB, Fookson O, Poizner H (1998) Pointing in 3D space to remembered targets. I. Kinesthetic versus visual target presentation. J Neurophysiol 79:2833–2846
Aimonetti JM, Hospod V, Roll JP, Ribot-Ciscar E (2007) Cutaneous afferents provide a neuronal population vector that encodes the orientation of human ankle movements. J Physiol 580:649–658. doi:jphysiol.2006.123075
Anderson VB, Wee E (2011) Impaired joint proprioception at higher shoulder elevations in chronic rotator cuff pathology. Arch Phys Med Rehabil 92:1146–1151. doi:10.1016/j.apmr.2011.02.004
Ariff G, Donchin O, Nanayakkara T, Shadmehr R (2002) A real-time state predictor in motor control: study of saccadic eye movements during unseen reaching movements. J Neurosci 22:7721–7729. doi:22/17/7721
Bosco G, Poppele RE, Eian J (2000) Reference frames for spinal proprioception: limb endpoint based or joint-level based? J Neurophysiol 83:2931–2945
Chapman J, Suprak DN, Karduna AR (2009) Unconstrained shoulder joint position sense does not change with body orientation. J Orthop Res 27:885–890. doi:10.1002/jor.20813
Cho S, Reggia JA (1994) Map formation in proprioceptive cortex. Int J Neural Syst 5:87–101
Clark FJ, Larwood KJ, Davis ME, Deffenbacher KA (1995) A metric for assessing acuity in positioning joints and limbs. Exp Brain Res 107:73–79
Darling WG, Gilchrist L (1991) Is there a preferred coordinate system for perception of hand orientation in three-dimensional space? Exp Brain Res 85:405–416
Dassonville P (1995) Haptic localization and the internal representation of the hand in space. Exp Brain Res 106:434–448
Ferrell WR, Gandevia SC, McCloskey DI (1987) The role of joint receptors in human kinaesthesia when intramuscular receptors cannot contribute. J Physiol 386:63–71
Fuentes CT, Bastian AJ (2010) Where is your arm? Variations in proprioception across space and tasks. J Neurophysiol 103:164–171. doi:10.1152/jn.0 0494.2009
Gandevia SC, Phegan CM (1999) Perceptual distortions of the human body image produced by local anaesthesia, pain and cutaneous stimulation. J Physiol 514(Pt 2):609–616
Goble DJ, Brown SH (2008) Upper limb asymmetries in the matching of proprioceptive versus visual targets. J Neurophysiol 99:3063–3074. doi:10.1152/jn.90259.2008
Goble DJ, Mousigian MA, Brown SH (2012) Compromised encoding of proprioceptively determined joint angles in older adults: the role of working memory and attentional load. Exp Brain Res 216:35–40. doi:10.1007/s00221-011-2904-8
Gooey K, Bradfield O, Talbot J, Morgan DL, Proske U (2000) Effects of body orientation, load and vibration on sensing position and movement at the human elbow joint. Exp Brain Res 133:340–348
Graziano MS, Taylor CS, Moore T (2002) Complex movements evoked by microstimulation of precentral cortex. Neuron 34:841–851. doi:S0896627302006980
Graziano MS, Cooke DF, Taylor CS, Moore T (2004) Distribution of hand location in monkeys during spontaneous behavior. Exp Brain Res 155:30–36. doi:10.1007/s00221-003-1701-4
Gritsenko V, Krouchev NI, Kalaska JF (2007) Afferent input, efference copy, signal noise, and biases in perception of joint angle during active versus passive elbow movements. J Neurophysiol 98:1140–1154 0162.2007
Hancock GR, Butler MS, Fischman MG (1995) On the problem of two-dimensional error scores: measures and analyses of accuracy, bias, and consistency. J Mot Behav 27:241–250. doi:10.1080/00222895.1995.9941714
Hung YJ, Darling WG (2012) Shoulder position sense during passive matching and active positioning tasks in individuals with anterior shoulder instability. Phys Ther 92:563–573. doi:10.2522/ptj.20110236
Kalaska JF, Cohen DA, Prud’homme M, Hyde ML (1990) Parietal area 5 neuronal activity encodes movement kinematics, not movement dynamics. Exp Brain Res 80:351–364
Karduna AR, McClure PW, Michener LA, Sennett B (2001) Dynamic measurements of three-dimensional scapular kinematics: a validation study. J Biomech Eng 123:184–190
King J, Harding E, Karduna A (2013) The shoulder and elbow joints and right and left sides demonstrate similar joint position sense. J Mot Behav 45:479–486. doi:10.1080/00222895.2013.832136
Lin YL, Karduna AR (2013) Sensors on the humerus are not necessary for an accurate assessment of humeral kinematics in constrained movements. J Appl Biomech 29:496–500
Lonn J, Crenshaw AG, Djupsjobacka M, Pedersen J, Johansson H (2000) Position sense testing: influence of starting position and type of displacement. Arch Phys Med Rehabil 81:592–597. doi:S0003-9993(00)90040-6
Poulton EC (1979) Models for biases in judging sensory magnitude. Psychol Bull 86:777–803
Poulton EC (2011) Human manual control. In: comprehensive physiology. Wiley, Hoboken, NJ
Proske U, Gandevia SC (2009) The kinaesthetic senses. J Physiol 587:4139–4146. doi:10.1113/jphysiol.2009.175372
Prud’homme MJ, Kalaska JF (1994) Proprioceptive activity in primate primary somatosensory cortex during active arm reaching movements. J Neurophysiol 72:2280–2301
Rincon-Gonzalez L, Buneo CA, Tillery SIH (2011) The proprioceptive map of the arm is systematic and stable, but idiosyncratic. PLoS ONE 6:e25214. doi:10.1371/journal.pone.0025214
Sanes JN (1986) Kinematics and end-point control of arm movements are modified by unexpected changes in viscous loading. J Neurosci 6:3120–3127
Schmidt RA, Lee TD (1999) Chapter 2: Methodology for studying motor performance. In: Schmidt RA, Lee TD (eds) Motor control and learning: a behavioral emphasis, 3rd edn. Human Kinetics, Champaign, IL, p xvi, 495
Soechting JF (1982) Does position sense at the elbow reflect a sense of elbow joint angle or one of limb orientation? Brain Res 248:392–395
Suprak DN, Osternig LR, van Donkelaar P, Karduna AR (2006) Shoulder joint position sense improves with elevation angle in a novel, unconstrained task. J Orthop Res 24:559–568. doi:10.1002/jor.20095
Suprak DN, Osternig LR, van Donkelaar P, Karduna AR (2007) Shoulder joint position sense improves with external load. J Mot Behav 39:517–525. doi:10.3200/JMBR.39.6.517-525
Tillery SI, Flanders M, Soechting JF (1994) Errors in kinesthetic transformations for hand apposition. NeuroReport 6:177–181
Tillery SI, Soechting JF, Ebner TJ (1996) Somatosensory cortical activity in relation to arm posture: nonuniform spatial tuning. J Neurophysiol 76:2423–2438
van Beers RJ, Sittig AC, van der Gon JJD (1998) The precision of proprioceptive position sense. Exp Brain Res 122:367–377
van Beers RJ, Wolpert DM, Haggard P (2002) When feeling is more important than seeing in sensorimotor adaptation. Curr Biol 12:834–837
Veeger HE, Yu B, An KN, Rozendal RH (1997) Parameters for modeling the upper extremity. J Biomech 30:647–652. doi:S0021929097000110
Wei JY, Simon J, Randic M, Burgess PR (1986) Joint angle signaling by muscle spindle receptors. Brain Res 370:108–118
Wilson ET, Wong J, Gribble PL (2010) Mapping proprioception across a 2D horizontal workspace. PLoS ONE 5:e11851. doi:10.1371/journal.pone.0011851
Winter DA (2009) Biomechanics and motor control of human movement. Wiley, Hoboken, NJ
Wolpert DM, Ghahramani Z, Jordan MI (1995) An internal model for sensorimotor integration. Science 269:1880–1882
Worringham CJ, Stelmach GE (1985) The contribution of gravitational torques to limb position sense. Exp Brain Res 61:38–42
Wu G, van der Helm FC, Veeger HE et al (2005) ISB recommendation on definitions of joint coordinate systems of various joints for the reporting of human joint motion–Part II: shoulder, elbow, wrist and hand. J Biomech 38:981–992
Zuckerman JD, Gallagher MA, Lehman C, Kraushaar BS, Choueka J (1999) Normal shoulder proprioception and the effect of lidocaine injection. J Shoulder Elbow Surg 8:11–16. doi:S1058-2746(99)90047-2
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
King, J., Karduna, A. Joint position sense during a reaching task improves at targets located closer to the head but is unaffected by instruction. Exp Brain Res 232, 865–874 (2014). https://doi.org/10.1007/s00221-013-3799-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-013-3799-3