
Abstract
This study investigated whether short-term modifications of gait could be induced in healthy adults and whether a combination of kinetic (a compliant force resisting deviation of the foot from the prescribed footpath) and visual guidance was superior to either kinetic guidance or visual guidance alone in producing this modification. Thirty-nine healthy adults, 20–33 years old, were randomly assigned to the three groups receiving six 10-min blocks of treadmill training requiring them to modify their footpath to match a scaled-down path. Changes of the footpath, specific joint events and joint moments were analyzed. Persons receiving combined kinetic and visual guidance showed larger modifications of their gait patterns that were maintained longer, persisting up to 2 h after intervening over-ground activities, than did persons receiving training with primarily kinetic guidance or with visual guidance alone. The results emphasize the short-term plasticity of locomotor circuits and provide a possible basis for persons learning to achieve more functional gait patterns following a stroke or other neurological disorders.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
People with neurologic disorders such as a stroke experience difficulty in walking due to significant neuromuscular impairments. Adaptation of their altered motor patterns is necessary to achieve a semblance of functional walking (Perry 1992). The atypical gait that often results, however, is generally marked by inefficiency and impaired postural stability, making community ambulation difficult if not impossible (Perry et al. 1995). This fact has led to attempts to develop more effective gait re-training programs to encourage more efficient and stable locomotor patterns. Human walking is thought to be more dependent on cortical processes than is the case in lower animals as evidenced, for example, by the fact that walking patterns are more difficult to induce following a complete spinal cord lesion (Dimitrijevic et al. 1998; Fedirchuk et al. 1998). This greater role of cortical and/or subcortical processes in humans provides a possible entrée for improving atypical gait patterns in persons following a stroke. Still, human gait is a relatively automatic process, particularly when walking in familiar and uncluttered environments. Given this fact, it is not surprising that gait re-training programs for stroke survivors have met with somewhat limited success (Teasell et al. 2003).
The capacity of humans without neurological impairments to adapt their gait pattern in response to dramatic environmental manipulations has been reported recently. For example, people trained on a split-belt treadmill demonstrate short-term interlimb gait adaptations immediately following training, although this adaptation does not persist (Reisman et al. 2005; Choi and Bastian 2007). Similar results including short-term transfer of the aftereffect of adaptation to over-ground walking have been described in stroke survivors, leading to a temporarily more symmetric gait (Reisman et al. 2009). Although gait patterns of both healthy adults and stroke survivors show adaptation when exposed to environmental constraints, the extent to which those gait patterns can be adapted, what type of feedback is needed to facilitate the strongest adaptation, and the exact nature of training required for short-term gait adaptations to become learned patterns (i.e., a relatively permanent change; (Schmidt 1988) are largely unknown. The current study investigated similar questions to the first of these two in healthy adults using a paradigm primarily designed to facilitate modification of a subject’s intralimb gait pattern rather than interlimb gait parameters. This work served as a starting point for current investigations of the efficacy of this gait-retraining paradigm, involving robotic guidance, in persons with neurological impairments such as stroke.
Many studies of upper extremity tasks such as reaching provide indirect evidence of intralimb adaptations that preserve quasi-straight-line reaching behavior (Shadmehr and Mussa-Ivaldi 1994; Brashers-Krug et al. 1996; Bhushan and Shadmehr 1999; Shadmehr and Moussavi 2000; Donchin and Shadmehr 2004; Hwang et al. 2006), including possible neural mechanisms underlying those adaptations and their memory consolidation (Shadmehr and Holcomb 1997; Krakauer et al. 2005; Krakauer and Shadmehr 2006; Shadmehr and Krakauer 2008). Various training paradigms have been developed to facilitate such adaptations.
Visual and proprioceptive information appear to play an important role in motor adaptations and in the learning of novel motor tasks. Although recent studies have demonstrated that real-time visual feedback may not be a critical factor when adapting to a novel dynamic task (Tong et al. 2002; Scheidt et al. 2005; Franklin et al. 2007), visual information is important for the fine-tuning of those movements, especially at movement termination (Franklin et al. 2007).
All of the above-mentioned studies, including studies of interlimb gait modifications in stroke survivors, have involved perturbations to the motor system that result in aftereffects. In the case of normal reaching behavior, aftereffects lead to unwanted deviations from a quasi-straight line movement path and are presumed to reflect a change in an internal model of reaching dynamics (Shadmehr and Holcomb 1997; Krakauer et al. 2005). In the case of interlimb adaptations in stroke survivors, the aftereffects are actually used to induce a positive change in gait symmetry (Patton et al. 2006). Thus, the sine qua non of motor adaptation appears to be the presence of an aftereffect that results from an attempt to maintain one’s current end-effector trajectory in the face of abnormal environmental dynamics. Although we envision the gait modifications reported in the current study to represent a general form of adaptation, reflecting changes in behavior in response to a training stimulus that persist in the short-term without intention, the perturbation induced by our training is different and the response lacks the aftereffects typically reported in the motor adaptation literature. These differences will be discussed in greater detail in the “Discussion” section.
The paradigm used in the current study compares robotic guidance of limb movement to visual guidance alone or a combination of the two to facilitate changes in a person’s normal gait pattern. Recent evidence suggests advantages of combining robotics with existing training programs to enhance functional improvements in movement tasks involving both upper and lower extremities in people with neurological disorders (Krebs et al. 1998; Daly et al. 2005). Robot technology applied to rehabilitation provides the possibility of continuous or intermittent on-line quantitative movement assessment (Reinkensmeyer et al. 2000). Results of previous studies have provided insights about the application of robot-assisted therapy in general, e.g., the advantage of applying certain types of force field (Dipietro et al. 2007).
The gait-retraining program developed in our laboratory directly targets the gait pattern by providing variable compliance and variable-width virtual footpath tunnels that limit the footpath to a range of footpaths rather than enforcing a fixed footpath. The control scheme encourages patients to voluntarily correct their atypical gait patterns to produce a walking patterns more similar to non-neurologically impaired individuals and, hopefully, a more efficient range of footpaths (Banala et al. 2007, 2009). A variation of this approach has been used in the training of upper limb function (Fasoli et al. 2003; Stein et al. 2004). This approach continually challenges the participant to match the prescribed target pattern, while various degrees of constraint (i.e., width and compliance of virtual elastic tunnel walls) are used to resist large deviations of the end-effector path from a desired path, combined with visual guidance. The results of the current study provide a proof of concept for our ongoing studies of gait retraining in persons with impaired gait patterns following a stroke. In the current study, we hypothesized that gait training that combined real-time kinetic guidance, provided by a robot, with visual guidance would lead to more significant and more persistent changes in the gait patterns of healthy individuals than would primarily real-time kinetic guidance or visual guidance alone.
Method
Subjects
Eight males and five females were randomly assigned to each of three groups receiving treadmill training: (1) with real-time visual guidance (VG) of participants’ ankle trajectory alone, referred to in what follows as the footpath (25.8 ± 5.3 years old, 175.0 ± 7.8 cm height, 69.3 ± 11.7 kg weight), (2) with primarily kinetic guidance provided by compliant force-field tunnels (FFC) used to limit the range of their footpaths (26.0 ± 4.5 years old, 173.1 ± 8.4 cm height, 70.0 ± 12.9 kg weight), and (3) with combined kinetic and visual guidance (FFC + VG) (24.9 ± 3.8 years old, 174.1 ± 7.2 cm height, 74.3 ± 12.1 kg weight), for a total of 39 participants. Based on statistical analysis of outliers using SPSS, we eliminated one subject from each group from the analysis, leaving 12 subjects in each group. Participants in the FFC group did receive a 30-s interval of visual information about the desired footpath in order to provide brief information about the goal of the training. Subjects had no musculoskeletal or neurological problems. Each participant signed an informed consent approved by the University’s Institutional Review Board before participating in the study.
Device description
The design of the active leg exoskeleton (ALEX) is described in detail elsewhere (Banala et al. 2007, 2009). It has five main components, i.e., trunk, thigh, shank and foot segments of the orthosis, and a walker which supports the weight of the orthosis. Each segment of the orthosis is adjusted based on the subject’s stature. The device allows only sagittal plane movements (flexion and extension) for the knee and ankle joints, and both sagittal and frontal plane movements for the hip joint. Sagittal plane hip and knee joint motions are actuated using two motors that can generate a maximum of 50-Nm peak joint moment. Encoders attached directly to the motors measure the joints’ angular position and displacement. A separate encoder at the ankle measures ankle joint motion. The physical interface between the orthosis and the human leg is by way of a thigh and shank cuff, and a plastic orthotic that fits into the person’s shoe. The device has two force-moment sensors, one mounted between the thigh segment of the orthosis and subject’s thigh, the other mounted between the shank segment of the orthosis and the subject’s actual shank. To minimize inertial effects of device on the subject while walking, the orthosis consists primarily of lightweight aluminum. The inertial effects during training period are small compared to the forces applied by a force-field controller.
Because currently there are only two force-torque motors and force sensors built into the device, control is actually of the trajectory of the ankle’s location in space rather than of the distal foot location. Ankle motions are important to provide for fine adjustments of the terminal foot position during swing, helping to determine foot clearance from the ground. However, the general spatial position of the foot is determined by knee and hip excursions, which determine the ankle’s location in space. Therefore, although the force constraints are applied to constrain motion of the distal shank, for simplicity, we refer to control of footpath in this article. The effect of the training on ankle motion also is examined, however.
Safety of the device is ensured by the presence of physical stops at the maximum allowable range of motion of each joint, by limiting the maximum force that the motors can apply, specified by the controller, by the limited capacity of the DC-motor, and by two emergency stops accessible to the participant and experimenter. The physical stops can withstand the maximum moment that the actuators can apply. The emergency stops are wired to stop both the robot actuators and the treadmill gradually.
Training procedure
Participants in all three groups performed treadmill walking while wearing the ALEX on their right leg. All training was performed in a single session involving six 10-min blocks of gait training with 2-min rest between blocks (Table 1). The training procedure of this study is similar to conventional therapeutic approach that gradually decreases the therapist’s assistance as the patient recovers functional ability. The participant’s preferred speed with ALEX was determined during a 5-min period of unconstrained, i.e., no forces applied, walking without visual guidance before beginning training and this speed was used for training and testing sessions. The preferred walking speed, which ranged from 1.6 mph to 2.0 mph (from 0.72 to 0.89 m/s), was not different among the three groups (P > 0.05).
The FFC + VG and VG groups both received continuous visual guidance about their footpath displayed on a computer monitor positioned in front of the treadmill (Fig. 1). The footpath was computed from the encoder data and represented the instantaneous position of the ankle joint relative to the hip joint. In addition, the prescribed footpath that participants were to match was displayed on the monitor. They were instructed to keep their actual footpath, indicated by a red cursor, as close to the prescribed footpath as possible. The prescribed footpath for this study was determined in preliminary studies to ensure that participants found the task challenging but could eventually track it. We determined that a footpath that was scaled down by 10% in the horizontal direction (step length) and 40% in the vertical direction (step height) from a participant’s normal (baseline) sagittal plane footpath fit these criteria. The FFC group was provided information about the instantaneous foot position and the prescribed footpath for 30-s intervals prior to the first block of training and after every two blocks of training to provide minimal information about the required task. Thus, this group did not receive purely kinetic guidance, although there was no visual guidance during training and visual feedback was minimal compared to the VG group.

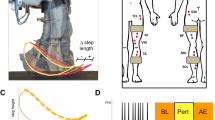
Photograph of participant walking on a treadmill with ALEX applied to his right leg. The computer monitor in front of the participant is used to provide visual guidance of both the actual footpath and the prescribed footpath
For both the FFC + VG and FFC groups, a force-field controller applied compliant constraints in the form of a virtual tunnel wall that constrained the amount of deviation of their footpath from the prescribed footpath. The controller generated virtual elastic tunnels that provided soft constraints for the footpaths. The constraints were changed over the course of training across three increasing wall widths, i.e., narrow (1 cm), medium (2 cm), and wide (4 cm), and two decreasing wall stiffness: [high] K Fn = 0.760 N and [low] K Fn = 0.125 N. This nonlinear parabolic normal force profile works like a stiffening nonlinear spring in restraining excessive deviation from the prescribed footpath. When the actual footpath encountered the virtual wall of the tunnel, further deviations beyond the virtual wall could occur, but these deviations were met with increasing resistance as the footpath deviation increased. At training onset, the footpath was maximally constrained with a narrow virtual wall width and high wall stiffness to approximate the desired trajectory. Then, six combinations of tunnel width and wall stiffness were incrementally changed after every 10-min training block for both the FFC + VG and FFC groups to reduce the constraint on the footpath (see Table 1).
When the force field was active, the robot actuators were used to apply desired torques to the hip and knee joints. The non-redundant mapping between footpath and joint angles allowed the application of joint torques that achieved the desired footpath constraints. Proper calibration and alignment of the device for each subject ensured that the joint axes of the device and subject were as congruent as possible. In addition, keeping the applied torque values low for the subject’s safety also ensured that any shear forces created from any slight misalignment was minimal.
A participant’s footpath was restricted to a range of footpaths, the possible range being determined by the width of the virtual tunnel and wall stiffness. The force-field controller provided almost zero impedance when the participant’s foot was within the tunnel walls and offered higher impedance with foot “contact” with the tunnel walls. Although the VG group walked in ALEX, no force-field constraint was applied during training. Nonetheless, they had to move against the inertia of the device.
Testing procedure
A 3 min of treadmill walking performance was evaluated in all groups prior to training (baseline) and at three post-training test sessions while they wore the exoskeleton on the right leg without an applied force field or vision of their own footpath or of the prescribed footpath used during training. The three post-training evaluation sessions were conducted immediately post training (IPT), after 10 min of over-ground walking out of the device (retention 1), and after 2 h of general activity out of the device (retention 2). During the IPT and retention evaluations, nothing was mentioned or implied about the previously prescribed footpath used during training. Participants were instructed to walk as normally as possible on the treadmill while looking straight ahead. Sample footpaths for the baseline, immediate post-training, and two retention tests are provided in Fig. 2a (a typical performing subject) and b (one of the best performing subjects) for two participants in the FFC + VG group.

Average changes of path of the ankle position a for a typical performing subject and b for a best performing subject in the FFC + VG group across test sessions: the dashed black line represents a prescribed path; the baseline path is represented by a thin, solid black line, representing the participant’s walking pattern before training; the immediate post-training (IPT) test session is shown as a dotted black line. Retention 1 (dash-dotted, black line) test was performed after a 10-min period of continuous over-ground walking following IPT. The Retention 2 (thick, solid gray line) test followed a 2-h period of normal activity outside the lab. Values on the y-axis represent the vertical position of the ankle relative to the hip joint
Data processing
Data processing was performed using MATLAB 7.3.0 (the MathWorks, Inc.). The variables presented in this report are limited to those obtained during the baseline, immediate post-training, and two retention test sessions when participants from all groups walked without the force-field on, without visual guidance of the desired foot template, and were asked to walk as normally as possible. They included a measure of footpath deviation, i.e., the area between actual and prescribed footpaths, joint angle variables related to step height and step length, integrated hip and knee joint moments, variability of the relative timing of maximum angular velocities during the swing phase, and measures of interlimb symmetry, including relative stance times and relative timing of left heel strike within the stride cycle of the right foot. The entire 3-min data (about 100 gait cycles per each testing period) were used to calculate the averages of the testing variables. All data from the encoders and force-moment sensors were collected at 1,000 Hz. The force-moment data were filtered at 50 Hz, and the encoder data (joint position) were filtered with an 8 Hz forward–backward Butterworth filter.
The area enclosed between a prescribed footpath and the actual footpath during the swing phase was used to define a metric to measure the amount of deviation. The curves shown in Fig. 3a are curves whose enclosed area needed to be determined. The solid curve is the actual footpath whereas the dashed curve is the prescribed footpath. First, we connect ends of the curves with straight lines. To find the area of a closed (possibly self-intersecting) polygon shown in Fig. 3b, we used a “plane-sweep” algorithm described in detail in O’Rourke (1994). This algorithm divides the polygon into several vertical slices, each vertical “cut” appearing at a sample point on the polygon. The slices may not be of equal width. Each slice can be approximated as a trapezoid, whose area we can find. Therefore, the net area of the polygon is the sum of areas of all the slices (Fig. 3b).

Method involved in determining the area enclosed between two curves. Solid curve is the actual footpath, while the dashed curve is the desired footpath. See the section of “Data processing” for the details of calculating this area
Joint angle measures were computed from the joint encoder signals. Joint moments of the hip and knee were computed using data from the encoders and force-moment sensors (Banala et al. 2006). Because we had no force-moment sensor at the ankle, ankle joint moments are not reported here. The integrated moment with respect to time, i.e., area under the moment versus time curve, for each joint over the swing phase, was calculated for two directions, i.e., flexion and extension, using the computed moments. In addition, the relative times (τ rel) required for the hip and knee joints to reach their maximum angular velocity during the swing phase were calculated as follows.
The standard deviation (SD) of the relative timing measures then was computed as a measure of timing variability.
The above measures were obtained only for the right leg because only this leg’s motion was affected directly by the exoskeleton, which contained encoders and force-moment sensors. However, foot switches were applied to the toe and heel of both feet. Foot switch data from both shoes were used then to compute stance time, swing time, and interlimb timing, or the time of left heel strike as a percentage of the right foot’s stride cycle (heel strike to subsequent heel strike). Because stance and swing times when expressed as a percent of the gait cycle (i.e., stance + swing) sum to 100%, only relative stance times were analyzed statistically.
Analysis
The area between the actual and prescribed footpaths obtained from the baseline evaluation was compared among the groups for initial differences using a one-way, between-subjects analysis of variance (ANOVA).
Our hypothesis was that as a result of training, participants’ footpaths would match more closely the prescribed footpath, leading to a reduction in the area computed between the two. If so, the area was expected to be much smaller after training than for the baseline test. To test this expectation and investigate differences in the training procedure, we conducted a group by session (baseline versus IPT session) ANOVA on the area measure.
To evaluate whether and to what extent an observed gait modification was maintained across the retention tests, and whether it differed among the groups, we subtracted the area measurement obtained at each post-training test session from the baseline measure. This measure is referred to in what follows as the relative area. If there was a substantial reduction in area between the actual and prescribed footpaths after training, indicating improved performance, then the relative area was expected to be large given the expected poor match between actual and prescribed footpaths at baseline (i.e., large area). If there was no change due to training, then the relative area should be close to zero. Thus, a large relative area indicates a positive training effect. The relative area was subjected to a mixed-model ANOVA with group (three levels) as the between-subjects factor and the post-training evaluations (three levels) as the within-subjects factor. Our a priori hypothesis was that the FFC + VG group would show the largest and longest lasting training effect. Thus, we also tested the relative area of each group at the 2-h retention test for differences from zero, which would reflect a return to baseline performance.
Comparable ANOVAs were also used to test for baseline differences in the joint angle measures, integrated joint moments, joint τ rel measures, as well as the interlimb measures and in differences of those measures between baseline and the IPT session. The difference between each post-training test and the baseline evaluation for joint angle measures (ΔΦ = θpost-training − θbaseline), relative timing (Δτ rel), and the standard deviation of relative timing (ΔSDτ rel) were evaluated with mixed-model ANOVAs (group by joint by direction by post-training session). The change of moment for a given post-training evaluation compared to the baseline was also investigated with a mixed-model ANOVA, the dependent variable being the ratio of the post-training to the baseline integrated joint moments (ΔMint). A positive value of change indicates an increase compared to baseline. A value greater than 1.0 for ΔMint indicated that there was an increase in the joint moment post training. Only if there were significant main effects or interaction effects were post hoc tests used to evaluate the source of the effect where appropriate.
One-way ANOVAs were performed on the interlimb symmetry measures to investigate differences at the baseline evaluation. Because a significant difference was present for these variables only at the baseline test, the baseline values were used as covariates to investigate differences among the groups as a result of training (ANCOVA).
Results
Area of the footpath
The area between participants’ footpaths and the prescribed footpath, which was not shown to participants during any of the test sessions, was relatively large at the baseline test but did not differ among the FFC + VG, FFC, and VG groups (F 2, 33 = 0.43, P > 0.05; Table 2).
Subjects’ footpaths became closer to the prescribed footpath, as evidenced by a significantly smaller area between the two, immediately after training when compared to the baseline test (F 1, 33 = 44.1, P < 0.01). Greater approximation of the actual and prescribed footpaths was found for all groups immediately after training, but the magnitude of the difference was dependent on the group (F 2, 33 = 3.6, P < 0.05), with a larger decrease in the area between actual and prescribed footpaths observed for the FFG + VG (Fig. 4, IPT).

The area between the prescribed and actual footpaths was computed as a measure of how well participants matched the prescribed path (Fig. 3). The average difference between the areas computed during the post-training tests (i.e., IPT, Retention1 and Retention 2) and the area computed during the baseline test are presented. Error bars represent the standard error of the mean (SEM). FFC + VG force-field constraint plus visual guidance, FFC force-field constraint, VG visual guidance. Improved matching of the prescribed footpath by the actual footpath would be represented by a large relative area (i.e., large baseline area minus small post-training area), whereas smaller improvement would result in a smaller relative area. The inset shows the actual areas for each training group obtained at baseline and immediately after training (IPT). Note that because the area on IPT as never zero, subjects did not perfectly match the prescribed path
The areas between actual and prescribed footpaths for the three post-training test sessions relative to the baseline area are presented in Fig. 4. This relative area measure differed significantly between the training groups (F 2, 33 = 4.8, P < 0.05). Post hoc analyses indicated that this difference was due to an overall larger relative area, i.e., smaller difference between the actual and prescribed footpath after training, for the FFC + VG group compared to either the FFC (P < 0.01) or VG (P < 0.05) group, while there was no overall difference between the latter groups (P > 0.05). The magnitude of the training effect decreased across the post-training test sessions (decreased relative area) for all groups (F 2, 66 = 24.0, P < 0.01), indicating a gradual washout of the training effect. The group by session interaction did not reach significance (F 4, 66 = 1.4, P > 0.05), however, indicating a relatively similar decrease in training effect for all groups. Nonetheless, the relative area for the FFC + VG group was still significantly different from zero (t 11 = −2.7, P < 0.05) at the 2-h test, indicating an actual footpath that was closer to the prescribed footpath than was the case at the baseline test session. This was not the case for either the FFC (t 11 = −0.49, P > 0.05) or VG (t 11 = 0.001, P > 0.05) groups.
Joint angle measures
Adaptation of the subjects’ footpaths requires changes in joint kinematics and kinetics. Here, we investigate kinematic changes related to the improved matching of subjects’ footpaths to the prescribed footpath as a result of training. Measures related to changes in step height and step length were investigated separately. At the baseline test session, none of the hip, knee, or ankle angular measurements differed among the three training groups (F 2, 33 = 0.62, P > 0.05; Table 2), nor was there an interaction between group and angular measurement (F 4,8 = 0.44, P > 0.05).
For the angular measures contributing to step height, i.e., maximum hip and knee flexion during swing, there was a significant group difference between the baseline and IPT (F 2, 33 = 5.7, P < 0.01). Both hip flexion and knee flexion decreased more for the FFC + VG group following training compared to the other groups, as evidenced by the larger decrease from baseline values illustrated by the negative values in Fig. 5. This reduction in step height was related most to a reduction in maximum knee flexion during swing (F 1, 33 = 69.3, P < 0.01), which decreased more immediately post training for the FFC + VG than the other groups (F 2, 33 = 3.9, P < 0.05; Fig. 5). In contrast, while the maximum hip flexion angle decreased overall with training (F 2, 33 = 12.8, P = 0.051), the effect of group only approached significance (F 2, 33 = 3.1, P = 0.06). None of the angular measures related to step length, i.e., hip extension or knee extension at heel strike, showed a significant group difference (F 2, 33 = 0.91, P > 0.05) or an interaction between group and test session (F 2, 33 = 1.2, P > 0.05).

Average difference in maximum hip and knee flexion during swing and the ankle angle at toe-off between each of the post-training tests and the baseline test. Positive and negative values indicate increase and decrease in the joint measures, respectively. FFC + VG: force-field constraint plus visual guidance, FFC force-field constraint, VG visual guidance, IPT immediate post-training, R1 retention 1, R2 retention 2. Error bars represent SEM
The ankle position at toe-off provides an indication of how much push-off occurs, which contributes to the energy of swing. Therefore, we investigated changes in this angle relative to the baseline test. Compared to the baseline test, the ankle was found to be more dorsiflexed immediately post training (F 1, 2 = 61.2, P < 0.01), and the amount of decrease was larger for the FFC + VG group (F 2, 33 = 3.9, P < 0.05), as illustrated in Fig. 5.
We next considered the changes (ΔΦ values) relative to the baseline measures across the three post-training test sessions for those measures shown to change significantly between baseline and IPT tests. Maximum hip flexion gradually increased over the post-training sessions, approaching the baseline condition (zero values of ΔΦ) by the 2-h retention test (F 2, 66 = 6.5, P < 0.01). Although this gradual increase in hip flexion across post-training sessions was similar for all groups (F 4, 66 = 1.1, P > 0.05), there was an overall group difference (F 2, 33 = 3.3, P = 0.05), with the FFC + VG group having slightly less maximum knee flexion than the other groups. Similar results were obtained for both maximum knee flexion and the ankle position at toe-off. The knee flexed more during swing as subjects approached 2 h post training (F 2, 66 = 11.4, P < 0.01), leading to a gradually increased step height. The gradual decrease in this measure across follow-up tests was not significantly different across groups (F 4, 66 = 0.89, P > 0.05), although there was a significant overall group difference when collapsing across the post-test sessions (F 2, 33 = 8.3, P < 0.01). This resulted from the FFC + VG group having a larger overall reduction in knee flexion during the post-test sessions compared to baseline (Fig. 5). The ankle angle gradually approached the baseline angle at toe-off across the post-training test sessions (F 2, 66 = 10.4, P < 0.01). However, there was no interaction with group (F 4, 66 = 0.85, P > 0.05). As with knee flexion, when collapsed across the post-training retention tests, the FFC + VG group exhibited a less plantar flexed ankle position at toe-off compared to the other groups (F 2, 33 = 5.7, P < 0.01; Fig. 5).
Integrated joint moment
Analysis of joint moments was limited to those most relevant to observed changes in the angular measures following training, i.e., changes in the hip extension moment used to limit hip flexion and the knee flexion moment related to knee flexion. Ankle moments were not considered because a force transducer was unavailable to measure them directly. There were no significant group differences (F 2, 33 = 0.27, P > 0.05; Table 2) in the integrated joint moments at the baseline test, nor was there an interaction between joint and group (F 2, 33 = 0.40, P > 0.05).
The hip extensor moment increased for the FFG + VG group immediately after training, whereas it decreased for the other two groups (F 2, 33 = 4.9, P < 0.05; Fig. 6). The knee flexor moment was reduced overall at the IPT session (F 1, 33 = 9.3, P< 0.01). Although this decrease was quantitatively greater in the FFC and VG groups (Fig. 6), the interaction of training method and group was not significant (F 2, 33 = 0.73, P > 0.05).

Average difference in integrated hip extensor and knee flexor moments between each of the post-training tests and the baseline test. Positive and negative values indicate increase and decrease in joint moment with respect to baseline, respectively. FFC + VG force-field constraint plus visual guidance, FFC force-field constraint, VG visual guidance, IPT immediate post-training, R1 retention 1, R2 retention 2. Error bars represent SEM
For hip extension, ΔMint did not change significantly across the post-training tests (F 2, 66 = 0.57, P > 0.05), nor was there an interaction between post-training test session and the training method (F 4, 66 = 1.3, P > 0.05). However, there was a significant overall difference between the groups following training (F 2, 33 = 7.8, P < 0.01), with the FFG + VG group maintaining a slight increase in hip extensor moment (ΔMint > 1.0), while the other two groups maintained a decreased moment compared to the baseline test (ΔMint < 1.0; Fig. 6). The reduced knee flexion moment following training, evidenced by ΔMint < 1.0, approached the baseline value across the three post-training tests (F 2, 66 = 11.1, P < 0.01). However, surprisingly, this increase in ΔMint was not affected significantly by the training method (F 4, 66 = 0.69, P > 0.05), nor was there an overall difference among the training groups (F 2, 33 = 1.0, P > 0.05).
Mean and variability of relative timing of maximum joint velocity
Examination of the relative timing (τ rel) of the velocity of hip and knee events during mid-swing revealed no training group difference (F 2, 33 = 0.30, P > 0.05), nor were there any interactions of either direction (flexion–extension) or joint with group (all P > 0.05). The same was true of relative timing variability (SDτ rel; F 2, 33 = 1.0, P > 0.05), with no significant interactions with group (all P > 0.05; Table 2).
There were no group differences of τ rel values immediately post training compared to the baseline test (F 2, 33 = 0.59, P > 0.05), nor were there any significant interactions involving training group (all P > 0.05). Consequently, analyses of Δτ rel across the post-training evaluations were not conducted.
A significant interaction of joint (hip vs. knee), direction (flexion vs. extension), test session (baseline vs. IPT), and training group was found for SDτ rel (F 2, 33 = 10.1, P < 0.05). Separate ANOVAs to examine simple interaction effects revealed no significant interactions of any variable with training group for relative timing variability for knee velocity events (all P > 0.05). In contrast, for hip velocity events, SDτ rel depended on the test session, direction and group (F 2, 33 = 5.6, P < 0.01). This effect was due to hip extension, the ANOVA indicating that SDτ rel was significantly higher after training for the FFC + VG group, whereas SDτ rel for the FFC and VG groups changed minimally following training. Thus, SDτ rel of peak hip extension velocity relative to its baseline value (ΔSDτ rel) was substantially greater than zero for the FFC + VG group (Fig. 7).

Average difference in the variability (SD) of relative timing of joint velocities within the gait cycle for the hip and knee joints in each direction, computed between each of the post-training tests and the baseline test. Positive and negative values indicate increase and decrease in joint relative timing variability compared to baseline, respectively. FFC + VG force-field constraint plus visual guidance, FFC force-field constraint, VG visual guidance, IPT immediate post-training, R1 retention 1, R2 retention 2. Error bars represent SEM
The overall group difference in ΔSDτ rel for hip extension was maintained for post-training tests (F 2, 33 = 5.7 P < 0.01) and did not change significantly across the three post-training tests (F 4, 66 = 2.1, P > 0.05), although there was a trend for ΔSDτ rel to decrease by the 2-h retention test (Fig. 7).
Measures of interlimb symmetry
Relative stance time
Table 3 presents the average (±SD) stance time of each limb relative to the gait cycle time. At the baseline evaluation, all groups exhibited a longer relative stance time on the left than on the right leg (F 1, 33 = 115.9, P < 0.01). Thus, wearing the exoskeleton induced a slight bilateral gait asymmetry for all groups. Although there was no overall group difference (F 2, 33 = 0.89, P > 0.05), there was a group by leg interaction (F 2, 33 = 3.6, P < 0.05). Despite identical performance conditions at baseline, the FFC + VG group exhibited a significantly larger interlimb stance time difference than did the FFC group (P < 0.05; Table 3). The FFC + VG and VG groups did not differ, however, on this measure (P > 0.05). Because of the initial differences at baseline, we used the ratio of right–left stance times as a covariate when investigating symmetry differences post training.
The ANCOVA investigating post-training differences in relative stance time between the legs revealed no significant effect of training group (F 2, 32 = 2.6, P > 0.05). Nor was there a significant interaction with between group, leg and test session (F 4, 64 = 0.55, P > 0.05) or between group and test session independent of leg (F 4, 64 = 1.3, P > 0.05).
Relative timing of left and right leg
Table 4 presents the relative time of occurrence of the left leg’s heel strike within the stride cycle of the right limb. At the baseline evaluation, there was a significant difference among the three training groups (F 2, 33 = 3.9, P < 0.05). This was due to a slightly later heel strike for the FFC group compared to both the FFC + VG (P < 0.05) and VG (P < 0.05) groups, which did not differ from each other (P > 0.05).
When controlling for the baseline differences in interlimb relative timing, no differences were found among the training groups (F 2, 32 = 0.49, P > 0.05) across post-training tests, and no significant interaction of test session with group (F 4, 64 = 0.57, P > 0.05).
Discussion
The current investigation revealed that short-term gait modifications lasting up to 2 h could be induced in healthy individuals. These modifications were achieved by subjects’ conscious effort to match a prescribed gait pattern. Providing subjects with visual information about the mismatch between the prescribed footpath and their actual footpath was sufficient to induce an immediate, short-lasting change of their gait pattern. Previous studies have shown that sensory inputs, including real-time visual feedback, can serve to promote desired gait changes in individuals recovering from a stroke (Morris et al. 1992; Colborne et al. 1993). In contrast, more basic studies have reported a limited effect of real-time visual feedback on adaptation to a novel dynamic task (Tong et al. 2002; Scheidt et al. 2005; Franklin et al. 2007). Nonetheless, real-time visual information may be important to fine-tune targeting movements (Franklin et al. 2007). However, in those studies, the target of the reaching behavior was present at all times, whereas in our study, no information was provided about the target (the prescribed footpath) during the baseline and post-training evaluations.
Providing kinetic information via a compliant force field that indicated to subjects that their footpath was deviating from the prescribed path (FFC group) led to a similar immediate post-training gait modification as did visual guidance alone (VG group). Although the FFC group received a very brief period of vision of their footpath relative to the prescribed path to provide them with basic information about the required task, this amounted to only 2.5% of the total treadmill training time (i.e., 1.5 min of the total 60 min). Thus, the training of this group was quite different from the FFC + VG group. Neither visual guidance alone nor primarily kinetic guidance led to a gait modification that lasted beyond the 10-min retention test, however. We cannot rule out that the FFC group, in particular, made other gait adaptations as a result of the unusual force applied to their leg even though this was not reflected in their footpath modification. The very brief visual information provided to this group about their footpaths and the prescribed footpath was an attempt to limit unrelated adaptations, however.
In contrast, the group receiving a combination of visual and kinetic guidance showed the largest change in their footpath from the baseline, and this group maintained their modified gait pattern to some extent for up to 2 h after performing over ground, everyday activities following training. Thus, at least in the context of this study, a combination of visual and kinetic guidance appears superior to either modality alone for achieving a desired change of a person’s gait pattern. Although this study was performed in healthy subjects and the effect diminished by 2 h after training, the results suggest a possible avenue for enhancing gait retraining in persons following a stroke and possibly other central neurological disorders. We emphasize that all testing conditions in the current study were identical for all groups, with no information provided to participants about their footpath, the prescribed footpath used during training, nor any kinetic guidance. In addition, participants were instructed to walk as normally as possible during these evaluation sessions.
Kinematic and kinetic changes underlying the gait modifications
Joint kinematics
Kinematic changes underlying changes in subjects’ footpaths were primarily related to events reducing the step height. All subjects exhibited a decrease in knee flexion during swing, with the greatest decrease immediately after training occurring in the FFC + VG group. These differences from baseline were still present to some extent by the 2-h retention test, particularly in the FFC + VG group (Fig. 5). This group also exhibited a decrease in hip flexion immediately after training, which was not the case for the other two groups. In contrast, angular changes most related to step length did not change significantly for any training group. This was likely due to the fact that required changes in step height (40% reduction) were substantially greater than the reduction in step length (10%) indicated by the prescribed footpath. Thus, subjects apparently focused most on the dimension that required the most change. This difference may also reflect a perceptual limit, i.e., that the amount of required change needs to exceed a particular value before subjects become sensitive to it, although the current results are not adequate to support this possibility.
We also examined changes in the ankle position at toe-off. One expects the ankle to be plantar flexed immediately after toe-off as a consequence of the propulsive force of the triceps surae, providing the initial energy for swing. With the requirement to reduce step height and length, it was reasonable to expect that there would be a reduction in this propulsive force and, consequently, a more dorsiflexed ankle at toe-off. Indeed, the results confirmed this hypothesis. All training methods led to a reduction in the amount of plantar flexion at toe-off. However, the greatest effects were, once again, in the FFC + VG group, with the ankle actually being dorsiflexed at toe-off, determined by foot switch events, for up to 10 min post training (cf. Table 2; Fig. 5). The ankle angle deviated from baseline in this group up to 2 h post training, and this tended to be the case for the FFC group as well.
The fact that the FFC + VG group exhibited both less ankle plantar flexion at toe-off and a smaller maximum knee flexion during swing compared to the baseline test that lasted up to 2 h post training seems remarkable. This is particularly the case given the typical stability of normal gait patterns in healthy young adults and the fact that the subjects performed their normal activities between the 10-min post-training test and the 2-h test. Of course to adapt the gait pattern to the scaled-down version used in this study, a decreased range of joint motion was required.
Joint kinetics
The gait modification was associated with small changes in the integrated knee and hip joint moments. No significant changes were found in either hip flexion or knee extension moments related to the training method. The hip extension moment changed in the opposite direction for the FFG + VG group compared to the other two groups. The increased hip extension moment could have two effects on limb kinematics. First, it would tend to reduce the maximum hip flexion achieved during swing. Only this group showed such a change after training (Fig. 5). In addition, reducing the momentum of the thigh would induce less acceleration of the knee into flexion (Goldberg et al. 2009). The contributions of the stance limb are likely also important in this regard (Arnold et al. 2007), although we had no way to directly measure these in the current study. This group exhibited a greater decrease in knee flexion after training than did the other groups.
Interestingly, the integrated knee flexion moment was reduced after training and, although this reduction was not affected by the training method, the magnitude of the reduction was quantitatively greater in the FFC and, to a lesser extent, the VG group, than the FFC + VG group. The combined results of the hip extension and knee flexion moments may suggest a different strategy used by the FFC + VG group compared to the other groups. That is, the FFC + VG group apparently tried to alter both hip and knee flexion by altering hip kinetics, which led to greater success in adopting the prescribed footpath.
Changes in the relative timing of joint motion
Although there no changes occurred in the relative timing of joint motions with training, changes in relative timing variability did occur that differed among the training methods. Once again, this was primarily related to the hip. The most substantial change in the relative timing of occurrence of joint velocities was for hip extension. Timing variability increased for the FFC + VG group following training. This increased variability was reduced quantitatively throughout the post-training test sessions but was maintained up to the 2-h test. In contrast, a similar change in joint timing variability was not present in either of the other groups. This result might reflect subjects in the FFC + VG group attempting to modulate their hip kinetics in light of changes in other joints to achieve the reduction in hip and knee flexion required to decrease their step height. In any case, the result is consistent with the greater changes in the hip extensor moment exhibited by this group.
Interlimb symmetry
Relative stance time
Because all subjects wore an exoskeleton on their right legs during testing, whether or not they received force feedback during training, changes in the gait symmetry could be expected. We evaluated whether these changes were present and whether they differed among the groups. All groups exhibited relative stance time asymmetries as a result of being in the device, relative stance times being longer on the left versus right legs. The magnitude of these interlimb differences at the baseline test was larger for the FFC + VG and VG groups than for the FFC group. However, when controlling for the baseline differences, the effect of training did not lead to additional differences between the training methods or interactions of other factors with training method.
Interlimb relative timing
We also examined the relative timing of the left leg’s heel strike within the stride time of the right limb. Once again, there were group differences at baseline, with the FFC + VG and VG groups having slightly shorter relative times of contact with the left leg, but when controlling for this difference, we found no differences among the training methods as a result of training. Thus, the results for relative stance time and relative interlimb timing indicate that wearing the exoskeleton did induce a gait asymmetry, but this did not appear to have an impact on the training itself.
Possible neural mechanisms underlying gait pattern modifications
What might account for the ability of healthy individuals to modify their gait to match an altered pattern following only 1 h of training? The cerebellum is known to be involved in short-term motor adaptation of arm movements to unusual force fields (Shadmehr and Krakauer 2008). Impaired adaptation of interlimb coordination has been reported in cats with cerebellar damage (Yanagihara and Kondo 1996). People with cerebellar lesions also have been shown to have limited interlimb adaptation during split-belt treadmill walking (Morton and Bastian 2006). These authors have suggested that the midline cerebellum, i.e., spinocerebellum, which projects to the brainstem, might be an important structure for normal gait adaptation (Morton and Bastian 2003, 2006; Reisman et al. 2005). The dorsal spinocerebellar tract, which provides proprioceptive inputs to spinocerebellum, is also known to be related to postural control and limb movement (Bosco et al. 1996; Bosco and Poppele 1997). Studies of dorsal spinocerebellar tract neurons suggest that neurons contributing to the ascending tract may carry information related to sensing and/or modulating the position and orientation of the limb in space (Bosco et al. 2000; Bosco and Poppele 2003). The cerebellum, especially the spinocerebellum, might be responsible for fine-tuning proprioceptive sensory inputs from dorsal spinocerebellar tract. Thus, cerebellar short-term plasticity may play a role in the gait modification exhibited by the persons in our study. However, as discussed in the following paragraphs, the short-term “learning” exhibited by our participants differs in important ways from the effects identified in recent motor adaptation studies.
Training method
In the current study, motor learning principles guided the selection of practice parameters. Participants in the FFC + VG group were constrained to walk while keeping their foot close to the prescribed footpath, while the strength of the force-field constraint was varied throughout practice. The strongest constraint was applied at the beginning of training to help the participant adjust his/her gait pattern to the altered pattern. Increasing the width of the virtual tunnel walls and reducing the wall stiffness across training gradually reduced the level of the constraint. The participant was encouraged to challenge himself/herself to match the prescribed trajectory. This approach is different from many current robot-assisted methods of gait retraining applied to help persons with neurological disorders. Those approaches typically move the patient’s limb passively through a preset trajectory during walking (Colombo et al. 2000; Hesse and Uhlenbrock 2000; Husemann et al. 2007; Mayr et al. 2007). In their recent research report, Ivanenko et al. (2009), however, emphasize the importance of patient involvement in correcting limb patterns for more effective rehabilitation. Optimal effectiveness of our gait-retraining paradigm in persons with neurological disorders will require the exploration of additional training factors, however. For example, further manipulation of learning parameters could be used to help enhance the gait changes obtained here, including the manipulation of the frequency of feedback and visual guidance. More work is clearly needed to determine the optimal parameters for training, including the width and stiffness of the applied virtual tunnel walls and how to progress it.
Evidence from studies of motor learning indicates that effective learning requires both the provision of a model of performance and appropriate feedback during training (Schmidt 1988; Winstein 1991). Although various feedback modes have been used to facilitate functional recovery of the upper limb after a stroke, little is known about what feedback mode is most beneficial for recovery of walking. Visual feedback of the sagittal plane footpath was used in the current study. The relative motion of lower extremity joint angles can also be used to help people improve their gait pattern. However, a body of literature suggests that movements typically are planned in terms of task-level variables rather than individual effector (joint) variables (Morasso 1981; Scholz et al. 2000; Latash et al. 2007), which is why we chose to provide visual feedback in terms of the sagittal plane end-point footpath in this initial study. Moreover, the studies of Bosco et al. (Bosco et al. 2000) indicate that the proprioceptive feedback received by the brain via dorsal spinocerebellar tract neurons may be related more to overall limb length and orientation than to individual joint angles. Other investigators have suggested that training using end-point trajectory feedback might be more effective for recovery of locomotion after spinal cord injury than attempting to train specific patterns of muscle activity (Grasso et al. 2004; Ivanenko et al. 2009). Although several different methods of RAGT have been presented for gait training (Hesse and Uhlenbrock 2000; Tong et al. 2006; Husemann et al. 2007; Mayr et al. 2007; Pohl et al. 2007; Hornby et al. 2008), the end-point trajectory control mechanism, to our knowledge, has not. Participants were required to visually track a desired, albeit atypical, footpath facilitated by applying compliant forces to the hip and knee joints. The concept of our training approach is supported by a recent animal study (Cai et al. 2006) in which adult spinal mice trained with compliant force field along a desired limb trajectory improved their stepping abilities. Moreover, the results of that study showed that providing error-correction mechanisms during stepping training facilitated learning a prescribed pattern.
Do the results reflect motor adaptation?
Based on the results of this study for the FFC + VG group in particular, it is difficult to conclude that the persistent, albeit diminished footpath modification observed at 2 h post training was a purely conscious effect in light of the testing instructions. Certainly, the training procedure itself involved more explicit than implicit learning principles, especially for the FFC + VG and VG groups. Nonetheless, the result of the training ultimately appeared to be “unconscious” because participants in the FFC + VG group at least maintained some gait modification at the final retention test when instructed to walk as normally as possible, following two hours of everyday activities away from the lab. How should this modification be characterized?
Learning is reflected by a relatively long-term change of behavior (Schmidt 1988). Thus, the results cannot be considered learning in a strict sense because it is unlikely that the effect would have persisted much longer than 2 h. Instead, the changes observed might best be characterized as a form of adaptation, a phenomenon related to learning but of relatively short duration. The presence of aftereffects has become a benchmark that most investigators expect in order to accept that motor adaptation has occurred (Shadmehr and Mussa-Ivaldi 1994; Kagerer et al. 1997; Shadmehr and Moussavi 2000; Buch et al. 2003; Krakauer et al. 2005; Scheidt et al. 2005). Aftereffects in the current study would have been reflected by a longer step length and higher step height immediately at the IPT test compared to the baseline test. However, this was not the case. Instead, all participants exhibited a footpath more or less consistent with the prescribed footpath and the FFC + VG group maintained this modified gait pattern for up to 2 h post training. If aftereffects are the sine qua non of motor adaptation, then the gait modifications observed in this study represent a different type of short-term “learning”.
The form of short-term “learning” observed in the current study may be more important than that observed in typical adaptation studies. Indeed, those studies typically have applied an artificial environmental perturbation (Shadmehr and Mussa-Ivaldi 1994; Kagerer et al. 1997; Shadmehr and Moussavi 2000; Buch et al. 2003; Krakauer et al. 2005; Scheidt et al. 2005) in an attempt to explore adaptation. Generally, however, there is no attempt to induce a lasting change in subjects’ movement patterns, although the aftereffect paradigm is currently being explored as a possible method to improve gait patterns in stroke survivors indirectly (Patton et al. 2006; Reisman et al. 2007). The current paradigm requires a person’s conscious attempt to adopt the prescribed pattern. The perturbation provided for the most successful training method, FFC + VG, was a mismatch between the actual footpath and the desired footpath, specified to the learner by visual information, as well as the presence of a compliant restoring force encountered when deviating excessively from the desired pattern. For all groups, and especially the FFC group, a perturbation occurred in the initial phases of training as they attempted to produce their normal foot trajectory but encountered a compliant force tending to drive them toward the prescribed trajectory. One can conjecture that if the FFC group had received no visual guidance and were told to walk in their preferred manner, an aftereffect might have occurred, i.e., if they had fought the perturbing force. Thus, whether or not an aftereffect occurs is likely due to the nature of the instructions and, therefore, the subject’s intention. Of course, we did not intend to induce permanent changes in subjects’ gait pattern in the current study of healthy individuals. Instead, the study served as a “proof of concept” for possible longer-term application to enhance the gait pattern of persons with gait impairments following a stroke. The results suggest that this is a promising direction. Ultimately, however, future scientific investigations will have to determine if this approach, engaging the subject’s intention to change their pattern, proves more or less effective than one that uses unintentional aftereffects to induce desired gait changes.
Conclusion
Results of this study showed that healthy young participants modified their footpaths to a prescribed, scaled-down footpath after training. Participants who trained with the combination of compliant force-field constraints on their ankle movement and visual guidance retained the gait adaptation for longer than did those trained with repetitive walking using visual guidance or primarily force-field constraints. The differences appeared to be due to greater changes in hip joint kinetics and kinematics in the FFC + VG group. These results might suggest that multiple modes of guidance allow better adaptation to a new gait pattern than information provided by one channel (vision or kinetic guidance). The results provide a basis for investigating the application of this method for the retraining of gait in persons following stroke and possibly other neurological disorders. Obviously, the patient’s gait pattern would have to be morphed gradually toward a more normal pattern and yet be different enough from their current pattern to challenge the stroke survivor’s walking and encourage increased joint excursion. It is also critical, of course, to be able to show that gait adaptations can be maintained more permanently. We have recently initiated such a study in persons with a stroke that compares RAGT training to body weight-supported treadmill training.
References
Arnold AS, Schwartz MH, Thelen DG, Delp SL (2007) Contributions of muscles to terminal-swing knee motions vary with walking speed. J Biomech 40:3660–3671
Banala S, Agrawal SK, Fattah A, Krishnamoorthy V, Hsu WL, Scholz JP, Rudolph K (2006) Gravity-balancing leg orthosis and its performance evaluation. IEEE Trans Robotics 22:1228–1237
Banala S, Kulpe A, Agrawal SK (2007) A powered leg orthosis for gait rehabilitation of motor-impaired patients. In: IEEE international conference on robotics and automation, Rome, Italy, pp 4140–4145
Banala SK, Kim SH, Agrawal SK, Scholz JP (2009) Robot assisted gait training with active leg exoskeleton (ALEX). IEEE Trans Neural Syst Rehabil Eng 17:2–8
Bhushan N, Shadmehr R (1999) Computational nature of human adaptive control during learning of reaching movements in force fields. Biol Cybern 81:39–60
Bosco G, Poppele RE (1997) Representation of multiple kinematic parameters of the cat hindlimb in spinocerebellar activity. J Neurophysiol 78:1421–1432
Bosco G, Poppele RE (2003) Modulation of dorsal spinocerebellar responses to limb movement. II. Effect of sensory input. J Neurophysiol 90:3372–3383
Bosco G, Rankin A, Poppele R (1996) Representation of passive hindlimb postures in cat spinocerebellar activity. J Neurophysiol 76:715–726
Bosco G, Poppele RE, Eian J (2000) Reference frames for spinal proprioception: limb endpoint based or joint-level based? J Neurophysiol 83:2931–2945
Brashers-Krug T, Shadmehr R, Bizzi E (1996) Consolidation in human motor memory. Nature 382:252–255
Buch ER, Young S, Contreras-Vidal JL (2003) Visuomotor adaptation in normal aging. Learn Mem 10:55–63
Cai LL, Fong AJ, Otoshi CK, Liang Y, Burdick JW, Roy RR, Edgerton VR (2006) Implications of assist-as-needed robotic step training after a complete spinal cord injury on intrinsic strategies of motor learning. J Neurosci 26:10564–10568
Choi JT, Bastian AJ (2007) Adaptation reveals independent control networks for human walking. Nat Neurosci 10:1055–1062
Colborne GR, Olney SJ, Griffin MP (1993) Feedback of ankle joint angle and soleus electromyography in the rehabilitation of hemiplegic gait. Arch Phys Med Rehabil 74:1100–1106
Colombo G, Joerg M, Schreier R, Dietz V (2000) Treadmill training of paraplegic patients using a robotic orthosis. J Rehabil Res Dev 37:693–700
Daly JJ, Hogan N, Perepezko EM, Krebs HI, Rogers JM, Goyal KS, Dohring ME, Fredrickson E, Nethery J, Ruff RL (2005) Response to upper-limb robotics and functional neuromuscular stimulation following stroke. J Rehabil Res Dev 42:723–736
Dimitrijevic MR, Gerasimenko Y, Pinter MM (1998) Evidence for a spinal central pattern generator in humans. Ann N Y Acad Sci 860:360–376
Dipietro L, Krebs HI, Fasoli SE, Volpe BT, Stein J, Bever C, Hogan N (2007) Changing motor synergies in chronic stroke. J Neurophysiol 98:757–768
Donchin O, Shadmehr R (2004) Change of desired trajectory caused by training in a novel motor task. Conf Proc IEEE Eng Med Biol Soc 6:4495–4498
Fasoli SE, Krebs HI, Stein J, Frontera WR, Hogan N (2003) Effects of robotic therapy on motor impairment and recovery in chronic stroke. Arch Phys Med Rehabil 84:477–482
Fedirchuk B, Nielsen J, Petersen N, Hultborn H (1998) Pharmacologically evoked fictive motor patterns in the acutely spinalized marmoset monkey (Callithrix jacchus). Exp Brain Res 122:351–361
Franklin DW, So U, Burdet E, Kawato M (2007) Visual feedback is not necessary for the learning of novel dynamics. PLoS One 2:e1336
Goldberg EJ, Requejo PS, Fowler E.G (2009) Joint moment contributions to swing phase knee extension acceleration during gait in children with spastic hemiplegic cerebral palsy. J Biomech (in press)
Grasso R, Ivanenko YP, Zago M, Molinari M, Scivoletto G, Lacquaniti F (2004) Recovery of forward stepping in spinal cord injured patients does not transfer to untrained backward stepping. Exp Brain Res 157:377–382
Hesse S, Uhlenbrock D (2000) A mechanized gait trainer for restoration of gait. J Rehabil Res Dev 37:701–708
Hornby TG, Campbell DD, Kahn JH, Demott T, Moore JL, Roth HR (2008) Enhanced gait-related improvements after therapist- versus robotic-assisted locomotor training in subjects with chronic stroke: a randomized controlled study. Stroke 39:1786–1792
Husemann B, Muller F, Krewer C, Heller S, Koenig E (2007) Effects of locomotion training with assistance of a robot-driven gait orthosis in hemiparetic patients after stroke: a randomized controlled pilot study. Stroke 38:349–354
Hwang EJ, Smith MA, Shadmehr R (2006) Adaptation and generalization in acceleration-dependent force fields. Exp Brain Res 169:496–506
Ivanenko YP, Poppele RE, Lacquaniti F (2009) Distributed neural networks for controlling human locomotion: lessons from normal and SCI subjects. Brain Res Bull 78:13–21
Kagerer FA, Contreras-Vidal JL, Stelmach GE (1997) Adaptation to gradual as compared with sudden visuo-motor distortions. Exp Brain Res 115:557–561
Krakauer JW, Shadmehr R (2006) Consolidation of motor memory. Trends Neurosci 29:58–64
Krakauer JW, Ghez C, Ghilardi MF (2005) Adaptation to visuomotor transformations: consolidation, interference, and forgetting. J Neurosci 25:473–478
Krebs HI, Hogan N, Aisen ML, Volpe BT (1998) Robot-aided neurorehabilitation. IEEE Trans Rehabil Eng 6:75–87
Latash ML, Scholz JP, Schöner G (2007) Toward a new theory of motor synergies. Mot Control 11:275–307
Mayr A, Kofler M, Quirbach E, Matzak H, Frohlich K, Saltuari L (2007) Prospective, blinded, randomized crossover study of gait rehabilitation in stroke patients using the Lokomat gait orthosis. Neurorehabil Neural Repair 21:307–314
Morasso P (1981) Spatial control of arm movements. Exp Brain Res 42:223–227
Morris ME, Matyas TA, Bach TM, Goldie PA (1992) Electrogoniometric feedback: its effect on genu recurvatum in stroke. Arch Phys Med Rehabil 73:1147–1154
Morton SM, Bastian AJ (2003) Relative contributions of balance and voluntary leg-coordination deficits to cerebellar gait ataxia. J Neurophysiol 89:1844–1856
Morton SM, Bastian AJ (2006) Cerebellar contributions to locomotor adaptations during splitbelt treadmill walking. J Neurosci 26:9107–9116
O’Rourke J (1994) Computational Geometry in C. Cambridge University Press, New York
Patton JL, Stoykov ME, Kovic M, Mussa-Ivaldi FA (2006) Evaluation of robotic training forces that either enhance or reduce error in chronic hemiparetic stroke survivors. Exp Brain Res 168:368–383
Perry J (1992) Gait analysis: normal and pathological function. Slack Incorporated, Thorofare
Perry J, Garrett M, Gronley JK, Mulroy SJ (1995) Classification of walking handicap in the stroke population. Stroke 26:982–989
Pohl M, Werner C, Holzgraefe M, Kroczek G, Mehrholz J, Wingendorf I, Hoolig G, Koch R, Hesse S (2007) Repetitive locomotor training and physiotherapy improve walking and basic activities of daily living after stroke: a single-blind, randomized multicentre trial (DEutsche GAngtrainerStudie, DEGAS). Clin Rehabil 21:17–27
Reinkensmeyer DJ, Kahn LE, Averbuch M, McKenna-Cole A, Schmit BD, Rymer WZ (2000) Understanding and treating arm movement impairment after chronic brain injury: progress with the ARM guide. J Rehabil Res Dev 37:653–662
Reisman DS, Block HJ, Bastian AJ (2005) Interlimb coordination during locomotion: what can be adapted and stored? J Neurophysiol 94:2403–2415
Reisman DS, Wityk R, Silver K, Bastian AJ (2007) Locomotor adaptation on a split-belt treadmill can improve walking symmetry post-stroke. Brain 130:1861–1872
Reisman DS, Wityk R, Silver K, Bastian AJ (2009) Split-belt treadmill adaptation transfers to overground walking in persons poststroke. Neurorehabil Neural Repair 23:735–744
Scheidt RA, Conditt MA, Secco EL, Mussa-Ivaldi FA (2005) Interaction of visual and proprioceptive feedback during adaptation of human reaching movements. J Neurophysiol 93:3200–3213
Schmidt RA (1988) Motor control and learning: a behavioral emphasis. Human Kinetics Publishers Inc, Champaign
Scholz JP, Schoner G, Latash ML (2000) Identifying the control structure of multijoint coordination during pistol shooting. Exp Brain Res 135:382–404
Shadmehr R, Holcomb HH (1997) Neural correlates of motor memory consolidation. Science 277:821–825
Shadmehr R, Krakauer JW (2008) A computational neuroanatomy for motor control. Exp Brain Res 185:359–381
Shadmehr R, Moussavi ZM (2000) Spatial generalization from learning dynamics of reaching movements. J Neurosci 20:7807–7815
Shadmehr R, Mussa-Ivaldi FA (1994) Adaptive representation of dynamics during learning of a motor task. J Neurosci 14:3208–3224
Stein J, Krebs HI, Frontera WR, Fasoli SE, Hughes R, Hogan N (2004) Comparison of two techniques of robot-aided upper limb exercise training after stroke. Am J Phys Med Rehabil 83:720–728
Teasell RW, Bhogal SK, Foley NC, Speechley MR (2003) Gait retraining post stroke. Topic Stroke Rehabil 10:34–65
Tong C, Wolpert DM, Flanagan JR (2002) Kinematics and dynamics are not represented independently in motor working memory: evidence from an interference study. J Neurosci 22:1108–1113
Tong RK, Ng MF, Li LS (2006) Effectiveness of gait training using an electromechanical gait trainer, with and without functional electric stimulation, in subacute stroke: a randomized controlled trial. Arch Phys Med Rehabil 87:1298–1304
Winstein CJ (1991) Knowledge of results and motor learning–implications for physical therapy. Phys Ther 71:140–149
Yanagihara D, Kondo I (1996) Nitric oxide plays a key role in adaptive control of locomotion in cat. Proc Natl Acad Sci USA 93:13292–13297
Acknowledgments
The authors are grateful to the National Center for Medical Rehabilitation Research, Grant HD38582 for support of this work. The authors also acknowledge the earlier assistance of Dr. Wei-Li Hsu, National Taiwan University, on the initial pilot experiments.
Author information
Authors and Affiliations
Corresponding author
Additional information
An erratum to this article can be found at http://dx.doi.org/10.1007/s00221-010-2238-y
Rights and permissions
About this article
Cite this article
Kim, S.H., Banala, S.K., Brackbill, E.A. et al. Robot-assisted modifications of gait in healthy individuals. Exp Brain Res 202, 809–824 (2010). https://doi.org/10.1007/s00221-010-2187-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-010-2187-5