
Abstract
Reweighting to multisensory inputs adaptively contributes to stable and flexible upright stance control. However, few studies have examined how early a child develops multisensory reweighting ability, or how this ability develops through childhood. The purpose of the study was to characterize a developmental landscape of multisensory reweighting for upright postural control in children 4–10 years of age. Children were presented with simultaneous small-amplitude somatosensory and visual environmental movement at 0.28 and 0.2 Hz, respectively, within five conditions that independently varied the amplitude of the stimuli. The primary measure was body sway amplitude relative to each stimulus: touch gain and vision gain. We found that children can reweight to multisensory inputs from 4 years on. Specifically, intra-modal reweighting was exhibited by children as young as 4 years of age; however, inter-modal reweighting was only observed in the older children. The amount of reweighting increased with age indicating development of a better adaptive ability. Our results rigorously demonstrate the development of simultaneous reweighting to two sensory inputs for postural control in children. The present results provide further evidence that the development of multisensory reweighting contributes to more stable and flexible control of upright stance, which ultimately serves as the foundation for functional behaviors such as locomotion and reaching.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Children, like adults, use information from multiple sensory systems to maintain their upright posture. Studies on postural development have shown age-related changes in the use of vision to control posture in infants (Bertenthal and Bai 1989, 1997; Foster et al. 1996; Lee and Aronson 1974) and in children (Foster et al. 1996; Kim 2004; Schmuckler 1997). Similarly, studies have demonstrated age-related trends in postural development when somatosensory inputs are manipulated in infants (Barela et al. 1999; Metcalfe and Clark 2000; Metcalfe et al. 2005a, b) and in children (Barela et al. 2003). While the manipulation of single sensory inputs has contributed greatly to our understanding of postural control development in infants and children, far less is known about how multiple sensory inputs are integrated and used in postural development.
The importance of sensory “integration” to postural development was first recognized by Forssberg and Nashner in their 1982 seminal paper (Forssberg and Nashner 1982). Although the authors suggested that children below the age of 7.5 years were unable to adaptively ‘reweight’ multiple sensory inputs, few have followed up on this suggestion and those who have examined children’s postural responses to more than one sensory input have not employed experimental procedures that would permit systematic examination of sensory weighting or reweighting. A recent experimental technique, however, has been developed that resolves this problem by presenting simultaneous sinusoidal sensory inputs at different frequencies and with differing amplitudes revealing the system’s ability to reweight sensory input dependent on input amplitude (Oie et al. 2002;Allison et al. 2006). The present study uses this technique to examine how early a child develops multisensory reweighting ability and how this ability develops through childhood. We tested children 4–10 years old to quantitatively characterize a “developmental landscape” of multisensory integration for postural control.
Previous studies that have explored postural control by varying a single sensory input (e.g., vision or somatosensory inputs) have shown that postural control develops gradually and improves with increased motor experience. Infants sway or even fall backwards with an approaching visual scene in early sitting (Bertenthal and Bai 1989) or standing (Lee and Aronson 1974). With increased experience in sitting and standing, children are less likely to fall, exhibit directionally appropriate postural responses and sway less than infants (Foster et al. 1996). When the visual scene oscillates, infants respond to the motion more consistently with increased age (Bertenthal and Bai 1997), while 3- to 6-year-old children exhibit a phase lag that increases with driving frequency (Schmuckler 1997). For 4- to 8-year-old children lightly touching an oscillating surface with their finger tip, phase lag also increases with frequency and gain (sway amplitude divided by stimulus amplitude) exhibits a peak at intermediate frequencies (Barela et al. 2003).
The pattern of gain and phase across frequency in these latter two studies is qualitatively similar to adults. However, such a pattern does not necessarily indicate an adult-like ability to adapt to multisensory information. Even in a linear non-adaptive system, gain and phase change with stimulus frequency (Glad and Ljung 2000). Therefore, varying stimulus frequency does not directly probe the critical ability to adaptively reweight different sensory modalities when sensory conditions change. A more direct way of studying sensory reweighting is by measuring gain changes across different stimulus amplitudes at the same frequency. Such amplitude-dependent gain changes indicate some type of nonlinearity, for example, adaptation. In adults, amplitude-dependent gain changes have been reported for visual scene motion (Peterka and Benolken 1995) and have been reproduced in models with sensory reweighting (Carver et al. 2005; van der Kooij et al. 2001). This amplitude-dependent gain change has important functional significance. If stimulus amplitude is too large, the postural system needs to downweight this information. Likewise, if individuals were to remain strongly coupled to a visual scene whose amplitude increased, they might sway too much or potentially fall. In other words, a constant gain to a change in stimulus amplitude is non-adaptive for a control system.
To our knowledge, only one study has reported similar amplitude-dependent gain changes to systematically manipulated changes in sinusoidal visual input in 4- and 6-year-old children (Kim 2004). In children, we hypothesize, as did Forssberg and Nashner (1982), that improvements in postural control with development may be due in part to increases in sensory reweighting. For example, the fact that children fall less often than infants in a visual moving room (Foster et al. 1996) may be because they more effectively downweight visual information when the room begins to move, something that the infants are not able to do (Lee and Aronson 1974).
Individuals are confronted with multiple sensory changes in everyday life. A change in one sensory modality does not always correspond to changes in other sensory modalities. For example, when standing on a sandy shoreline watching trees blown by the breeze, wave action determines how fast the sand is washed away under your feet (and how much somatosensory information changes) whereas wind speed determines how much visual information changes produced by the movements of leaves. Ambiguity may occur because of incongruent sensory information from different sources (e.g. waves and leaves do not move in synchronization). Nevertheless, the central nervous system has the ability to integrate multisensory information adaptively to solve the ambiguity produced by physical stimuli and to establish a coherent internal percept. This multisensory fusion ability has been proposed to be critical for postural control (Jeka et al. 2000; Peterka 2002).
In adults, multisensory reweighting in posture control has been studied by Oie et al. using a paradigm that systematically manipulates the amplitudes of simultaneous visual scene and touch bar oscillations across trials (Oie et al. 2002). Gain to each individual sensory modality depends not only on that specific modality’s amplitude but also on the amplitude of the other simultaneously presented modality. For example, the dependence of vision gain on visual movement amplitude is interpreted as intra-modal reweighting; whereas the dependence of vision gain on touch bar amplitude is interpreted as inter-modal reweighting. Analogously, the dependence of touch gain on touch bar movement is interpreted as intra-modal reweighting, whereas the dependence of touch gain on visual movement amplitude is interpreted as inter-modal reweighting. In children, Foster et al. (1996) proposed that the inability to switch from an unreliable to a reliable source of perceptual information may explain why young infants fall more frequently than older children in the visual moving room. However, there are no studies that report sensory weights when two sensory inputs are simultaneously oscillating. In summary, currently there is only limited evidence demonstrating that children reweight to sensory input amplitude adaptively for postural control. Moreover, the evidence is limited to a single sensory modality, vision (Kim 2004).
In this study, we implement the same protocol as Oie et al. (2002) with children 4–10 years of age. The purpose is to characterize the development of multisensory reweighting for postural control. Specifically, we ask these questions: (1) Do children reweight to multiple sensory inputs? (2) Do children exhibit both intra- and inter-modal reweighting to two simultaneously oscillating sensory inputs? (3) Does reweighting increase with age?
Method
Subjects
Forty-one typically developing children (20 girls and 21 boys) were recruited to participate in this study. Their age ranged from 4.2 to10.8 years old with a mean age of 7.5 years. The age of the participants was distributed evenly across the age range (see data distribution along age axis in Fig. 4). All subjects were given oral instructions and explanations. Both an informed consent and videotaping agreements were signed by parents. The guidelines approved by the Internal Review Board at the University of Maryland were followed. Each child was tested on Movement Assessment Battery for Children (MABC) (Henderson and Sugden 1992) to screen their current motor ability in manual dexterity, ball skills and balance for participation eligibility. Subjects with MABC below twentieth percentile were excluded from the study.
Task and experimental setup
Children assumed a modified semi-tandem (heel-to-toe) stance while quietly looking at a front screen with their right index finger lightly touching a bar (Fig. 1). Children choose which foot to be in front of the other and kept the inner edge of the front heel in the same sagittal plane of the inner edge of the rear foot. The same stance configuration was kept throughout the test after each child established a comfortable position. During quiet standing, children looked straight at a front screen 40 cm away with 100 random dots (0.2° × 0.2°) projection while the room illumination was dimmed. They also wore goggles to limit their visual range to approximately 100° high × 120° wide. Wearing goggles kept the screen edge from being visible. Subjects simultaneously maintained contact with the right index finger to a rigid bar level with their right hip. The touch bar is a 4.4 cm diameter, 45.7 cm long PVC convex surface that is “touchable” without being “graspable” by the children. To ensure the touch bar provided primarily sensory information, a threshold was set at 1 N vertical touch force to trigger an auditory alarm. Children were informed that the alarm would sound only if they pressed too heavily on the touch bar. They were instructed to maintain contact with the touch bar while reducing the applied force so that the alarm no longer sounded. Touch force time series were monitored during data acquisition to insure that the child’s finger contacted the touch bar throughout the trial. The trial was stopped if the child lifted the finger off the touch bar and the trial was repeated. Only a few children need one or two repeated trials due to the finger not touching the bar. Movement of the touch bar was controlled by a servo-motor.

Experimental set-up in which a child is performing the multisensory posture task (room illumination not dimmed for illustrative purposes; fewer dots are plotted for a clear view of child’s posture)
To test how children used visual and somatosensory (touch) information for their stance control, visual scene and touch bar positions were simultaneously oscillated during a trial. These will be referred to as “drives” hereafter because the postural response is driven by these sinusoidal oscillations. Specifically, the touch bar oscillation is referred to as the touch drive (Tdrive); and the visual scene oscillation is referred to as the visual drive (Vdrive). Postural sway was recorded by a 3D ultrasound position tracking system (Logitech, Inc). A tracking marker was attached to the back of subject’s head (occipital protuberance) and to the approximate center of mass (CM) (at the level of the fifth lumbar vertebra). A customized Lab View program was used to integrate data collection via National Instrument data acquisition board (PCI-MIO-16E-4) for kinematic postural sway, sensory drives (Tdrive and Vdrive), and applied touch force. Data were collected at a sampling rate of 50.33 Hz.
Experimental design
The experimental design was based on a previous study, which maintained constant amplitude sinusoidal motion for one modality while the amplitude of the other modality was systematically manipulated (Oie et al. 2002). This protocol investigates whether the postural response is sensitive to changes in the modality that changes amplitude as well as the modality that remains constant, which is interpreted as fusion of the two modalities.
Tdrive and Vdrive moved in the medio-lateral direction at 0.28 and 0.20 Hz, respectively. These two frequencies were chosen with an approximate ratio of √2 to avoid common low order harmonics. The five amplitude pairs constituting the test conditions were T8V2, T4V2, T2V2, T2V4 and T2V8. Subscripts indicate mean-to-peak amplitude in mm. For example, T8V2 means that Tdrive moves with amplitude of 8 mm while Vdrive simultaneously moves with amplitude of 2 mm. Each trial was 90 s long and each condition was repeated 3 times (total 15 trials). Trials were grouped into three blocks, each consisting of the five conditions in random order. Subjects were not informed that the drive amplitudes were being manipulated. Breaks were provided as the child requested (usually after 2–3 trials). The test lasted about 2.5 h and the child was paid a nominal sum for one visit to our laboratory.
Analysis
Pre-processing
Customized MatLab programs were implemented for data analysis. All raw signals were mean subtracted and filtered by a zero-phase digital filtering using filtfilt function in Matlab. A fourth order Butterworth filter with low pass frequency at 5 Hz was used to filter the signals in both the forward and reverse directions. Figure 2 shows the time series for two drives and CM postural sway for a T4V2 trial. Only medio-lateral postural sway is illustrated here and analyzed hereafter as this was the direction of the visual scene and touch bar motions.

Exemplar time series from the T4V2 condition in a 10-year old child. The touch bar oscillation (Tdrive) amplitude is 4 mm at 0.28 Hz. The visual scene oscillation (Vdrive) amplitude is 2 mm at 0.2 Hz. The middle trace is the medio-lateral postural response recorded at approximate center of mass (CMml). The three time series are offset vertically for illustrative purposes. Tdrive and Vdrive oscillate simultaneously and continuously in medio-lateral direction
Transfer functions (TFs) with gains and phases
The transfer function (TF) at the driving frequency was used to quantify the postural response to the drive. One TF is calculated for the postural sway recorded by each marker (head or CM) to each drive (Tdrive or Vdrive). The TF is a complex number that characterizes the response strength (gain) and the response timing (phase). Gain is calculated as the magnitude of the postural response divided by the magnitude of the drive. The phase describes the temporal relationship between postural sway and the drive. A positive phase indicates that the postural response leads the driving stimulus. The TF was computed for the last 75-s segment of the drive and sway signals using the Welch’s method with 25-s windows and 50% overlap. The first 15 s of the signal was not analyzed so as to exclude transient postural responses to the drives’ onset. The 25-s window was chosen because it is an integer multiple of the drives’ periods. TFs were averaged across the 3 trials for each subject and condition.
Statistical analysis
For all statistical tests, condition was treated as within-subject repeated factor, and age as inter-subject non-repeated factor; P < 0.05 was considered significant and P < 0.1 was considered marginally significant.
Nonlinear multivariate regression model
A separate nonlinear multivariate regression analysis was conducted for the postural response recorded from each marker (head and CM) to each drive (Tdrive and Vdrive). The nonlinear multivariate regression model was:
where n = 41 is the number of subjects, K = 5 is the number of conditions, a i is the age of the ith subject, and T ik is the TF of the ith subject in the kth condition. The TFs dependence on age and condition were described by group gain g k (a) and group phase ϕ k (a), the absolute value and argument of the mean TF in condition k at age a, respectively. We assumed that group gain and phase were polynomial functions of age:
where m is the regression order, g jk are gain coefficients, and ϕ jk are phase coefficients (j = 0,...,m and k = 1,...,K). For the ith subject, random variation of TFs is described by the vector v i = (δ i1, ..., δ iK , ε i1, ..., ε iK ) of random variables, which was assumed to come from a zero-mean multivariate normal distribution. The covariance of v i was assumed to be the same for all subjects.
An alternative approach to model (1) would be to regress the individual subject gains and phases directly on age. We chose the approach of model (1) because estimates of TFs are unbiased (Bendat and Piersol 2000), consistent with the way that random variation is specified in model (1). When true gain is low, gains estimated from individual subjects have a positive bias, which would lead to a bias in the fitted gain curves in the alternative approach. Also, the fact that phase is a circular variable (Fisher 1995) is naturally incorporated into model (1), but not the alternative approach. This distinction is important when phase values are not tightly clustered, as occurred in some cases in our data (Fig. 4b).
Model fitting and hypothesis testing
Statistical analysis of our data based on model (1) was performed using custom Matlab programs using the optimization and statistical toolboxes. Model (1) has 2K(m + 1) parameters: the gain coefficients g jk and the phase coefficients ϕ jk (j = 0, ...,m and k = 1, ...,K). Parameters were fit based on the empirical TFs by maximizing the model’s concentrated log-likelihood (Seber and Wild 2003). The fitted parameters were then used to compute the fitted gain and phase curves g k (a) and ϕ k (a) of Eqs. (2). The approximate standard errors of g k (a) and ϕ k (a) were computed as \( {\sqrt { - {\mathbf{w}}_{k} (a)^{T} D^{{ - 1}} {\mathbf{w}}_{k} (a)} }, \) where w k (a) is the gradient vector of g k (a) or ϕ k (a) with respect to model parameters and D is the matrix of second derivatives of the concentrated log-likelihood with respect to model parameters, evaluated at the fitted parameters.
To test a null hypothesis H about model parameters, we fit the model with parameters constrained by the null hypothesis. We then compared the maximum concentrated log-likelihood for the constrained model, M H , to the maximum concentrated log-likelihood of the unconstrained model, M, using either a likelihood ratio test applied to R = 2(M – M H ) (Seber and Wild 2003) or a F-test applied to Wilks’ Λ = exp(−R/n) (Seber 1984; Polit 1996). The F-test is somewhat more accurate, whereas the likelihood ratio test has the flexibility to test any null hypothesis.
Various hypotheses about the model were tested. First, regression orders m of 0, 1, 2 and 3 were compared using Wilks’ Λ. This comparison led to the selection of the model with m = 1 (gain and phase are linear functions of age) as appropriate for further analysis (see “Results”). Next, we tested the selected first order model for an overall dependence on condition to address our primary question whether children demonstrate reweighting across amplitude conditions.
To describe our data’s dependence on age and condition in more detail, we focused on the three conditions in which visual-scene and touch-bar motions were at their highest or lowest amplitudes: T8V2 , T2V2 and T2V8. Since gain and phase were modeled as linear functions of age, fitted lines for gain and phase could be fully specified by their end points at the minimum age (4.2 years) and maximum age (10.8 years) of our subjects. For each pair of conditions, we compared the fitted gain curves at both age ends. The following changes in gain between conditions were interpreted as reweighting. Intra-modal reweighting is an increase in touch gain from T8V2 to T2V2 or a decrease in vision gain from T2V2 to T2V8. Inter-modal reweighting is an increase in touch gain from T2V2 to T2V8 or a decrease in vision gain from T8V2 to T2V2. Total reweighting (sum of intra- and inter-modal reweighting) is an increase in touch gain or a decrease in vision gain from T8V2 to T2V8 (conditions between which stimulus amplitudes are most different). We tested for total reweighting because it increased our power to detect reweighting if both intra- and inter-modal reweighting were small. Given these interpretations, an increase (or decrease) of re-weighting with age corresponds to the gain difference between two conditions increasing (or decreasing) with age. We tested for such age-dependent reweighting for each pair of conditions by testing for an age-by-condition interaction.
In summary, nine tests involving gain were performed (three condition pairs compared at minimum age, at maximum age, and tested for an age-by-condition interaction). Tests were conducted using likelihood ratio tests and were based on model (1) reduced to three condition (K = 3). A closed testing procedure (Hochberg and Tamhane 1987) was used to adjust P-values to control the familywise Type I error rate for the nine tests. The same tests were also performed on phase.
Results
Exemplar: TFs, gains and phases from a 10-year-old child
Figure 3 shows the TFs, gains and phases from a 10-year-old child, illustrating the postural response distribution in the complex plane, and how gains and phases are extracted from TFs. As would be expected for segments higher up the kinematic chain, the postural response is larger for the head than for the CM. Transfer functions plotted for the head in Fig. 3a are further from the origin than those for the CM in Fig. 3d. Likewise, the head gains in Fig. 3b are larger than those for the CM in Fig. 3e.

Transfer functions (TFs), gains, and phases from a 10-year-old subject. Upper graphs a–c show responses of the head to the touch and visual drives. Lower graphs d–f show responses of the approximate center of mass (CM) to the drives. In a and d, the average TFs across the three trials are shown in the complex plane. The length of the line from each TF to the origin (denoted as multisign) represents the gain (plotted in b and e). Phase is the angle between this line and the positive real axis (plotted in c and f). Postural response is larger for the head than for the CM. This shows in the TFs (greater distances from the origin in a than d) and in gain (larger values in b than e). Both intra- and inter-modal reweighting patterns are observed for head (b) and CM (e)
Gains across conditions for each modality are not constant, indicating both intra-modality and inter-modal reweighting. Intra-modal reweighting is signified by an increase in touch gain from T8V2 to T2V2; and a decrease in vision gain from T2V2 to T2V8. Inter-modal reweighting is signified by an increase in touch gain from T2V2 to T2V8; and a decrease in vision gain from T8V2 to T2V2. Thus, both intra- and inter-modal reweighting patterns were observed in this child. Phase was relatively constant across conditions (Fig. 3c, d).
Fitted gain and phase curves
For each marker (head and CM) and modality (touch and vision), we modeled gain and phase as being either constant, linear functions of age, quadratic functions of age, or cubic functions of age (Eqs. 2 with m = 0, ...,3). For each model, we simultaneously fit gain and phase curves using the TFs from all five conditions (see “Method”). Figure 4 shows an example of one such model fit. Here linear gain and phase functions were fit based on head touch TFs from each subject and condition. The individual gains and phases shown in Fig. 4 were computed from these TFs.

Gains and phases from all individual subjects with fitted gain lines and fitted phase lines from head response to touch input. In upper row, each graph illustrates the gains from the 41 individual subjects and fitted gain lines with associated standard error. Similar plots for phase are illustrated in lower row. Graphs in each column are for the indicated condition. These fitted gain lines and fitted phase lines (total 10 lines) were simultaneously fitted using a multivariate statistical model. Note that the phases in our data were not always tightly clustered
For each marker and modality, the linear model fit the data significantly better than the constant model, indicating that postural responses changed with age (head touch: Wilks’ Λ( = 0.49, F 10,30 = 3.08, P = 0.008; head vision: Λ( = 0.47, F 10,30 = 3.32, P = 0.005; CM touch: Λ( = 0.41, F 10,30 = 4.26, P = 0.001; CM vision: Λ( = 0.52, F 10,30 = 2.76, P = 0.015). Also, the quadratic and cubic models were not significantly better than the linear model (P > 0.05). Therefore, we conclude that the model with linear gain and phase functions provides an adequate description of age-dependent changes for our data set. Condition effects were highly significant for this model (head touch: Λ( = 0.16, F 16,64 = 6.06, P < 0.0001; head vision: Λ( = 0.09, F 16,64 = 9.17, P < 0.0001; CM touch: Λ( = 0.08, F 16,64 = 10.07, P < 0.0001; CM vision: Λ( = 0.11, F 16,64 = 8.15, P < 0.0001).
Gain
Since gain and phase were modeled as linear functions of age, each fitted line in Fig. 4 is completely specified by its endpoint values at the minimum age (4.2 years) and maximum age (10.8 years) of our subjects. For the five fitted gain lines, these endpoint values are plotted in Fig. 5a. Thus, Fig. 5a is simply a concise way of representing the five fitted gain lines of Fig. 4. Since they come from fitted gain lines, each gain value in Fig. 5a is based on the TFs of all subjects. Along with touch gain for the head, Fig. 5 also uses endpoint values to specify the linear fitted gain curves for vision gain for the head, touch gain for the CM, and vision gain for the CM. In what follows we will refer to Fig. 5 when testing certain hypotheses concerning gain. It is important to remember that each statement concerning Fig. 5 corresponds to an equivalent statement about the fitted gain lines. For example, testing whether fitted gain values for two conditions are the same at the minimum age is equivalent to testing whether the corresponding two fitted gain lines intersect at minimum age. Also, testing whether an age-by-condition interaction exists for two conditions is equivalent to testing whether the slopes of the two fitted gain curves are different.

Fitted gains at minimum and maximum ages. From each graph in Fig. 4, the fitted gains with associated standard errors at age endpoints are extracted from the corresponding fitted lines. Fitted gains from 5 conditions are plotted in the a to summarize intra-, inter-modal and total reweighting of head touch gains. Similarly, fitted gains for other marker and modality are extracted and plotted in b, c, d. To summarize, a is the fitted touch gain for head for minimum age (open triangle) and maximum age (filled triangle). b is the fitted vision gain for head for minimum age (open circle) and maximum age (filled circle). Similarly, fitted touch gain for CM is plotted in c, and fitted vision gain for CM in (D). * indicates significant condition effect (***** for p < 0.0001, **** for p < 0.001, *** for p < 0.01, ** for p < 0.05, and * for marginal significance with p < 0.1). The solid bracket symbol indicates which two conditions are being compared. For example, the larger solid bracket is for the total reweighting between T8V2, and T2V8. The smaller bracket is for T8V2 & T2V2 condition pair, or T2V2 & T2V8 condition pair. Symbols associated with the brackets are to indicate fitted touch gain at minimal age (open triangle), fitted touch gain at maximal age (filled triangle), fitted vision gain at minimal age (open circle) and fitted vision gain at maximal age (filled circle). The age-by-condition interaction is indicated by a bracket symbol with the text (By Age)
Interpreting gain changes across conditions as reweighting
If subjects reweight sensory modalities across conditions, we expect touch gain (Fig. 5a, c) to increase from left to right, since touch should be downweighted when the touch amplitude increases (intra-modal reweighting) and upweighted when the visual amplitude increases (inter-modal reweighting). Similarly, we expect vision gain (Fig. 5b, d) to decrease from left to right. To check whether the condition dependence matched these expected patterns for reweighting, we made pair wise comparisons between conditions at the minimum and maximum ages. For touch gain, we defined intra-modal reweighting as an increase in gain from T8V2 to T2V2, inter-modal reweighting as an increase in gain from T2V2 to T2V8, and total (sum of intra- and inter-modal) reweighting as an increase in gain from T8V2 to T2V8. For vision gain, we defined reweighting in the analogous way. Using these pair wise comparisons, we tested for each type of reweighting at both the minimum and maximum age. We also tested whether the amount of reweighting changed across age by testing for age-by-condition interactions.
Touch gain (Fig. 5a, c) shows evidence of total and intra-modal reweighting. Total reweighting is significant at both age endpoints for the head and the CM (P < 0.05 for head and P < 0.01 for CM at minimum; P < 0.001 for head and P < 0.0001 for CM at maximum). Intra-modal reweighting is significant only at the maximum age (P < 0.0001 for head; P < 0.001 for CM) with a significant age-by-condition interaction for head (P < 0.05). There is no evidence of inter-modal reweighting for touch gain either for the head or the CM. Vision gain (Fig. 5b, d) shows evidence of total reweighting and both intra- and inter-modal reweighting. Total reweighting is significant at both age endpoints for the head and the CM (P < 0.001 for head and P < 0.05 for CM at minimum; P < 0.0001 at maximum for both head and CM). Total reweighting for CM shows a significant age-by-condition interaction (P < 0.01). This indicates that even though total reweighting is demonstrated at both the youngest and oldest age between the CM and the Vdrive, the amount of total reweighting increases with age. Intra-modal reweighting is significant at both age endpoints for the head and CM (all P < 0.0001) with a marginally significant age-by-condition interaction for CM (P < 0.1). As for the inter-modal reweighting, it is only significant at the maximum age (P < 0.1 for head and P < 0.01 for CM) with a significant age-by-condition interaction for CM (P < 0.05). Because the age-by-condition interaction for inter-modal reweighting is not significant for head, multiple interpretations are provided (see “Discussion”).
Phase
Generally, changes in phase across conditions are in the opposite direction of predicted changes in gain (see “Interpreting gain changes across conditions as reweighting”). For all significant changes in touch phase, phase decreases from left to right (Fig. 6a, c). Analogously, for all significant changes in vision phase, phase increases from left to right (Fig. 6b, d). Specifically, at maximum age touch phase decreases from left to right (Fig. 6a, c), while touch gain increases (Fig. 5a, c) across total and intra-modal reweighting conditions (P < 0.01 for head, P < 0.001 for CM). Touch phase does not depend significantly on condition at minimum age. The condition dependence of touch phase generally increases with age, supported by a significant age-by-condition interactions (P < 0.05 for intra-modal conditions for head and CM and total reweighting conditions for CM). The vision phase of head increases from left to right across total reweighting conditions (P < 0.1) and inter-modal reweighting conditions (P < 0.05) at minimum age (Fig. 6b). Vision phase for CM (Fig. 6d) shows a marginally significant increase from left to right across total reweighting conditions at maximum age (P < 0.1).

Discussion
We implemented a multisensory paradigm with simultaneously oscillating visual scene and touch bar to characterize the developmental profile of adaptive multisensory reweighting in children. We found that children even as young as 4 years old can reweight to multisensory inputs. Specifically, intra-modal reweighting was exhibited by children as young as 4 years of age; however, inter-modal reweighting was only observed in the older children. Inter-modal reweighting is interpreted as the adaptive fusion of two sensory modalities, because the postural response to one modality depends on the amplitude of the other modality (Oie et al. 2002). For example, from condition T8V2 to T2V2, the vision gain in older children decreased even though the visual scene amplitude remained constant, indicating the adaptive fusion of touch and vision inputs. Thus, it is suggested that fusing sensory information from different modalities may be a key ingredient of flexible, adult-like control of upright stance. Moreover, we also found that the amount of reweighting increased with age indicating development of a better adaptive ability.
Does inter-modal reweighting develop later in childhood?
Our results show that children from 4 to 10 years old demonstrate reweighting to both sensory inputs between conditions when stimulus amplitudes are most different (i.e. T8V2 to T2V8). We provide direct evidence confirming Forssberg and Nashner’s (1982) suggestion on the role of sensory reweighting for the development of postural control. Moreover, we show that children as young as 4 years old can reweight to multisensory inputs, which is lower than the age of 7.5 years that Forssberg and Nashner reported. Furthermore, we found a developmental difference for different modes of reweighting. Specifically, there is evidence of intra-modal reweighting for children 4–10 years old. However, no touch inter-modal reweighting was observed. A previous study using the same protocol with young adults also did not show significant touch inter-modal reweighting (Oie et al. 2002). As for vision inter-modal reweighting, it was only observed in older children. We propose two possibilities for the development of vision inter-modal reweighting. One possibility is that the two reweighting modes may not develop concurrently; inter-modal reweighting may develop only later in childhood. It may be that younger children can reweight adaptively to sensory inputs, but they adapt less optimally, emphasizing a developmental process. A second possibility is that the two reweighting modes (intra- and inter-) develop concurrently but inter-modal reweighting in younger children is less detectable due to its smaller effect size.
Unlike gain, our reweighting hypothesis makes no specific predictions about phase. However, our results show a consistent pattern of condition dependence for both touch and vision phase. Specifically, phase decreases across conditions where gain is expected to increase. This condition dependence of phase was not reported in adults using the same protocol (Oie et al. 2002). However, a similar pattern of phase increasing while gain decreases was reported with an oscillating-translational visual display movement in young adults (Ravaioli et al. 2005) and the elderly (Jeka et al. 2006). The source of this phase dependency on condition, which indicates a nonlinear process, is unknown (Ravaioli et al. 2005; Jeka et al. 2006).
Developmentally, the condition dependence of touch phase increases with age and is only significant at the maximum age. Like gain, this may indicate that the condition dependence is either absent or small at the minimum age. Metcalfe et al. (2005) showed that infants 1 month before to 9 months after walking onset, when touching an oscillating surface with their hand, show increased temporal consistency between touch bar movement and postural sway. If the touch phase is more variable for younger children in the present multisensory paradigm as it is more variable for younger infants in the touch bar movement paradigm, then the high phase variability at a younger age may make the condition dependence less likely to be detected.
Multisensory reweighting increases with age in children
Children’s multisensory ability for postural control has been conceptualized in different ways. For example, visual dominance has been proposed as the mechanism through which young children resolve sensory conflict (Shumway-Cook and Woollacott 1985; Woollacott et al. 1987). Comparing support surface perturbations with eyes open and closed, these authors found postural responses to be far more variable without vision. They concluded that vision is dominant in early childhood, with 4 to 6 years being a transitional age. Children then develop more adult-like dependence on multiple sources of sensory information after this transitional period (Shumway-Cook and Woollacott 1985; Woollacott et al. 1987).
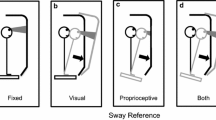
The contrasting view emphasizes “sensory integration” rather than the dominance of any particular modality (Forssberg and Nashner 1982). However, very few studies have quantified “sensory integration” in children. One such study used the Sensory Organization Test (SOT) to examine children’s ability to integrate multiple sensory inputs for postural control (Foudriat et al. 1993). In the SOT, a subject stands on a surface that is either fixed or rotates to maintain the body angle constant with respect to surface as the subject sways, a technique called sway-referencing that makes ankle proprioception unreliable. The visual surround can be sway-referenced as well. The most difficult SOT condition is when the support surface and visual scene are sway-referenced simultaneously, leaving primarily vestibular information for the estimation of body dynamics. Children as young as 3 years old are capable of keeping balance when the support surface and visual surround are sway-referenced. Their performance improves with age and the development rate is context specific, i.e. development rate differs for each condition in the SOT, with the visual and support surface sway referencing condition improving more slowly than other less-challenging conditions.
Even though Foudriat et al. (1993) provided important information on postural development, the SOT is not designed to quantify the sensory fusion process. It quantifies decrements in performance when sensory information is attenuated. In this study, we show that children reweight to both touch bar and visual display movements even at the minimum age (4.2 years old), but such reweighting is primarily intra-modal. At the oldest age (10.8 years old), children also reweight in an inter-modal manner. The development of inter-modal reweighting with age is functionally important, suggesting that sensory information is now fused together and reflecting the reality that the stimulation rarely acts upon a single modality. As Lackner (1992, p. 308) states, “In virtually any terrestrial circumstance involving natural movements, changes in peripheral vestibular activity will be accompanied by changes in the activity of somatosensory, proprioceptive, visual and auditory receptors. Consequently, it is difficult to ferret out a specifically vestibular contribution to orientation.” Thus, older children are able to adjust sensory weights in response to changes both within and across modalities, suggesting a more integrated and mature internal model capable of flexibly downweighting unreliable sensory input and upweighting reliable input.
We view the visual dominance hypothesis as a special case of the reweighting hypothesis. The concept of visual dominance stems from early “visual capture” perceptual studies (e.g., Hay et al. 1965; Rock and Harris 1967). The current view, however, is that “visual dominance” is caused by a number of factors, including the forced decision design generally imposed in such studies as well as parameters influencing the salience of the stimuli (e.g., ambient light level, noise level). For example, the noise level of the visual and haptic modalities has been found to influence how multisensory information is integrated in a statistically optimal fashion (Ernst and Banks 2002). When visual noise level is high, haptic information determines the percept. Visual dominance only occurs when the variance associated with visual modality is lower than the variance associated with the haptic estimate.
A similar phenomenon exists in our protocol in which subjects attempt to estimate their self-motion based on the motion of sensory inputs. Lower gain is associated with larger amplitude which provides less reliable information about self-motion. Taking vision as an example, vision is downweighted when visual movement amplitude increases across conditions (e.g. from T2V2 to T2V8 condition), reflecting intra-modal reweighting. Vision is also downweighted in response to upweighted touch gain when touch bar movement decreases across conditions (e.g., from T8V2 to T2V2), reflecting inter-modal reweighting. Reweighting depends on the amplitudes of both sensory inputs and vision does not always dominate.
Amplitude-dependent gain changes reflect sensory reweighting
To interpret amplitude-dependent gain changes, we consider postural control as consisting of two processes: state estimation and control (Carver et al. 2005; Kiemel et al. 2002; Kuo 1995, 2005; van der Kooij et al. 1999, 2001). In state estimation (sensory fusion), an internal model and noisy sensory measurements are used to continually estimate relevant state variables (Kiemel et al. 2002) and adjust the sensory weights adaptively (Carver et al. 2005; van der Kooij et al. 2001). In the control process, the state estimates are used to specify appropriate motor commands to stabilize upright posture. Thus, two alternative interpretations for the observed amplitude-dependent gain changes exist. One is that they reflect changes in the control parameters. The second interpretation attributes the gain changes to sensory mechanisms.
In adults, Oie et al. (2002) used time series models to measure changes in sway dynamics across the same five sensory conditions used in this study. Finding little change in parameters associated with control, they concluded that changes in gain were most consistent with changes in sensory weights. Sensory reweighting in postural control has been modeled using adaptive control models by van der Kooij et al. (2001) and Carver et al. (2005). The latter model has been extended (Jeka et al. 2005) and shown to qualitatively reproduce both the intra- and inter-modal amplitude-dependent gain changes observed in this study. An alternative explanation for amplitude-dependent postural gain changes has been proposed by Mergner et al. (2003). They developed a model with thresholds in central sensory processing that reproduces observed gain changes when the amplitude of a force perturbation is varied. Further study is needed to determine if such central thresholds can also explain our observed intra- and inter-modal gain changes in response to sensory perturbations.
In children, we reason that new constraints posed by the gradually changing physical properties along the developmental time line can be solved by a mechanism similar to optimal control. However, the physical properties of each individual subject do not change across amplitude conditions in current study. Furthermore, the amplitude-dependent gain change occurs in a time scale much shorter than developmental time scale. It requires a more rapid adaptation mechanism, such as sensory reweighting, to account for the observed gain changes across amplitude conditions. In summary, we consider sensory reweighting (adaptive state estimation) rather than a change in control process a more plausible explanation for the observed amplitude-dependent gain change.
Conclusion
In summary, we conclude that adaptive multisensory reweighting exists in early childhood and it develops gradually. The increased reweighting with age supports a more adaptive reweighting mechanism in older children with the possibility that inter-modal reweighting develops later in childhood. Mature sensory reweighting uses information from all sensory modalities simultaneously, reflecting the fact that a change in one sensory input leads to changes in response to all sensory inputs. The challenge for the developing child is to distinguish changes that are externally generated from changes due to their own self-motion, requiring a sophisticated internal model that can predict the sensory consequences of self-motion. The present results provide further evidence that the development of multisensory reweighting is an important property of this internal model, leading to more stable and flexible control of upright stance, which ultimately serves as the foundation for functional behaviors such as locomotion and reaching.
Reference
Allison LK, Kiemel T, Jeka JJ (2006) Multisensory reweighting of vision and touch is intact in healthy and fall-prone older adults. Exp Brain Res 175:342–352
Barela JA, Jeka JJ, Clark JE (1999) The use of somatosensory information during the acquisition of independent upright stance. Infant Behav Dev 22:87–102
Barela JA, Jeka JJ, Clark JE (2003) Postural control in children—coupling to dynamic somatosensory information. Exp Brain Res 150:434–442
Bendat JS, Piersol AG (2000) Random data: analyis and measurement procedures. Wiley, New York
Bertenthal BI, Bai DL (1989) Infants’ sensitivity to optical flow for controlling posture. Dev Psychol 25:936–945
Bertenthal BI, Bai DL (1997) Perception-action coupling in the development of visual control of posture. J Exp Psychol Hum Percept Perform 23:1631–1643
Carver S, Kiemel T, van der Kooij H, Jeka JJ (2005) Comparing internal models of the dynamics of the visual environment. Biol Cybern 92:147–163
Ernst MO, Banks MS (2002) Humans integrate visual and haptic information in a statistically optimal fashion. Nature 415:429–433
Fisher NI (1995) Statistical analysis of circular data. Cambridge University Press, Cambridge
Forssberg H, Nashner LM (1982) Ontogenetic development of postural control in man: adaptation to altered support and visual conditions during stance. J Neurosci 2:545–552
Foster EC, Sveistrup H, Woollacott MH (1996) Transitions in visual proprioception: a cross-sectional developmental study of the effect of visual flow on postural control. J Motor Behav 28:101–112
Foudriat BA, Di Fabio RP, Anderson JH (1993) Sensory organization of balance responses in children 3–6 years of age: a normative study with diagnostic implications. Int J Pediatric Otorhinolaryngol 27:255–271
Glad T, Ljung L (2000) Control theory: multivariable and nonlinear methods. Taylor & Francis, London
Hay JC, Pick HL, Ikeda K (1965) Visual capture produced by prism spectacles. Psychon Sci 2:215–216
Henderson SE, Sugden D (1992) Movement Assessment Battery for Children. The Psychological Corporation, London
Hochberg Y, Tamhane AC (1987) Multiple comparison procedures. Wiley, New York
Jeka J, Oie KS, Kiemel T (2000) Multisensory information for human postural control: integrating touch and vision. Exp Brain Res 134:107–125
Jeka J, Carver S, Allison L, Kiemel T (2005) Dynamics of sensory reweighting: time scales, transient and asymptotic dynamics. IV Conference on Motor control MCC2005—from basic motor control to functional recovery, Sofia
Jeka J, Allison L, Saffer M, Zhang Y, Carver S, Kiemel T (2006) Sensory reweighting with translational visual stimuli in young and elderly adults: the role of state-dependent noise. Exp Brain Res 174:517–527
Kiemel T, Oie KS, Jeka JJ (2002) Multisensory fusion and the stochastic structure of postural sway. Biol Cybern 87:262–277
Kim S (2004) The use of vision in children’s postural control. Master Thesis, University of Maryland, College Park
Kuo AD (1995) An optimal-control model for analyzing human postural balance. IEEE Trans Biomed Eng 42:87–101
Kuo AD (2005) An optimal state estimation model of sensory integration in human postural balance. J Neural Eng 2:S235–S249
Lackner JR (1992) Multimodal and motor influences on orientation: implications for adapting to weightless and virtual environments. J Vestib Res 2:307–322
Lee DN, Aronson E (1974) Visual proprioceptive control of standing in human infants. Percept Psychophys 15:529–532
Mergner T, Maurer C, Peterka RJ (2003) A multisensory posture control model of human upright stance. Prog Brain Res 142:189–201
Metcalfe JS, Clark JE (2000) Somatosensory information affords the exploration of posture in newly walking infants and toddlers. Infant Behav Dev 23:391–405
Metcalfe JS, Chen LC, Chang TY, McDowell K, Jeka JJ, Clark JE (2005a) The temporal organization of posture changes during the first year of independent walking. Exp Brain Res 161:405–416
Metcalfe JS, McDowell K, Chang TY, Chen LC, Jeka JJ, Clark JE (2005b) Development of somatosensory-motor integration: an event-related analysis of infant posture in the first year of independent walking. Dev Psychobiol 46:19–35
Oie KS, Kiemel T, Jeka JJ (2002) Multisensory fusion: simultaneous re-weighting of vision and touch for the control of human posture. Cogn Brain Res 14:164–176
Peterka RJ, Benolken MS (1995) Role of somatosensory and vestibular cues in attenuating visually induced human postural sway. Exp Brain Res 105:101–110
Peterka RJ (2002) Sensorimotor integration in human postural control. J Neurophysiol 88:1097–1118
Polit DF (1996) Data analysis & statistics for nursing research. Appleton & Lange, Stamford
Ravaioli E, Oie KS, Kiemel T, Chiari L, Jeka JJ (2005) Nonlinear postural control in response to visual translation. Exp Brain Res 160:450–459
Rock I, Harris CS (1967) Vision and touch. Sci Am 216:96–104
Schmuckler MA (1997) Children’s postural sway in response to low- and high-frequency visual information for oscillation. J Exp Psychol Hum Percept Perform 23:528–545
Seber GAF (1984) Multivariate observations. Wiley, New York
Seber GAF, Wild CJ (2003) Nonlinear regression. Wiley-Interscience, Hoboken
Shumway-Cook A, Woollacott MH (1985) The growth of stability: postural control from a developmental perspective. J Motor Behav 17:131–147
van der Kooij H, Jacobs R, Koopman B, Grootenboer H (1999) A multisensory integration model of human stance control. Biol Cybern 80:299–308
van der Kooij H, Jacobs R, Koopman B, van der Helm F (2001) An adaptive model of sensory integration in a dynamic environment applied to human stance control. Biol Cybern 84:103–115
Woollacott MH, Debû B, Mowatt M (1987) Neuromuscular control of posture in the infant and child: is vision dominant? J Motor Behav 19:167–186
Acknowledgments
This project is supported by NIH HD42527 to Dr. Jane E. Clark and a scholarship from the Taiwan Ministry of Education to Woei-Nan Bair.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Bair, WN., Kiemel, T., Jeka, J.J. et al. Development of multisensory reweighting for posture control in children. Exp Brain Res 183, 435–446 (2007). https://doi.org/10.1007/s00221-007-1057-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00221-007-1057-2