
Abstract
Rationale
Galantamine (GAL), a reversible and competitive inhibitor of acetylcholinesterase, is used clinically in the treatment of Alzheimer's dementia. Some preclinical and clinical studies support the potential efficacy of cholinesterase inhibitors for smoking cessation, although their effects on the behavioral and physiological responses to nicotine have not been examined. The goal of this study was to characterize GAL's actions on multiple outcomes, including withdrawal severity and cognitive performance, as well as subjective and physiological responses to nicotine administered intravenously.
Methods
A total of 12 smokers participated in a double-blind, placebo-controlled, crossover study. Smokers had two 4-day treatment periods, assigned in random sequence, to GAL (8 mg/day) or placebo treatment. On day 4 of each treatment phase, smokers had an experimental session in which they received an intravenous (IV) dose of saline or 1 mg/70 kg nicotine, 1 h apart, in a random order.
Results
GAL attenuated the self-reported rating of “craving for cigarettes” and prevented decrements in performance in a Go/No-Go task. In response to IV nicotine, GAL treatment attenuated the self-report ratings of “like the drug effects,” “good drug effects,” “bad drug effects,” and “stimulated.”
Conclusions
These findings support the potential utility of GAL as a treatment for smoking cessation.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Despite the availability of effective pharmacotherapies (Fiore et al. 2008; Herman and Sofuoglu 2010), 70 to 90 % of smokers resume smoking within a year of treatment. Accordingly, development of novel and effective nicotine dependence pharmacotherapies continues to be an important goal. Given the critical role of nicotinic acetylcholine receptors (nAChR) in nicotine addiction (Miwa et al. 2011), it is not surprising that all first-line pharmacotherapies for nicotine addiction, including nicotine replacement therapy (NRT), bupropion, and varenicline, affect the nAChR. While NRTs are nonspecific agonists for the nAChR, varenicline is a partial agonist of alpha4beta2 and a full agonist of alpha7 nAChR (Mihalak et al. 2006; Rollema et al. 2007). Bupropion, in addition to being a weak inhibitor of dopamine and norephinephrine transporter, is an antagonist of alpha4beta2 and alpha7 nAChR (Damaj et al. 2004; Mooney and Sofuoglu 2006; Paterson 2009; Slemmer et al. 2000). Thus, nAChR is an important target in the development of new medications for nicotine addiction.
Acetylcholinesterase (AChE) inhibitors are a group of medications that enhance cholinergic transmission (Sofuoglu and Mooney 2009). AChE rapidly terminates the actions of acetylcholine (ACh), the endogenous ligand for the cholinergic receptors. Many AChE inhibitors, including tacrine, rivastigmine, donepezil, and galantamine (GAL), are clinically used as cognitive enhancers in the treatment of dementia and are being tested as treatments for traumatic brain injury (Silver et al. 2006), stimulant addiction (Sofuoglu and Mooney 2009), and neuropsychiatric conditions associated with cognitive deficits (Huang and Fu 2010). Cumulating evidence from clinical studies supports the potential efficacy of AChE inhibitors for the treatment of nicotine dependence. For example, in alcohol-dependent smokers, rivastigmine (Diehl et al. 2009) or GAL (Diehl et al. 2006) treatment was associated with reduced smoking behavior without providing any specific behavioral treatments for cigarette smoking. In spite of this limitation, these studies support the potential use of AChE inhibitors for the treatment of nicotine addiction.
The purpose of this study was to examine the potential utility of GAL for nicotine addiction. Of the currently available AChE inhibitors, GAL has a unique feature in that it acts as an allosteric potentiating ligand of nAChR in addition to inhibiting AChE, resulting in greater stimulation of the nAChR than the other AChE inhibitors (Schilstrom et al. 2007). Because of its additional nAChR-potentiating effects, we hypothesized that GAL could be more effective than other AChE inhibitors as a treatment for nicotine addiction. As a first step, we examined GAL's effects on withdrawal symptoms and sustained attention function, as well as subjective and physiological responses to pure nicotine administered via intravenous (IV) route. We hypothesized that the administration of GAL would result in an attenuated subjective response to IV nicotine, improved cognitive performance, and a reduced urge for smoking in abstinent smokers, similar to the effects of administration of partial or full nAChR agonists.
Materials and methods
Participants
Twelve nontreatment-seeking smokers (11 men and 1 woman) were recruited from the New Haven, Connecticut area. Seven additional smokers dropped out prior to study's completion due to noncompliance with the study procedures (n = 5) and possible adverse events, including diarrhea (n = 2) and nausea (n = 1); therefore, they were not included in the analyses. This sample of nontreatment-seeking smokers was comprised of African-Americans (n = 4), Caucasians (n = 5), and Hispanics (n = 3). The average age (SD) of the smokers was 37.2 (8.1). Participants smoked an average of 15.0 (6.2) cigarettes/day and had a Fagerstrom Test for Nicotine Dependence (Heatherton et al. 1991) score of 4.8 (2.3). The average baseline plasma cotinine levels were 269 ng/ml (192). Participants were not dependent on drugs or alcohol other than nicotine during the study, and all physical, laboratory, and psychiatric examinations were within normal limits. Before participating in the study, participants provided written signed consent. This study was approved by the VA Connecticut Healthcare System Human Subjects Subcommittee. Experimental sessions were conducted in the Biostudies Unit located at the VA Connecticut Healthcare System, and participants were paid for their participation, with bonus payment for compliance with nonsmoking and other study procedures.
Procedures
We utilized an outpatient randomized, double-blind, crossover study design. Following an adaptation session, smokers had two 4-day treatment periods, assigned in random sequence, to GAL (8 mg/day) or placebo (PLA) treatment. Each treatment period was separated by a washout period lasting a minimum of 4 days, long enough to minimize carryover effects from GAL, which has an elimination half-life of 7 h (Robinson and Plosker 2006).
On each of the first 3 days of the treatment periods, smokers had clinic visits twice daily to receive the study medications and to complete outcome measures. Starting at midnight on day 1, smokers were asked to stop smoking until the morning of day 4. Abstinence from smoking was verified with expired carbon monoxide (CO) (<10 parts per million). On day 4 of each treatment phase, smokers began an experimental session. First, smokers had an indwelling catheter placed in an antecubital vein. After baseline measures were collected, smokers received an oral dose of either GAL or placebo. One hour after the medication administration, when the peak plasma levels of GAL are expected, smokers received two randomly ordered injections of nicotine (1 mg/70 kg) or placebo. The injections were given at 60-min intervals to allow sufficient time for the physiological and subjective effects of nicotine to return to baseline levels. Our previous work demonstrated that this dose of nicotine produces robust physiological and subjective responses (Sofuoglu et al. 2005, 2006, 2009).
Drugs
Nicotine and GAL administration
Nicotine bitartrate was acquired from Interchem Corporation (Manchester, Connecticut). All nicotine samples were prepared by a research pharmacist at the VA CT Healthcare System. A total volume of 5 ml nicotine was injected intravenously over 60 s via a catheter located in a forearm vein. GAL immediate-release capsules, 8 mg/day, were administered in the clinic twice daily by the study nurse. The recommended initial dose is 8 mg/day, given in two divided daily doses, and the maintenance dose is 8–24 mg/day, with gradual titration of the doses.
Outcome measures
Our outcome measures assessed biochemical, physiological, subjective, and cognitive domains. Biochemical measures included CO and plasma cotinine levels. Expired CO and plasma cotinine concentrations were used to verify abstinence from smoking and to assess the amount of nicotine intake, respectively, (Benowitz et al. 2002). Plasma cotinine measurements were taken before study participation, and CO levels were obtained daily during each treatment phase. The physiological measures included systolic and diastolic blood pressures and heart rate, which were measured daily during medication treatment. Physiological measures were taken in the experimental sessions at 0, 1, 2, 3, 5, 8, 10, 15, 30, and 45 min in relation to saline or nicotine injections. The subjective measures included the Questionnaire on Smoking Urges-Brief (QSU-B), the Profile of Mood States (POMS), and the Drug Effects Questionnaire (DEQ). The QSU-B is a 10-item scale that was originally developed by Tiffany and Drobes (1991) (Cox et al. 2001). Smokers are asked how strongly they agree or disagree with items on a 7-point Likert scale. This scale has two factors: factor 1 reflects an urge to smoke for stimulation, and factor 2 reflects an urge to smoke to relieve negative mood and withdrawal (Cox et al. 2001). This scale has been found to be highly reliable and reflects levels of nicotine deprivation (Bell et al. 1999; Morgan et al. 1999). The POMS includes 65 items (rated on a scale from 0, “not at all,” to 4, “very much so” for the past 24 h) that make up six subscales: tension–anxiety, depression–dejection, anger–hostility, vigor–activity, fatigue–inertia, and confusion–bewilderment (McNair et al. 1971). The QSU-B and POMS were administered daily during each treatment phase, and on the test session, they were administered three times: at the beginning, 1 h after the medication treatment, and at the end of each experimental session. The DEQ was used to measure acute effects of IV nicotine and consisted of the following items: “feel drug strength,” “feel stimulated,” “like the drug effects,” “good drug effects,” “feel high,” “bad drug effects,” “feel down,” and “feel anxious.” Smokers rated each item on a 100-mm scale, from “not at all” to “extremely.” The DEQ was given at 1, 3, 5, 8, 10, 15, 30, and 45 min after saline or nicotine administration.
Cognitive performance was assessed with the Sustained Attention to Response Test (SART). The SART is a 225-trial Go/No-Go task (Robertson et al. 1997; Sofuoglu et al. 2008) that assesses the ability to withhold responses to an infrequently occurring target (No-Go trials). Reaction times (RTs) and errors on Go trials are also assessed. The SART was administered twice: on day 4 of each treatment period and 1 h after GAL or placebo administration. Because the effect of AChE inhibitors on sustained attention may be most pronounced at the end of the task (Tenovuo et al. 2009), we examined treatment effects over time. Data from one participant were excluded due to equipment malfunction, meaning that 11 participants were included in the analyses of SART data.
Data analysis
Study outcomes were analyzed with a mixed-effect repeated-measures crossover model using the Statistical Analysis System, version 9.1.3 (SAS Institute Inc. 2007). Each model included fixed main effect terms for treatment (placebo or GAL) and time of measurement (day in the study, time since treatment, or trial in task for the SART) as well as the interaction of these two effects. We also included a random effect for subject and a blocking factor for treatment sequence. For blood pressure, heart rate, and DEQ, multiple measurements were obtained following saline and nicotine injections under placebo or GAL treatment. For these outcomes, separate analyses were conducted, focusing on the main contrasts of interest—whether treatment (GAL vs. placebo) changes saline and nicotine responses. For the SART, we included a random effect for subject and session variables (first vs. second session). Analyses of errors (for both No-Go and Go trials) used repeated measures logistic regression (SAS PROC GLIMMIX), using maximum likelihood with adaptive quadrature estimation. Trial number was included as a continuous independent variable, and we tested the treatment by time interaction term. Trial was included as a continuous independent variable, and we tested the treatment by time interaction term; values of p < 0.05 were considered statistically significant, based on two-tailed tests, unless otherwise specified. Significant treatment or treatment-by-time interactions (p < 0.05) were followed up by post hoc comparisons of GAL relative to placebo. To account for multiple testing, statistical significance was set at p < 0.016 for these comparisons.
Results
Physiological responses to IV nicotine
Following nicotine administration, peak heart rate and blood pressure values were reached at 1 min and returned to baseline in approximately 15 min (Fig. 1). GAL treatment did not change the heart rate [treatment main effect; F(1,164) = 3.6; p > 0.05] or systolic blood pressure [treatment main effect; F(1,164) = 3.5; p > 0.05] responses to IV nicotine. GAL reduced the diastolic blood pressure response to nicotine [treatment main effect; F(1,164) = 4.4; p < 0.05]. No treatment effects were observed in response to saline for any of the outcomes (p > 0.05).

The average (with SEM) heart rate and systolic and diastolic pressures responses to saline or 1 mg/70 kg intravenous nicotine administration. The doses were given in random order, 60 min apart. Measurements were taken just before and 1, 2, 3, 5, 8, 10, 15, 25, and 45 min after dose delivery. Some of the time-point error bars are not shown for clarity
Subjective responses to IV nicotine
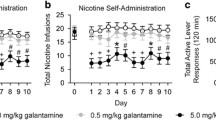
Following nicotine administration, peak subjective responses were reached at 1 min and returned close to baseline values within 15 min (Fig. 2). The treatment effects on the subjective responses to IV nicotine measured with DEQ are shown in Fig. 2. GAL reduced ratings of “stimulated” [treatment main effect; F(1,54) = 8.7; p < 0.001], “like the drug effects” [treatment main effect; F(1,120) = 4.9; p < 0.05], “good drug effects” [treatment main effect; F(1,120) = 5.7; p < 0.05], and “bad effects” [treatment main effect; F(1,120) = 4.5; p < 0.05]. The effect sizes for these DEQ items ranged from 0.8 to 1.1, a large effect as defined by Cohen (1988). There were no treatment effects for the rating of “feel drug strength,” “feel high,” “feel down,” or “feel anxious.” There was no treatment effect in response to saline administration.

The average (with SEM) selected subjective responses to saline or 1 mg/70 kg intravenous nicotine administration under placebo treatment. The doses were given in ascending order, 30 min apart. Measurements were taken at 1, 3, 5, 8, and 10 min after dose delivery. Some of the error bars are not shown for clarity
Brief questionnaire of smoking urges
Regarding the QSU‐B rating, no treatment effect was observed for factors 1 [treatment main effect; F(1,76) = 0.5; p > 0.05] and 2 [treatment main effect; F(1,76) = 1.4; p > 0.05]. For the experimental session, GAL treatment was associated with a lower rating for factor 1 [treatment main effect; F(1,54) = 4.5; p < 0.05], but not factor 2 of QSU-B. The average (SD) factor 1 scores of BQSU were 16.7 (9.2) at baseline, 16.5 (9.4) 1 h after medication treatment, and 16.4 (9.6) at the end of the session under placebo treatment. The corresponding values were 17.1 (8.5), 16.4 (8.3), and 15.6 (99.0) under GAL treatment (yielding an effect size of 0.82). There were no treatment effects on the POMS (p > 0.05).
Biochemical measures
For daily breath CO measurements, there were no significant main effects for treatment or treatment-by-time interaction (p > 0.05). Out of 72 CO assessments, there were a total of four CO levels that were >10 ppm: two under GAL and two under placebo conditions. All subjects had CO < 10 ppm at baseline on day 4, with average (SEM) CO levels of 4.6 (0.7) under placebo and 3.7 (0.8) under GAL treatment.
Cognitive measures
On No-Go trials, the mean error rate was 47.3 % (SD = 26.3 %) in the GAL condition, and 38.9 % (SD = 29.2 %) in the PLA condition. The error rate was significantly lower with GAL treatment [treatment main effect; F(1,535) = 4.88, p < .05]. The treatment-by-trial number interaction was also significant F(1,535) = 7.10, p < 0.01] and is illustrated in Fig. 3. The error rate on No-Go trials increased over time in the placebo condition [F(1,263) = 10.8, p < 0.01], but not in the GAL condition [F(1,263) = 0.03, p > 0.8]. On Go trials, in the GAL condition, the mean error rate was 4.5 % (SD = 5.6 %), and the mean RT was 421.2 ms (SD = 126.3 ms). In the PLA condition, the mean error rate was 4.6 % (SD = 4.9 %), and the mean RT was 429.3 ms (SD = 132.7 ms). There were no significant effects of treatment on Go trials (errors and RTs) (ps > 0.05). Order of drug condition (GAL first vs. PLA first) across the two sessions did not have any significant effects on any of the dependent variables (ps > 0.05).

Probability of error on No-Go trials in the SART by treatment condition and time (n = 11). As noted in the text, trial number was included as a continuous independent variable in the GLIMMIX analysis. For illustrative purposes, trials are grouped into nine bins in the figure. Each trial bin represents 25 trials (9 trial bins × 25 trials = 225 trials in total). For each assessment, the expected number of No-Go trials within each bin is 2.78 (25 divided by 9). We computed the probability of an error in each bin for each drug condition separately
Discussion
GAL treatment (8 mg/day for 4 days) attenuated some of the subjective responses to nicotine compared to placebo treatment. Furthermore, smokers reported reduced cravings for cigarettes and showed improved performance on the No-Go trials of a Go/No-Go task. GAL also reduced the increases in diastolic blood pressure induced by IV nicotine. Overall, GAL treatment was well tolerated by cigarette smokers during the 4-day treatment.
The effects of AChE inhibitors on nicotine reinforcement have not been well characterized. In a recent study, GAL produced partial generalization to nicotine's discriminative stimulus effect in rats (Giarola et al. 2010) similar to those observed for partial nAChR agonist cytisine or varenicline (LeSage et al. 2009). These findings are noteworthy, given that the subjective effect of drugs in humans can be modeled in animals through the use of discriminative stimuli (Smith and Stolerman 2009). In our study, GAL attenuated some, but not all, of the subjective effects of nicotine, including “like the drug effects,” “good drug effects,” “bad drug effects,” and “stimulated.” Pleasurable or hedonic effects from cigarettes before an attempt to quit smoking have been predictive characteristics of smoking relapse (Shiffman and Kirchner 2009; Strong et al. 2011). These studies suggest that medications targeting the pleasurable effects of smoking may facilitate quitting smoking. It remains to be determined if GAL also reduces the pleasurable effects of smoking cigarettes.
GAL treatment attenuated cigarette cravings in the experimental session without affecting the craving during the first 3 days of treatment. The reason for these discrepant findings is unclear, but could be due emergence of galantamine's effects following several days of treatment. Although our study did not assess smoking behavior, several studies support the potential effectiveness of AChE inhibitors for smoking cessation. In a 12-week clinical trial for the treatment of alcohol addiction that included 26 alcoholic smokers, rivastigmine treatment of 6 mg/day reduced the number of cigarettes smoked, the amount of exhaled carbon monoxide, and the craving for cigarettes (Diehl et al. 2009). In another clinical trial for alcohol dependence, GAL treatment reduced smoking behaviors, including cigarettes used per day, as well as cotinine levels in 114 alcohol-dependent smokers (Diehl et al. 2006). In a human laboratory study, 9 days of rivastigmine at a dose of 3 mg/day reduced the craving for cigarettes in 13 methamphetamine-dependent smokers; however, this effect was not statistically significant (De La Garza and Yoon 2011). Not all studies, examining AChE inhibitors in smokers, have been positive. A study with schizophrenic smokers reported that GAL was not beneficial for smoking behavior based on the Fagerstrom test for nicotine dependence scores and exhaled CO levels (Kelly et al. 2008). The study, however, did not have standard measures of smoking behavior, including cigarettes smoked per day or cotinine levels. It is important to note that these four studies did not use AChE inhibitors for the primary treatment of nicotine addiction. In fact, no specific behavioral treatments for cigarette smoking were provided.
In abstinent smokers, GAL treatment prevented the decline in performance on a Go/No-Go test, which is sensitive to sustained attention and response inhibition functions. Consistent with our findings, in previous studies, AChE inhibitors improved attention in individuals with mild cognitive impairment, traumatic brain injury and, more recently, cocaine addiction (Huang and Fu 2010; Silver et al. 2006; Sofuoglu et al. 2011). This study is the first to suggest that AChE inhibitors may also improve cognitive function in abstinent smokers. Our findings are consistent with a study in which GAL reversed the deficit in contextual conditioning induced by nicotine withdrawal in mice (Wilkinson and Gould 2011). Many studies have shown that nicotine abstinence is associated with decreased cognitive function, including difficulty concentrating, impairment of sustained attention, and poorer working memory efficiency in smokers (Ernst et al. 2001; Harrison et al. 2009; Jacobsen et al. 2005; Snyder and Henningfield 1989). Nicotine, especially in abstinent smokers, enhances several domains of cognition, including attention, working memory, and complex task performance (Baschnagel and Hawk 2008; Foulds et al. 1996; Heishman et al. 2010). The cognition-enhancing effects of nicotine may also contribute to the maintenance of nicotine addiction (Heishman et al. 2010). Improvement of cognitive function can be a potential treatment strategy for smokers trying to quit smoking. Conceivably, GAL and other similar medications may facilitate smoking cessation by improving cognitive deficits induced by abstinence. This hypothesis remains to be tested in future studies.
GAL's capacity to attenuate some of nicotine's acute subjective and physiological effects, while improving the sustained attention and cigarette craving in abstinent smokers, suggests that GAL may act like a nicotine agonist similar to NRT (Diehl et al. 2009). NRT, while reducing the acute subjective response to nicotine (Sobel et al. 2004), also alleviates withdrawal symptoms and improves cognitive performance during abstinence (Heishman et al. 2010). The evidence from preclinical studies also suggests an agonist-like effect with GAL. GAL produced a partial generalization to nicotine's discriminative stimulus effect in rats (Giarola et al. 2010). Furthermore, GAL reversed the deficit in contextual conditioning induced by nicotine withdrawal in mice (Wilkinson and Gould 2011). GAL acutely potentiates nicotinic currents induced by nAChR agonist such as ACh or nicotine in cell cultures (Schrattenholz et al. 1996). However, 4 days of exposure to GAL or nicotine reduced nicotine-induced dopamine and norepinephrine release in the cell cultures (Barik et al. 2005), possibly mediated by upregulation and/or desensitization of nAChR (Clarke et al. 1994; Di Angelantonio et al. 2004; Reid and Sabbagh 2008). These findings are consistent with the agonist effects of GAL on nAChRs and provide potential mechanisms of action for the proposed therapeutic effect of GAL on nicotine addiction.
Our study had several limitations. First, we used only one dose of GAL, 8 mg/day, which is lower than the usual clinical doses of GAL ranging from 8 to 24 mg/day. Second, the treatment duration was brief, only 4 days, and it is possible that longer treatment with GAL may produce different effects. Third, the cognitive assessment did not include a battery of tasks that are needed to better examine the cognitive effects of GAL in abstinent smokers. Lastly, the study had a small sample of mostly men and included multiple measurements of different domains, increasing the probability of type I errors. Given these limitations, the study findings should be regarded as preliminary, warranting future replication studies.
To summarize, GAL's capacity to attenuate nicotine's subjective effects and to improve cigarette craving and sustained attention function suggests that it may have therapeutic value for smoking cessation. Our findings are also supported by previous work conducted with other AChE inhibitors. Nicotine reward, reinforcement, withdrawal, and cognitive difficulties have been proposed as potential treatment targets to develop novel treatments for nicotine addiction. Further studies are warranted to test GAL's efficacy in smoking cessation.
References
Barik J, Dajas-Bailador F, Wonnacott S (2005) Cellular responses to nicotinic receptor activation are decreased after prolonged exposure to galantamine in human neuroblastoma cells. Br J Pharmacol 145:1084–1092
Baschnagel JS, Hawk LW Jr (2008) The effects of nicotine on the attentional modification of the acoustic startle response in nonsmokers. Psychopharmacology 198:93–101
Bell SL, Taylor RC, Singleton EG, Henningfield JE, Heishman SJ (1999) Smoking after nicotine deprivation enhances cognitive performance and decreases tobacco craving in drug abusers [in process citation]. Nicotine Tob Res 1:45–52
Benowitz NL, Jacob PI, Ahijevich K, Jarvis MJ, Hall S, LeHouzec J, Lichenstein E, Henningfield JE, Tsoh J, Hurt RD, Velicer W (2002) Biochemical verification of tobacco use and cessation. Report from the SRNT subcommittee on biochemical verification. Nicotine Tob Res 4:149–159
Clarke PB, Reuben M, el-Bizri H (1994) Blockade of nicotinic responses by physostigmine, tacrine and other cholinesterase inhibitors in rat striatum. Br J Pharmacol 111:695–702
Cohen J (1988) Statistical power analysis for the behavioral sciences, 2nd edn. L. Erlbaum Associates, Hillsdale
Cox LS, Tiffany ST, Christen AG (2001) Evaluation of the brief questionnaire of smoking urges (QSU-brief) in laboratory and clinical settings. Nicotine Tob Res 3:7–16
Damaj MI, Carroll FI, Eaton JB, Navarro HA, Blough BE, Mirza S, Lukas RJ, Martin BR (2004) Enantioselective effects of hydroxy metabolites of bupropion on behavior and on function of monoamine transporters and nicotinic receptors. Mol Pharmacol 66:675–682
De La Garza R 2nd, Yoon JH (2011) Evaluation of the effects of rivastigmine on cigarette smoking by methamphetamine-dependent volunteers. Prog Neuro-psychopharmacol Biol Psychiatry 35:1827–1830
Di Angelantonio S, Bernardi G, Mercuri NB (2004) Donepezil modulates nicotinic receptors of substantia nigra dopaminergic neurones. Br J Pharmacol 141:644–652
Diehl A, Nakovics H, Croissant B, Smolka MN, Batra A, Mann K (2006) Galantamine reduces smoking in alcohol-dependent patients: a randomized, placebo-controlled trial. Int J Clin Pharmacol Ther 44:614–622
Diehl A, Nakovics H, Mutschler J, Hermann D, Kiefer F (2009) Rivastigmine reduces tobacco craving in alcohol-dependent smokers. Pharmacopsychiatry 42:89–94
Ernst M, Heishman SJ, Spurgeon L, London ED (2001) Smoking history and nicotine effects on cognitive performance. Neuropsychopharmacol: Off Publ Am Coll Neuropsychopharmacol 25:313–319
Fiore MC, Jaen CR, Baker TB (2008) Treating tobacco use and dependence: 2008 update. Clinical practice guideline. U.S. Department of Health and Human Services, Rockville
Foulds J, Stapleton J, Swettenham J, Bell N, McSorley K, Russell MA (1996) Cognitive performance effects of subcutaneous nicotine in smokers and never-smokers. Psychopharmacol (Berl) 127:31–38
Giarola A, Auber A, Chiamulera C (2010) Acetylcholinesterase inhibitors partially generalize to nicotine discriminative stimulus effect in rats. Behav Pharmacol 22:1–6
Harrison EL, Coppola S, McKee SA (2009) Nicotine deprivation and trait impulsivity affect smokers' performance on cognitive tasks of inhibition and attention. Exp Clin Psychopharmacol 17:91–98
Heatherton TF, Kozlowski LT, Frecker RC, Fagerstrom KO (1991) The Fagerstrom test for nicotine dependence: a revision of the Fagerstrom tolerance questionnaire. Br J Addictions 86:1119–1127
Heishman SJ, Kleykamp BA, Singleton EG (2010) Meta-analysis of the acute effects of nicotine and smoking on human performance. Psychopharmacology 210:453–469
Herman AI, Sofuoglu M (2010) Comparison of available treatments for tobacco addiction. Curr Psychiatry Rep 12:433–440
Huang F, Fu Y (2010) A review of clinical pharmacokinetics and pharmacodynamics of galantamine, a reversible acetylcholinesterase inhibitor for the treatment of Alzheimer's disease, in healthy subjects and patients. Curr Clin Pharmacol 5:115–124
Jacobsen LK, Krystal JH, Mencl WE, Westerveld M, Frost SJ, Pugh KR (2005) Effects of smoking and smoking abstinence on cognition in adolescent tobacco smokers. Biol Psychiatry 57:56–66
Kelly DL, McMahon RP, Weiner E, Boggs DL, Dickinson D, Conley RR, Buchanan RW (2008) Lack of beneficial galantamine effect for smoking behavior: a double-blind randomized trial in people with schizophrenia. Schizophr Res 103:161–168
LeSage MG, Shelley D, Ross JT, Carroll FI, Corrigall WA (2009) Effects of the nicotinic receptor partial agonists varenicline and cytisine on the discriminative stimulus effects of nicotine in rats. Pharmacol Biochem Behav 91:461–467
McNair D, Lorr M, Dropperman L (1971) Manual for profile of mood states. Educational and industrial testing services, San Diego
Mihalak KB, Carroll FI, Luetje CW (2006) Varenicline is a partial agonist at alpha4beta2 and a full agonist at alpha7 neuronal nicotinic receptors. Mol Pharmacol 70:801–805
Miwa JM, Freedman R, Lester HA (2011) Neural systems governed by nicotinic acetylcholine receptors: emerging hypotheses. Neuron 70:20–33
Mooney ME, Sofuoglu M (2006) Bupropion for the treatment of nicotine withdrawal and craving. Expert Rev Neurother 6:965–981
Morgan MJ, Davies GM, Willner P (1999) The questionnaire of smoking urges is sensitive to abstinence and exposure to smoking-related cues. Behav Pharmacol 10:619–626
Paterson NE (2009) Behavioural and pharmacological mechanisms of bupropion's anti-smoking effects: recent preclinical and clinical insights. Eur J Pharmacol 603:1–11
Reid RT, Sabbagh MN (2008) Effects of cholinesterase inhibitors on rat nicotinic receptor levels in vivo and in vitro. J Neural Transm (Vienna, Austria: 1996) 115:1437–1444
Robertson IH, Manly T, Andrade J, Baddeley BT, Yiend J (1997) ‘Oops!’: performance correlates of everyday attentional failures in traumatic brain injured and normal subjects. Neuropsychologia 35:747–758
Robinson DM, Plosker GL (2006) Galantamine extended release. CNS Drugs 20:673–681, discussion 682-3
Rollema H, Chambers LK, Coe JW, Glowa J, Hurst RS, Lebel LA, Lu Y, Mansbach RS, Mather RJ, Rovetti CC, Sands SB, Schaeffer E, Schulz DW, Tingley FD 3rd, Williams KE (2007) Pharmacological profile of the alpha4beta2 nicotinic acetylcholine receptor partial agonist varenicline: an effective smoking cessation aid. Neuropharmacology 52:985–994
SAS Institute Inc (2007) The SAS system for windows. SAS Institute Inc., Cary
Schilstrom B, Ivanov VB, Wiker C, Svensson TH (2007) Galantamine enhances dopaminergic neurotransmission in vivo via allosteric potentiation of nicotinic acetylcholine receptors. Neuropsychopharmacology 32:43–53
Schrattenholz A, Pereira EF, Roth U, Weber KH, Albuquerque EX, Maelicke A (1996) Agonist responses of neuronal nicotinic acetylcholine receptors are potentiated by a novel class of allosterically acting ligands. Mol Pharmacol 49:1–6
Shiffman S, Kirchner TR (2009) Cigarette-by-cigarette satisfaction during ad libitum smoking. J Abnorm Psychol 118:348–359
Silver JM, Koumaras B, Chen M, Mirski D, Potkin SG, Reyes P, Warden D, Harvey PD, Arciniegas D, Katz DI, Gunay I (2006) Effects of rivastigmine on cognitive function in patients with traumatic brain injury. Neurology 67:748–755
Slemmer JE, Martin BR, Damaj MI (2000) Bupropion is a nicotinic antagonist. J Pharmacol Exp Ther 295:321–327
Smith JW, Stolerman IP (2009) Recognising nicotine: the neurobiological basis of nicotine discrimination. Handbook of experimental pharmacology 295-333
Snyder FR, Henningfield JE (1989) Effects of nicotine administration following 12h of tobacco deprivation: assessment on computerized performance tasks. Psychopharmacology 97:17–22
Sobel BF, Sigmon SC, Griffiths RR (2004) Transdermal nicotine maintenance attenuates the subjective and reinforcing effects of intravenous nicotine, but not cocaine or caffeine, in cigarette-smoking stimulant abusers. Neuropsychopharmacol: Off Publ Am Coll Neuropsychopharmacol 29:991–1003
Sofuoglu M, Mooney M (2009) Cholinergic functioning in stimulant addiction: implications for medications development. CNS drugs 23:939–952
Sofuoglu M, Mouratidis M, Yoo S, Culligan K, Kosten T (2005) Effects of tiagabine in combination with intravenous nicotine in overnight abstinent smokers. Psychopharmacol (Berl) 181:504–510
Sofuoglu M, Poling J, Mouratidis M, Kosten T (2006) Effects of topiramate in combination with intravenous nicotine in overnight abstinent smokers. Psychopharmacol (Berl) 184:645–651
Sofuoglu M, Waters AJ, Mooney M (2008) Modafinil and nicotine interactions in abstinent smokers. Hum Psychopharmacol 23:21–30
Sofuoglu M, Waters AJ, Mooney M, O'Malley SS (2009) Minocycline reduced craving for cigarettes but did not affect smoking or intravenous nicotine responses in humans. Pharmacol Biochem Behav 92:135–140
Sofuoglu M, Waters AJ, Poling J, Carroll KM (2011) Galantamine improves sustained attention in chronic cocaine users. Exp Clin Psychopharmacol 19:11–19
Strong DR, Leventhal AM, Evatt DP, Haber S, Greenberg BD, Abrams D, Niaura R (2011) Positive reactions to tobacco predict relapse after cessation. J Abnorm Psychol 120:999–1005
Tenovuo O, Alin J, Helenius H (2009) A randomized controlled trial of rivastigmine for chronic sequels of traumatic brain injury—what it showed and taught? Brain Inj 23:548–558
Tiffany ST, Drobes DJ (1991) The development and initial validation of a questionnaire on smoking urges. Br J Addict 86:1467–1476
Wilkinson DS, Gould TJ (2011) The effects of galantamine on nicotine withdrawal-induced deficits in contextual fear conditioning in C57BL/6 mice. Behav Brain Res 223:53–57
Acknowledgments
This research was supported by the Veterans Administration's Mental Illness Research, Education and Clinical Center (MIRECC) and the National Institute on Drug Abuse grant K02-DA-021304 (MS). MS serves as an expert witness on behalf of Pfizer in lawsuits related to varenicline.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Sofuoglu, M., Herman, A.I., Li, Y. et al. Galantamine attenuates some of the subjective effects of intravenous nicotine and improves performance on a Go No-Go task in abstinent cigarette smokers: a preliminary report. Psychopharmacology 224, 413–420 (2012). https://doi.org/10.1007/s00213-012-2763-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00213-012-2763-4