
Abstract
The aim of this study was to characterize the interaction between tiagabine (TGB) and ethosuximide (ETS), two antiepileptic drugs, in pentylenetetrazole (PTZ)-induced clonic seizures in mice using isobolographic analysis. The nature of the interaction between the drugs administered in combination was ascertained by estimating plasma and brain concentrations of ETS and TGB using fluorescence polarization immunoassay (FPIA) and high-performance liquid chromatography (HPLC). The results indicated that both drugs produced clear anticonvulsant effects against PTZ-induced clonic seizures in mice, but that their dose-response relationship curves (DRRCs) were not parallel, consequently necessitating the isobolographic analysis for non-parallel DRRCs. The isobolographic analysis revealed that the combination of TGB with ETS at the fixed-ratio of 1:1 exerted an additive interaction against PTZ-induced clonic seizures in mice. FPIA documented that TGB significantly elevated brain ETS concentrations (by 64%), while having no effect on plasma ETS concentrations in experimental animals. In contrast, ETS had no significant impact on plasma and brain concentrations of TGB in mice, as measured by HPLC. It can be concluded that the additive interaction between TGB and ETS at the fixed-ratio of 1:1 in the PTZ test was complicated by a significant pharmacokinetic increase in total brain ETS concentrations. At present, there are no recommendations to use this drug combination in epileptic patients.
Similar content being viewed by others
Avoid common mistakes on your manuscript.
Introduction
Accumulating experimental evidence indicates that the method of isobolographic analysis can be accepted as a gold standard during the evaluation of drug interactions. There are currently several types and various modifications of the isobolographic analysis (Berenbaum 1989; Greco et al. 1995). The isobolographic analysis has also been successfully applied in experimental epileptology to characterize interactions among antiepileptic drugs (AEDs) in preclinical studies (Deckers et al. 2000; Leach 2000; Löscher and Wauquier 1996). In this field, it has been proven to be a valuable method that allows the precise classification of exact types of interactions among drugs, comprehensively evaluating their nature as supra-additive (synergistic), sub-additive (relatively antagonistic), infra-additive (absolutely antagonistic), indifferent or additive (Berenbaum 1989; Greco et al. 1995; Luszczki and Czuczwar 2003; Luszczki et al. 2006; Tallarida 2000). There are two types of isobolographic analysis: type I, which is used if all examined drugs are fully active, and type II, which is used if one of the drugs produces no effect and is considered to be virtually ineffective in an experimental model (Berenbaum 1989; Porreca et al. 1990). Quite recently, a novel variant of isobolography for non-parallel dose-response relationship curves (DRRCs) of drugs administered separately has been introduced for use in experimental studies (Grabovsky and Tallarida 2004; Luszczki 2007; Tallarida 2006, 2007).
It has been reported that tiagabine (TGB, a newer AED) has a DRRC that was parallel to those of oxcarbazepine, loreclezole, felbamate and gabapentin in the pentylenetetrazole (PTZ)-induced seizure test in mice, thereby producing an additive interaction with type I isobolographic analysis for parallel DRRCs (Luszczki and Czuczwar 2004, 2005). In contrast, gabapentin and topiramate had non-parallel DRRCs in the maximal electroshock-induced seizure test in mice and the drugs produced supra-additivity (synergy) with the isobolographic analysis for non-parallel DRRCs (Luszczki 2007). There is no doubt that the type I isobolographic analysis for non-parallel DRRCs is more complicated than the isobolographic analysis for parallel DRRCs. When the interactions of two drugs, whose DRRCs are not parallel are analysed, two various additive equations are determined from which two theoretically additive values are calculated (for more details, see Grabovsky and Tallarida 2004; Luszczki 2007; Tallarida 2007).
It is therefore of pivotal importance to characterize the interaction profile between TGB and ethosuximide (ETS, a conventional AED), whose DRRCs were not parallel in the PTZ test in mice. It is widely accepted that the PTZ-induced seizure test can be considered to be an experimental model of myoclonic seizures and, to a certain extent, of absence seizures in man (Löscher and Schmidt 1988; Löscher et al. 1991). As such, the test can be considered to be appropriate for assessing the characteristics of the interaction between TGB and ETS in the study reported here. The acute adverse-effect profile for the combination of TGB with ETS was also investigated in relation to motor performance in the chimney test, long-term memory in the passive avoidance task and skeletal muscular strength in the grip-strength test in mice. To ascertain whether the observed anticonvulsant effects for the combination of TGB with ETS were the result of a pharmacodynamic and/or a pharmacokinetic interaction, plasma and brain concentrations of ETS and TGB were evaluated using fluorescence polarization immunoassay (FPIA) and high-performance liquid chromatography (HPLC).
Material and methods
Animals and experimental conditions
All experiments were performed on adult male albino Swiss mice each weighing 22–26 g. The mice were kept in colony cages with free access to food and tap water, under standardized housing conditions (natural light–dark cycle, ambient temperature of 22 ± 1°C, relative humidity of 55 ± 5%). After 7 days of adaptation to laboratory conditions, the animals were randomly assigned to experimental groups consisting of eight mice. Each mouse was used only once. All tests were performed between 0900 and 1500 hours. Procedures involving animals and their care were conducted in accordance with current European Community and Polish law on the experimentation and protection of animals. Additionally, all efforts were made to minimize animal suffering and to use only the number of animals necessary to produce reliable scientific data. The experimental protocols and procedures listed were approved by the Local Ethics Committee at the Medical University of Lublin (License no. 425/2003/451/2003) and complied with the European Communities Council Directive of 24 November 1986 (86/609/EEC).
Drugs
The following AEDs were used in this study: TGB (as a pharmaceutical formulation, Gabitril; Sanofi Winthrop, Gentilly, France) and ETS (as a pure substance; Sigma, St. Louis, MO). Both drugs were suspended in a 1% solution of Tween 80 (Sigma) in saline and administered intraperitoneally (i.p.), as two separate injections, in a volume of 5 ml/kg body weight. The control animals received an adequate volume of vehicle (1% solution of Tween 80 in saline). Fresh drug solutions were prepared on each day of experimentation. Tiagabine was administered 15 min and ETS was administered 45 min prior to the PTZ, chimney, passive avoidance and grip-strength tests as well as before the plasma and brain sampling for the measurement of AED concentrations. The route of systemic (i.p.) administration and pretreatment times before the testing of the AEDs were based on information retrieved from the literature on their biological activity and from previous experiments carried out in our laboratory (Luszczki et al. 2003a, 2005). Pentylenetetrazole (Sigma) was dissolved in sterile saline and administered subcutaneously (s.c.) into a loose fold of skin in the midline of the neck in a volume of 5 ml/kg body weight.
Pentylenetetrazole-induced convulsions
The anticonvulsant activities of ETS and TGB against PTZ-induced clonic seizures were determined following the s.c. administration of PTZ at its CD97 (convulsive dose 97—the dose of PTZ that produced clonic seizures in 97% of mice, which in this study was 100 mg/kg). Following PTZ administration, the mice were placed separately into transparent Plexiglas cages (25 × 15 × 10 cm) and observed for 30 min for the occurrence of clonic seizures. Clonic seizure activity was defined as clonus of the whole body lasting for more than 3 s, with an accompanying loss of the righting reflex. The number of animals convulsing among the total number of mice tested was noted for each treatment regimen. The animals were given increasing doses of the AEDs, and the anticonvulsant activity of each drug was evaluated as the ED50 (median effective dose of an AED—the dose that protected 50% of mice against clonic convulsions). At least four groups of animals were used to estimate each ED50 value, which was calculated from the respective log-probit dose-response relationship curve (DRRC) according to Litchfield and Wilcoxon (1949). The anticonvulsant activity of TGB administered alone was studied at doses of 0.25, 0.5, 1, 2 and 3 mg/kg, whereas that of ETS administered alone was studied at doses of 110, 130, 150, and 170 mg/kg against the clonic phase of PTZ-induced seizures in mice. Similarly, the anticonvulsant activity of a mixture of TGB with ETS was evaluated and expressed as ED50 mix, corresponding to the dose of the mixture of both drugs required to protect 50% of animals tested against PTZ-induced clonic convulsions. This experimental procedure has been described in more detail by Luszczki et al. (2003a, 2005).
Measurement of plasma and brain AED concentrations
The animals were administered ETS + vehicle, TGB + vehicle or the combination of ETS + TGB, at doses corresponding to the ED50 mix value at the fixed-ratio of 1:1 from the PTZ test. Mice were killed by decapitation at times chosen to coincide with that scheduled for the PTZ test, and samples of blood of approximately 1 ml were collected into heparinized Eppendorf tubes. Simultaneously, the whole brains of mice were removed from the skulls, weighed, harvested and homogenized with Abbott buffer (1:2 w/v) in an Ultra-Turrax T8 homogenizer (IKA Werke, Staufen, Germany). The brain homogenates were centrifuged at 10,000 g for 10 min. Blood samples containing ETS were centrifuged at 5000 g for 5 min and plasma samples (100 μl) or the supernatant samples (100 μl) were analysed for ETS content by FPIA using a TDx analyser and reagents exactly as described by the manufacturer (Abbott Laboratories, North Chicago, IL). Thus, in the present study, total plasma and total brain concentrations of ETS were measured with FPIA. At exactly the same time, the identically prepared blood samples containing TGB were centrifuged at 5000 g for 5 min and plasma (400 μl) was transferred into an Amicon Centrifree Micropartition System (MPS-1; Millipore, Billerica, MA) for the separation of free (non-protein bound) concentrations of TGB from that which is protein-bound. The MPS-1 tubes were centrifuged at 5000 g for 10 min. The filtrate samples (200 μl) or the identically prepared supernatant samples (200 μl) containing TGB were analysed using an automated Gilson HPLC system (Anachem, Bedfordshire, UK) consisting of a Gilson 234 autosampler and Gilson 306 pumps. The mobile phase comprised methanol (20 mmol), acetonitrile and citric buffer (pH = 3) in a ratio of 25:30:40 (v:v:v). Chromatographic separation was achieved using a Hypersil BDS-2-C18 5 lm column (Agilent Technologies, Santa Clara, CA). Plasma and brain supernatant samples were prepared for analysis, as follows: 200 μl of plasma or brain supernatant was pipetted into a C8 column conditioned with methanol (2 × 1 ml) and water (2 × 1 ml) and eluted with methanol (2 × 0.2 ml) and 0.4 ml of water. The samples were then centrifuged for 5 min, and 200 μl of eluant was transferred into the HPLC column. Thus, in this study, free (non-protein-bound) plasma and total brain concentrations of TGB were measured by HPLC. The concentrations of ETS were expressed in micrograms per millilitre of plasma or brain supernatant, while those of TGB were expressed in nanograms per millilitre as the means ± SD of at least eight determinations (separate plasma and brain preparations).
Isobolographic analysis of interactions
Isobolographic analysis of the interactions between TGB and ETS was performed according to the methodology previously detailed (Luszczki and Czuczwar 2003, 2004, 2005, 2006; Luszczki et al. 2003a, 2006) and modified according to Grabovsky and Tallarida (2004), Tallarida (2006, 2007) and Luszczki (2007) for drugs with non-parallel DRRCs. The evaluation of the ED50 values of AEDs administered alone was performed using the log-probit method according to Litchfield and Wilcoxon (1949). Based upon these ED50 values, the median additive doses of the mixture of TGB with ETS—i.e. doses of the mixture that theoretically should protect 50% of the animals tested against PTZ-induced clonic seizures (ED50 add)—were then calculated from two equations of additivity reported by Tallarida (2006, 2007). For the lower line of additivity, the equation at a 50% effect is y = ED50_ETS − [ED50_ETS/(ED50_TGB/x)q/p], where y is the dose of ETS, x is the dose of TGB and q and p are curve-fitting parameters (Hill coefficients) for ETS and TGB, respectively. Similarly, for the upper line of additivity, the equation at a 50% effect is y = ED50_ETS [(ED50_TGB − x)/ED50_TGB]q/p. The curve-fitting parameters (p and q) were calculated by transforming the probits of response for ETS and TGB administered alone to percentage effect. It is important to note that when two drugs produce a maximal effect but are “heterodynamic” (i.e. have non-parallel DRRCs), the additivity is represented as an area bounded by two defined curves (lower and upper isoboles of additivity). The experimentally derived ED50 values are statistically different if their points are placed outside this region. For supra-additivity (synergy), the experimentally derived ED50 mix points are placed below the area bounded by the lower and upper isoboles of additivity, and for sub-additivity (antagonism), they are placed above this region (Tallarida 2006, 2007). In isobolography, it is accepted that half the ED50_1 of one drug plus half the ED50_2 of the second drug should be as effective therapeutically as a full dose of either drug administered separately. This concept of adding fractions of the ED50 values of drugs is a basic principle of isobolography (Berenbaum 1989; Loewe 1953). The proportions of TGB and ETS in the mixture were then calculated for the fixed-ratio combination of 1:1, and the mixture of TGB with ETS was administered to the animals. The evaluation of the experimentally derived ED50 mix at the fixed-ratio of 1:1 was based upon the dose of the mixture protecting 50% of animals tested against PTZ-induced seizures in mice. Statistical comparison of the experimentally derived ED50 mix value with its corresponding theoretically additive ED50 add values was undertaken using the unpaired Student’s t test, according to Tallarida (2000). Finally, the separate doses of TGB and ETS in the mixture were determined by multiplying the ED50 mix value by the respective proportions of AEDs (denoted for purely additive mixture). Further details regarding these concepts have been published by Luszczki (2007) and Tallarida (2006, 2007).
Chimney test
The effect of the combination of TGB with ETS (at doses corresponding to the ED50 mix for the fixed-ratio of 1:1 from the PTZ test) on motor coordination impairment was quantified using the chimney test of Boissier et al. (1960). In this test, animals had to climb backwards up a plastic tube (inner diameter 3 cm, length 30 cm length). Motor impairment was indicated by the inability of the animals to climb backwards up the transparent tube within 60 s. Data are presented as a percentage of animals that failed to successfully perform the chimney test. This experimental procedure has been described in detail by Luszczki and Czuczwar (2007) and Luszczki et al. (2005).
Grip-strength test
The effect of the combination of TGB with ETS (at doses corresponding to the ED50 mix for the fixed-ratio of 1:1 from the PTZ test) on muscular strength in mice was quantified by the grip-strength test of Meyer et al. (1979). The time before the commencement of the grip-strength test (after drug administration) was identical to that for the PTZ test. The grip-strength apparatus (BioSeb, Chaville, France) comprised a wire grid (8 × 8 cm) connected to an isometric force transducer (dynamometer). The mice were lifted by the tails so that their forepaws could grasp the grid. The mice were then gently pulled backward by the tail until the grid was released. The maximal force exerted by the mouse before losing grip was recorded. The mean of three measurements for each animal was calculated and the mean maximal force of eight animals per group was subsequently determined. The skeletal muscular strength in mice was expressed in Newtons (N) as means ± SEM of at least eight determinations. This experimental procedure has been described in detail by Luszczki and Czuczwar (2007).
Step-through passive avoidance task
On the first day before training, each animal was administered TGB in combination with ETS at doses corresponding to the ED50 mix for the fixed-ratio of 1:1 from the PTZ test. The time before the commencement of the training session (after drug administration) was identical to that for the PTZ test. The animals were then placed in an illuminated box (10 × 13 × 15 cm) connected to a larger dark box (25 × 20 × 15 cm) equipped with an electric grid floor. Entrance of animals to the dark box was punished by an adequate electric footshock (0.6 mA for 2 s). The animals that did not enter the dark compartment were excluded from subsequent experimentation. On the following day (24 h later), the pre-trained animals were placed again into the illuminated box and observed for up to 180 s. Mice that avoided the dark compartment for 180 s were considered to have remembered the task. The time that the mice took to enter the dark box was noted, and the median latencies (retention times) with 25th and 75th percentiles were calculated. The step-through passive avoidance task provides information about the ability to acquire the task (learning) and to recall the task (retrieval). Therefore, it may be regarded as a measure of long-term memory (Venault et al. 1986). This experimental procedure has been described in detail by Luszczki and Czuczwar (2007) and Luszczki et al. (2003a, 2005).
Statistics
The percentage protection of animals against PTZ-induced clonic seizures per dose of the AEDs and the DRRCs for ETS and TGB administered alone and in combination at the fixed-ratio of 1:1 were fitted using log-probit linear regression analysis according to Litchfield and Wilcoxon (1949). The ED50 values with their 95% confidence limits were calculated by computer-assisted log-probit analysis according to Litchfield and Wilcoxon (1949). To precisely analyse the experimental data, the test for parallelism of the DRRCs for TGB and ETS was presented as indispensable conditions for testing AED interactions with isobolography. The obtained 95% confidence limits were transformed to standard errors of the mean as described previously (Luszczki et al. 2006). Statistical evaluation of isobolographic interactions was performed using Student’s t test in order to detect the differences between the experimentally derived (ED50 mix) and theoretical additive (ED50 add) values, according to Porreca et al. (1990) and Tallarida (2000). Total plasma and brain concentrations of ETS and TGB were statistically analysed using the unpaired Student’s t test. Qualitative variables from the chimney test were compared using the Fisher’s exact probability test. The results from the step-through passive avoidance task were statistically analysed using the Kruskal–Wallis nonparametric ANOVA test followed by the post-hoc Dunn’s test. The data from the grip-strength test were statistically analysed using one-way ANOVA followed by the post-hoc Bonferroni’s test. All statistical tests were performed using GraphPad Prism ver. 4.0 for Windows software (GraphPad Software, San Diego, CA). Differences among values were considered to be statistically significant if P < 0.05.
Results
Effects of TGB and ETS administered alone on PTZ-induced clonic seizures
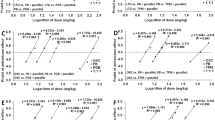
The anticonvulsant effects of TGB, expressed as the percentage of protection against PTZ-induced clonic seizures in mice, ranged between 25% for TGB at the dose of 0.5 mg/kg and 87.5% for TGB at the dose of 3 mg/kg (Table 1). The log-probit analysis of DRRC for TGB enabled the calculation of its ED50 value, which was 0.99 (0.57–1.73) mg/kg (Table 1; Fig. 1). Similarly, ETS exerted clear-cut anticonvulsant effects in the PTZ test in mice, and its ED50 value, as denoted from the log-probit method, was 145.2 (126.1–167.3) mg/kg (Table 1; Fig. 1). In this case, ETS at the dose of 110 mg/kg produced a 12.5% protection against PTZ-induced clonic seizures, whereas ETS at the highest tested dose of 170 mg/kg provided a 75% anticonvulsant effect in the PTZ test in mice (Table 1). The test of parallelism of two DRRCs for TGB and ETS administered alone in the PTZ test revealed that the DRRC of both AEDs were non-parallel to one another (Table 1; Fig. 1).

Log-probit analysis and dose-response relationship curves (DRRCs) for tiagabine (TGB) and ethosuximide (ETS) administered alone and their combination at the fixed-ratio of 1:1 in the pentylenetetrazole (PTZ) test in mice. Doses of TGB and ETS administered alone were transformed to logarithms, whereas the protective effects offered by the AEDs against PTZ-induced clonic seizures were transformed to probits (Litchfield and Wilcoxon 1949). Linear regression equations of DRRCs are presented on the graph, where y is the probit of response and x is the logarithm (to the base 10) of a drug dose. The dotted lines represent the median effective doses (ED 50 values) for TGB and ETS administered alone and their combination at the fixed-ratio of 1:1. The dashed line reflects the DRRC for the mixture of TGB with ETS at the fixed-ratio of 1:1. The test for parallelism of DRRCs (for TGB and ETS) revealed that both lines are not parallel to one another (Litchfield and Wilcoxon 1949). For more details, see the footnotes to Tables 1 and 2
Isobolographic assessment of interaction between TGB and ETS
The mixture of TGB and ETS at the fixed-ratio of 1:1 exerted an additive interaction in the PTZ test in mice. The ED50 mix for this fixed-ratio combination was 47.29 mg/kg, whereas the corresponding ED50 add values were 41.69 mg/kg (for the lower ED50 add) and 104.52 mg/kg (for the upper ED50 add; Table 2). In this case, the ED50 mix (i.e., dose protecting 50% of animals against PTZ-induced clonic seizures) did not significantly differ from the ED50 add values, thereby indicating the additive interaction between drugs (Table 2, Fig. 2).

Isobologram showing an additive interaction between tiagabine (TGB) and ethosuximide (ETS) against pentylenetetrazole (PTZ)-induced clonic seizures in mice. The median effective doses (ED50) for TGB and ETS are shown plotted graphically on the X- and Y-axes, respectively. The lower and upper isoboles of additivity represent the curves connecting the ED 50 values for TGB and ETS administered alone. The dotted line starting from the point (0,0) corresponds to the fixed-ratio of 1:1 for the combination of TGB with ETS. The points A′ and A″ depict the theoretically calculated ED50 add values for both the lower and upper isoboles of additivity. The point M represents the experimentally derived ED50 mix value for total dose of the mixture expressed as the proportions of TGB and ETS that produced 50% anticonvulsant effects in the PTZ test in mice. The point S on the graph reflects the ED50 add value denoted theoretically from the Loewe’s equation for the fixed-ratio combination of 1:1. On the graph, the SEM values are presented as horizontal and vertical error bars for every ED50 value. The ED50 mix value is placed close to the lower line of additivity and within the area of additivity bounded by two isoboles of additivity, indicating additive interaction between TGB and ETS in the PTZ test in mice. The sum of the X- and Y-coordinates for each point placed on the isobologram (M, A′, A″, S), corresponds to the respective ED50 values that are as follows: A′ (0.282; 41.41), A′′ (0.707; 103.81), S (0.495; 72.61), M (0.320; 46.97)
Total plasma and total brain ETS concentrations
Total plasma ETS concentration was evaluated for ETS co-administered with TGB at doses corresponding to the ED50 mix at the fixed-ratio of 1:1 from the PTZ test. With the FPIA technique, the total plasma concentration of ETS, administered singly at 47.0 mg/kg, was 26.03 ± 6.11 μg/ml and did not significantly differ from that evaluated for the mixture of ETS (47.0 mg/kg) with TGB (0.3 mg/kg), which was 29.84 ± 5.40 μg/ml. In contrast, total brain concentration of ETS for the mixture of ETS (47.0 mg/kg) with TGB (0.3 mg/kg) was 5.15 ± 1.89 μg/ml and considerably differed from that evaluated for ETS administered singly at 47.0 mg/kg, which was 3.15 ± 1.16 μg/ml (P < 0.05).
Free (non-protein-bound) plasma and total brain TGB concentrations
The free plasma TGB concentration was evaluated for TGB co-administered with ETS at doses corresponding to the ED50 mix at the fixed-ratio of 1:1 from the PTZ test. With the HPLC technique, the free plasma concentration of TGB, administered singly at 0.3 mg/kg, was 206.15 ± 58.79 ng/ml and did not significantly differ from that evaluated for the mixture of TGB (0.3 mg/kg) with ETS (47.0 mg/kg), which was 181.78 ± 56.24 ng/ml. Similarly, total brain concentration of TGB for the mixture of TGB (0.3 mg/kg) with ETS (47.0 mg/kg) was 40.75 ± 11.81 ng/ml and did not considerably differ from that evaluated for TGB administered singly at 0.3 mg/kg, which amounted to 45.18 ± 11.92 ng/ml.
Effects of TGB, ETS and their combination at the fixed-ratio of 1:1 on long-term memory, motor coordination and muscular strength in mice
When TGB was co-administered with ETS at the fixed-ratio of 1:1, motor coordination in mice did not differ significantly from that of the control (vehicle-treated) animals (Table 3). Furthermore, the AEDs combined at the fixed-ratio of 1:1 did not impair long-term memory in mice, as determined in the passive avoidance task (Table 3). Similarly, the combination of TGB with ETS had no effect on muscular strength, as assessed by the grip-strength test (Table 3). Moreover, TGB and ETS administered alone at doses of 0.99 mg/kg and 145.2 mg/kg, which was their ED50 values determined from the PTZ test, did not significantly affect long-term memory, muscular strength and motor performance in animals (Table 3).
Discussion
The results indicate that the combination of TGB with ETS at the fixed-ratio of 1:1 exerted an additive interaction against PTZ-induced clonic seizures in mice. It is worth noting that the isobolographic analysis of interaction was performed in this study only for the fixed-ratio of 1:1 due to the lack of parallelism of two DRRCs for the drugs administered alone. Other fixed-ratio combinations, such as: 1:3 and 3:1, among others, could not be evaluated appropriately with this method because of the changing proportions of the drugs in the mixture along with the increase in AED doses (Luszczki 2007; Tallarida 2007). In general, the proportions of drugs in a mixture are calculated from the Loewe’s equation based on fixed fractions of drugs present in the mixture (Loewe 1953). In the case of two parallel DRRCs, the proportions of drugs in the mixture are constant for every effect ranging between 16 and 84% (or 4 and 6 probits, respectively). However, if two drugs have non-parallel DRRCs, the proportions of drugs in the mixture change along with the increase in observed effect (Luszczki 2007; Tallarida 2006, 2007). This is why only the fixed-ratio combination of 1:1 for the 50% effect (i.e. when both drugs were present in the mixture at equi-effective doses), was examined in this study.
It should be stressed that the additive interaction documented for the combination of TGB with ETS against PTZ-induced clonic seizures is consistent with that reported earlier for the combinations of TGB with oxcarbazepine, loreclezole, felbamate and gabapentin in the PTZ test in mice (Luszczki and Czuczwar 2004, 2005).
The evaluation of acute adverse effects for the combination of TGB with ETS, administered at doses corresponding to the ED50 mix value, as estimated from the PTZ test, revealed no significant impairment of motor coordination in mice subjected to the chimney test, no deficits in long-term memory in mice challenged with the step-through passive avoidance task and no significant changes in the skeletal muscular strength of mice in the grip-strength test. However, the pharmacokinetic study revealed that TGB significantly increased (by 64%) total brain ETS concentrations, while TGB remained without effect on total plasma ETS concentrations in experimental animals. Moreover, the pharmacokinetic estimation of free plasma and total brain concentrations of TGB revealed that ETS had no significant effect on TGB concentrations in experimental animals. Thus, the observed additive interaction between TGB and ETS in the PTZ test was complicated only by a significant increase in total brain ETS concentrations. It is worthwhile mentioning that the pharmacokinetic profile of interaction of TGB with ETS was verified bidirectionally because both plasma and brain concentrations of two AEDs (TGB and ETS) were measured in this study. The bidirectional estimation of plasma and brain AED concentrations allowed the interaction from the PTZ test to be classified as being pharmacokinetic in nature. Moreover, it is important to note that the plasma protein binding for ETS is <5%, whereas that for TGB is 96% (Leppik 2001), which explains why the free plasma TGB and total plasma ETS concentrations were estimated in this study.
Given the fact that TGB increased ETS concentration in the brain, one can ascertain that the interaction between these drugs was primarily antagonistic in nature and secondarily masked by the pharmacokinetic increase in total brain ETS concentrations, which finally produced additivity in the PTZ test with the isobolographic analysis. It should be stressed that during a pharmacokinetic evaluation of AED concentrations, total brain concentrations are of pivotal importance because they precisely reflect the exact characteristics of interaction between AEDs. The selective estimation of total plasma ETS concentrations in this study would provide incorrect and false conclusions due to the fact that there was no pharmacokinetic interaction between TGB and ETS in the plasma of experimental animals. As documented earlier, only total brain AED concentrations have been found to provide valuable information about the exact nature of interactions between drugs in experimental animals (Cadart et al. 2002; Luszczki et al. 2003b). Nevertheless, the results of this study revealed that the characterization of the interaction between TGB and ETS is complicated, especially, if the DRRCs of the AEDs are non-parallel and produce a significant pharmacokinetic increase in total brain AED concentrations. The combination of TGB with ETS is a good example of just how complicated an analysis of the interaction between drugs in preclinical studies may be.
Another important fact to bear in mind while explaining the observed interaction between ETS and TGB in the PTZ test in mice was that the combination of TGB at a dose of 0.33 mg/kg with ETS at a dose of 46.9 mg/kg was as therapeutically effective as TGB at 0.99 mg/kg or ETS at 145.2 mg/kg administered separately in the PTZ test. Although the doses of TGB and ETS in the mixture at the fixed-ratio of 1:1 were reduced by threefold, the observed interaction between the AEDs was additive. The isobologram illustrates that the experimentally-derived ED50 mix is placed close to the lower line of additivity and at a certain distance from the centre of symmetry, suggesting a tendency toward synergy for the drug combination at the fixed-ratio of 1:1. Nevertheless, statistical analysis of the data with the unpaired Student’s t test revealed that the ED50 mix value did not significantly differ from the ED50 add values, indicating an additive interaction between TGB and ETS against PTZ-induced seizures in mice. As discussed earlier, only a statistical evaluation of isobolographic data provides researchers with convincing evidence on the exact nature of analysed interactions and their real classification (Luszczki and Czuczwar 2003, 2004). Other methods (especially, those based on a comparison of overlapping 95% confidence limits of ED50 mix with ED50 add or the calculation of the interaction index for the drug combination) used separately without a statistical analysis of the data are not recommended for the experimental characterization of interactions between drugs (for more details see the discussion in Luszczki and Czuczwar 2003, 2004, 2006). Consequently, statistical analysis of the interaction in the study reported here was performed with the unpaired Student’s t test, without calculation of the interaction index or a comparison of 95% confidence limits. This is the reason why the 95% confidence limits of ED50 mix and ED50 add were transformed to their respective SEM in order to perform an adequate statistical analysis of the data.
The combination of ETS with TGB in the PTZ test has some clinical limitations because ETS is not a drug used clinically in patients with myoclonic seizures, but it does suppress the absence of seizures in children (Brodie and Schachter 2001). With respect to TGB, the drug can aggravate myoclonic seizures in epileptic patients or even evoke non-convulsive status epilepticus (Brodie and Schachter 2001). Although the PTZ test in rodents is considered to be an animal model of myoclonic seizures in humans (Löscher and Schmidt 1988; Löscher et al. 1991), the combination of TGB with ETS cannot be recommended for patients with myoclonic seizures. On the other hand, there are several epileptic syndromes with various complex seizure types for which the combination of ETS with TGB may be favorable.
On the basis of the result of the preclinical study reported here, one can ascertain that the characteristics of interaction may be complicated by the lack of parallelism of the DRRCs of the analysed AEDs and the pharmacokinetic increase in total brain AED concentrations. The combination of ETS with TGB is an example of a drug combination that should be avoided in further clinical settings. At present, there are no recommendations for the concomitant administration of TGB with ETS in clinical settings, unless their anticonvulsant effects are efficacious against various complex seizure types in patients.
References
Berenbaum MC (1989) What is synergy? Pharmacol Rev 41:93–141 Erratum published in (1989) Pharmacol Rev 41:422
Boissier JR, Tardy J, Diverres JC (1960) Une nouvelle methode simple pour explorer l’action «tranquilisante»: le test de la cheminee. Med Exp (Basel) 3:81–84
Brodie MJ, Schachter SC (2001) Fast Facts. Epilepsy, 2nd edn. Health Press, Oxford
Cadart M, Marchand S, Pariat C, Bouquet S, Couet W (2002) Ignoring pharmacokinetics may lead to isoboles misinterpretation: illustration with the norfloxacin-theophylline convulsant interaction in rats. Pharm Res 19:209–214
Deckers CLP, Czuczwar SJ, Hekster YA, Keyser A, Kubova H, Meinardi H, Patsalos P, Renier WO, van Rijn CM (2000) Selection of antiepileptic drug polytherapy based on mechanism of action: the evidence reviewed. Epilepsia 41:1364–1374
Grabovsky Y, Tallarida RJ (2004) Isobolographic analysis for combinations of a full and partial agonist: curved isoboles. J Pharmacol Exp Ther 310:981–986
Greco WR, Bravo G, Parsons JC (1995) The search for synergy: a critical review from response surface perspective. Pharmacol Rev 47:331–385
Leach JP (2000) Antiepileptic drugs: safety in numbers. Seizure 9:170–178
Leppik IE (2001) Contemporary diagnosis and management of the patients with epilepsy, 5th edn. Handbooks in health care. Newtown, Pennsylvania
Litchfield JT, Wilcoxon F (1949) A simplified method of evaluating dose-effect experiments. J Pharmacol Exp Ther 96:99–113
Loewe S (1953) The problem of synergism and antagonism of combined drugs. Arzneimittelforschung 3:285–290
Löscher W, Schmidt D (1988) Which animal models should be used in the search for new antiepileptic drugs? A proposal based on experimental and clinical considerations. Epilepsy Res 2:145–181
Löscher W, Wauquier A (1996) Use of animal models in developing guiding principles for polypharmacy in epilepsy. Epilepsy Res Suppl 11:61–65
Löscher W, Hönack D, Fassbender CP, Nolting B (1991) The role of technical, biological and pharmacological factors in the laboratory evaluation of anticonvulsant drugs. III. Pentylenetetrazole seizure models. Epilepsy Res 8:171–189
Luszczki JJ (2007) Isobolographic analysis of interaction between drugs with nonparallel dose-response relationship curves: a practical application. Naunyn Schmiedebergs Arch Pharmacol 375:105–114
Luszczki JJ, Czuczwar SJ (2003) Isobolographic and subthreshold methods in the detection of interactions between oxcarbazepine and conventional antiepileptics-a comparative study. Epilepsy Res 56:27–42
Luszczki JJ, Czuczwar SJ (2004) Isobolographic profile of interactions between tiagabine and gabapentin: a preclinical study. Naunyn Schmiedebergs Arch Pharmacol 369:434–446
Luszczki JJ, Czuczwar SJ (2005) Isobolographic characterisation of interactions among selected newer antiepileptic drugs in the mouse pentylenetetrazole-induced seizure model. Naunyn Schmiedebergs Arch Pharmacol 372:41–54
Luszczki JJ, Czuczwar SJ (2006) Biphasic characteristic of interactions between stiripentol and carbamazepine in the mouse maximal electroshock-induced seizure model: a three-dimensional isobolographic analysis. Naunyn Schmiedebergs Arch Pharmacol 374:51–64
Luszczki JJ, Czuczwar SJ (2007) Isobolographic characterization of interactions between vigabatrin and tiagabine in two experimental models of epilepsy. Prog Neuropsychopharmacol Biol Psychiatry 31:529–538
Luszczki JJ, Swiader M, Parada-Turska J, Czuczwar SJ (2003a) Tiagabine synergistically interacts with gabapentin in the electroconvulsive threshold test in mice. Neuropsychopharmacology 28:1817–1830
Luszczki JJ, Swiader M, Czuczwar M, Kis J, Czuczwar SJ (2003b) Interactions of tiagabine with some antiepileptics in the maximal electroshock in mice. Pharmacol Biochem Behav 75:319–327
Luszczki JJ, Wojcik-Cwikla J, Andres MM, Czuczwar SJ (2005) Pharmacological and behavioral characteristics of interactions between vigabatrin and conventional antiepileptic drugs in pentylenetetrazole-induced seizures in mice: an isobolographic analysis. Neuropsychopharmacology 30:958–973
Luszczki JJ, Ratnaraj N, Patsalos PN, Czuczwar SJ (2006) Isobolographic analysis of interactions between loreclezole and conventional antiepileptic drugs in the mouse maximal electroshock-induced seizure model. Naunyn Schmiedebergs Arch Pharmacol 373:169–181
Meyer OA, Tilson HA, Byrd WC, Riley MT (1979) A method for the routine assessment of fore- and hindlimb grip strength of rats and mice. Neurobehav Toxicol 1:233–236
Porreca F, Jiang Q, Tallarida RJ (1990) Modulation of morphine antinociception by peripheral [Leu5]enkephalin: a synergistic interaction. Eur J Pharmacol 179:463–468
Tallarida RJ (2000) Drug synergism and dose-effect data analysis. Chapman and Hall/CRC, Boca Raton,
Tallarida RJ (2006) An overview of drug combination analysis with isobolograms. J Pharmacol Exp Ther 319:1–7
Tallarida RJ (2007) Interactions between drugs and occupied receptors. Pharmacol Ther 113:197–209
Venault P, Chapouthier G, de Carvalho LP, Simiand J, Morre M, Dodd RH, Rossier J (1986) Benzodiazepine impairs and beta-carboline enhances performance in learning and memory tasks. Nature 321:864–866
Acknowledgements
This study was supported by a grant (DS 345/2003–2005) from the Medical University of Lublin. The author expresses his thanks to Dr. G. Raszewski (Institute of Agricultural Medicine, Lublin, Poland) for the skilful determination of the plasma and brain concentrations of tiagabine with HPLC.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Luszczki, J.J. Interactions of tiagabine with ethosuximide in the mouse pentylenetetrazole-induced seizure model: an isobolographic analysis for non-parallel dose-response relationship curves. Naunyn-Schmied Arch Pharmacol 378, 483–492 (2008). https://doi.org/10.1007/s00210-008-0305-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00210-008-0305-8