
Abstract
Introduction and hypothesis
One of the main outcomes in the assessment of the treatment of pelvic organ prolapse in women is quality of life. Using quality of life as an outcome measure is increasing in the majority of clinical trials. The aim of current study was to determine the effects of the treatment of pelvic organ prolapse on patients’ quality of life using systematic review and meta-analysis.
Methods
A systematic search for finding randomized controlled studies on pelvic organ prolapse published before October 2012 was conducted. The JAMA users’ guide to the medical literature quality assessment scales for randomized clinical trials was used to assess the quality of included articles. The mean difference in total quality of life score between before and after intervention (surgical or pelvic floor training) with 95 % confidence interval (CI) was considered as a primary summary measure. Egger’s test was used to evaluate the publication bias. Heterogeneity was assessed using I2 Index.
Results
Fifty-seven RCT were critically appraised. Thirty-two articles were eligible after critical evaluation. Mean difference in change in the total quality of life score with 95 % CI for surgical treatment was 74.03 (66.3–81.6) by PFDI-20 and was 44.57 (22.53–66.65) by PFIQ-7. The mean difference in changed in the total quality of life score with 95 % CI was 1.32 (−2.8–5.4) for pelvic floor training (PFT).
Conclusion
We found that surgical interventions on prolapse can improve the quality of life of women. There was a relative effect of PFT on the quality of life of women with prolapse in systematic review. This effect was not seen in meta-analysis, probably because of finding few eligible studies to pool the effect size.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
The bladder, uterus and rectum are all located around the vaginal canal. Owing to the arrangement of these organs, bulging into the vaginal canal in the case of weakness of the supportive tissues for these organs is common. The descent of one or more out of the anterior vaginal wall, posterior vaginal wall, the uterus (cervix) or the apex of the vagina (vaginal vault or cuff scar after hysterectomy) was defined as pelvic organ prolapse [1].
It has been shown that almost 50 % of women lose some of the supportive mechanisms of the pelvic floor owing to childbirth [2]. The prevalence of symptomatic prolapse ranges from 3 to 28 % [3–5]. Prolapse can lead to discomfort in the vagina, leakage of urine, and difficulties using the toilet. These symptoms can greatly affect women’s quality of life [6] and can have a social, psychological and sexual impact [7].
Treatment options for prolapse depend on the severity of the symptoms. Mild to moderate prolapse is usually treated with conservative methods such as electrical stimulation, pelvic-floor muscle training, and biofeedback. More severe prolapse often needs surgery. Various types of surgery are used to repair prolapse.
The efficacy of various measures in repairing prolapse is measured by relief of symptoms, prolapse recurrence rate, and improvement in sexual function and quality of life [8–10].
A large and increasing body of studies has shown the relevance of the assessment of health-related quality of life (HR-QoL) and functional status as important adjuncts to standard clinical outcomes [11]. One of the most important outcomes in assessing the effect of various approaches to treatment of pelvic organ prolapse (POP) is quality of life. It is recommended that investigators explain the impact of POP treatment on the quality of life. There is a large number of studies in which the impact of various treatments is assessed by measuring quality of life [12–14]. There are many and various instruments for evaluating changes in the quality of life in women with POP after treatment [15]. Performing a systematic review is the best way to cumulate the effects of POP treatment on quality of life. The aim of the current study is to review systematically the studies focusing on changing the quality of life after any POP treatments in women.
Materials and methods
Data source, search strategy and eligible studies
A systematic search for finding randomized controlled studies published before October 2012 was conducted. Literature databases (EMBASE, MEDLINE, ELSEVIER, SCOPUS, PROQUEST, WEB OF SCIENCE, and COCHRANE) and the reference list of relevant studies and electronic journals were searched. The reference lists of all the articles included were searched for further studies too.
The key words using MESH for our search as a PICO abbreviation included: P; women with pelvic organ prolapse, (((“Pelvic Organ Prolapse”[Mesh]), I; surgery or conservative treatment, (“Therapeutics”[Mesh] OR “therapy” [Subheading] OR “Estrogen Replacement Therapy”[Mesh] OR “Nondirective Therapy”[Mesh] OR “Drug Therapy, Computer-Assisted”[Mesh] OR “Physical Therapy Modalities”[Mesh] OR “Short-Wave Therapy”[Mesh] OR “Medication Therapy Management”[Mesh])),C; comparison group treated with placebo or conventional therapy, (“General Surgery”[Mesh] OR “Surgical Procedures, Operative”[Mesh] OR “Colorectal Surgery”[Mesh] OR “Surgery, Plastic”[Mesh] OR “Second-Look Surgery”[Mesh] OR “Gynecologic Surgical Procedures”[Mesh] OR “Ultrasonic Surgical Procedures”[Mesh] OR “Unnecessary Procedures”[Mesh] OR “Surgical Procedures, Minor”[Mesh])) and O; Improvement in quality of life “Quality of Life”[Mesh].
Conservative treatments were defined as any drug therapy, computer-assisted or physical therapy, physiotherapy and pelvic floor muscle exercise. Surgical interventions for managing pelvic organ prolapse are defined as general surgery, any surgical procedures, second-look surgery, gynecological and surgical procedures or colorectal surgery.
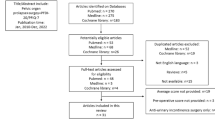
There was no age limit for our search. To be included, studies had to have been a randomized clinical trial (RCT), published as a full-text English-language article, and reported their results as the mean difference (MD) in total quality of life score before and after intervention or having required data to calculate them with 95 % confidence intervals (CI). We excluded the following studies: review articles, non-randomized clinical trials, studies on pelvic organ prolapse in pregnant women or women with cancer of the genital organs, and studies without data to calculate mean differences. Figure 1 shows the selection process for the articles included in this systematic review/meta analysis.

The selection process for the studies included in the systematic review/meta analysis
Quality evaluation of articles
Two independent investigators (MN and AN) conducted data extraction using pre-specified inclusion and exclusion criteria. The JAMA users’ guide to the medical literature quality assessment scales for RCT was used to assess the quality of the articles included. This user guide includes three main questions about internal validity, external validity and the results of studies. We used items of internal validity to assess studies. Internal validity has six key questions about:
-
1.
Randomization
-
2.
Allocation of treatment
-
3.
Blinding of patient and physician
-
4.
Similarity of control and intervention groups
-
5.
Follow-up period
-
6.
The type of analysis
The item got a score of “1” if the item score was “yes”. Then we aggregated the score of all six items. We considered a study eligible to be included if it fulfilled 3 of a maximum score of 6. Discrepancies were resolved by discussion between reviewers and by reaching a consensus.
Quality assessment based on the JAMA users’ guide was applied to all 57 studies included for systematic review. Out of 32 eligible studies, 22 articles were finally included in the meta-analysis and all of them (100 %) fulfilled the criteria of the key questions of the users’ guide (Fig. 1). The following characteristics of the studies included were extracted: treatment type, participants, first author name, the country of origin, date of the study, date of publication, population sampled, sample size, type of intervention and mean/standard deviation total score of quality of life in each group before and after intervention. We calculated the mean difference for any intervention in each article separately.
Statistical analysis and synthesis of results
The MD of the total quality of life score before and after intervention (surgical or conservative) with 95 % CI was considered the primary summary measure. If the MD was not presented in the individual study, it was estimated by Excel calculators. We pooled the score of same questionnaires to assess the common effect of a change in the quality of life. We carried out a meta-analysis of five studies [16–20] with 11 surgical interventions in which the Pelvic Floor Distress Inventory Questionnaire (PFDI) and Pelvic Floor Impact Questionnaire (PFIQ-7) were used. Only two studies [2, 21] with conservative treatment were eligible to enter in the meta-analysis in which the International Consultation on Incontinence Questionnaire (ICIQ) were used. The heterogeneity between the articles was defined as P < 0.1 or I2 index >50 %. The I2 index was calculated as 100 × (Cochrane’s Q - df) / Cochrane’s Q [22, 23]. The random-effects model meta-analysis was used of there was heterogeneity between the studies. Egger’s test with a significant level of 0.05 was used to evaluate the publication bias. STATA version 12 software (Stata, College Station, TX, USA) was used for statistical analysis.
This study was approved by the research and ethical committees of Tehran University of Medical Sciences.
Results
We found 1,075 studies based on a defined search strategy. After excluding 400 duplicated records, 675 studies were screened according title and abstract. At the end of this step, 618 studies were excluded and the remaining 57 studies were critically appraised. Thirty-two articles [2, 8, 14, 16–21, 24–46] were eligible for systematic review after critical evaluation. We could not pool the mean difference of ten articles in which social, mental and physical aspects of quality of life were assessed owing to high heterogeneity. Also, 15 articles [8, 24, 26, 27, 30, 33, 35, 36, 38–40, 43, 45–47] were excluded from meta-analysis because of the use of different tools to evaluate the total score of quality of life. Finally, we carried out a meta-analysis on just 7 studies including 5 studies on surgical and 2 studies on conservative treatments for POP (Fig. 1, Tables 1, 2 and 3). We pooled the MD of the score for quality of life before and after surgery in articles in which PFDI and PFIQ were used. We used the same approach to calculating the MD of the ICIQ score for studies in which conservative treatments were considered.
Publication bias across studies
There was no evidence of publication bias in studies with surgical treatments, but there was some evidence of that in studies with conservative interventions. Egger’s test results for publication bias are shown in Figs. 2, 3 and 4

Cumulative mean difference of the effect of surgical intervention on total quality of life score (using the Pelvic Floor Distress Inventory Questionnaire [PFDI])

Cumulative mean difference of the effect of surgical intervention on the total quality of life score (using the Pelvic Floor Impact Questionnaire [PFIQ]-7)

Cumulative mean difference of the effect of conservative interventions on the total quality of life score (using the International Consultation on Incontinence Questionnaire [ICIQ])
Surgical interventions
A total of 28 studies [8, 16–20, 24–26, 28–30, 32–47] had evaluated the effect of surgical interventions on total and other aspects of quality of life. Out of 28 studies, 9 articles [20, 24, 30, 32, 33, 35, 38, 40, 45] had considered just the total quality of life score (Table 1). Four articles had evaluated mesh therapy versus other interventions [20, 24, 32, 45]. In each group of interventions, the difference in quality of life scores before and after surgery was calculated separately. Cystocele prolapse repair [24], colporrhaphy, vaginal repair with mesh, [45] and vaginal mesh, conventional repair [20], and graft in the anterior vaginal wall [32] were various interventions in these studies. In all studies but one [45] the group with mesh intervention had a better quality of life after treatment than before treatment.
In one study, the effect of physiotherapy was evaluated as an adjunct with prolapse surgery. In this study the women in the adjunct group had a better quality of life than the other group [40]. Ten out of 32 studies had assessed the effect of surgical interventions on social, mental, and physical aspects of quality of life using different tools such as the RAND-36 (RAND 36-item Health Survey), the SF-36 (36-Item Short-Form Health Survey), the KHQ (King’s Health Questionnaire), the POP-Q (Pelvic Organ Prolapse Questionnaire), the P-QOL(Prolapse Quality of Life Questionnaire), and the IIQ (Incontinence Impact on the Quality of life) [8, 14, 25, 28, 29, 36, 37, 41, 42, 44]. In these studies a variety of surgical methods were used. The results of these surgical interventions with regard to mental and social aspects of the quality of life were very different. Also, 19 studies evaluated the physical aspects of the quality of life after surgery [8, 16–18, 21, 25–29, 34, 36, 37, 39, 41–44, 46]. Various tools such as the SF36, the UDI (Urogenital Distress Inventory), the IIQ, the KHQ, the ICI (International Consultation on Incontinence), the RAND-36, the SF-36, the PISQ-12 (Prolapse/Urinary Incontinence Sexual Questionnaire), the P-QOL, and the POP-Q (Pelvic Organ Prolapse Quantification system) were used in the studies mentioned. In all 19 articles, the physical aspect of the quality of life was better after treatment than before intervention.
The first study using the PFDI and PFIQ-7 in our meta-analysis compared conventional laparoscopic and robot-assisted laparoscopic sacrocolpopexy as different interventions for vaginal apex prolapse in a single-center, blinded, randomized trial. The authors showed that the robotic approach has a longer operating time, with high pain and cost versus laparoscopic sacrocolpopexy. Finally, this study showed that laparoscopic sacrocolpopexy can improve QOL more than intervention [16].
The second study was a randomized controlled trial that had compared vaginal prolapse repair with and without mesh. The authors showed that there is no significant difference in the improvement of QOL between groups. Objective and subjective recovery were seen after vaginal prolapse repair with or without mesh [17].
The other study had evaluated outcomes of a randomized controlled trial comparing polypropylene mesh-reinforced anterior vaginal prolapse repair versus anterior colporrhaphy. This study showed that repair with polypropylene mesh reinforcement has a lower anatomical recurrence than anterior colporrhaphy at 1 year. However, QOL was improved in both groups [18].
There was a study in which the outcomes of three different rectocele repair techniques were compared. In this study, the results of posterior colporrhaphy and site-specific rectocele repairs were similar in anatomical and functional outcomes. The addition of a porcine-derived graft did not improve the anatomical outcomes. All three methods resulted an obvious improvement in QOL [19].
Finally, the last study had examined the outcomes of traditional vaginal prolapse surgery without mesh versus vaginal surgery with mesh in a double-blind, multicenter, randomized, controlled trial. There was no significant difference in overall objective and subjective healing rates between the two groups [20].
The MD in changing the total quality of life score with 95 % CI for surgical treatment using the PFDI was 74.03 (66.36–81.69; Fig. 2). The mean difference in changing the total quality of life score with 95 % CI for surgical treatment using the PFIQ-7 was 44.57 (22.53–66.65; Fig. 3).
Conservative interventions
We included four studies [2, 14, 21, 31] in the systematic review to assess the effect of conservative interventions on quality of life. One study had assessed mental, social, and physical aspects of QOL [14]. In this study pelvic floor muscle training for the treatment of pelvic organ prolapse was evaluated in an assessor-blinded, randomized, controlled trial. The authors could not show any significant difference in changing the quality of life score based on social, mental, and physical aspects of the quality of life [14].
All four articles had evaluated the physical aspects of QOL after conservative interventions using different tools [2, 14, 21, 31]. Two studies had evaluated the effect of pelvic floor training (PFT) on the total quality of life in women with prolapse using the ICIQ [2, 21] .
We used these two studies in meta-analysis to assess the effect of PFT on QOL. The first one was a multi-centre randomized controlled trial in which pelvic floor muscle training (PFMT) was assessed on POP. The second study had evaluated the effect of the Colpexin sphere on pelvic floor muscle strength, quality of life, and prolapse stage [21].
The mean difference in changing of the total quality of life score with 95 % CI using the ICIQ in these two studies was 1.32 (−2.84 to 5.48) for conservative treatments (Fig. 3).
Discussion
In this systematic review/meta-analysis we found that surgical interventions could improve the total quality of life in women with pelvic organ prolapse. In particular mesh repair in pelvic organ prolapse surgery can improve quality of life in women versus specific repair, graft, and conventional repair. Only in one study did colporrhaphy have a better impact on the quality of life versus mesh in vaginal repair [45]. Improvement in the prolapse and urinary subscales of the PFDI-20 and PFIQ-7 were more significant in the polypropylene mesh cure than the anterior colporrhaphy group [18]. The effect of physiotherapy as an adjunct to prolapse surgery was very effective in improving quality of life [21]. Some studies had assessed social, mental, and physical aspects of quality of life with different tools [8, 25, 28, 29, 36, 37, 41, 42, 44]. We could not carry out a meta-analysis on these studies owing to high heterogeneity (based on I2) and using different devices. Based on a systematic review of these studies, we found that surgical interventions can improve the physical aspects of QOL too. Physical role and function improve after surgical interventions, such as tension-free vaginal tape and colposuspension [42].
Two out of four studies on PFT interventions evaluated total QOL [2, 21] with the same measures (ICIQ). In the first one, two groups under study (PFMT versus lifestyle advice sheet ) had a better QOL over time without any significant difference between groups [2]. There were no reports on the significant difference in ICIQ score over time in this study. In the second study the Colpexin sphere plus pelvic floor muscle exercise (intervention group) had been used versus exercise only (control group). The authors showed that QOL was better after intervention in both groups [21]. In this study there was no significant difference for the QOL domain of the ICIQ score in both groups after 16 weeks of intervention compared with baseline. However, in a meta-analysis of these two studies we could not find any significant difference in ICIQ score over time. The main reason could be the small sample size (just two studies) in the meta-analysis. The other reason could be the actual effect of these interventions on QOL in women with POP. This means that these interventions could not change QOL significantly over time. Also, assessment of heterogeneity for these two papers could be not significant owing to the small sample size. This is a common problem with meta-analysis if there are only a few articles. Because of low number of papers included, the chance of a type two error could be increased. Therefore, we could not reject the null hypothesis of low heterogeneity.
There was no significant improvement in the physical, mental, and social aspects of QOL in patients with POP in another study of the use of PFMT as a conservative intervention either [14]. This study was not included in the meta-analysis owing to the use of different tools to assess QOL.
We found that women who had undergone multiple surgical procedures such as vaginal, abdominal, laparoscopic, or robotic surgery, had a better QOL compared with pre-intervention stage. Also, surgical interventions were effective in improving mental, social, and physical aspects of quality of life. One explanation for these findings is the rapid improvement of symptoms such as urinary incontinence, pelvic pain, dyspareunia, and fecal incontinence which leads to improvement, especially of the physical aspects of the quality of life [48]. Although postoperative outcomes such as bleeding, postoperative pain, anemia, enforced bed rest, and fasting in the first few hours after surgery are very uncomfortable, the benefits gained from the rapid improvement of symptoms could compensate for these complications [49].In some patients, postoperative complications such as recurrent prolapse many years after surgery can cause the patients to require surgery again [50]. However, the patient’s quality of life improvement and rapid recovery after surgery makes this intervention less unpleasant for them. Conservative therapies such as exercise and PFMT did not incur the complications of surgery [21, 25]. Our study showed that these treatments are not effective in improving the quality of life of patients. One explanation for this finding is that conservative treatments are only useful in the early stages of prolapse and are not for the most part useful in advanced prolapse [39]. Ghroubi et al. mentioned that conservative interventions are effective in the primary stages of pelvic organ prolapse. These interventions can improve clinical symptoms and urodynamic parameters, even up to 2 years after treatment [51].
The majority of patients with prolapse see a doctor when their disease has progressed and conservative therapy is no longer useful. This could be another explanation for our findings regarding the effect of PFT treatment on quality of life. It is very important to know that there is no single procedure that improves all prolapse symptoms. Finally, the most important explanation could be the heterogeneity of results and using different tools to avoid us having to pool MD for PFT interventions.
The balance between profit and loss for surgical procedures, such as the duration of the operation, the longer time needed to return to daily activities, and increases in the cost of the procedure should be used for decision making and selecting the type of procedure in the approach to prolapse.
We reduced the heterogeneity of the results by using subgroup analysis. To achieve this goal, only the studies that had used PFDI and PFIQ-7 in conjunction were included in the meta-analysis of surgical treatments. We used the ICIQ for a meta-analysis of the effectiveness of PFT. However, heterogeneity was seen despite this subgroup selection for PFT interventions.
Finally, there is a strong need to conduct further clinical trials in the broad aspects of pelvic prolapse and an understanding of women’s issues arising from complications of prolapse is required.
We carried out a wide search to find relevant studies on changing the quality of life of women after treatment for prolapse. This is the first systematic review on the quality of life of women with prolapse. This study provided powerful evidence of an improvement in the quality of life after surgical treatment for prolapse. Although we tried to avoid bias and errors to identify studies, our study has some limitations. One important limitation was about using different tools to assess quality of life in articles. This problem provided a few studies to use in the meta-analysis and calculation of a pooled effect size, especially for PFT. Also, there was such a wide range of surgical and conservative treatments for prolapse that pooling them was impossible owing to their heterogeneity. The other limitation could be the language restriction of articles to English. This may limit the generalizability of our results.
In conclusion, we found that surgical interventions to treat prolapse can improve quality of life for women. There was a relative effect of PFT treatments on the total quality of life of women with prolapse in systematic review. This effect was not seen in the meta-analysis, probably because we found few eligible studies to be able to pool the effect size.
References
Haylen BT, de Ridder D, Freeman RM, Swift SE, Berghmans B, Lee J, et al. (2010) An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J 21(1):5–26
Hagen S, Stark D, Glazener C, Sinclair L, Ramsay I (2009) A randomized controlled trial of pelvic floor muscle training for stages I and II pelvic organ prolapse. Int Urogynecol J Pelvic Floor Dysfunct 20(1):45–51
Ghanbari Z, Eftekhar T, Goodarzi SH, Haj Baratali B, Bashiri SA, Shariat M (2009) Posterior intravaginal slingplastyversus abdominal sacrocolpopexy for the treatment of vaginal prolapse. Tehran Univ Med J (TUMJ) 67(3):215–220
Elias Kovoor PH (2008) Assessment and management of pelvic organ prolapse. Obstet Gynaecol Reprod Med 18(9):241–246
Borello-France DFHV, Brown MB, Goode P, Kreder K, Scheufele LL, Weber AM (2007) Pelvic-floor muscle function in women with pelvic organ prolapse. Phys Ther 87(4):399–407
Smith DA (2007) Pelvic organ prolapse. A new option offers effectiveness and ease of use. Adv Nurse Pract 15(8):39–42
Wagner TH, Hu T (1998) Economic costs of urinary incontinence in 1995. Urology 51(3):355–361
Abdel-Fattah M, Ramsay I, Pringle S, Hardwick C, Ali H, Young D et al (2011) Evaluation of transobturator tension-free vaginal tapes in management of women with recurrent stress urinary incontinence. Urology 77(5):1070–1075
Sotirios Vimplis PH (2005) Assessment and management of pelvic organ prolapse. Curr Obstet Gynaecol 15:387–393
Natale F, La Penna C, Padoa A, Agostini M, Panei M, Cervigni M (2010) High levator myorraphy versus uterosacral ligament suspension for vaginal vault fixation: a prospective, randomized study. Int Urogynecol J 21(5):515–522
Jelovsek JEBM (2006) Women seeking treatment for advanced pelvic organ prolapse have decreased body image and quality of life. Am J Obstet Gynecol 194(5):1455–1461
Hagen S, Stark D (2011) Conservative prevention and management of pelvic organ prolapse in women. Cochrane Database Syst Rev 7(12):CD003882
Lopes ED, Lemos NL, Carramao Sda S, Lunardelli JL, Ruano JM, Aoki T et al (2010) Transvaginal polypropylene mesh versus sacrospinous ligament fixation for the treatment of uterine prolapse: 1-year follow-up of a randomized controlled trial. Int Urogynecol J 21(4):389–394
Stüpp L, Resende AP, Oliveira E, Castro RA, Girao MJ, Sartori MG (2011) Pelvic floor muscle training for treatment of pelvic organ prolapse: an assessor-blinded randomized controlled trial. Int Urogynecol J 22(10):1233–1239
Hendrix SLCA, Nygaard I, Aragaki A, Barnabei V, McTiernan A (2002) Pelvic organ prolapse in the Women’s Health Initiative: gravity and gravidity. Am J Obstet Gynecol 186(6):1160–1166
Paraiso MF, Jelovsek JE, Frick A, Chen CC, Barber MD (2011) Laparoscopic compared with robotic sacrocolpopexy for vaginal prolapse: a randomized controlled trial. Obstet Gynecol 118(5):1005–1013
Sokol AI, Iglesia CB, Kudish BI, Gutman RE, Shveiky D, Bercik R et al (2012) One-year objective and functional outcomes of a randomized clinical trial of vaginal mesh for prolapse. Am J Obstet Gynecol 206(1):86 e1–86 e9
Nguyen JN, Burchette RJ (2008) Outcome after anterior vaginal prolapse repair: a randomized controlled trial. Obstet Gynecol 111(4):891–898
Paraiso MF, Barber MD, Muir TW, Walters MD (2006) Rectocele repair: a randomized trial of three surgical techniques including graft augmentation. Am J Obstet Gynecol 195(6):1762–1771
Iglesia CB, Sokol AI, Sokol ER, Kudish BI, Gutman RE, Peterson JL et al (2010) Vaginal mesh for prolapse: a randomized controlled trial. Obstet Gynecol 116(2 Pt 1):293–303
Manonai J, Harnsomboon T, Sarit-apirak S, Wattanayingcharoenchai R, Chittacharoen A, Suthutvoravut S (2012) Effect of Colpexin Sphere on pelvic floor muscle strength and quality of life in women with pelvic organ prolapse stage I/II: a randomized controlled trial. Int Urogynecol J 23(3):307–312
Dinnes JDJ, Kirby J, Roderick P (2005) A methodological review of how heterogeneity has been examined in systematic reviews of diagnostic test accuracy. Health Technol Assess 9(12):1–113
Huedo-Medina T, Sanchez-Meca J, Marin-Martinez, F, Botella, J (2006) Assessing heterogeneity in metaanalysis: Q statistic or I2 index? CHIP Documents. Paper 19
Sivaslioglu AA, Unlubilgin E, Dolen I (2008) A randomized comparison of polypropylene mesh surgery with site-specific surgery in the treatment of cystocoele. Int Urogynecol J Pelvic Floor Dysfunct 19(4):467–471
Roovers JP, van der Bom JG, van der Vaart CH, van Leeuwen JH, Scholten PC, Heintz AP (2005) A randomized comparison of post-operative pain, quality of life, and physical performance during the first 6 weeks after abdominal or vaginal surgical correction of descensus uteri. Neurourol Urodyn 24(4):334–340
Maher CF, Qatawneh AM, Dwyer PL, Carey MP, Cornish A, Schluter PJ (2004) Abdominal sacral colpopexy or vaginal sacrospinous colpopexy for vaginal vault prolapse: a prospective randomized study. Am J Obstet Gynecol 190(1):20–26
Guerette NL, Peterson TV, Aguirre OA, VanDrie DM, Biller DH, Davila GW (2009) Anterior repair with or without collagen matrix reinforcement a randomized controlled trial. Obstet Gynecol 114(1):59–65
Feldner PC Jr, Castro RA, Cipolotti LA, Delroy CA, Sartori MG, Girao MJ (2010) Anterior vaginal wall prolapse: a randomized controlled trial of SIS graft versus traditional colporrhaphy. Int Urogynecol J 21(9):1057–1063
Natale F, La Penna C, Padoa A, Agostini M, De Simone E, Cervigni M (2009) A prospective, randomized, controlled study comparing Gynemesh®, a synthetic mesh, and Pelvicol®, a biologic graft, in the surgical treatment of recurrent cystocele. Int Urogynecol J Pelvic Floor Dysfunct 20(1):75–81
Costantini E, Lazzeri M, Bini V, Del Zingaro M, Zucchi A, Porena M (2008) Burch colposuspension does not provide any additional benefit to pelvic organ prolapse repair in patients with urinary incontinence: a randomized surgical trial. J Urology 180(3):1007–1012
Brækken IH, Majida M, Engh ME, Bø K (2010) Can pelvic floor muscle training reverse pelvic organ prolapse and reduce prolapse symptoms? An assessor-blinded, randomized, controlled trial. Am J Obstet Gynecol 203(2):170.e1–170.e7
Menefee SA, Dyer KY, Lukacz ES, Simsiman AJ, Luber KM, Nguyen JN (2011) Colporrhaphy compared with mesh or graft-reinforced vaginal paravaginal repair for anterior vaginal wall prolapse: a randomized controlled trial. Obstet Gynecol 118(6):1337–1344
Schierlitz L, Dwyer PL, Rosamilia A, Murray C, Thomas E, De Souza A et al (2008) Effectiveness of tension-free vaginal tape compared with transobturator tape in women with stress urinary incontinence and intrinsic sphincter deficiency: a randomized controlled trial. Obstet Gynecol 112(6):1253–1261
De Tayrac R, Mathé ML, Bader G, Deffieux X, Fazel A, Fernandez H (2008) Infracoccygeal sacropexy or sacrospinous suspension for uterine or vaginal vault prolapse. Int J Gynaecol Obstet Off Organ Int Fed Gynaecol Obstet 100(2):154–159
Paraiso MF, Walters MD, Karram MM, Barber MD (2004) Laparoscopic Burch colposuspension versus tension-free vaginal tape: a randomized trial. Obstet Gynecol 104(6):1249–1258
Maher CF, Feiner B, DeCuyper EM, Nichlos CJ, Hickey KV, O’Rourke P (2011) Laparoscopic sacral colpopexy versus total vaginal mesh for vaginal vault prolapse: a randomized trial. Am J Obstet Gynecol 204(4):360 e1–360 e7
Dietz V, van der Vaart CH, van der Graaf Y, Heintz P, Schraffordt Koops SE (2010) One-year follow-up after sacrospinous hysteropexy and vaginal hysterectomy for uterine descent: a randomized study. Int Urogynecol J 21(2):209–216
Costantini E, Lazzeri M, Bini V, Del Zingaro M, Zucchi A, Porena M (2011) Pelvic organ prolapse repair with and without prophylactic concomitant Burch colposuspension in continent women: a randomized, controlled trial with 8-year followup. J Urol 185(6):2236–2240
Jarvis SK, Hallam TK, Lujic S, Abbott JA, Vancaillie TG (2005) Peri-operative physiotherapy improves outcomes for women undergoing incontinence and or prolapse surgery: results of a randomised controlled trial. Aust N Z J Obstet Gynaecol 45(4):300–303
Frawley HC, Phillips BA, Bo K, Galea MP (2010) Physiotherapy as an adjunct to prolapse surgery: an assessor-blinded randomized controlled trial. Neurourol Urodynam 29(5):719–725
Vollebregt A, Fischer K, Gietelink D, van der Vaart CH (2011) Primary surgical repair of anterior vaginal prolapse: a randomised trial comparing anatomical and functional outcome between anterior colporrhaphy and trocar-guided transobturator anterior mesh. BJOG Int J Obstet Gynaecol 118(12):1518–1527
Ward KL, Hilton P, UK and Ireland TVT Trial Group (2008) Tension-free vaginal tape versus colposuspension for primary urodynamic stress incontinence: 5-year follow up. BJOG Int J Obstet Gynaecol 115(2):226–233
Schierlitz L, Dwyer PL, Rosamilia A, Murray C, Thomas E, De Souza A et al (2012) Three-year follow-up of tension-free vaginal tape compared with transobturator tape in women with stress urinary incontinence and intrinsic sphincter deficiency. Obstet Gynecol 119(2 Pt 1):321–327
Withagen MI, Milani AL, den Boon J, Vervest HA, Vierhout ME (2011) Trocar-guided mesh compared with conventional vaginal repair in recurrent prolapse: a randomized controlled trial. Obstet Gynecol 117(2 Pt 1):242–250
Carey M, Higgs P, Goh J, Lim J, Leong A, Krause H et al (2009) Vaginal repair with mesh versus colporrhaphy for prolapse: a randomised controlled trial. BJOG Int J Obstet Gynaecol 116(10):1380–1386
Madhuvrata P, Glazener C, Boachie C, Allahdin S, Bain C (2011) A randomised controlled trial evaluating the use of polyglactin (Vicryl) mesh, polydioxanone (PDS) or polyglactin (Vicryl) sutures for pelvic organ prolapse surgery: outcomes at 2 years. J Obstet Gynaecol 31(5):429–435
Guerette NL, Peterson T, Aguirre OA, Vandrie DM, Biller DH, Davila GW (2009) Anterior repair with or without collagen matrix reinforcement: a randomized controlled trial. Obstet Gynecol 114(1):59–65
Bui CBM, Chereau E, Guillo E, Darai E (2010) Résultats fonctionnels et qualité de vie après double promontofixation coelioscopique pour la cure du prolapsus génital. Gynecol Obstet Fertil 38(10):563–568
Cundiff GW, Amundsen CL, Bent AE, Coates KW, Schaffer JI, Strohbehn K et al (2007) The PESSRI study: symptom relief outcomes of a randomized crossover trial of the ring and Gellhorn pessaries. Am J Obstet Gynecol 196(4):405 e1–405 e8
Culligan PJ, Goldberg RP, Sand PK (2003) A randomized controlled trial comparing a modified Burch procedure and a suburethral sling: long-term follow-up. Int Urogynecol J Pelvic Floor Dysfunct 14(4):229–233, discussion 233
Ghroubi S, Kharrat O, Chaari M, Ben Ayed B, Guermazi M, Elleuch MH (2008) Effect of conservative treatment in the management of low-degree urogenital prolapse. Ann Readapt Med Phys 51(2):96–102
Acknowledgements
The authors would like to thank Dr. Aliakbar Haghdoost, for his kind consultation at the analysis stage.
Funding
This study was funded by Tehran University of Medical Sciences.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Doaee, M., Moradi-Lakeh, M., Nourmohammadi, A. et al. Management of pelvic organ prolapse and quality of life: a systematic review and meta-analysis. Int Urogynecol J 25, 153–163 (2014). https://doi.org/10.1007/s00192-013-2141-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00192-013-2141-8