
Abstract
Purpose
Which total knee arthroplasty (TKA) design represents the better solution to restore a correct knee biomechanics is still debated. The aim of this study was to compare posterior stabilized (PS) and cruciate retaining (CR) version of the same TKA design (femoral component with an anatomic sagittal radius—J-curve design) by the use of dynamic Roentgen stereophotogrammetric analysis (RSA). The hypothesis was that the two models influence differently in vivo knee kinematic.
Methods
A cohort of 16 randomly selected patients was evaluated 9 months after surgery: Zimmer PERSONA® was implanted, eight with CR design and eight with PS design. The kinematic evaluations were performed using a Dynamic RSA (BI-STAND DRX 2) developed in our Institute, during the execution of the sit-to-stand motor task. The motion parameters were obtained using the Grood and Suntay decomposition and the low-point kinematics methods.
Results
PS TKA lateral femoral compartment had a wider anterior translation (17 ± 2 mm) than the medial one (11 ± 2 mm), while the two compartments of CR TKA showed a similar anterior translation (medial: 9 ± 2 mm/lateral: 11 ± 2 mm). T test for comparison between CR and PS TKA of antero-posterior translation showed a statistically significant difference (p < 0.05) in the flexion range between 15° and 40°. The CR prosthesis did not anteriorly translate during flexion. The PS design translated anteriorly showing a roll-forward mechanism during extension from 80° to 18° of flexion and a posterior translation from 18° to 0°. The same significant differences (p < 0.05) between the PS and CR groups were found comparing the low-point positions of the femoral condyles in the range of flexion between 25° and 40° for the medial compartment and between 15° and 25° for the lateral compartment.
Conclusions
Dynamic RSA was able to investigate for the first time in vivo the kinematic behaviour of PS and CR version of the same TKA J-curve design. PS type showed a medial pivot during sit-to-stand motion task, while the CR type showed a cylindrical movement. Further studies are needed to evaluate the impact of different TKA designs on clinical results.
Level of evidence
IV.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Many new total knee arthroplasty (TKA) designs have been developed during years and the modern ones have nowadays reached in 83% of the cases a survival rate up to 25 years [1]. However, more than 20% of patients are still not satisfied in terms of pain relief and clinical improvement [2]. Which design represents the better solution to restore a correct knee biomechanics is still debated. The role of posterior cruciate ligament (PCL) in TKA and the level of constraint given by the polyethylene insert appears to be one of the most crucial topic [3,4,5,6]. The cruciate retaining (CR) design preserves the posterior cruciate ligament (PCL) and its role of primary stabilizer in antero-posterior translations, influencing joint stability and kinematics [7]. This implant disadvantage is that the surgical balance of the PCL is not always easy and that sometimes the ligament can result insufficient. On the contrary, in posterior stabilized (PS) prosthesis, the PCL is resected and substituted with a “Post and Cam mechanism” which should avoid paradoxical anterior translation of the femur during knee flexion (roll-forward) and allow a greater range of motion (ROM) [8,9,10]. To evaluate joint kinematics in vivo, under weight-bearing conditions, Roentgen stereophotogrammetric analysis (RSA) appears to be one of the most accurate techniques (based on the principles of optical photogrammetry) through the measurement of micromotions between two rigid bodies in three-dimensional space [11]. The purpose of the present study was to compare the biomechanical behaviour of two different prosthetic models, CR and PS version of a multi-radius J-curve design using a model-based dynamic RSA that had already shown to be able to asses TKA biomechanical properties [12]. This work is focused on the PERSONA® (Zimmer Inc, Warshaw, Indiana, USA) which has been highlighted as one of the best TKA designs in meeting the morphological variability of the distal femur across the global population [13]. The PERSONA® CR femoral condyle shape is asymmetric and the posterior lateral part results lower than the medial one. This asymmetry matches the polyethylene insert improving its congruency. The PS femoral condyles, on the contrary, are symmetric and the polyethylene insert shape was developed to facilitate the postero-lateral contact with the femoral component to allow an easier roll-back. The hypothesis of the present study was that a different biomechanical behaviour would be present between the PS and the CR types during chair raising, a weight bearing, in vivo motor task that exemplifies common activities of daily living.
The clinical relevance of the present study is that, understanding biomechanical behaviour of different TKA design we could better understand the impact of the design on the clinical results.
Materials and methods
Patient selection
The number of patients was defined starting from a power analysis. The two populations T test was considered with a p < 0.05. The standard deviation of the two populations was set to 3 mm in AP translations, as reported in the literature [4, 14, 15]. The true difference of means was set to 5 mm. The power value was 0.9. On the basis of this analysis, the number of patients resulted eight subjects per prosthesis design and a total number of 16 subjects.
Thus, a cohort of 16 randomly selected patients was evaluated in this study. The randomization was carried out using a random numbers generator available on the website of Italian National Health System (https://www.servizi.regione.emilia-romagna.it/generatore/). This software generated 16 casual numbers within the interval (1, 45), which were used to select the patients from the waiting list for TKA between January and December 2015.
The inclusion criteria were: (1) age 50–90 years, (2) severe radiographic osteoarthritis (Kellgren–Lawrence grade > 3), and (3) patients scheduled for a primary TKA.
The exclusion criteria were: (1) previous corrective osteotomy on the affected lower limb, (2) post-traumatic arthritis, (3) severe preoperative valgus deformity (hip knee ankle angle > 10°), (4) BMI > 40 kg/m2, (5) rheumatoid arthritis, (6) chronic inflammatory joint diseases, (7) patients with a pre-pathological abnormal gait (amputated, neuromuscular disorders, poliomyelitis, developmental dysplasia of the hip), (8) severe ankle osteoarthritis (Kellgren–Lawrence > 3), (9) severe hip osteoarthritis (Kellgren–Lawrence > 3), (10) previous total hip or ankle replacement, and (11) unwilling to take part in study and providing HIPAA authorization.
All patients were recruited after signing an informed consent. This study obtained the approval of the Ethics Committee of the IRCCS Rizzoli Orthopaedic Institute (IRB statement: 0012645 approved 2014/04/03).
Computerized randomization was conducted to allocate them in a proportion of 1:1 either to “PS group” or “CR group”.
The patients were divided into groups according to the prosthesis models.
Eight PS: five males, three females, six right knees, two left knees, mean age 68 years (95% CI 50–86), average BMI 30.
Eight CR: two males, six females, two right knees, six left knees, mean age 67 years (95% CI 55–79), average BMI 26.
Motor task
Patients were evaluated at 9-month follow-up (FU). The motor task evaluated for this study was the sit-to-stand: from the sitting position, the patient stands up. The used chair was made of a radiolucent material and had a height of 40 cm. Before starting the acquisition, the position of the image detector was adjusted according to the patient height to centre the knee in the field of view of the detector. The motor task was not standardized, to maintain the natural movement of the body of the patient. The motion test was performed three times. In the first and the second, the patient gain comfort with the experimental setup (no X-ray exposure), in the third, data were acquired (X-ray exposure).
Dynamic RSA
The RSA analysis was performed using an RSA device (BI-STAND DRX 2) developed in IRCCS Rizzoli Orthopaedic Institute, with the collaboration of ASSING (ASSING Group, Rome, Italy). The RSA device has two X-ray tubes (RTM 101HS, IAE, Milan, Italy) and two digital flat panels (PIXIUM RF4343, Thales Electron Devices S.A, Vélizy-Villacoublay, France). The two beamlines were positioned perpendicular to each other, as showed in Fig. 1.

Beamlines setup used for the dynamic RSA evaluations of the patients
The beamlines are synchronized to acquire two contemporary set images with a frame rate of eight frame for seconds (fps). The X-ray equipment was set at 70 kV, 125 mA, with AEC enabled at the image centre. During the acquisition, a solid-state dosimeter (Unfors Multi-O-meter 510L, Unfors RaySafe AB, Billdal, Sweden) was posed at the beam centre. The total measured dose was 3.0 ± 0.1 mGy. After motor task, the images of the calibration box (50 kV, 50 mA) were acquired to perform the data analysis and 3D reconstruction of the RSA scene.
Data analysis
The RSA images were processed using MATLAB® (R2016a, The MathWorks Inc., Natick, MA, USA) using the Model-Based RSA (MBRSA) algorithms [16,17,18] (Fig. 2).

Screenshot of the model-based positioning software used to process the RSA data. A PS model is shown
The output of the image processing was a 3D reconstruction of the movement of femur and tibia. The kinematical quantitative data for each patient were calculated using the Grood and Suntay decomposition [19, 20] and the contact areas between femur and tibia (low point).
The reference systems associated to femur and tibia are shown in Fig. 3.

Position of the femoral and tibial reference systems used in the RSA processing
The X-axis was chosen from medial to lateral direction and used to evaluate the flexion angle. The Y-axis was orientated from posterior to anterior direction and used to evaluate the anterior–posterior translations. The Z-axis was directed perpendicularly with respect to the other axes (Fig. 3).
Statistical analysis
The accuracy of the Dynamic RSA system was 1 mm for translations and 1° for rotations. The analyzed populations were so variable that the evaluated standard deviations were 4 mm and 4°. For this reason, the uncertainties associated to the results were evaluated according to the JCGM100 definition [21]. Thus, uncertainties of 1.4 mm and 1.4° have to be considered for all data in the following section. The groups (PS and CR) were compared to evaluate statistically significant differences during the motor task between the different prosthesis models. The comparison was performed using T test (p < 0.05). The T test was applied by pairing the kinematic data according to the normalized time. In this way, significant differences can be detected in specific moments of the motor task.
The compared kinematical parameters were: anterior/posterior translations, and the lowest point position of the femoral condyles (medial/lateral) with respect to the tibial component.
Results
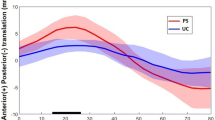
Regarding the anterior/posterior translation of the femur with respect to the tibia, a statistically significant difference between the two groups (p < 0.05) has been found between 15° and 40° of knee flexion with a translation difference from 5.1 ± 1.4 mm at 18° to 2.4 ± 1.4 mm at 40° (Fig. 4).

Plots of the anterior/posterior displacements of the PS and CR models. Bracket indicates the significant difference range
Moreover, the PS model shows an anterior translation, from − 3.1 ± 1.4 mm to 5.4 ± 1.4 mm during the movement between 80° and 18° of knee flexion and a posterior movement, from 5.4 ± 1.4 mm to 0.9 ± 1.4 mm, from 18° to 0° of knee flexion. On the contrary, the CR model does not show any significant translation during the whole motor task, and ranges from − 1.4 ± 1.4 mm to a maximum of 0.9 ± 1.4 mm.
Regarding the low-point kinematic of the medial compartment of the femur with respect to the tibia, a statistically significant difference (p < 0.05) has been found between 25° and 40° of knee flexion, with differences from 3.0 ± 1.4 mm to 3.8 ± 1.4 mm (Fig. 5).

Plots of the low-point positions of the femoral medial compartment of the PS and CR models. Bracket indicates the significant difference range
Regarding the low-point kinematic of the lateral compartment of the femur with respect to the tibia, a statistically significant difference (p < 0.05) was found between 15° and 25° of knee flexion, with differences from 2.0 ± 1.4 mm, to 3.8 ± 1.4 mm (Fig. 6).

Plots of the low-point positions of the femoral lateral compartment of the PS and CR models. Bracket indicates the significant difference range
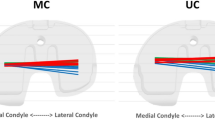
A comparison of the low-point ranges between PS and CR models is represented in Fig. 7 and in Table 1.

Plots of the low-point kinematic during the sit-to-stand of the PS and CR models
The internal–external (IE) and varus–valgus (VV) rotations did not show any statistically significant difference between CR and PS models.
Discussion
The most important finding of the present study is that the PS model of a J-curve TKA design showed wider medial pivoting compared to the CR model in the described setting using Dynamic RSA. During years, a great number of knee prosthesis design have been proposed, always with the goal to resemble as much as possible the normal knee motion and to achieve satisfactory clinical result for the patients. One of these new TKA is the PERSONA® which peculiarity is the femoral component with an anatomic sagittal radius (J-curve design). The PERSONA® CR type femoral condyle shape is asymmetric, and its lateral side is thinner than the medial one.
The PERSONA® PS type on the other hand, has symmetric femoral condyles. Even though this specific prosthesis have been already studied in terms of clinical outcomes [14, 22], and femoral component fit [13] to the authors’ knowledge, its kinematical features have never been investigated in vivo during the execution of motor tasks simulating activities of daily living.
The differences found in this study were statistically significant in terms of AP translation and low-point contact areas. Those parameters are the most affected by the presence or absence of the PCL as an AP translational stabilizer of the joint [23].
Concerning AP translations, the significant difference occurred in the range from 40° to 10° of flexion. The CR design seems not to translate and remains substantially in the same position during the whole range of extension (Fig. 4). The different prosthetic types and the functionality of the PCL can explain the different translation pattern. PS TKA femoral component, indeed, has a roll-forward movement during extension and, when the post engages the cam, the constraints make the femur slide backward in the final part of the extension, avoiding anterior luxation. Otherwise, the spared PCL in the CR TKA was not able to induce a similar anterior translation.
Focusing on low-point kinematic, it was possible to understand better the medial and lateral compartment behaviours. Figures 5 and 6 show that the CR TKA lateral compartment had an anterior translation slightly greater than the medial side. The difference between the medial and lateral side translation of the PS TKA femoral component was more significant. Therefore, if both prostheses performed a medial pivot, it resulted more evident for the PS group. This difference can be ascribed to polyethylene shape of the CR design which is highly congruent to femoral condyles, avoiding anterior paradoxical translation but also limiting the movement of the two compartments.
However, the overall behaviour of both PS and CR TKA agrees with the normal knee motion as described by Komistek et al. [24]. Using uniplanar fluoroscopy during sit-to-stand, they found an anterior translation of femoro-tibial contact areas, greater for the lateral compartment than the medial one. Our results were, also, in line with a Banks and Hodge [25] study which collected 213 TKA knees. The patients performed stair stepping under fluoroscopic control. They found that the PS TKAs analyzed had a medial centre of rotation (75%) while in CR TKAs it was lateral (63%).
In addition, Carvalho [26] found a significantly lower femoral roll back in terms of AP translation, in CR prosthesis than in PS prosthesis, in a fluoroscopic model-based study on 38 knees.
However, the kinematical pattern observed in this study appears in contrast with other different comparative studies of CR and PS designs [27, 28]. Yoshiya’s work, during weight-bearing deep knee bend, found that CR TKA performed a significant anterior shift of both medial and lateral side between 30° and 60° of flexion. On the contrary, PS TKA compartments remained almost constant throughout the range of motion [28].
Banks et al. [27] conducted an in vivo analysis with uniplanar fluoroscopy on a stair climb task that exhibited significantly lower ranges of femoral condylar translation for PS group, than PCL-retaining TKAs which also showed a larger lateral condylar translations with respect to the medial condyle. The authors explained these findings stating that the PCL exerted greater medial constraint when fully maintained.
Most of the differences found in the literature with the results presented in the present study could be due to PCL. This ligament alone, in fact, seemed not able to give enough constraint and induce a medial pivot in CR group as wide as in PS group. This is supported by Tang et al. [5] who evaluated the intra-articular forces in PS and CR TKA. They showed that PCL distributed forces more equally on medial and lateral sides whereas the presence of the post and cam mechanism facilitated the medial pivot and avoided paradoxical AP translations.
If there is accordance, in the literature, about the ability of PS and CR prosthesis to regain a good function [5, 29] and a long-lasting survivorship [1, 9, 30,31,32], biomechanical issues are still present. Not unique results are reported in the literature in terms of AP stability and roll-back mechanism, the majority did not find statistically significant differences [31, 33]. Baier et al. [34] reported only a slight mid-flexion instability in CR group, which did not occur in this study. Other studies detected a paradoxical femoral translation at low flexion angles for both PS and CR TKAs [35, 36], which was not observed in this study.
It is clear that different kinematic results can be obtained with different examination conditions. In vitro studies have the advantage to analyse fewer factors to evaluate the knee movement. On the other hand, in vivo studies can describe the movement in usual daily conditions. The disadvantage is the number of variables that affect the knee kinematics.
Then the implants studied in the literature have diverse features than the PERSONA® TKA. This could be one of the reasons why such different kinematical pattern is demonstrated. In fact, as confirmed by various authors, different geometrical solutions used by different TKA designs affected the kinematical behaviour of operated knees [7, 37].
The present study revealed some important limitations.
First, the motors task performed is not strictly standardized and so reproducible. The reason is that we wanted the patient to perform the movement in the most natural condition. But for this, some patients may had started the movement with a more pronounced external rotation of the knee, and so contact patterns and translations could be influenced by the initial position of the femur relative to the tibia. Due to this, to compare the data of every patient, the data were normalized, thus all the movements started and ended at the same time (see “Materials and methods” for details).
Another limitation concerns the relationship between the ratio of absorbed radiation dose and the numbers of frame per second. To reduce patient’s exposure to radiation, the number of frames per second had to be set a priori, resulting in a limitation of the potential of the instrument.
Third, dynamic RSA evaluation was performed only after surgery, so it was not possible to compare joint kinematics before and after implant. It must be said that this was not an aim of the study: joint kinematics of an arthritic knee is not as the native one and also, involving the use of radiations, it was decided to avoid an excessive exposure.
Further studies are needed to understand the correlation between kinematical behaviour and clinical outcomes.
The clinical relevance of the present study is that understanding biomechanical behaviour of different TKA design we could better understand the impact of the design on the clinical results.
Conclusions
Model-based dynamic RSA proved to be an effective tool in comparing kinematical features of the PS and the CR types of a J-curve TKA. In particular, a statistically significant difference in terms of AP translation and low-point femoral contact areas has been detected between this specific PS and CR TKA. The PS model had a medial pivot movement during knee extension, while the CR model performed a more cylindrical movement. This derives from the specific shape of the CR prosthesis polyethylene which is highly congruent with the femoral component.
Abbreviations
- ACL:
-
Anterior cruciate ligament
- AEC:
-
Automatic exposure control
- AP:
-
Anterior/posterior
- BMI:
-
Body mass index
- fps:
-
frames per second
- FU:
-
Follow-up
- HIPAA:
-
Health Insurance Portability and Accountability Act
- OA:
-
Osteoarthritis
- PCL:
-
Posterior cruciate ligament
- PS:
-
Posterior stabilized
- CR:
-
Cruciate retaining
- RSA:
-
Roentgen stereophotogrammetric analysis
- TKA:
-
Total knee arthroplasty
References
Evans JT, Walker RW, Evans JP, Blom AW, Sayers A, Whitehouse MR (2019) How long does a knee replacement last? A systematic review and meta-analysis of case series and national registry reports with more than 15 years of follow-up. Lancet 393:655–663
Clement ND, Bardgett M, Weir D, Holland J, Gerrand C, Deehan DJ (2018) Three groups of dissatisfied patients exist after total knee arthroplasty: early, persistent, and late. Bone Joint J 100-B:161–169
van den Boom LGH, Brouwer RW, van den Akker-Scheek I, Bulstra SK, van Raaij JJAM (2009) Retention of the posterior cruciate ligament versus the posterior stabilized design in total knee arthroplasty: a prospective randomized controlled clinical trial. BMC Musculoskelet Disord 10:119
Hamai S, Okazaki K, Shimoto T, Nakahara H, Higaki H, Iwamoto Y (2015) Continuous sagittal radiological evaluation of stair-climbing in cruciate-retaining and posterior-stabilized total knee arthroplasties using image-matching techniques. J Arthroplasty 30:864–869
Tang H, Chen H, Yang D, Jiang Y, Zhang C, Zhou Y (2017) Distinctions of introarticular force distribution between genesis-II posterior stabilized and cruciate retaining total knee arthroplasty: an intraoperative comparative study of 45 patients. Clin Biomech (Bristol, Avon) 42:1–8
Verra WC, van den Boom LGH, Jacobs W, Clement DJ, Wymenga AAB, Nelissen RGHH (2013) Retention versus sacrifice of the posterior cruciate ligament in total knee arthroplasty for treating osteoarthritis. Cochrane Database Syst Rev 10:CD004803
Bull AMJ, Kessler O, Alam M, Amis AA (2008) Changes in knee kinematics reflect the articular geometry after arthroplasty. Clin Orthop Relat Res 466:2491–2499
Bignozzi S, Zaffagnini S, Akkawi I, Marko T, Bruni D, Neri MP, Colle F, Marcacci M (2014) Three different cruciate-sacrificing TKA designs: minor intraoperative kinematic differences and negligible clinical differences. Knee Surg Sports Traumatol Arthrosc 22:3113–3120
Li G, Zayontz S, Most E, Otterberg E, Sabbag K, Rubash HE (2001) Cruciate-retaining and cruciate-substituting total knee arthroplasty: an in vitro comparison of the kinematics under muscle loads. J Arthroplasty 16:150–156
Li N, Tan Y, Deng Y, Chen L (2014) Posterior cruciate-retaining versus posterior stabilized total knee arthroplasty: a meta-analysis of randomized controlled trials. Knee Surg Sports Traumatol Arthrosc 22:556–564
Selvik G (1990) Roentgen stereophotogrammetric analysis. Acta Radiol 31:113–126
Bragonzoni L, Marcheggiani Muccioli GM, Bontempi M, Roberti di Sarsina T, Cardinale U, Alesi D, Iacono F, Neri MP, Zaffagnini S (2019) New design total knee arthroplasty shows medial pivoting movement under weight-bearing conditions. Knee Surg Sports Traumatol Arthrosc 27:1049–1056
Dai Y, Scuderi GR, Penninger C, Bischoff JE, Rosenberg A (2014) Increased shape and size offerings of femoral components improve fit during total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc 22:2931–2940
Galea VP, Botros MA, Madanat R, Nielsen CS, Bragdon C (2019) Promising early outcomes of a novel anatomic knee system. Knee Surg Sports Traumatol Arthrosc 27:1067–1074
Kolisek FR, McGrath MS, Marker DR, Jessup N, Seyler TM, Mont MA, Lowry Barnes C (2009) Posterior-stabilized versus posterior cruciate ligament-retaining total knee arthroplasty. Iowa Orthop J 29:23–27
Fong JW-Y, Veljkovic A, Dunbar MJ, Wilson DA, Hennigar AW, Glazebrook MA (2011) Validation and precision of model-based radiostereometric analysis (MBRSA) for total ankle arthroplasty. Foot Ankle Int 32:1155–1163
Gascoyne TC, Morrison JB, Turgeon TR (2014) The effect of patient positioning on the precision of model-based radiostereometric analysis. J Biomech 47:1914–1917
Seehaus F, Emmerich J, Kaptein BL, Windhagen H, Hurschler C (2013) Dependence of model-based RSA accuracy on higher and lower implant surface model quality. Biomed Eng Online 12:32
Dabirrahmani D, Hogg M (2017) Modification of the Grood and Suntay Joint Coordinate System equations for knee joint flexion. Med Eng Phys 39:113–116
Grood ES, Suntay WJ (1983) A joint coordinate system for the clinical description of three-dimensional motions: application to the knee. J Biomech Eng 105:136–144
JCGM (2008) JCGM100: guide to the expression of uncertainty in measurements. https://www.iso.org/sites/JCGM/GUM-JCGM100.htm
Rajgopal A, Aggarwal K, Khurana A, Rao A, Vasdev A, Pandit H (2017) Gait parameters and functional outcomes after total knee arthroplasty using persona knee system with cruciate retaining and ultracongruent knee inserts. J Arthroplasty 32:87–91
Bergfeld JA, McAllister DR, Parker RD, Valdevit AD, Kambic H (2001) The effects of tibial rotation on posterior translation in knees in which the posterior cruciate ligament has been cut. J Bone Joint Surg Am 83:1339–1343
Komistek RD, Dennis DA, Mahfouz M (2003) In vivo fluoroscopic analysis of the normal human knee. Clin Orthop Relat Res 410:69–81
Banks SA, Hodge WA (2004) Implant design affects knee arthroplasty kinematics during stair-stepping. Clin Orthop Relat Res 426:187–193
Carvalho LH, Temponi EF, Soares LFM, Gonçalves MJB (2014) Relationship between range of motion and femoral rollback in total knee arthroplasty. Acta Orthop Traumatol Turc 48:1–5
Banks SA, Markovich GD, Hodge WA (1997) In vivo kinematics of cruciate-retaining and -substituting knee arthroplasties. J Arthroplasty 12:297–304
Yoshiya S, Matsui N, Komistek RD, Dennis DA, Mahfouz M, Kurosaka M (2005) In vivo kinematic comparison of posterior cruciate-retaining and posterior stabilized total knee arthroplasties under passive and weight-bearing conditions. J Arthroplasty 20:777–783
Chaudhary R, Beaupré LA, Johnston DWC (2008) Knee range of motion during the first two years after use of posterior cruciate-stabilizing or posterior cruciate-retaining total knee prostheses. A randomized clinical trial. J Bone Joint Surg Am 90:2579–2586
Abdel MP, Morrey ME, Jensen MR, Morrey BF (2011) Increased long-term survival of posterior cruciate-retaining versus posterior cruciate-stabilizing total knee replacements. J Bone Joint Surg Am 93:2072–2078
Maruyama S, Yoshiya S, Matsui N, Kuroda R, Kurosaka M (2004) Functional comparison of posterior cruciate-retaining versus posterior stabilized total knee arthroplasty. J Arthroplasty 19:349–353
Mayne A, Harshavardhan H, Johnston L, Wang W, Jariwala A (2017) Cruciate Retaining compared with Posterior Stabilised Nexgen total knee arthroplasty: results at 10 years in a matched cohort. Ann R Coll Surg Engl 99:602–606
Kim Y-H, Choi Y, Kwon O-R, Kim J-S (2009) Functional outcome and range of motion of high-flexion posterior cruciate-retaining and high-flexion posterior cruciate-substituting total knee prostheses. A prospective, randomized study. J Bone Joint Surg Am 91:753–760
Baier C, Springorum H-R, Götz J, Schaumburger J, Lüring C, Grifka J, Beckmann J (2013) Comparing navigation-based in vivo knee kinematics pre- and postoperatively between a cruciate-retaining and a cruciate-substituting implant. Int Orthop 37:407–414
Ginsel BL, Banks S, Verdonschot N, Hodge WA (2009) Improving maximum flexion with a posterior cruciate retaining total knee arthroplasty: a fluoroscopic study. Acta Orthop Belg 75:801–807
Murakami K, Hamai S, Okazaki K, Ikebe S, Nakahara H, Higaki H, Shimoto T, Mizu-Uchi H, Kuwashima U, Iwamoto Y (2017) Kinematic analysis of stair climbing in rotating platform cruciate-retaining and posterior-stabilized mobile-bearing total knee arthroplasties. Arch Orthop Trauma Surg 137:701–711
Joglekar S, Gioe TJ, Yoon P, Schwartz MH (2012) Gait analysis comparison of cruciate retaining and substituting TKA following PCL sacrifice. Knee 19:279–285
Funding
This study was partially funded by Zimmer Inc., Warshaw, Indiana, USA.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Ethical approval
This study obtained the approval of the Ethics Committee of the IRCCS Rizzoli Orthopaedic Institute (IRB statement: 0012645 approved 2014/04/03).
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Bontempi, M., Roberti di Sarsina, T., Marcheggiani Muccioli, G.M. et al. J-curve design total knee arthroplasty: the posterior stabilized shows wider medial pivot compared to the cruciate retaining during chair raising. Knee Surg Sports Traumatol Arthrosc 28, 2883–2892 (2020). https://doi.org/10.1007/s00167-019-05645-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-019-05645-6