
Abstract
Recent publications have generated renewed interest in the anatomy of the anterolateral capsule. Knowledge of the biomechanical function of the anterolateral components is lacking. Further research is required to evaluate the influence of the anterolateral capsule on rotatory laxity of the knee. The role of surgical procedures, such as an extra-articular tenodesis or lateral plasty, has to be defined based on quantification of the injury. This article seeks to summarize the current literature and discusses the role of the anterolateral capsule and reconstructive techniques in combined ligamentous knee trauma.
Level of evidence V.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
The interplay between the dynamic and static stabilizers of the knee joint is complex. The lateral side of the knee is especially reliant on these stabilizers due to its inherent bony instability from the opposing convex surfaces [56]. Beyond the collateral and cruciate ligaments of the knee, there are significant strength and stabilizing effects from the lesser-known ligaments of the knee. The first description of an injury to the lateral capsular ligaments was an avulsion fracture [46]. The Segond fracture is said to result from an avulsion of the lateral proximal tibia due to the insertion of a ligamentous structure. Recently, there have been an increased number of publications on the static stabilizers of the anterolateral knee [10].
The nomenclature has varied in the literature including the mid-third lateral capsular ligament [18, 26, 28, 31, 39, 51, 52, 58], anterior oblique band of the fibular collateral ligament (FCL) [6, 27], the capsulo-osseous layer of the iliotibial band [29, 50, 53, 54], or the anterolateral ligament [10, 54, 55]. For the purpose of this article, we will refer to this lateral stabilizing structure as the anterolateral capsule (ALC). The anatomy of the ALC is controversial given that it has interdigitating fibres with the iliotibial band. Often, a capsular thickening rather than a distinct ligament, such as the anterior cruciate ligament (ACL), is present.
Significant clinical interest exists whether ALC injuries in anterior ACL-deficient knees should be surgically addressed at the time of ACL surgery. Some have postulated that a combined intra- and extra-articular reconstruction can achieve improved post-operative stability and may result in a decreased incidence in post-traumatic arthritis. However, biomechanical studies regarding the function of the ALC are lacking. So far, determination of rotatory laxity is mainly based on subjective grading using the pivot shift test. Even though a standardized pivot shift test has been proposed [22], the clinical grading and the tibial translation still vary between examiners.
A better method to test rotatory knee laxity is by quantitative pivot shift testing. An image analysis method, which tracks markers on the lateral knee, was found to accurately calculate lateral compartment translation during the pivot shift [2, 3, 24]. Subsequently, an iPad application was developed to aid in processing of the image capture as well as calculation of translation [23]. An inertial sensor strapped non-invasively to the anterior tibia is another quantitative pivot shift tool [34]. This device is able to calculate acceleration of the proximal tibia during the reduction movement of the pivot shift test and is sensitive to rupture of the ACL [33]. The importance of quantitative pivot shift testing does not only provide objective laxity parameters but more importantly provide side-to-side comparison of the healthy and injured knee.
The purpose of this article was to summarize the current knowledge on the ALC. The clinical relevance is to rationalize the current applications for surgical reconstruction of the ALC structures for anterolateral rotatory instability of the knee.
Material and methods
A comprehensive review of the MEDLINE database was carried out to identify relevant articles using different keywords (e.g. “anterolateral ligament”, “anterolateral capsule”, “anterolateral rotatory laxity”, “lateral structures of the knee”, “Segond fracture”). Our search strategy yielded 1062 articles. Two authors screened the articles and excluded 1020 articles. Articles not written in English, not pertaining to the knee, or not specifically addressing the area of interest or directly associated structures were excluded. The reference lists of the reviewed articles were searched for additional relevant articles. The references were divided into history, anatomy, histology, imaging, biomechanics, and treatment. However, biomechanical, histological, and prospective randomized studies were rare.
History
The structures of the ALC were subjects of multiple research projects during the last century. Segond originally described a pearly, resistant, fibrous band in this area [46]. Hughston later described a lateral capsular ligament as a thickening of the capsule which is divided into anterior, middle, and posterior thirds as well as a division into menisco-femoral and menisco-tibial components [25]. The mid-third lateral capsular ligament was the most structurally important and attached to Segond fragments [51, 57]. The mid-third lateral capsular ligament description has been supported in other anatomic descriptions [29, 39, 52], identified on MRI scans [18, 29], and associated with injuries causing anterolateral laxity [26, 31]. Other studies described an anterior oblique bundle of the FCL, which originated from the FCL in an oblique fashion and inserted at the lateral mid-portion of the tibia and blending with posterior fibres of the iliotibial tract [6, 27]. This description is similar to Hughston’s description of the mid-third capsular ligament stated above. Additionally, the recent literature described an anterolateral ligament to attach anteriorly to the socket from which the FCL originated [10]. This description is also similar since the FCL is known to attach only millimetres away from the lateral femoral epicondyle [30]. The insertion of the ligamentous structure into the tibia was consistent in all of the above papers. It was described as posterior to the insertion of the iliotibial band at Gerdy’s tubercle [6, 18, 26, 27, 29, 31, 39, 51, 52, 55].
The intimate relationship between the anterolateral capsule and the iliotibial band was frequently mentioned in the previous literature. In fact, the capsulo-osseous layer has been called the “true knee anterolateral ligament” and was described to have attachments and orientation similar to Hughston [54]. Attachments between the capsulo-osseous layer of the iliotibial band and the ACL create an inverted horseshoe sling around the posterior femoral condyle preventing the anterolateral tibial subluxation that occurs in the pivot shift test [50]. Because of similar descriptions of the attachment sites and interdigitating fibres [28] between a ligamentous structure in the ALC and the capsulo-osseous layer of the iliotibial band, it is worthwhile to consider that these two structures may be synonymous.
The anterolateral ligament
Recently, there have been a number of new studies dedicated to the anatomy of the ALC. Each article was unique in its surgical approach to identify a ligamentous structure and as a result, the anatomic findings differed. Table 1 lists the number of specimens used, the anthropometric data, and the proposed origins and insertions of the structure for all recent anatomy articles included in this article. Table 2 lists quantitative measurements from these studies for the anatomy of the structure. After resection of the skin, subcutaneous fat tissue, and iliotibial band, different approaches were proposed for visualization. In one approach, the knee was flexed to 60° and an internal torque was applied. All visible distinct fibres were isolated at the proximal tibia, posterior and proximal to Gerdy’s tubercle, and on the lateral femur [10]. In another approach, varus and internal rotational forces were applied between 30° and 60° flexion to highlight any structure coming under tension. Any tissue in the anterolateral region of the knee that did not come under tension was resected, leaving only a ligamentous structure [7]. Other authors placed a Hohmann retractor between the femur and the tibia tightening the lateral joint capsule until a ligament became visible. In addition, they examined 30 patients undergoing knee arthroplasty. In all 30 cases, they identified and dissected a ligamentous structure free from the lateral joint capsule [55]. Dodds et al. [13] disarticulated knees with only the anterolateral structures remaining intact. Then, using transillumination, they identified a potential capsular thickening above and below the lateral meniscus. Sonnery-Cottet et al. [47] arthroscopically identified a ligament both in vivo in patients undergoing treatment for iliotibial band syndrome, and in cadavers followed by an open dissection, to confirm the correct identification of the structure. Another study described the structure as a thickening of the knee joint capsule, which was not always clearly morphologically differentiated from the remainder of the joint capsule [48]. The authors describe a broad, translucent fibrous band connecting the lateral femoral epicondyle to a point on the proximal tibial midway between Gerdy’s tubercle and the fibular head, whose fibres were continuations of the iliotibial band.
The attachments of the ligamentous structures are also controversial. Some studies describe an attachment between the ligament and the lateral meniscus [7, 10, 20, 48]. Other studies claim that the structure does not insert into the rim of the lateral meniscus, although there were branching attachments to it [13]. Still others mention that the majority of fibres came close to the meniscal tissue, but continued without interruption towards the tibial plateau [55].
Recently, a systematic review summarized the different approaches to provide and discuss a universal surgical course of action [43]. The authors conclude that anatomic variability should be taken into account when identifying a ligamentous structure in the area of the ALC.
Histology
In a histological analysis with haematoxylin and eosin, the ALC was compared to the ACL in four knees [7]. The collagen pattern of the structure was organized into individual bundles, indicating that the structure was a combination of multiple thickenings of the lateral joint capsule and not a homogenous entity such as the ACL. However, the femoral and tibial attachments contained more a consistent collagenous pattern, and the transition between the ALC and the mineralized cartilage and bone was indicative of ligamentous tissue. Furthermore, immunohistochemistry and serial sectioning indicated that this part of the ALC has a peripheral nervous innervation and mechanoreceptors [7]. Another study performed histological analysis using haematoxylin and eosin staining on ten specimens after removing the ALC structure en bloc. They concluded that a distinct fibrous structure is present in contact with the synovium [55]. The presence of dense connective tissue with arranged fibres and little cellular material was described in ten specimens [20].
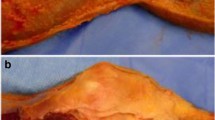
A recent research study [14] performed histology on two specimens that were identified with a thickening of the anterolateral capsule in MRI (Fig. 1). The thickening appeared as a transition from loose connective tissue similar to the capsule to an organized structure similar to ligamentous tissue. In the area of the thickening, elongated nuclei were positioned between aligned collagen. However, the structural organization was not as regular as the FCL.

Histological comparison of the fibular collateral ligament (FCL) (a) and a thickening of the anterolateral capsule (ALC) (b), which was confirmed by MRI prior to the dissection (scale 100 μm)
Imaging
Different qualities of imaging have been proposed to determine the structures of the ALC. What is the role they play in the evaluation of anterolateral laxity? The origin and insertion of a potential ligamentous structure in this area were described in radiographic studies [19, 44]. Historical literature stated that a Segond fracture correlates with an injury of the ALC. A recent study concluded that the avulsion resulted from the attachment of a ligamentous structure [9]. Others mention that the iliotibial band may be involved in the Segond avulsion as well [12]. Summing up, the presence of a Segond fracture on radiographs can be a hint that rotational instability is present.
The structures of the ALC can also be evaluated using ultrasound [8]. However, the gold standard is still evaluation by MRI [49]. A study revealed the presence of a 2–4 mm thickening of the central third of the lateral capsule in 3 of 10 specimens (Fig. 2) [14]. Other studies reported that a ligamentous structure was visualized in 97.4 [21] and 100 % [7]. So far, only one study correlated MRI findings with rotational stability using the iPad technology [23] as described before.

MRI with (a) and without (b) thickening of the lateral capsule (t2 fat sat sequence)
Biomechanics
Lateral instability of the knee is less frequent but more disabling than medial instability of a comparable amount [4]. It is known that similar to the menisci, the anterolateral capsule is a secondary stabilizer of anterior translation and rotation of the lateral compartment [37]. Increased anterior translation in flexion as well as in extension and increased internal rotation at 90° of flexion has been shown to be consistent with combined injury to the anterior cruciate ligament and the anterolateral structures [59]. Moreover, cadaveric navigation studies showed an increase in pivot shift grade after the section of lateral capsule or ALL compared to isolate ACL cut, suggesting its importance in the control of dynamic rotational laxity [37]. Given the previous literature documenting the role of a ligamentous structure in the ALC in anterolateral rotatory stability [6, 26, 28, 31, 46, 58], it seems as though the proposed structure and the capsulo-osseous layer of the iliotibial band are similar biomechanically.
However, there is a paucity of biomechanical studies on the ALC. A recent study measured changes in length of a ligamentous structure in eight knees from 0° to 90° of flexion during neutral, internal, and external rotation torque. Small metal eyelets were screwed into the bone at the origin and the insertion of the ligament. The changes in the distance between the eyelets were measured using a monofilament suture and a linear variable displacement transducer [13]. Another study measured the strain in the structure using polydimethylsiloxane gauges [62]. Both studies conclude that more work is needed to confirm the function.
Recently, a study evaluating the biomechanical function of the capsular structures using robotic technology showed that these structures are important stabilizers of internal rotation at higher knee flexion angles [41].
Quantification of injuries to the ALC is of high importance. The pivot shift test was performed in knees with different steps of injuries including the ACL and ALC and after surgical treatment (ACL reconstruction and extra-articular tenodesis). Tibial motion relative to the femur was tracked by an electromagnetic system during the physical examination. This study showed that either an isolated ACL reconstruction or a combined ACL reconstruction and extra-articular tenodesis restored intact knee kinematics in isolated ACL injury. However, an extra-articular tenodesis was necessary to restore intact kinematics when a lateral capsule lesion was present (unpublished data). A similar effect of the lateral plasty was demonstrated with an in vitro cadaveric study using a navigation system (unpublished data). A new approach to measure rotatory laxity of the knee is optical tracker fixation, which is non-invasive and validated by a commercial free navigation system that showed increased agreement compared with devices measuring tibial rotation by foot position alone [45].
Treatment
A combined intra- and extra-articular reconstruction may provide a more normal restoration of knee kinematics after ACL injury with concomitant anterolateral rotational laxity. Some authors advocate it, due to the longer lever arm of the lateral reconstruction, which may allows efficient control of tibial rotation [16]. Furthermore, the tenodesis may provide a “backup” since it persists in cases of intra-articular graft failure [15]. Finally, the extra-articular tenodesis has been found to decrease the stress on the intra-articular graft by more than 40 %, lending credence to the possible load-sharing role of the native structure [16, 17]. More recently, an extra-articular tenodesis as a minimally invasive anatomic reconstruction of the ALL was described [10] using a gracilis-tendon autograft.
The effects of extra-articular tenodesis have been extensively evaluated with navigation studies. Bignozzi et al. acquired in vivo knee kinematics before and after the execution of lateral tenodesis in adjunct to single bundle “over the top” ACL reconstruction. They proved that the lateral plasty was able to reduce the anterior translation of the lateral compartment during the Lachman test, compared to isolated ACL reconstruction [5]. The same researchers performed also a randomized study aimed to compare single bundle plus lateral plasty with double-bundle reconstruction [61], showing that both techniques worked similarly for static knee laxity, while the lateral plasty technique better controlled tibial rotations and the displacement of lateral compartment during anterior drawer test. Similar biomechanical insights were reported also with different techniques of extra-articular tenodesis, suggesting the lateral tenodesis as a key element to reduce the tibial rotation and control the pivot shift phenomenon [11, 38].
Discussion
The most important finding of the present study was that knowledge regarding the biomechanical function of the anterolateral components of the knee is lacking. This article carefully analyses anterolateral rotatory instability in ligamentous knee trauma to determine the suitability for additional procedures, such as an extra-articular tenodesis.
Biomechanically and anatomically, the structures of the anterolateral capsule have held multiple names throughout history. Recently, there has been a dramatic increase in the number of articles related to these structures. While there is some disagreement in describing anatomy as indicated in Table 1, the majority of historical and current articles state that a ligamentous structure is present, whose origin is close to the lateral femoral epicondyle and whose insertion is slightly inferior to the tibial articular surface posterior to Gerdy’s tubercle. However, there is still broad variation within the literature regarding the frequency with which the ligament can be identified and regarding its nature of capsular thickening or distinct ligament. Biomechanical studies regarding the function of the structure are lacking. Despite this, some authors already propose surgical treatment of ALC injuries. What is known at this time is that the ALC is an important secondary stabilizer to rotatory knee laxity [37]. In cases where anterolateral laxity remains despite an anatomic ACL reconstruction, an extra-articular tenodesis might be beneficial. However, it is important to note that this should be pursued in a minority of patients. The idea of an extra-articular reconstruction was first popularized in the 1970s, when open surgery with patellar tendon graft was the standard procedure for ACL reconstruction [36]. Lemaire in Europe [32], McIntosh in the USA [4], and others introduced extra-articular techniques with the aim of restoring rotatory stability of the knee. With the establishment and advancement of arthroscopic ACL reconstruction, extra-articular procedures became less common. Critics cited the higher pressure on the lateral compartment and the restricted range of motion due to the anterior position of the femoral insertion as disadvantages of the extra-articular tenodesis. Furthermore, in 2001, Anderson et al. [1] failed to show benefit of extra-articular tenodesis over intra-articular ACL reconstruction. However, in recent years, Neyret et al. and Marcacci et al. [35] were able to show excellent long-term results [42] with high satisfaction and few signs of osteoarthritis. Moreover, Zaffagnini et al. [60], through a randomized study, showed higher clinical results and faster return to sport at 5-year follow-up in patients treated with single-bundle ACL reconstruction plus lateral plasty compared to single-bundle four-strand hamstrings or patellar tendon. Moreover, an improved dynamic laxity behaviour of the extra-articular reconstructed knee was reported as well [56].
Advantages and disadvantages have to be considered when anterolateral instability is present. Individualized ACL surgery is the goal to maximize patient’s outcome and functional return. The quantification of the individual injury is the first step to improve the outcome. Non-invasive assessment of pivot shift testing using software loaded on a tablet computer as before mentioned [23, 34] can be used pre-operatively to help grade ACL injury, intra-operatively to help adjust ACL reconstruction in real time, and post-operatively to track ACL graft function during rehabilitation [40].
Further research is required to evaluate the influence of ALC structures on rotatory laxity of the knee. It is of high clinical relevance to establish treatment algorithms and to define the role of additional procedures, such as the extra-articular tenodesis. However, this should be done cautiously and should be delayed until the function of the ALC has been better defined. When an extra-articular tenodesis is performed, the higher pressure on the lateral compartment and the restricted range of motion is a concern that should be discussed with the patients. The post-operative treatment and the physical therapy protocol have to be adapted or tailored to the specific procedure being performed.
Conclusions
Further research is required to evaluate the influence of the ALC on rotatory laxity of the knee. The role of additional procedures, such as an extra-articular tenodesis or lateral plasty, has to be defined based on quantification of the injury to the anterolateral capsule in combined ligamentous knee trauma.
References
Anderson AF, Snyder RB, Lipscomb AB Jr (2001) Anterior cruciate ligament reconstruction. A prospective randomized study of three surgical methods. Am J Sports Med 29(3):272–279
Araujo PH, Ahlden M, Hoshino Y, Muller B, Moloney G, Fu FH, Musahl V (2012) Comparison of three non-invasive quantitative measurement systems for the pivot shift test. Knee Surg Sports Traumatol Arthrosc 20(4):692–697
Bedi A, Musahl V, Lane C, Citak M, Warren RF, Pearle AD (2010) Lateral compartment translation predicts the grade of pivot shift: a cadaveric and clinical analysis. Knee Surg Sports Traumatol Arthrosc 18(9):1269–1276
Bertoia JT, Urovitz EP, Richards RR, Gross AE (1985) Anterior cruciate reconstruction using the MacIntosh lateral-substitution over-the-top repair. J Bone Joint Surg Am 67(8):1183–1188
Bignozzi S, Zaffagnini S, Lopomo N, Martelli S, Iacono F, Marcacci M (2009) Does a lateral plasty control coupled translation during antero-posterior stress in single-bundle ACL reconstruction? An in vivo study. Knee Surg Sports Traumatol Arthrosc 17(1):65–70
Campos JC, Chung CB, Lektrakul N, Pedowitz R, Trudell D, Yu J, Resnick D (2001) Pathogenesis of the Segond fracture: anatomic and MR imaging evidence of an iliotibial tract or anterior oblique band avulsion. Radiology 219(2):381–386
Caterine S, Litchfield R, Johnson M, Chronik B, Getgood A (2014) A cadaveric study of the anterolateral ligament: re-introducing the lateral capsular ligament. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3117-z
Cianca J, John J, Pandit S, Chiou-Tan FY (2014) Musculoskeletal ultrasound imaging of the recently described anterolateral ligament of the knee. Am J Phys Med Rehabil 93(2):186
Claes S, Luyckx T, Vereecke E, Bellemans J (2014) The Segond fracture: a bony injury of the anterolateral ligament of the knee. Arthroscopy. doi:10.1016/j.arthro.2014.05.039
Claes S, Vereecke E, Maes M, Victor J, Verdonk P, Bellemans J (2013) Anatomy of the anterolateral ligament of the knee. J Anat 223(4):321–328
Colombet P (2011) Knee laxity control in revision anterior cruciate ligament reconstruction versus anterior cruciate ligament reconstruction and lateral tenodesis: clinical assessment using computer-assisted navigation. Am J Sports Med 39(6):1248–1254
De Maeseneer M, Boulet C, Willekens I, Lenchik L, De Mey J, Cattrysse E, Shahabpour M (2014) Segond fracture: involvement of the iliotibial band, anterolateral ligament, and anterior arm of the biceps femoris in knee trauma. Skeletal Radiol. doi:10.1007/s00256-014-2044-x
Dodds AL, Halewood C, Gupte CM, Williams A, Amis AA (2014) The anterolateral ligament: anatomy, length changes and association with the Segond fracture. Bone Joint J 96-B(3):325–331
Dombrowski ME, Costello JM, Ohashi B, Murawski CD, Rothrauff BB, Arilla FV, Friel NA, Fu FH, Debski RE, Musahl V (2015) Macroscopic anatomical, histological and magnetic resonance imaging correlation of the lateral capsule of the knee. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-015-3517-8
Draganich LF, Reider B, Ling M, Samuelson M (1990) An in vitro study of an intraarticular and extraarticular reconstruction in the anterior cruciate ligament deficient knee. Am J Sports Med 18(3):262–266
Duthon VB, Magnussen RA, Servien E, Neyret P (2013) ACL reconstruction and extra-articular tenodesis. Clin Sports Med 32(1):141–153
Engebretsen L, Lew WD, Lewis JL, Hunter RE (1990) The effect of an iliotibial tenodesis on intraarticular graft forces and knee joint motion. Am J Sports Med 18(2):169–176
Haims AH, Medvecky MJ, Pavlovich R Jr, Katz LD (2003) MR imaging of the anatomy of and injuries to the lateral and posterolateral aspects of the knee. AJR Am J Roentgenol 180(3):647–653
Helito CP, Demange MK, Bonadio MB, Tirico LE, Gobbi RG, Pecora JR, Camanho GL (2014) Radiographic landmarks for locating the femoral origin and tibial insertion of the knee anterolateral ligament. Am J Sports Med 42(10):2356–2362. doi:10.1177/0363546514543770
Helito CPDM, Bonadio MB, Tirico LEP, Gobbi RG, Pecora JR, Camanho GL (2013) Anatomy and histology of the knee anterolateral ligament. Orthop J Sports Med 1(7):2325967113513546
Helito CP, Helito PV, Costa HP, Bordalo-Rodrigues M, Pecora JR, Camanho GL, Demange MK (2014) MRI evaluation of the anterolateral ligament of the knee: assessment in routine 1.5-T scans. Skeletal Radiol 43(10):1421–1427
Hoshino Y, Araujo P, Ahlden M, Moore CG, Kuroda R, Zaffagnini S, Karlsson J, Fu FH, Musahl V (2012) Standardized pivot shift test improves measurement accuracy. Knee Surg Sports Traumatol Arthrosc 20(4):732–736
Hoshino Y, Araujo P, Ahlden M, Samuelsson K, Muller B, Hofbauer M, Wolf MR, Irrgang JJ, Fu FH, Musahl V (2013) Quantitative evaluation of the pivot shift by image analysis using the iPad. Knee Surg Sports Traumatol Arthrosc 21(4):975–980
Hoshino Y, Kuroda R, Nagamune K, Araki D, Kubo S, Yamaguchi M, Kurosaka M (2012) Optimal measurement of clinical rotational test for evaluating anterior cruciate ligament insufficiency. Knee Surg Sports Traumatol Arthrosc 20(7):1323–1330
Hughston JC, Andrews JR, Cross MJ, Moschi A (1976) Classification of knee ligament instabilities. Part I. The medial compartment and cruciate ligaments. J Bone Joint Surg Am 58(2):159–172
Hughston JC, Andrews JR, Cross MJ, Moschi A (1976) Classification of knee ligament instabilities. Part II. The lateral compartment. J Bone Joint Surg Am 58(2):173–179
Irvine GB, Dias JJ, Finlay DB (1987) Segond fractures of the lateral tibial condyle: brief report. J Bone Joint Surg Br 69(4):613–614
Johnson LL (1979) Lateral capsular ligament complex: anatomical and surgical considerations. Am J Sports Med 7(3):156–160
LaPrade RF, Gilbert TJ, Bollom TS, Wentorf F, Chaljub G (2000) The magnetic resonance imaging appearance of individual structures of the posterolateral knee. A prospective study of normal knees and knees with surgically verified grade III injuries. Am J Sports Med 28(2):191–199
LaPrade RF, Ly TV, Wentorf FA, Engebretsen L (2003) The posterolateral attachments of the knee: a qualitative and quantitative morphologic analysis of the fibular collateral ligament, popliteus tendon, popliteofibular ligament, and lateral gastrocnemius tendon. Am J Sports Med 31(6):854–860
LaPrade RF, Terry GC (1997) Injuries to the posterolateral aspect of the knee. Association of anatomic injury patterns with clinical instability. Am J Sports Med 25(4):433–438
Lemaire M, Combelles F (1980) Plastic repair with fascia lata for old tears of the anterior cruciate ligament (author’s transl). Rev Chir Orthop Reparatrice Appar Mot 66(8):523–525
Lopomo N, Signorelli C, Bonanzinga T, Marcheggiani Muccioli GM, Neri MP, Visani A, Marcacci M, Zaffagnini S (2014) Can rotatory knee laxity be predicted in isolated anterior cruciate ligament surgery? Int Orthop 38(6):1167–1172. doi:10.1007/s00264-014-2287-0
Lopomo N, Zaffagnini S, Signorelli C, Bignozzi S, Giordano G, Marcheggiani Muccioli GM, Visani A (2012) An original clinical methodology for non-invasive assessment of pivot-shift test. Comput Methods Biomech Biomed Eng 15(12):1323–1328
Marcacci M, Zaffagnini S, Giordano G, Iacono F, Presti ML (2009) Anterior cruciate ligament reconstruction associated with extra-articular tenodesis: a prospective clinical and radiographic evaluation with 10- to 13-year follow-up. Am J Sports Med 37(4):707–714
Martens M (2013) The extra-articular lateral tenodesis for an ACL-deficient knee. Aspetar Sports Med J 2(TT1–Football Injuries):170–175
Monaco E, Ferretti A, Labianca L, Maestri B, Speranza A, Kelly MJ, D’Arrigo C (2012) Navigated knee kinematics after cutting of the ACL and its secondary restraint. Knee Surg Sports Traumatol Arthrosc 20(5):870–877
Monaco E, Maestri B, Conteduca F, Mazza D, Iorio C, Ferretti A (2014) Extra-articular ACL reconstruction and pivot shift: in vivo dynamic evaluation with navigation. Am J Sports Med 42(7):1669–1674
Moorman CT 3rd, LaPrade RF (2005) Anatomy and biomechanics of the posterolateral corner of the knee. J Knee Surg 18(2):137–145
Musahl V, Zaffagnini S, Becker R, Karlsson J (2014) Should peripheral structures be addressed in ACL reconstruction? Knee Surg Sports Traumatol Arthrosc 22(9):1964–1965
Parsons EM, Gee AO, Spiekerman C, Cavanagh PR (2015) The biomechanical function of the anterolateral ligament of the knee. Am J Sports Med 43(3):669–674
Pernin J, Verdonk P, Si Selmi TA, Massin P, Neyret P (2010) Long-term follow-up of 24.5 years after intra-articular anterior cruciate ligament reconstruction with lateral extra-articular augmentation. Am J Sports Med 38(6):1094–1102
Pomajzl R, Maerz T, Shams C, Guettler J, Bicos J (2014) A review of the anterolateral ligament of the knee: current knowledge regarding its incidence, anatomy, biomechanics, and surgical dissection. Arthroscopy. doi:10.1016/j.arthro.2014.09.010
Rezansoff AJ, Caterine S, Spencer L, Tran MN, Litchfield RB, Getgood AM (2014) Radiographic landmarks for surgical reconstruction of the anterolateral ligament of the knee. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3126-y
Russell DF, Deakin AH, Fogg QA, Picard F (2014) Repeatability and accuracy of a non-invasive method of measuring internal and external rotation of the tibia. Knee Surg Sports Traumatol Arthrosc 22(8):1771–1777
Segond P (1879) Recherches cliniques et expérimentales sur les épanchements sanguins du genou par entorse. Progrés Méd 7:297–299, 319–321, 340–341
Sonnery-Cottet B, Archbold P, Rezende FC, Neto AM, Fayard JM, Thaunat M (2014) Arthroscopic identification of the anterolateral ligament of the knee. Arthrosc Tech 3(3):e389–e392
Stijak L, Bumbasirevic M, Radonjic V, Kadija M, Puskas L, Milovanovic D, Filipovic B (2014) Anatomic description of the anterolateral ligament of the knee. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-014-3422-6
Taneja AK, Miranda FC, Braga CA, Gill CM, Hartmann LG, Santos DC, Rosemberg LA (2014) MRI features of the anterolateral ligament of the knee. Skeletal Radiol. doi:10.1007/s00256-014-2052-x
Terry GC, Hughston JC, Norwood LA (1986) The anatomy of the iliopatellar band and iliotibial tract. Am J Sports Med 14(1):39–45
Terry GC, LaPrade RF (1996) The biceps femoris muscle complex at the knee. Its anatomy and injury patterns associated with acute anterolateral-anteromedial rotatory instability. Am J Sports Med 24(1):2–8
Terry GC, LaPrade RF (1996) The posterolateral aspect of the knee. Anatomy and surgical approach. Am J Sports Med 24(6):732–739
Terry GC, Norwood LA, Hughston JC, Caldwell KM (1993) How iliotibial tract injuries of the knee combine with acute anterior cruciate ligament tears to influence abnormal anterior tibial displacement. Am J Sports Med 21(1):55–60
Vieira EL, Vieira EA, da Silva RT, Berlfein PA, Abdalla RJ, Cohen M (2007) An anatomic study of the iliotibial tract. Arthroscopy 23(3):269–274
Vincent JP, Magnussen RA, Gezmez F, Uguen A, Jacobi M, Weppe F, Al-Saati MF, Lustig S, Demey G, Servien E, Neyret P (2012) The anterolateral ligament of the human knee: an anatomic and histologic study. Knee Surg Sports Traumatol Arthrosc 20(1):147–152
Wahl CJ, Westermann RW, Blaisdell GY, Cizik AM (2012) An association of lateral knee sagittal anatomic factors with non-contact ACL injury: sex or geometry? J Bone Joint Surg Am 94(3):217–226
Weber WN, Neumann CH, Barakos JA, Petersen SA, Steinbach LS, Genant HK (1991) Lateral tibial rim (Segond) fractures: MR imaging characteristics. Radiology 180(3):731–734
Woods GW, Stanley RF, Tullos HS (1979) Lateral capsular sign: x-ray clue to a significant knee instability. Am J Sports Med 7(1):27–33
Wroble RR, Grood ES, Cummings JS, Henderson JM, Noyes FR (1993) The role of the lateral extraarticular restraints in the anterior cruciate ligament-deficient knee. Am J Sports Med 21(2):257–262
Zaffagnini S, Marcacci M, Lo Presti M, Giordano G, Iacono F, Neri MP (2006) Prospective and randomized evaluation of ACL reconstruction with three techniques: a clinical and radiographic evaluation at 5 years follow-up. Knee Surg Sports Traumatol Arthrosc 14(11):1060–1069
Zaffagnini S, Signorelli C, Lopomo N, Bonanzinga T, Marcheggiani Muccioli GM, Bignozzi S, Visani A, Marcacci M (2012) Anatomic double-bundle and over-the-top single-bundle with additional extra-articular tenodesis: an in vivo quantitative assessment of knee laxity in two different ACL reconstructions. Knee Surg Sports Traumatol Arthrosc 20(1):153–159
Zens M, Ruhhammer J, Goldschmidtboeing F, Woias P, Feucht MJ, Mayr HO, Niemeyer P (2014) A new approach to determine ligament strain using polydimethylsiloxane strain gauges: exemplary measurements of the anterolateral ligament. J Biomech Eng 136(12):124504-1–124504-5
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Guenther, D., Griffith, C., Lesniak, B. et al. Anterolateral rotatory instability of the knee. Knee Surg Sports Traumatol Arthrosc 23, 2909–2917 (2015). https://doi.org/10.1007/s00167-015-3616-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-015-3616-6