
Abstract
Purpose
The aim of the present study was to clarify whether varus–valgus laxities under static stress in extension, femoral condylar lift-off during walking, and patient-reported outcomes after total knee arthroplasty (TKA) were correlated with each other.
Methods
Ninety-four knees, which had undergone posterior-stabilized TKA, were analysed. The varus–valgus laxity during knee extension was measured using a stress radiograph. New Knee Society Score (KSS) questionnaires were mailed to all patients. Correlations between the values of stress radiographs and KSS were analysed. Additionally, continuous radiological images were taken of 15 patients while each walked on a treadmill to determine condylar lift-off from the tibial tray using a 3D-to-2D image-to-model registration technique. Correlations between the amount of lift-off and either the stress radiograph or the KSS were also analyzed.
Results
The mean angle measured was 5.9 ± 2.7° with varus stress and 5.0 ± 1.6° with valgus stress. The difference between them was 0.9 ± 2.8°. Varus–valgus laxities, or the differences between them, did not show any statistically significant correlation with either component of the KSS (p > 0.05). The average amount of femoral condylar lift-off during walking was 1.4 ± 0.8 mm (medial side) and 1.3 ± 0.6 mm (lateral side). The amount of lift-off did not correlate with either varus–valgus laxities or the KSS (p > 0.05).
Conclusions
No correlations were found among varus–valgus laxities under static stress in extension, femoral condylar lift-off during walking, or patient-reported outcomes after well-aligned TKA. This study suggests that small variations in coronal laxities do not influence lift-off during walking and the patient-reported outcomes.
Level of evidence
IV.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is an effective surgical procedure for relieving pain and restoring function in patients with advanced knee osteoarthritis. However, a recent report investigating patient-reported outcomes after TKA indicated that patient satisfaction levels for TKA were lower than for total hip arthroplasty. Poor subjective outcomes may be attributed to preoperative patient characteristics such as age, body mass index, complications, and severity of arthritis [3, 17, 21]. Other possible reasons are imbalance of the replaced knee, malalignment of implants, and postoperative kinematics such as abnormal rotational pattern and femoral condylar lift-off [13, 14, 16, 24]. In particular, postoperative gap balancing affects the range of motion (ROM), function, and polyethylene wear [2, 25, 26]; thus, ligament balance could be associated with the subjective outcomes of patients. However, there are few reports about the relationship between coronal stability of replaced knees and patient-reported outcomes.
Femoral condylar lift-off occurs under weight-bearing conditions [4, 7, 8, 10, 18, 23]. Stiehl et al. [23] reported that 90 % of subjects had significant lift-off during the stance phase of walking. Jennings et al. [11] described lift-off as a cause of excessive stress on polyethylene inserts. However, the authors of the current study could not find a report describing whether abnormal movement, such as femoral condylar lift-off after TKA, affects patient-reported outcomes. Furthermore, although lift-off may be related to postoperative coronal stability, Hamai et al. [7] reported no relationship between the coronal stability and lift-off during activities following cruciate-retaining TKA. The relationship between coronal stability and lift-off should be replicated following posterior-stabilized (PS) TKA. However, the relationship between these three factors, namely coronal stability, condylar lift-off, and patient-reported outcomes, appears not to have been reported.
Based on existing reports, we therefore asked the following questions: (1) Does postoperative varus–valgus laxity under static stress affect patient-reported outcomes? and (2) Does condylar lift-off relate to the postoperative varus–valgus laxity and affect patient-reported outcomes? We hypothesized that coronal laxity correlates with both patient-reported outcomes and condylar lift-off during walking, and that lift-off affects patient-reported outcomes.
Materials and methods
Ninety-four knees in 68 patients, who underwent TKA and agreed to participate in the current study, were evaluated. Patients who visited our hospital from April 2011 to October 2012 for the purpose of scheduled postoperative follow-up and agreed with this study were enrolled to this study. They were originally underwent TKA by three experienced surgeons at a single centre from June 2000 to January 2012. The total number of primary TKA during the period was 874. Preoperative diagnoses included osteoarthritis in 60 patients and rheumatoid arthritis in eight patients. Patients with a history of prior arthroplasty, osteotomy, a severe extra-articular deformity with a more than 20° varus/valgus angle between the thigh and lower leg, or fractures around the knee were excluded. The average preoperative hip-knee-ankle (HKA) angle in a full-standing radiograph was 192.1 ± 6.1° (range 181–209°). All the patients received a PS fixed-bearing TKA (Nexgen LPS or LPS-Flex, Zimmer, Warsaw, IN). The number of LPS and LPS-Flex was 44 and 50, respectively. The KSS questionnaires were mailed to the patients. The follow-up period represented the time until the KSS questionnaires were completed. The mean (±standard deviation) follow-up period for the assessment of the new KSS was 4.6 ± 2.7 years (range 1.1–11.0 years). The postoperative ROM values were obtained when the stress radiograph was taken. The mean knee extension angle was −3.3 ± 5.6° (range −10–0°), and the flexion angle was 120 ± 8.6° (range 75–125°).
Surgical technique
The medial parapatellar approach was applied using a tourniquet. Using the measured-resection technique, the femoral and tibial components were aligned perpendicular to the mechanical axis in the coronal plane. The femoral component was positioned along the surgical epicondylar axis (SEA) in the axial plane. The rotational alignment of the tibial component was adjusted to the medial one-third of the tibial tuberosity. A computer navigation system was used for the bone preparation in 24 knees, and the conventional alignment rod was used in 70 knees. Ligament balancing was performed in 0° extension and 90° flexion by additional releases until the surgeon determined the balance was acceptable based on measurements performed using the spacer block and/or a tensor device to determine the angle and gap length between the cut surfaces. The first step included removal of any residual osteophytes at the posterior part of the medial femoral condyle and at the medial-to-posterior part of the tibia. This was coupled with the release of the deep medial collateral ligament (MCL). The second step included the release of the posteromedial capsule and the release of the superficial MCL. Additional releases were performed on the deep layer of the MCL in 22 knees, the deep and superficial layer of the MCL in 25 knees, the semimembranosus in 20 knees, and the posterior capsule in 66 knees. The patella was resurfaced in all cases.
Evaluation of the varus–valgus laxity
Anteroposterior radiographs were taken of the knee with varus and valgus stress in extension [7, 9, 10, 15, 20]. The laxity assessment was performed 4.1 ± 2.8 years after TKA. The time between the laxity assessment and KSS assessment was less than 3 months in all cases. The subjects were in a supine position on the table with their knee flexed at 10° to place the tibial plateau perpendicular to the film cassette. A varus and valgus stress of 150 N of was applied to the knee with a Telos device (Telos, Weiterstadt, Germany). The angle made by the tangential lines on the femoral condyles and tibial plateau was measured on film to assess the varus and valgus laxities. The intraclass correlation coefficient and the standard error (SE) for the three measurements conducted by the same examiner were 0.97 and 0.38, respectively, whereas the interclass correlation coefficient and SE for the same measurements made by three examiners were 0.91 and 0.34, respectively.
Evaluation of patient-reported outcomes
The new KSS questionnaire [16, 19, 22] was mailed to all patients. No patients were recalled specifically for this study; all data were obtained from medical records and the questionnaires. The scores of each component of the KSS were used to evaluate patient-reported outcomes including the following: “symptoms”, “patient satisfaction”, “patient expectations”, “walking and standing”, “standard activities”, and “advanced activities”. A total of 26 patients who underwent bilateral TKA were asked to provide separate KSS responses for each knee; however, 17 patients provided the same responses for both knees. Based on this finding, these patients were analyzed separately and defined as the “bilateral group”. The patient group that provided separate responses to for each knee was defined as the “unilateral group”. Patients who underwent a unilateral TKA were also included in the “unilateral group”. There were 60 knees belonging to 51 patients in the unilateral group and 34 knees belonging to 17 patients in the bilateral group. The study included 10 men and 58 women with a mean age of 72.5 years (range 50–86 years).
Kinematic analysis
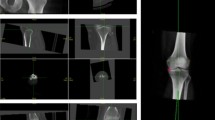
A total of 19 knees, from 15 out of 74 subjects (20 %) who were randomly selected, were assessed after a mean 2.3 ± 1.5 years (range 0.5–5.5 years) following surgery to evaluate the relationship between coronal laxity and patient-reported outcomes or knee kinematics. Of the 15 patients, 14 women and one man were analyzed. Five patients underwent bilateral TKA. Continuous dynamic sagittal radiological images of subjects walking on a level treadmill at 1.0 km/h were obtained for each patient using a flat-panel detector (Toshiba, Ultimax-I, Tochigi, Japan). This produced 10 frames per second using a digital X-ray system (1,024 × 1,024 × 12 bit/pixel, 7.5-Hz serial spot images as a DICOM file). Images of several steps were captured during the walking activity. Using a previously reported 3D-to-2D image-to-model registration technique, femoral condylar lift-off was evaluated [6, 7]. Accuracy of the relative motion between metal components was estimated to be 0.2° in rotation and 0.2 mm in translation. The minimum distances between the femoral condyles and the articular surfaces of the polyethylene insert were measured separately in the medial and lateral compartment, and the maximum difference in distance between the medial and lateral compartment for each subject was thus considered to demonstrate the amount of lift-off. Measurement error in the relative distance was 0.2 ± 0.1 mm, for which the 95 % confidence interval was 0.4 mm. Informed consent was provided by the subjects, and the Institutional Review Board of Kyushu University Hospital approved this study (ID: 24-166).
Statistical analysis
The relationship between postoperative varus and valgus laxities or differences in the laxities and the new KSS results or postoperative HKA angles were analyzed by dividing into a unilateral group and a bilateral group. Correlations between femoral condylar lift-off and the two laxities or differences in the laxities and the new KSS were estimated. Statistical analyses were performed using the Pearson correlation coefficient with JMP version 9.0 (SAS Institute Inc, Cary, NC, USA). Significance was set at a p value of <0.05.
Results
The subjects had an average angle of 5.9 ± 2.7° (range 1.0–12.7°) in varus stress and 5.0 ± 1.6° (range 1.5–9.0°) in valgus stress. The average difference in the laxities was 0.9 ± 2.8° (range −5.0–8.2°) (Table 1). The average postoperative HKA angle in a full-standing radiograph was 180.9 ± 3.7° (range 170–191°). Table 2 shows the mean and the range of each component of the new KSS and shows the p value and the correlation coefficient of the correlation between varus laxity, valgus laxity and the difference and the new KSS. Neither varus–valgus laxities nor the differences between varus and valgus laxities showed any statistically significant correlation with either component of the new KSS or postoperative HKA angles. The coronal laxities also did not correlate with the new KSS results or HKA angles when the patients were separately analyzed based on unilateral group or bilateral group (Table 2).
The average amount of femoral condylar lift-off was 1.4 ± 0.8 mm (0.1–3.0 mm) on the medial side and 1.3 ± 0.6 mm (0.4–2.4 mm) on the lateral side. Table 3 shows p values for the correlations between varus knees or valgus knees and lift-off. Neither varus–valgus laxities nor the differences between varus and valgus laxities showed any statistically significant correlation with lift-off. There was no statistically significant correlation between lift-off and either the total score or category component scores of the new KSS. There were no differences in coronal laxities and lift-off between LPS and LPS-Flex prostheses.
Discussion
The most important finding of the present study was that there was no relationship between knee laxity or imbalance in extension and the new KSS questionnaire scores used to evaluate patient-reported outcomes after PS TKA performed by the measured-resection technique. Furthermore, there was no relationship between static postoperative laxity, condylar lift-off during walking, or the new KSS.
There are some limitations associated with the present study. First, coronal stability was evaluated only in knee extension. It is deemed necessary to analyze coronal stability in mid-flexion because knee flexion angle during walking can approach approximately 50° [1]. Second, the study was limited by the small number of subjects with regard to kinematic analysis, and a power analysis was not performed for this study; hence, the results may not apply more generally in larger populations. Knees with a loss of stability could potentially demonstrate significant condylar lift-off. A wider variation in postoperative laxity and alignment might be needed to provide more robust results. Third, the time until kinematic analysis for one of the 19 knees assessed was short (0.5 years). Over a longer period of time, lift-off may cause polyethylene wear and affect patient-reported outcomes. However, even after excluding the knee followed-up after only 0.5 years, the lift-off of other knees followed-up after more than 1 year did not show a significant correlation with patient-reported outcomes in this study. Finally, the amount of lift-off includes a certain amount of potential measurement error. Using a possible <0.4 mm threshold before more confidently defining loss of contact on the unilateral compartment of the knee could include both false-negative and false-positive errors.
In the current study, laxity in varus stress was 5.9° and laxity in valgus stress was 5.0°. Draganich et al. [5] reported that in a 3D testing system, PS mobile-bearing prostheses had 4° and 3° of laxity in varus and valgus orientations, respectively. Ishii et al. [9] reported that the average values for knee abduction and adduction with PS prostheses were 4.6° and 4.0°, respectively. Although the mean laxities in the present study slightly exceeded results in the other studies, varus–valgus laxities, or the differences between varus and valgus laxities, did not affect patient-reported outcomes. Therefore, the additional remaining laxity or imbalance within this range may be acceptable from the viewpoint of patient-reported outcomes.
Femoral condylar lift-off did not correlate with the varus–valgus laxities, the differences between varus and valgus laxities, or patient-reported outcomes. The results of the present study do not support our hypothesis. Hamai et al. [7] reported that subjects had an average angle of 6.8° in varus stress, a 6.6° angle in valgus stress, and condylar lift-off values were less than 1.0 mm with cruciate-retaining (CR) prostheses. Their results also showed that that knee laxity did not correlate with femoral condylar lift-off. Dennis et al. [4] reported that condylar lift-off during walking in patients who underwent surgery performed via the measured-resection technique was significantly greater than for those on whom the gap-balancing technique was performed. Lift-off occurred in patients in the current study who underwent surgery with the measured-resection technique; however, lift-off did not correlate with varus–valgus laxities. Other possible causes of condylar lift-off include the abduction–adduction moment in flexion [12] and the rotational alignment of the femoral component [8]. The mean and maximum amount of condylar lift-off during a single-leg stance in the current study was smaller than that in previous studies [8, 23]. Results of this study suggest that the small amount of lift-off does not affect patient-reported outcomes. Moreover, the lack of correlation between the coronal stability or lift-off and patient-reported outcomes might be attributable to the neutral coronal alignment of the femoral and tibial components relative to the mechanical axis [16].
Conclusion
The current study was designed to determine whether there were any correlations among coronal laxities under static stress in extension, femoral condylar lift-off during walking, and patient-reported outcomes after PS TKA. The results of this study showed that small variations in coronal laxities in extension did not influence patient-reported outcomes or condylar lift-off during a single-leg stance, and the lift-off did not influence patient-reported outcomes.
References
Bejek Z, Paróczai R, Szendröi M, Kiss RM (2011) Gait analysis following TKA: comparison of conventional technique, computer-assisted navigation and minimally invasive technique combined with computer-assisted navigation. Knee Surg Sports Traumatol Arthrosc 19:285–291
Berend ME, Ritter MA, Meding JB, Faris PM, Keating EM, Redelman R, Faris GW, Davis KE (2004) Tibial component failure mechanisms in total knee arthroplasty. Clin Orthop Relat Res 428:26–34
Clement ND, Burnett R (2013) Patient satisfaction after total knee arthroplasty is affected by their general physical well-being. Knee Surg Sports Traumatol Arthrosc 21:2638–2646
Dennis DA, Komistek RD, Kim RH, Sharma A (2010) Gap balancing versus measured resection technique for total knee arthroplasty. Clin Orthop Relat Res 468:102–107
Draganich LF, Pottenger LA (2000) The TRAC PS mobile-bearing prosthesis: design rationale and in vivo 3-dimensional laxity. J Arthroplast 15:102–112
Hamai S, Miura H, Higaki H, Matsuda S, Shimoto T, Sasaki K, Yoshizumi M, Okazaki K, Tsukamoto N, Iwamoto Y (2008) Kinematic analysis of kneeling in cruciate-retaining and posterior-stabilized total knee arthroplasties. J Orthop Res 26:435–442
Hamai S, Miura H, Okazaki K, Shimoto T, Higaki H, Iwamoto Y (2013) No influence of coronal laxity and alignment on lift-off after well-balanced and aligned total knee arthroplasty. Knee Surg Sports Traumatol Arthrosc. doi:10.1007/s00167-013-2500-5
Insall JN, Scuderi GR, Komistek RD, Math K, Dennis DA, Anderson DT (2002) Correlation between condylar lift-off and femoral component alignment. Clin Orthop Relate Res 403:143–152
Ishii Y, Matsuda Y, Ishii R, Sakata S, Omori G (2003) Coronal laxity in extension in vivo after total knee arthroplasty. J Orthop Sci 8:538–542
Ishii Y, Noguchi H, Matsuda Y, Takeda M, Walker SA, Komistek RD (2007) Effect of knee laxity on in vivo kinematics of meniscal-bearing knee prostheses. Knee 14:269–274
Jennings LM, Bell CI, Ingham E, Komistek RD, Stone MH, Fisher J (2007) The influence of femoral condylar lift-off on the wear of artificial knee joints. Proc Inst Mech Eng H 221:305–314
Kanekasu K, Banks SA, Honjo S, Nakata O, Kato H (2004) Fluoroscopic analysis of knee arthroplasty kinematics during deep flexion kneeling. J Arthroplasty 19:998–1003
Kawahara S, Okazaki K, Matsuda S, Nakahara H, Okamoto S, Iwamoto Y (2013) Internal rotation of femoral component affects functional activities after TKA-survey with the 2011 Knee Society Score. J Arthroplast. doi:10.1016/S0883-5403(13)00862-0
Kuster MS, Bitschnau B, Votruba T (2004) Influence of collateral ligament laxity on patient satisfaction after total knee arthroplasty: a comparative bilateral study. Arch Orthop Trauma Surg 124:415–417
Matsuda Y, Ishii Y (2004) In vivo laxity of low contact stress mobile-bearing prostheses. Clin Orthop Relat Res 419:138–143
Matsuda S, Kawahara S, Okazaki K, Tashiro Y, Iwamoto Y (2013) Postoperative alignment and ROM affect patient satisfaction after TKA. Clin Orthop Relat Res 471:127–133
Merle-Vincent F, Couris CM, Schott AM, Conrozier T, Piperno M, Mathieu P, Vignon E (2011) Factors predicting patient satisfaction 2 years after total knee arthroplasty for osteoarthritis. Joint Bone Spine 78:383–386
Moynihan AL, Varadarajan KM, Hanson GR, Park SE, Nha KW, Suggs JF, Johnson T, Li G (2010) In vivo knee kinematics during high flexion after a posterior-substituting total knee arthroplasty. Int Orthop 34:497–503
Noble PC, Scuderi GR, Brekke AC, Sikorskii A, Benjamin JB, Lonner JH, Chadha P, Daylamani DA, Scott WN, Bourne RB (2012) Development of a new Knee Society scoring system. Clin Orthop Relat Res 470:20–32
Okazaki K, Miura H, Matsuda S, Takeuchi N, Mawatari T, Hashizume M, Iwamoto Y (2006) Asymmetry of mediolateral laxity of the normal knee. J Orthop Sci 11:264–266
Schnurr C, Jarrous M, Güdden I, Eysel P, König DP (2013) Pre-operative arthritis severity as a predictor for total knee arthroplasty patients’ satisfaction. Int Orthop 37:1257–1261
Scuderi GR, Bourne RB, Noble PC, Benjamin JB, Lonner JH, Scott WN (2012) The new Knee Society knee scoring system. Clin Orthop Relat Res 470:3–19
Stiehl JB, Dennis DA, Komistek RD, Crane HS (1999) In vivo determination of condylar lift-off and screw-home in a mobile-bearing total knee arthroplasty. J Arthroplast 14:293–299
Turcot K, Sagawa Y Jr, Fritschy D, Hoffmeyer P, Suvà D, Armand S (2013) How gait and clinical outcomes contribute to patients’ satisfaction three months following a total knee arthroplasty. J Arthroplast 28:1297–1300
Van Hal CT, van Hellemondt GG, Wymenga AB, Jacobs WC (2007) The anterior-posterior laxity after total knee arthroplasty inserted with a ligament tensor. Knee Surg Sports Traumatol Arthrosc 15:1019–1022
Warren PJ, Olanlokun TK, Cobb AG, Walker PS, Iverson BF (1994) Laxity and function in knee replacements. A comparative study of three prosthetic designs. Clin Orthop Relat Res 305:200–208
Acknowledgments
This work was supported by institutional funding from the Grant-in-Aid for Specially Promoted Research of Japan Society for the Promotion of Science (23000011).
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Nakahara, H., Okazaki, K., Hamai, S. et al. Does knee stability in the coronal plane in extension affect function and outcome after total knee arthroplasty?. Knee Surg Sports Traumatol Arthrosc 23, 1693–1698 (2015). https://doi.org/10.1007/s00167-014-3122-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-014-3122-2