
Abstract
Multiple differing surgical techniques are currently utilized to perform total knee arthroplasty (TKA). We compared knee arthroplasties performed using either a measured resection or gap balancing technique to determine if either operative technique provides superior coronal plane stability as measured by assessment of the incidence and magnitude of femoral condylar lift-off. We performed 40 TKA using a measured resection technique (20 PCL-retaining and 20 PCL-substituting) and 20 PCL-substituting TKA were implanted using gap balancing. All subjects were analyzed fluoroscopically while performing a deep knee bend. The incidence of coronal instability (femoral condylar lift-off) was then determined using a 3-D model fitting technique. The incidence of lift-off greater than 0.75 mm was 80% (maximum, 2.9 mm) and 70% (maximum, 2.5 mm) for the PCL-retaining and substituting TKA groups performed using measured resection versus 35% (maximum, 0.88 mm) for the gap-balanced group. Lift-off greater than 1 mm occurred in 60% and 45% of the PCL-retaining and -substituting TKA using measured resection versus none in the gap-balanced group. Rotation of the femoral component using a gap balancing technique resulted in better coronal stability which we suggest will improve functional performance and reduce polyethylene wear.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Stability of total knee arthroplasty is dependent on correct and precise rotation of the femoral component. Femoral component malrotation has been associated with numerous adverse sequelae, including patellofemoral and tibiofemoral instability, knee pain, arthrofibrosis, and abnormal knee kinematics [1, 3, 4, 12, 21, 23]. Controversy exists, however, regarding the most favorable method to determine accurate femoral component rotation. Some favor a measured resection technique in which bony landmarks (femoral epicondyles, posterior femoral condyles, or the anteroposterior axis) are the primary determinants of femoral component rotation [2, 10, 18, 20, 22, 24]. Others recommend a gap-balancing methodology in which the femoral component is positioned parallel to the resected proximal tibia with each collateral ligament equally tensioned [5, 9, 15].
We therefore asked whether a measured resection or gap balancing technique would result in (1) a higher incidence of coronal plane instability, as measured by the presence of femoral condylar lift-off greater than both 0.75 mm and 1.0 mm, was higher using; (2) a greater mean maximum lift-off; (3) a greater maximum lift-off; and (4) a differing lift-off location.
Patients and Methods
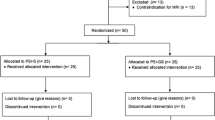
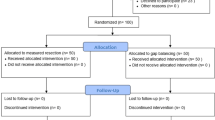
We analyzed 60 selected patients who had TKA performed using one of two operative techniques. Only TKAs judged clinically successful (Hospital for Special Surgery Knee scores [13] > 90 points), with no substantial ligamentous laxity or pain were included. Ligamentous assessment was performed manually by the operating surgeon. Additional selection criteria included a preoperative diagnosis of osteoarthritis, a minimum of six months of postoperative followup duration to assure complete recovery before analysis, preoperative deformity of less than 15 degrees, and patient willingness to participate in the testing protocol. Patient selection was nonsequential and nonrandomized. All procedures were performed from 2003 to 2006. Forty were performed using a measured resection technique in which a combination of bony landmarks (femoral epicondyles, posterior condylar axis, and anterior-posterior axis) was used to determine proper rotation of the femoral component (Fig. 1); of those 40, 20 had a PCL-retaining (PCR) TKA and 20 received a PCL-substituting (PS) TKA design. The remaining 20 patients received a PS TKA implanted using a gap-balancing technique in which the extension gap was initially established by resection of the distal femoral and proximal tibial articular surfaces. A spacer block was then inserted into the extension gap and alignment and soft tissue balance were assessed. If either of these factors was deemed to be suboptimal, additional soft tissue ligamentous balancing was performed to obtain a balanced extension gap and satisfactory alignment along the mechanical axis. Thereafter, the femoral component was positioned parallel to the resected proximal tibia with each collateral ligament tensioned as equally as possible with two laminar spreaders. The patella was subluxated and not everted in an attempt to lessen extensor mechanism tension and distortion of the true dimensions of the flexion gap (Fig. 2). The preoperative femorotibial alignment of all three study groups was similar. Preoperative varus femorotibial alignment predominated in each study cohort (Table 1). All TKA implants were from the same implant design system (PFC Sigma; DePuy Orthopaedics, Inc; Warsaw, IN). All patients were evaluated clinically and fluoroscopically at a minimum of 6 months (range, 6–24 months) following their operative procedure and were considered fully recovered before analysis. IRB approval was received for this study from each center of investigation and informed consent was obtained from every patient participating in this study.

Femoral component rotation was determined using a measured resection technique.

A femoral component is positioned using a gap-balancing technique. (Reprinted with permission from SLACK, Inc. from Dennis DA. Measured resection: an outdated technique in total knee arthroplasty. Orthopedics. 2008;31:940, 943–944.)
Each patient was asked to perform a deep knee bend from full extension to maximum knee flexion while under fluoroscopic surveillance. Fluoroscopic images were captured and then downloaded to a workstation computer for analysis. Three-dimensional kinematics for each knee were recovered from the 2-D fluoroscopic images using a previously described automated model-fitting technique that determined the in vivo orientation of the femoral component relative to the tibial component [7, 11]. Error analyses of this 3-D model-fitting technique have shown a 3-D error of less than 0.5 mm in translation, less than 0.5° in rotation, and less than 0.75 mm in determining femoral condylar lift-off [17]. Fluoroscopic images initially were analyzed to determine the three dimensional position of the femoral and tibial components at full extension, and then at 30° increments of knee flexion to maximum flexion. The mean maximum weight-bearing flexion among the three TKA patient cohorts was similar when tested in a passive, nonweight-bearing fashion (PCR measured resection 127°; PS measured resection 123°; PS gap balancing 127°). Assessment of weight-bearing flexion during testing revealed 110° and 118° in the PCR and PS measured resection groups respectively versus 124° in the PS gap balancing cohort.
After the model fitting process was completed, coronal plane instability was assessed by rotating the images to a frontal view to assess for coronal instability as measured by the presence of femoral condylar lift-off. This was determined by performing digital measurements of the distances from the medial and lateral femoral condyles to the tibial tray [8] (Fig. 3). The incidence of femoral condylar lift-off greater than both 0.75 mm and 1 mm which occurred at any of the flexion values analyzed (full extension, 30°, 60°, 90°, and maximum flexion) in each subgroup was then determined and statistically compared. Lastly, the mean maximum and maximum magnitude of femoral condylar lift-off at any flexion increment was recorded and compared.

Frontal plane analysis of a 3-D model was used to determine the presence of femoral condylar lift-off.
We determined the differences in the incidence of femoral lift-off greater than 0.75 mm and 1.0 mm between the gap balancing and measured resection techniques using Fisher’s exact test. For this analysis 2 × 2 contingency tables were created comparing the gap balancing cohort versus the PCR measured resection cohort, the gap balancing versus the PS measured resection cohort and PCR measured resection versus the PS measured resection cohorts. For comparison of mean of the maximum lift-off values, the groups were analyzed for normality using the Shapiro-Wilks test which yielded probability values of 0.0637, 0.7084 and 0.2032 for PCR measured resection, PS measured resection, and gap balancing groups respectively. Therefore a comparison was first performed using the nonparametric Kruskal-Wallis test. Since the Kruskal-Wallis test yielded a low probability value, comparisons of all pairs using the Tukey-Kramer HSD was performed to analyze which groups had differing mean values. All statistical tests were carried out in the commercially available JMP® Statistical DiscoveryTM Software (SAS Institute Inc, Cary, NC).
Results
The incidence of coronal instability (femoral condylar lift-off) greater than 0.75 mm occurring at any flexion interval analyzed (0°, 30°, 60°, 90°, and maximum flexion) was lower (p = 0.003) in the gap balancing group (7 of 20) than in either group performed using measured resection; coronal instability greater than 0.75 mm occurred 16 of 20 and 14 of 20 of the PCR and in PS TKA groups respectively performed using a measured resection technique (Table 2). Femoral condylar lift-off greater than 1 mm occurred more frequently (p < 0.0001) in the measured resection than the than in gap balancing TKA subjects who exhibited no femoral condylar lift-off greater than 1 mm: lift-off greater than 1 mm was seen in 14 of 20 and 11 of 20 of the PCR and PS TKA groups respectively performed using a measured resection technique.
The mean maximum femoral condylar lift-off values for the PCR and PS TKA groups performed using a measured resection technique were 1.45 mm (SD = 0.74) and 1.11 mm (SD = 0.60), respectively, which were both greater (p = 0.0003) than the mean maximum femoral condylar lift-off value of 0.67 mm (SD = 0.16) for those implanted using gap balancing. We observed no differences when comparing mean maximum femoral condylar lift-off values of the PCR and PS TKA groups in which a measured resection technique was chosen.
The maximum magnitude of femoral condylar lift-off observed at any flexion increment was also less (p = 0.0002) in the TKA group implanted using gap balancing (0.9 mm) than with either the PCR (3.1 mm) or PS TKA (2.5 mm) groups in which measured resection was used. We observed no differences in maximum femoral condylar lift-off values of the two measured resection groups.
The lift-off location (medial or lateral) was highly variable in all three cohorts with some knee arthroplasties lifting off laterally, some medially, and others exhibiting lift-off both medially and laterally depending on the flexion interval evaluated. There were no major differences noted in location of lift-off among the three groups. We observed no statistical correlation in any of the groups when comparing preoperative alignment versus the location, incidence, or magnitude of lift-off although the numbers of subjects analyzed may be inadequate to determine statistical differences in these parameters.
Discussion
Obtaining satisfactory stability in the coronal plane is critical for the long-term success of TKA and requires precise rotational alignment of the femoral component. Malrotation of the femoral component has been associated with numerous undesirable conditions including patellofemoral and tibiofemoral instability, arthrofibrosis, knee pain, and disturbed knee kinematics [1, 3, 4, 11, 19, 21]. The best method to determine correct femoral component rotation and subsequent coronal plane stability is debated. Many utilize a measured resection technique [2, 10, 18, 20, 24] in which bony landmarks (femoral epicondyles, anterior-posterior axis, posterior condylar axis) are used alone or in combination to determine femoral component rotation. Advocates of this technique recommend placement of the femoral component either parallel to the transepicondylar axis [2, 10, 20], perpendicular to the anteroposterior axis [24], or approximately 3° to 4º externally rotated relative to posterior condylar axis [19]. Others prefer using a gap-balancing methodology in which the femoral component is positioned parallel to the resected proximal tibia with equal collateral ligamentous tension [5, 9, 15]. We therefore asked whether a measured resection or gap balancing technique would result in (1) a higher incidence of coronal plane instability, as measured by the presence of femoral condylar lift-off greater than both 0.75 mm and 1.0 mm; (2) a greater mean maximum lift-off; (3) a greater maximum lift-off; and (4) a differing lift-off location (medial versus lateral).
The first limitation of this study is that selected patients were not consecutive or randomized and only those with high clinical and functional knee scores were analyzed. This methodology was chosen to assure that only subjects judged clinically excellent were analyzed and therefore limit variables such as pain, stiffness, or instability which might impair a patient’s ability to perform a deep knee bend maneuver. It is unknown if similar results would be obtained if subjects with inferior clinical results were analyzed. A second limitation is the authors’ inability to state, with 100% certainty, that all of the kinematic findings observed in this analysis are only limited to variations in surgical technique. Previous kinematic analyses performed in our laboratory have documented substantial kinematic variances are common following TKA [6–8, 23]. Multiple factors influence kinematics including technique type and quality, implant design, and variances in the individuals tested (motion, stability, alignment, etc.). All of these factors have likely played a role in the kinematic variability we have observed in previous studies. The authors have tried to control as many variables as possible by having only one experienced surgeon perform all of the operative procedures, selecting only patients who were considered clinically excellent (knee scores > 90 points), and by using a single implant design system in which the three different implants analyzed had similar prosthetic dimensions. Third, some observers may question whether the presence of femoral condylar lift-off will have adverse effects on the clinical results of TKA. We believe lift-off will prove to be a major factor in the long term polyethylene wear of TKA. This is supported by the work of Jennings et al. [14], who studied the effect of femoral condylar lift-off on wear of ultra high molecular weight polyethylene of both fixed bearing and rotating platform TKA using a physiologic knee simulator. In the absence of lift-off, the rotating platform knees exhibited a lower wear rate of 5.2 ± 2.2 mm3 per million cycles (mm3/MC) compared with 8.8 ± 4.8 mm3/MC for the fixed bearing knees. The presence of femoral condylar lift-off substantially accelerated (greater than two fold) the wear of the fixed bearing and rotating platform knees tested to 16.4 ± 2.9 and 16.9 ± 2.9 mm3/MC, respectively [14]. Fourth, the findings pertain to the patients selected, the specific implants utilized and the technique and skill of the operating surgeon and may not be reflective of results that might be obtained in a similar analysis with a different patient population, implant design or operating surgeon. Finally, a combination technique, using gap balancing in conjunction with the bony landmarks used in a measured resection approach, was not evaluated. Use of a combination of these two techniques was not utilized so that each technique could be individually analyzed. The senior surgeon currently selects gap balancing as the primary determinant of femoral rotation and uses the transepicondylar and anteroposterior axes as secondary assessment factors.
Our analysis demonstrated less coronal plane instability (incidence and magnitude) in subjects who received a TKA using gap balancing. The authors hypothesize these findings are related to surgeon inability to precisely identify critical bony landmarks when deciding correct femoral component rotation using a measured resection methodology. Numerous reports support this hypothesis. Kinzel et al. [16] reported on a series of 74 TKA in which the femoral epicondyles were marked with pins intraoperatively and postoperative CT scans performed to assess the accuracy of epicondylar identification. They observed that the epicondyles were correctly identified to within ± 3° in only 75% of the cases with a wide range of error (6° of external rotation to 11° of internal rotational error). Yau et al. [25] performed an additional analysis and similarly found a wide range of error in intraoperative surgeon identification of the femoral epicondyles (28° error range; 11° external rotation to 17° of internal rotation). In this same report [25], a 32° range of error with use of the anteroposterior axis was observed (15° external rotation to 17° of internal rotation) while Nagamine et al. [19] reported substantial external rotation error with use of the anteroposterior axis in varus knees with medial compartment osteoarthritis.
The problem with use of the posterior condylar axis as a measured resection reference to determine proper femoral component rotation is twofold. First, selection of 3° to 4º of femoral component external rotation relative to this axis is based on mean data and investigations demonstrate wide anatomic variations in the relationship of the posterior condylar axis to the transepicondylar axis (1–10°) [18, 20]. Therefore, if a patient’s anatomical relationship of the posterior condylar axis is 7º of external rotation versus the transepicondylar axis and instrumentation is used which places the femoral component in 3º of external rotation, the femoral component will actually be internally rotated 4º relative to the transepicondylar axis. Second, hypoplasia or erosion of the posterior aspect of the lateral femoral condyle in knees with valgus deformity (and also the posterior aspect of the medial femoral condyle in varus knees with chronic insufficiency of the anterior cruciate ligament) will lead to erroneous femoral component position if the posterior condylar axis is used as the primary determinant of femoral component rotation. This is supported by the analysis of Schnurr et al. [22] who assessed flexion gap stability in a series of 100 TKA implanted using computer navigation and observed a rectangular flexion gap would have been obtained in only 51% of cases if the posterior condylar axis had been utilized to determine femoral component rotation.
Similar findings to the current analysis were reported by Fehring [9] who found superior stability and femoral component rotational alignment was obtained when gap balancing was utilized to perform TKA. He compared flexion gap balance in 100 TKAs using gap balancing versus a measured resection technique and found rotational errors of at least 3° occurred in 45% of patients when rotation was determined using fixed bony landmarks.
Use of gap balancing is not without potential errors. It is dependent on the surgeon’s ability to make an accurate proximal tibial resection. Should this technique be used and a varus tibial cut is made, placement of the femoral component parallel to the resected tibia will result in internal rotation of the femoral component. Conversely, if a valgus error is made during proximal tibial resection, excessive external rotation of the femoral component will result. The gap balancing method is also dependent on integrity of the collateral ligaments. Particularly if the superficial medial tibial ligament is deficient, tensioning of the medial flexion gap will result in excessive medial flexion gap width and excessive internal rotation of the femoral component if the component is placed parallel to the resected tibia. Similarly, excessive femoral component external rotation will occur if the lateral collateral ligament-popliteus tendon complex is deficient. Because of these factors, the authors recommend secondary use of bony landmarks to ensure the chosen rotational position of the femoral component using gap balancing is not widely divergent from the position that would be selected if bony landmarks (measured resection) were used.
This study emphasizes that coronal plane stability and precision of femoral component rotation can be affected by the type of surgical technique utilized. The findings of this report support use of a gap balancing method to obtain optimal coronal stability.
References
Berger RA, Crossett LS, Jacobs JJ, Rubash HE. Malrotation causing patellofemoral complications after total knee arthroplasty. Clin Orthop Relat Res. 1998;356:144–153.
Berger RA, Rubash HE, Seel MJ, Thompson WH, Crossett LS. Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis. Clin Orthop Relat Res. 1993;286:40–47.
Boldt JG, Stiehl JB, Hodler J, Zanetti M, Munzinger U. Femoral component rotation and arthrofibrosis following mobile-bearing total knee arthroplasty. Int Orthop. 2006;30:420–425. Epub 2006 Mar 7.
Crossett LS. Fixed- versus mobile-bearing total knee arthroplasty: technical issues and surgical tips. Orthopedics. 2002;25(2 Suppl):s251–s256.
Dennis, DA. Measured resection: An outdated technique in total knee arthroplasty. Orthopedics. 2008;31:940, 943–944.
Dennis DA, Komistek RD, Colwell CE Jr. Ranawat CS, Scott RD, Thornhill TS, Lapp MA. In vivo anteroposterior femorotibial translation of total knee arthroplasty: a multicenter analysis. Clin Orthop Relat Res. 1998;356:47–57.
Dennis DA, Komistek RD, Mahfouz MR. In vivo fluoroscopic analysis of fixed-bearing total knee replacements. Clin Orthop Relat Res. 2003;410:114–130.
Dennis DA, Komistek RD, Walker SA, Cheal EJ, Stiehl JB. Femoral condylar lift-off in vivo total knee arthroplasty. J Bone Joint Surg Br. 2001;83:33–39.
Fehring TK. Rotational malalignment of the femoral component in total knee arthroplasty. Clin Orthop Relat Res. 2000;380:72–79.
Griffin FM, Math K, Scuderi GR, Insall JN, Poilvache PL. Anatomy of the epicondyles of the distal femur: MRI analysis of normal knees. J Arthroplasty. 2000;15:354–359.
Hoff WA, Komistek RD, Dennis DA, Gabriel SM, Walker SM. A three-dimensional determination of femorotibial contact positions under in vivo conditions using fluoroscopy. Clin Biomech. 1998;13:455–472.
Incavo SJ, Wild JJ, Coughlin KM, Beynnon BD. Early revision for component malrotation in total knee arthroplasty. Clin Orthop Relat Res. 2007;458:131–136.
Insall JN, Hood RW, Flawn LB, Sullivan DJ. Total condylar knee prosthesis in gonarthrosis. A five to nine-year follow-up of the first one hundred consecutive replacements. J Bone Joint Surg. 1983;65:619–628.
Jennings LM, Bell CI, Ingham E, Komistek RD, Stone MH, Fisher J. The influence of femoral condylar lift-off on the wear of artificial knee joints. Proc Inst Mech Eng [H]. 2007;221:305–314.
Katz MA, Beck TD, Silber JS, Seldes RM, Lotke PA. Determining femoral rotational alignment in total knee arthroplasty: reliability of techniques. J Arthroplasty. 2001;16:301–305.
Kinzel V, Ledger M, Shakespeare D. Can the epicondylar axis be defined accurately in total knee arthroplasty. Knee. 2005;12:293–296.
Mahfouz MR, Hoff WA, Komistek RD, Dennis DA. A robust method for registration of three-dimensional knee implant models to two-dimensional fluoroscopy images. IEEE Trans Med Imaging. 2003;22;1561–1574.
Mantas JP, Bloebaum RD, Skedros JG, Hofmann AA. Implications of reference axes used for rotational alignment of the femoral component in primary and revision knee arthroplasty. J Arthroplasty. 1992;7:531–535.
Nagamine R, Miura H, Inoue Y, Urabe K, Matsuda S, Okamoto Y, Nishizawa M, Iwamoto Y. Reliability of the anteroposterior axis and the posterior condylar axis for determining rotational alignment of the femoral component in total knee arthroplasty. J Orthop Sci. 1998;3:194–198.
Poilvache PL, Insall JN, Scuderi GR, Font-Rodriguez DE. Rotational landmarks and sizing of the distal femur in total knee arthroplasty. Clin Orthop Relat Res. 1996;331:35–46.
Romero J, Stähelin T, Binkert C, Pfirrmann C, Hodler J, Kessler O. The clinical consequences of flexion gap asymmetry in total knee arthroplasty. J Arthroplasty. 2007;22:235–240.
Schnurr C, Nessler J, König DP. Is referencing the posterior condyles sufficient to achieve a rectangular flexion gap in total knee arthroplasty? Int Orthop. 2008 Oct 28. [Epub ahead of print].
Scuderi GR, Komistek RD, Dennis DA, Insall JN. The impact of femoral component rotational alignment on condylar lift-off. Clin Orthop Relat Res. 2003;410:148–154.
Whiteside LA, Arima J. The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty. Clin Orthop Relat Res. 1995;321:168–172.
Yau WP, Chiu KY, Tang WM. How precise is the determination of rotational alignment of the femoral prosthesis in total knee arthroplasty: an in vivo study. J Arthroplasty. 2007;22:1042–1048.
Acknowledgments
We thank Kendall Slutzky for her assistance in manuscript preparation and numerous engineering students at the Center for Musculoskeletal Research (University of Tennessee) for their assistance in patient fluoroscopy testing and three dimensional kinematic analysis.
Author information
Authors and Affiliations
Corresponding author
Additional information
An institution of the authors (Center for Musculoskeletal Research) and one author (DAD) have received funding from DePuy, Inc. (Warsaw, IN).
Each author certifies that his or her institution has approved the reporting of these cases, that all investigations were conducted in conformity with ethical principles of research, and that informed consent for participation in the study was obtained.
This work was performed at Center for Musculoskeletal Research, University of Tennessee, Knoxville, TN and the Rocky Mountain Musculoskeletal Research Laboratory, Denver, CO.
About this article
Cite this article
Dennis, D.A., Komistek, R.D., Kim, R.H. et al. Gap Balancing versus Measured Resection Technique for Total Knee Arthroplasty. Clin Orthop Relat Res 468, 102–107 (2010). https://doi.org/10.1007/s11999-009-1112-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11999-009-1112-3