
Abstract
Purpose
To compare the clinical and radiographic results of fixed-bearing and mobile-bearing total knee arthroplasty (TKA).
Methods
We searched the PubMed, Medline, Embase, Cochrane Central Register of Controlled Trials, and Google Scholar databases from 1966 to January 2012. No language restriction was applied. Reference lists of all the selected articles were hand-searched for any additional trials. Trial quality was assessed using the modified Jadad scale. Two authors independently extracted data from all eligible studies, including study design, participants, interventions, and outcomes (Knee Society Score, range of movement, radiolucent line, patient preference, walking support, pain score, and complications). The data were using fixed-effects or random-effects models with mean differences and risk ratios for continuous and dichotomous variables, respectively.
Results
A total of 24 studies involving 2,799 patients were identified in this analysis. Meta-analysis showed lower pain score (OR, 0.66, 95 % CI 0.46, 0.94) in mobile-bearing TKA than fixed-bearing TKA. There was no significant difference between the two treatment groups regarding Knee Society Score (SMD, −0.17, 95 % CI: −0.60, 0.26), range of movement (SMD, −0.05, 95 % CI: −0.63, 0.53), radiolucent line (OR, 1.03, 95 % CI 0.74, 1.44), patient preference (OR, 1.15, 95 % CI 0.82, 1.61), walking support (OR, 1.07, 95 % CI 0.68, 1.70), and complications (OR, 0.85, 95 % CI 0.59, 1.21).
Conclusions
The available evidence suggested that there was no significant difference between clinical and radiographic results of fixed-bearing and mobile-bearing TKA except for pain score. Regarding clinical relevance, the less incidence of pain could be the advantage for selecting mobile-bearing TKA.
Level of evidence
II.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
Total knee arthroplasty (TKA) is the most effective treatment for relieving pain and restoring function to the older patients with end-stage osteoarthritis (OA) and other destructive knee problems. Currently, based on the different fundamental design principles, total knee prosthesis devices can be divided into two types: fixed-bearing knees and mobile-bearing knees [23]. Since the introduction of mobile-bearing polyethylenes into TKA, they have attracted considerable attention because they offer possible solutions to the limitations of fixed-bearing designs in TKA. When compared with fixed-bearing prostheses, the mobile-bearing prosthesis was introduced to minimize interface stresses between the implant and the bone [2]. One commonly stated reason for using a mobile-bearing TKA was that it improves the range of motion, and it reduces wear of the tibial polyethylene bearing [6, 26]. Dislocations of the bearing and higher implant costs have been considered disadvantageous [9]. Although the mobile-bearing total knee prosthesis has shown many of the theoretical advantages, controversy still exists regarding which total knee design is superior in the long-term clinical and radiographic results in TKA patient.
Recently, two systematic reviews [27, 30] (of randomized controlled trials) that compared the clinical results of fixed-bearing and mobile-bearing TKA found that no statistically significant difference was present in terms of Knee Society Score, radiolucent line, patient preference, and complications as compared to the fixed- and mobile-bearing knee design at mid-term follow-up, but their reviews only included 15 studies at most. Seven randomized controlled trials that compared the clinical results of fixed-bearing and mobile-bearing TKA had recently been completed [14–16, 21, 22, 32, 35]. The results of these studies are controversial and not in accordance with previous systematic reviews. In order to provide the best available evidence to compare the clinical results of fixed-bearing and mobile-bearing TKA on Knee Society Score, range of movement, radiolucent line, patient preference, walking support, pain score, and complications, we carried out a systematic review of randomised controlled trials updating meta-analysis of clinical studies.
Materials and methods
Criteria for considering studies for this review
Studies included
Prospective, randomized controlled trials were included.
Types of participants
The study population included adults who underwent total knee arthroplasty (TKA).
Types of interventions
All patients underwent a mobile-bearing total knee arthroplasty or a fixed-bearing total knee arthroplasty. And, only the appropriate comparisons between mobile-bearing versus fixed-bearing prosthesis were selected.
Types of outcome measures
Outcome measures included Knee Society Score (KSS), Western Ontario McMasters University (WOMAC), Pain score, Function score, Range of movement (ROM), and Radiolucent line. Other outcomes such as complications, walking support, walking distance, and patient preference also were considered.
Search strategy for identification of studies
All relevant RCTs meeting the inclusion criteria were identified by the following:
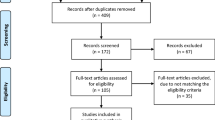
The PubMed, Embase, Cochrane Central Register of Controlled Trials, and Google Scholar databases were searched. Two authors independently searched for relevant studies in any language from 1966 to January 2012. The search strategy was created with the assistance of a librarian using a combination of terms including TKA; knee prosthesis; joint replacement; mobile-bearing; fixed-bearing; meniscal bearing; gliding bearing; rotating platform; randomized controlled trials (RCT); meta-analysis; and systematic review. We limited searches to RCT, systematic reviews, and meta-analyses and imposed no language or other limitations. The electronic search was complemented by the following hand searching reference lists. Figure 1 gives details of the search strategy.

Keywords and boolean (logical) operators used in the database searches
Selection of studies
Two reviewers (Li and Wu) independently screened the titles and abstracts of studies identified by the search strategy and discarded clearly irrelevant studies. The same two reviewers also independently applied the selection criteria to the studies retrieved by the literature search. They discussed to resolve any disagreement; if any uncertainty remained, they consulted further reviewer and expert (Feng) to decide.
Data extraction and management
Two reviewers independently extracted the data using a standardized form regarding inclusion criteria (study design, participants, interventions, and outcomes). A consensus method was used to resolve disagreements, and a third reviewer was consulted if disagreements persisted.
Methodological Quality of Included Studies
Two reviewers assessed the quality of the studies independently; revised Jadad scale was used to perform the quality assessment. This scale includes the random sequence production (2 points), allocation concealment (2 points), appropriateness of blinding (2 points), and description of dropouts and withdrawals (1 point). The total score is 7 points; 0–3 points mean poor quality, and 4–7 points mean high quality. And, Consolidated Standards on Reporting Trials (CONSORT) checklist and scoring system was used to evaluate the quality of included trials: scores of 18–22 are considered excellent study quality; 13–17, good; 8–12, fair; and less than 7, poor.
Statistical analysis
For dichotomous variables, we derived the relative risks and 95 % confidence intervals for each outcome. For continuous variables, we calculated the mean differences and 95 % confidence intervals for each outcome. We performed the meta-analysis using a fixed-effect model if no significant heterogeneity was present. To assess heterogeneity between studies, we performed a chi-square test and estimated the I 2 statistic. A random-effects model was selected to account for heterogeneity in the design and patient selection among included studies. And, the subgroup analyses were conducted for different outcomes.
Results
Search results
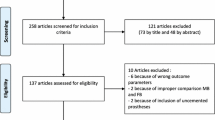
A search of the PubMed, Embase, Cochrane Central Register of Controlled Trials, and Google Scholar databases retrieved 997 articles. We excluded 279 duplicate articles after we reviewed the titles and abstracts. Then, by reading the whole paper, we included 24 papers. These studies included a total population of 2,799 participants. Fixed-bearing total knee prosthesis was implanted in 1,638 knees, and mobile-bearing total knee prosthesis was implanted in 1,659 knees. Figure 2 summarizes the study selection process.

Flowchart of trials selection process
Included studies
Twenty-two studies were published in English [1–3, 7, 10–20, 22, 25, 29, 31–34], and two studies [21, 35] were published in Chinese. All studies reported mean follow-up more than 12 months after randomization, and all studies presented appropriate comparisons between fixed-bearing TKA versus mobile-bearing total knee arthroplasty.
Characteristics of the 24 studies were described in Table 1. All the studies were RCT. Of the 24 trials, 20 studies reported the Knee Society Score; 15 studies reported range of movement; 7 studies reported pain score; 11 studies reported radiolucent line; 12 studies reported complications; 5 studies reported WOMAC; 5 studies reported patient preference; 5 studies reported percentage of walking support; and 8 studies reported function score.
Methodological quality
Of all the 24 trials, 4 studies were level I evidence; 20 studies were level II evidence (Table 1). For the revised Jadad scale, no studies were 1–3 points with a poor quality; all studies were 4–7 points with a high quality. Twenty-four RCTs were evaluated by Consolidated Standards on Reporting Trials (CONSORT) checklist and scoring system; 5 studies were 8–12 scores; 9 studies were 13–17 scores; and 10 studies were 18–22 scores. All the RCTs had satisfied quality. The details were described in Table 2.
Outcomes
Knee Society Score
All 14 included trials reported Knee Society Score (Table 3), and the pooled standardized mean difference was −0.17 (95 % CI: −0.60, 0.26; n.s.) with notable heterogeneity (I 2 = 94.5 %). And, the results found no evidence of a significant difference between mobile-bearing and fixed-bearing prosthesis groups (Fig. 3).

Forest plots of pooling Knee Society Score
Range of movement
Eleven of the trials reported on the range of movement (Table 3). No evidence indicated a difference in the ROM between two groups (Fig. 4). The pooled standardized mean difference was −0.05 (95 % CI: −0.63, 0.53; n.s.), and evidence showed a notable heterogeneity (I 2 = 94.8 %).

Forest plots of pooling range of movement
Radiolucent line
All 11 included trials reported radiolucent line (Table 4), and the pooled analysis across all studies showed evidence of no significant difference in radiolucent line between mobile-bearing and fixed-bearing prosthesis groups (OR, 1.03, 95 % CI 0.74, 1.44; I 2 = 0.0 %, n.s.). Evidence showed no heterogeneity (Fig. 5).

Forest plots of pooling radiolucent line
Patient preference
Six of the trials reported patient preference for two kinds of prosthesis (Table 4). Overall, there were no significant differences in patient preference between mobile-bearing and fixed-bearing prosthesis groups (OR, 1.15, 95 % CI 0.82, 1.61; I 2 = 0.0 %, n.s.). Evidence showed no heterogeneity, and the pooled result was stable (Fig. 6).

Forest plots of pooling patient preference
Walking support
Four of the trials reported the percentage of walking support after TKA (Table 4). A pooled analysis of the studies found no significant difference in percentage of walking support between mobile-bearing and fixed-bearing prosthesis groups (OR, 1.07, 95 % CI 0.68, 1.70; I 2 = 0.0 %, n.s.). Evidence showed no heterogeneity (Fig. 7).

Forest plots of pooling the percentage of walking support after TKA
Pain score
Five of the trials reported the pain score after operation (Table 4). The pooled analysis of the studies found a significant difference in pain score between two groups (OR, 0.66, 95 % CI 0.46, 0.94; p = 0.022, I 2 = 25.5 %). Evidence showed moderate heterogeneity (Fig. 8).

Forest plots of pooling the pain score after TKA
Complications
Twelve of the trials reported complications (Table 4). A pooled analysis of the studies found no evidence of a significant difference in complications between mobile-bearing and fixed-bearing prosthesis groups (OR, 0.85, 95 % CI 0.59, 1.21; I 2 = 27.1 %, n.s.) (Fig. 9). Evidence showed moderate heterogeneity, and the pooled result was stable.

Forest plots of pooling the complications after TKA
Discussion
The most important findings of the present study were concluded below. With regard to Knee Society Score and range of movement, a random-effects model was used in the meta-analysis. There was significant heterogeneity between studies (I 2 > 50 %), as shown in Figs. 3. 4; however, results showed no significant difference between mobile-bearing and fixed-bearing prosthesis groups. For the other measures, the results of radiolucent line, patient preference, walking support, and complications all showed no significant difference between two groups with no significant heterogeneity between studies (I 2 < 50 %). Only for the pain score, a significant difference between two groups was demonstrated with low heterogeneity (I 2 < 50 %). For the mobile-bearing TKA, one theoretical advantage is the ability to self-align and therefore to accommodate small errors in component placement. So, this reason might explain the less incidence of anterior knee pain in mobile-bearing TKA group.
Our findings were basically consistent with a recent meta-analysis by Wen et al. [30], which included 15 trials, and another systematic review by Smith et al. [27], which included 14 trials; however, more studies with higher amount cases were included in the analysis. Furthermore, this study was a complete meta-analysis about clinical and radiological results in TKA using either mobile or fixed bearing; comprehensive evaluating indicators were discussed in this study, which included Knee Society Score, range of movement, radiolucent line, patient preference, walking support, and complications. So, this study provided a more credible and stable evidence in comparing the outcomes between mobile-bearing TKA and fixed-bearing TKA. Reviewing a meta-analysis of fixed versus mobile-bearing unicompartmental knee replacement (UKR) by. Smith et al. [28], they got the same conclusions with our study that there was no significant difference in clinical outcome or complication rate between mobile- and fixed-bearing UKR.
Mobile meniscal-bearing knee replacements have some theoretical advantages over fixed-bearing devices, including improved stress distribution between the femoral and tibial components, reducing loosening forces at the bone-implant interface and minimizing polyethylene wear [4, 8, 24]. Rotational mobility of the bearing surface might also allow for better reproduction of tibial internal rotation during flexion and improved patellofemoral tracking, which could result in decreased problems with stability and anterior knee pain. Laboratory data from joint simulator and computerized simulation analysis using static and dynamic finite element models seem to suggest that mobile-bearing designs are advantageous in reducing linear polyethylene wear caused by delamination and pitting [5]. However, clinical studies have not yet proven better results or increased knee function for mobile-bearing design series when compared with fixed-bearing designs. The purpose of this meta-analysis is to combine the data from all available RCT to establish whether the use of mobile-bearing implants improves the clinical results of patients over those of fixed-bearing knee implants.
There were several strengths in this review; an exhaustive search strategy was used, including great amount high quality RCTs. All included studies were assessed rigorously by revised Jadad scale and Consolidated Standards on Reporting Trials (CONSORT) checklist and scoring system. When came to heterogeneity, a random-effects model was performed to control the veracity and stability of pooled results.
Although this study was believed to be the most comprehensive meta-analysis of RCT-based evidence for the comparisons between mobile-bearing and fixed-bearing prosthesis groups, we acknowledged that this study has a number of limitations. The general lack of random sequence production and allocation concealment methods in the included RCTs made it difficult to assess their methodological quality, thereby the risk of bias and potential to overestimate the effect may be existent. Our evidence showed considerable statistical heterogeneity for several outcomes across the trials. Although we minimized selection bias by including only RCTs, it is usually impossible to blind people accepting an operation, so performance bias is inevitable in the present meta-analysis. The different follow-up between trials was also considered to cause statistical heterogeneity. What is more, we did not limit the language in the process of literature retrieval, but only Chinese- and English-language trials were identified according to inclusion criteria, and this might have resulted in language bias.
Conclusion
This meta-analysis demonstrated that the fixed- and mobile-bearing prostheses share no obvious statistical difference in terms of clinical and radiologic outcomes except the pain score. The pooled analysis of large numbers of RCT showed mobile-bearing prostheses had no obvious advantages over fixed-bearing prostheses. However, the less incidence of pain could be the advantage for selecting mobile-bearing TKA in clinical work. For exploring the efficacy of mobile-bearing prostheses perfectly, well-designed RCTs to compare the different types of prosthesis are still needed to be run.
References
Aglietti P, Baldini A, Buzzi R, Lup D, De Luca L (2005) Comparison of mobile-bearing and fixed-bearing total knee arthroplasty: a prospective randomized study. J Arthroplast 20:145–153
Bhan S, Malhotra R, Kiran EK, Shukla S, Bijjawara M (2005) A comparison of fixed-bearing and mobile-bearing total knee arthroplasty at a minimum follow-up of 4.5 years. J Bone Jt Surg Am 87:2290–2296
Breugem SJ, Sierevelt IN, Schafroth MU, Blankevoort L, Schaap GR, van Dijk CN (2008) Less anterior knee pain with a mobile-bearing prosthesis compared with a fixed-bearing prosthesis. Clin Orthop Relat Res 466:1959–1965
Buechel FF, Pappas MJ (1990) Long-term survivorship analysis of cruciate-sparing versus cruciate-sacrificing knee prostheses using meniscal bearings. Clin Orthop Relat Res 260:162–169
Callaghan JJ, Insall JN, Greenwald AS, Dennis DA, Komistek RD, Murray DW, Bourne RB, Rorabeck CH, Dorr LD (2000) Mobile-bearing knee replacement: concepts and results. J Bone Jt Surg 82:1020–1041
Delport HP, Banks SA, De Schepper J, Bellemans J (2006) A kinematic comparison of fixed- and mobile-bearing knee replacements. J Bone Jt Surg Br 88:1016–1021
Gioe TJ, Glynn J, Sembrano J, Suthers K, Santos ER, Singh J (2009) Mobile and fixed-bearing (all-polyethylene tibial component) total knee arthroplasty designs. A prospective randomized trial. J Bone Jt Surg Am 91:2104–2112
Goodfellow JW, O’Connor J (1978) The mechanics of the knee and prosthesis design. J Bone Jt Surg Br 60:358–369
Grupp TM, Kaddick C, Schwiesau J, Maas A, Stulberg SD (2009) Fixed and mobile bearing total knee arthroplasty–influence on wear generation, corresponding wear areas, knee kinematics and particle composition. Clin Biomech (Bristol, Avon) 24:210–217
Hansson U, Toksvig-Larsen S, Jorn LP, Ryd L (2005) Mobile vs. fixed meniscal bearing in total knee replacement: a randomised radiostereometric study. Knee 12:414–418
Harrington MA, Hopkinson WJ, Hsu P, Manion L (2009) Fixed- vs mobile-bearing total knee arthroplasty: does it make a difference?–a prospective randomized study. J Arthroplast 24:24–27
Hasegawa M, Sudo A, Uchida A (2009) Staged bilateral mobile-bearing and fixed-bearing total knee arthroplasty in the same patients: a prospective comparison of a posterior-stabilized prosthesis. Knee Surg Sports Traumatol Arthrosc 17:237–243
Higuchi H, Hatayama K, Shimizu M, Kobayashi A, Kobayashi T, Takagishi K (2009) Relationship between joint gap difference and range of motion in total knee arthroplasty: a prospective randomised study between different platforms. Int Orthop 33:997–1000
Jacobs WC, Christen B, Wymenga AB, Schuster A, van der Schaaf DB, Ten Ham A, Wehrli U (2012) Functional performance of mobile versus fixed bearing total knee prostheses: a randomised controlled trial. Knee Surg Sports Traumatol Arthrosc 20:1450–1455
Jawed A, Kumar V, Malhotra R, Yadav CS, Bhan S (2012) A comparative analysis between fixed bearing total knee arthroplasty (PFC Sigma) and rotating platform total knee arthroplasty (PFC-RP) with minimum 3-year follow-up. Arch Orthop Trauma Surg 132:875–881
Jolles BM, Grzesiak A, Eudier A, Dejnabadi H, Voracek C, Pichonnaz C, Aminian K, Martin E (2012) A randomised controlled clinical trial and gait analysis of fixed- and mobile-bearing total knee replacements with a five-year follow-up. J Bone Jt Surg Br 94:648–655
KAT Trial Group, Johnston L, MacLennan G, McCormack K, Ramsay C, Walker A (2009) The Knee Arthroplasty Trial (KAT) design features, baseline characteristics, and two-year functional outcomes after alternative approaches to knee replacement. J Bone Jt Surg Am 91:134–141
Kim YH, Kim DY, Kim JS (2007) Simultaneous mobile- and fixed-bearing total knee replacement in the same patients. A prospective comparison of mid-term outcomes using a similar design of prosthesis. J Bone Jt Surg Br 89:904–910
Kim YH, Yoon SH, Kim JS (2009) Early outcome of TKA with a medial pivot fixed-bearing prosthesis is worse than with a PFC mobile-bearing prosthesis. Clin Orthop Relat Res 467:493–503
Lädermann A, Lübbeke A, Stern R, Riand N, Fritschy D (2008) Fixed-bearing versus mobile-bearing total knee arthroplasty: a prospective randomised, clinical and radiological study with mid-term results at 7 years. Knee 15:206–210
Liu Y, Cao L, Li G, Zeng Y, Peng G, Gong B (2011) Comparison of anterior knee pain between fixed-bearing prosthesis and mobile-bearing prosthesis after total knee arthroplasty. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 25:266–271
Lizaur-Utrilla A, Sanz-Reig J, Trigueros-Rentero MA (2012) Greater satisfaction in older patients with a mobile-bearing compared with fixed-bearing total knee arthroplasty. J Arthroplast 27:207–212
McEwen HM, Barnett PI, Bell CJ, Farrar R, Auger DD, Stone MH, Fisher J (2005) The influence of design, materials and kinematics on the in vitro wear of total knee replacements. J Biomech 38:357–365
O’Connor JJ, Goodfellow JW (1996) Theory and practice of meniscal knee replacement: designing against wear. Proc Inst Mech Eng 210:217–222
Price AJ, Rees JL, Beard D, Juszczak E, Carter S, White S, de Steiger R, Dodd CA, Gibbons M, McLardy-Smith P, Goodfellow JW, Murray DW (2003) A mobile-bearing total knee prosthesis compared with a fixed-bearing prosthesis. A multicentre single-blind randomised controlled trial. J Bone Jt Surg Br 85:62–67
Sansone V, da Gama MalchèrM (2004) Mobile-bearing total knee prosthesis: a 5- to 9-year follow-up of the first 110 consecutive arthroplasties. J Arthroplast 19:678–685
Smith H, Jan M, Mahomed NN, Davey JR, Gandhi R (2011) Meta-analysis and systematic review of clinical outcomes comparing mobile bearing and fixed bearing total knee arthroplasty. J Arthroplast 26:1205–1213
Smith TO, Hing CB, Davies L, Donell ST (2009) Fixed versus mobile bearing unicompartmental knee replacement: a meta-analysis. Orthop Traumatol Surg Res 95:599–605
Watanabe T, Tomita T, Fujii M, Hashimoto J, Sugamoto K, Yoshikawa H (2005) Comparison between mobile-bearing and fixed-bearing knees in bilateral total knee replacements. Int Orthop 29:179–181
Wen Y, Liu D, Huang Y, Li B (2011) A meta-analysis of the fixed-bearing and mobile-bearing prostheses in total knee arthroplasty. Arch Orthop Trauma Surg 131:1341–1350
Wohlrab D, Hube R, Zeh A, Hein W (2009) Clinical and radiological results of high flex total knee arthroplasty: a 5 year follow-up. Arch Orthop Trauma Surg 129:21–24
Woolson ST, Epstein NJ, Huddleston JI (2011) Long-term comparison of mobile-bearing vs fixed-bearing total knee arthroplasty. J Arthroplast 26:1219–1223
Woolson ST, Northrop GD (2004) Mobile- vs. fixed-bearing total knee arthroplasty: a clinical and radiologic study. J Arthroplast 19:135–140
Wylde V, Learmonth I, Potter A, Bettinson K, Lingard E (2008) Patient-reported outcomes after fixed- versus mobile-bearing total knee replacement: a multi-centre randomised controlled trial using the Kinemax total knee replacement. J Bone Jt Surg Br 90:1172–1179
Zeng Y, Cao L, Liu Y, Peng GF, Peng LB, Yang DS, A DL, Xu BY, Gong BJ (2011) Early clinical outcomes of fixed-bearing versus mobile-bearing total knee arthroplasty. Zhonghua Yi Xue Za Zhi 91:752–756
Conflict of interest
The authors declare that they have no conflict of interest.
Author information
Authors and Affiliations
Corresponding author
Additional information
Yu-Lin Li and Qiang Wu have equal contribution to this research.
Rights and permissions
About this article
Cite this article
Li, YL., Wu, Q., Ning, GZ. et al. No difference in clinical outcome between fixed- and mobile-bearing TKA: a meta-analysis. Knee Surg Sports Traumatol Arthrosc 22, 565–575 (2014). https://doi.org/10.1007/s00167-012-2313-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-2313-y