
Abstract
Purpose
An ongoing controversy exists on whether mobile-bearing design is superior over fixed-bearing design in unicondylar knee arthroplasties (UKAs). The present study conducted a systematic review to ascertain differences in performance between fixed- and mobile-bearing designs in UKAs.
Methods
A literature search was performed in PubMed, Embase, Scopus and the Cochrane Library. A total of 9 comparative studies involving 915 knees comparing outcomes of mobile-bearing UKAs with fixed-bearing UKAs were included in the current analysis. Outcomes of interest included knee function, quality of life, radiographic outcomes, reasons and incidence of reoperation, timing of failures, and survivorship.
Results
The results presented no significant differences between the two designs in terms of knee scores, range of motion, limb alignment, implant positioning, incidence of radiolucent lines and overall reoperation rates. However, their differences have been noted in their modes and timing of failures. Early failures are related to the risk of bearing dislocation in the mobile-bearing design. In contrast, later failures are related to the risk of polyethylene wear in the fixed-bearing design.
Conclusions
The available evidence has not confirmed the advantage of mobile-bearing UKAs over fixed-bearing UKAs but pointed out specific modes of failure.
Level of evidence
Therapeutic study (systematic review and meta-analysis), Level III.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
A variety of surgical options are available in the treatment of isolated compartment arthritis of the knee [8, 24, 62]. These options include unicondylar knee arthroplasty (UKA) and total knee arthroplasty (TKA). Early published outcomes of the UKA have shown unfavourable performance with subsidence, loosening, high wear and progression of arthritis to the remaining compartments [40, 48]. Recently, performing UKA has been a resurgence of interest, considering the advances in surgical technique, instrumentation, material and implant design [11, 12, 35, 59]. Numerous studies have suggested good survivorship and excellent function for selected patients with intact anterior cruciate ligaments and unicompartmental osteoarthritis following UKAs, even among the active and obese population [17, 41, 66]. The proposed advantages of the UKA include smaller incision, less blood loss [26, 65], greater range of motion (ROM) [36, 46], faster recovery [18, 47, 50], lower perioperative morbidity [19, 46], preservation of normal kinematics [36, 52] and less overall costs [56, 64]. Furthermore, conversion of a failed UKA to TKA is not as complicated as a revision TKA due to the preservation of bone stock and sparing of ligaments [27, 37, 60].
Currently, two different fundamental design concepts are available on UKAs: fixed-bearing (FB) and mobile-bearing (MB) knee prostheses [4, 16, 63]. MB design proponents cite the potential advantages of a congruent bearing with lower contact stresses and polyethylene wear rates [44, 45, 61]. In addition, the mobile design is considered to recreate native knee kinematics more closely [1]. MB design has been experiencing an increase in popularity due to its theoretical advantages over the FB design. However, several clinical studies have not been consistent in demonstrating the advantages of one bearing design over the other [3, 7, 9, 15, 16, 21, 39, 51, 67]. In three cohort studies [16, 51, 67], no mid-term differences and long-term differences in survivorship were found between these two designs in UKAs.
The debate of whether MB UKA offers clinical and radiographic advantages over FB UKA for isolated end-stage symptomatic osteoarthritis of the knee has continued to generate substantial controversy in the orthopedic community [5, 42, 63]. Although there is already a meta-analysis on clinical differences between fixed- and mobile-bearing UKAs [63], more RCTs have been coming out with different outcomes in the past few years [3, 7, 51, 67]. The present study has presented an evidence-based review to determine whether the MB and FB designs of medial UKAs differ in knee score, ROM, quality of life, radiographic outcomes, reasons and incidence of reoperation, timing of failures, and survivorship.
Materials and methods
Only studies meeting the following criteria were included in this systematic review: (1) prospective and retrospective studies directly comparing MB with FB knee prostheses; (2) patients with isolated medial compartment arthrosis of the knee; and (3) reported clinical and radiographic outcomes of UKAs. All patients in these studies were scheduled to undergo their primary UKA surgery. Studies with the following conditions were excluded from the present study: (1) all case reports, case series, comments, letters, editorials, expert opinions, review and other non-comparative studies; (2) publications presenting data from national registries; and (3) in vitro/vivo wear testing, cadaver study and retrieval specimen study.
Two reviewers performed a systematic search of the medical literature published between January 1990 and December 2011 independently. The searched sources included PubMed, EMBASE, Scopus and the Cochrane Central Register of Controlled Trials. The search strategy was based on combinations of “fixed-bearing”, “mobile-bearing”, “meniscal-bearing”, “unicondylar”, “unicompartmental”, “replacement” and “arthroplasty”. In addition, these electronic searches were supplemented with manual searches in published articles, major orthopedic textbooks and table of contents from six major orthopedic journals, namely The Journal of Bone and Joint Surgery (American and British volumes), Clinical Orthopedic and Related Research, The Journal of Arthroplasty, The Knee, and Knee Surgery Sports Traumatology Arthroscopy. No restrictions regarding the language of publication were imposed.
The two independent reviewers extracted the relevant data in duplicate, including number of patients/knees, preoperative diagnosis, demographic data (age, sex, weight, height, etc.), duration of the follow-up, type of prosthesis, surgical approach, and clinical and radiographic outcome measures. They assessed the levels of evidence from the included articles according to the rating measure published in The Journal of Bone and Joint Surgery (American Volume) [68]. The outcome measures of the current study included knee scores, ROM, quality of life, limb alignment, implant positioning, radiolucent lines (RLLs), reason and incidence of reoperation, timing of failure, and survivorship.
Statistical analysis
Statistical analysis for categorical variables was carried out using risk ratio (RR) as the summary statistic. For continuous variables, statistical analysis was carried out using the weighted mean difference (WMD) as the summary statistic. The outcome measure tested was assessed for heterogeneity by measuring the chi-square statistic and calculated I 2. A value of less than 25 % was considered low heterogeneity, 50 % moderate heterogeneity and 75 % high heterogeneity [25]. In any case, a random effects model (DerSimonian-Laird method) was used to calculate the summary WMD/RR and 95 % CI. The random effect model assumes variation among studies, and therefore, the calculated ratio has a more conservative value [10]. The present work estimated publication bias using a graphical method (funnel plot). Statistical analyses were performed with the Review Manager version 5.0 for Windows XP (Copenhagen: the Nordic Cochrane Centre, Cochrane Collaboration) and SPSS version 13.0 for Windows (SPSS Inc., Chicago, Illinois).
Results
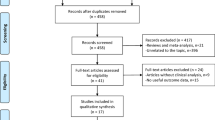
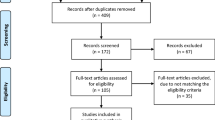
Initial electronic and manual search identified 303 studies. A total of 160 were excluded for the following reasons: (1) UKA revision; (2) lateral UKA; (3) cadaver study; (4) retrieval study; and (5) in vivo/vitro wear analyses. The remaining 143 studies were retrieved for more detailed evaluation. Next, 68 studies were excluded for the following reasons: they included data from national registries; they are traditional or systematic literature reviews; they did not have control group; and they did not present outcome of interest. A total of 9 studies reporting 797 participants (915 knees) met the eligibility criteria of the present work. A flow diagram is shown in Fig. 1. From the 9 studies, 3 were RCTs/qRCTs [9, 21, 39] and 6 were retrospective comparative studies [3, 7, 15, 16, 51, 67]. One study [15] omitted the patient’s age and gender. The other 8 studies demonstrated that the total MB population included 160 males and 191 females with mean age ranging from 63 to 74 years. The total FB population was 202 males and 264 females with mean age ranging from 62.8 to 70.3 years. Mean weight or body mass index was reported in five studies [16, 21, 39, 51, 67]. Preoperative knee score was reported in three studies [9, 21, 51]. Preoperative limb alignment was reported in three studies [15, 16, 51]. Mean height was reported in only two studies [7, 16]. Most studies assessed whether the two treatment arms are comparable with important preintervention parameters, such as age, sex, weight and ROM, which can affect postoperative outcomes following UKAs. The mean follow-up period range was from 12.4 months to 17.2 years; the follow-up period was not stated in one study [15]. In seven studies, the follow-up period duration was beyond 4 years [3, 7, 9, 16, 21, 51, 67], whereas in one study, it was beyond 10 years [51]. Table 1 shows additional details about study characteristics and participant demographics.

Flowchart for the identification of eligible studies
The 9 eligible studies noted the use of FB knee prostheses from five manufacturers: Miller-Galante (Zimmer), Robert Brigham (Johnson & Johnson), St.Georg (LINK) and Optetrak (Exactech). The MB knee prostheses were from two manufacturers: AMC (Alphanorm) and Oxford (Biomet). Although most of the reports included conventional criteria for patient selection, the indication of the index procedure varied among these studies to a certain degree. The indication/contraindication proposed by Kozinn and Scott [33] was applied to patients with UKA in four studies [7, 15, 16, 39], and three other studies [3, 21, 67] adhered to the criteria of Goodfellow et al. [22].
Knee score and ROM
Five studies assessed the Knee Society Score (KSS) [9, 16, 39, 51, 67]; two studies assessed the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score [39, 67]; one studies assessed the Oxford Knee Score (OKS) [21]; one study assessed the Italian Orthopaedic UKR’s Users Group(GIUM) score [9]; one study assessed the International Knee Society score [7]; and one study assessed the Bristol knee score [21]. These studies reported no significant statistical differences between MB and FB patients on all knee scores measures. Although statistical heterogeneity was high in the assessment of KSS (knee score and function score; I 2 = 87 % and I 2 = 89 %, respectively), data from meta-analysis did not show significant statistical differences between FB and MB UKAs (P = 0.92 and P = 0.16, respectively). Postoperative ROM or flexion was assessed in four studies [8, 22, 40, 54]. On review, all studies reported similar ROM or flexion for both groups (P = 0.4; WMD = 3.4; 95 % CI, −4.6 to 11.2).
Quality of life
Quality of life was measured using two methods: Short Form (SF)-12 and SF-36. Li et al. [39] found that SF-36 scores improved significantly from preoperative to 2 years postoperatively in both groups without significant differences between the groups. Whittaker et al. [67] observed higher scores in the MB group in the SF-12 scores at the latest follow-up for both mental (P = 0.04) and physical (P = 0.04) components compared with the FB group.
Radiographic assessments
According to the Kennedy classification [30], malalignment of the knee is defined as a deviance from Zone 2 or C. It occurred in 11.2 % of knees in the MB group versus 12.5 % of knees in the FB group (P = 0.7; RR = 0.9; 95 % CI, 0.5–1.7). The MB group displayed the following postoperative results: 135 knees had correct alignment, 2 knees had alignment in varus, and 15 knees had alignment in valgus. The FB group displayed the following postoperative results: 147 knees had correct alignment, 13 knees had alignment in varus, and 8 knees had alignment in valgus.
Based on the radiographs, the frequency of RLL was higher in the MB group than in the FB group (30.8 vs. 12.5 %), but their difference was not significant (P = 0.8, RR = 0.8; 95 % CI, 0.1–5.7).
Reason and incidence of reoperation, timing of failures, and survivorship
In the MB group with a mean of 5.0 years (range of 0.1–17.7), 41 knees experienced failure and underwent subsequent reoperations. Reoperations were performed for aseptic loosening in 13 patients with a mean of 5.9 years (range of 1.0–17.7); progression of osteoarthritis in 12 patients with a mean of 7.4 years (range of 2.9–11.0); bearing dislocation in 7 patients with a mean of 0.4 years (range of 0.2–0.7); postoperative persistent pain in 2 patients with a mean of 3.3 year (range, 2.8–3.7); postoperative infection in 2 patients with a mean of 6.5 years (range of 0.1–12.9); detained cement in 2 patients; atraumatic medial tibial plateau fracture in 1 patients at 8 months; bearing impingement in 1 patient at 3 years; and inflammatory arthritis in 1 patient at 2 years.
A total of 52 knees from the FB group were reoperated on at a later mean of 6.3 years. The failure occurred in 15 patients for polyethylene wear at a mean of 8.3 years (range of 2.0–14.3 years); 14 patients for progression of osteoarthritis at a mean of 7.1 years (range of 2.0–15.0); 13 patients for aseptic loosening at a mean of 5.7 years (range of 2.0–14.6); and six patients for persistent pain at a mean of 3.8 years (range of 1.5–7.2). Two additional patients were reoperated for tibial fracture and instability following trauma at 31 months and 3.4 years, respectively. A single patient had a reoperation due to septic loosening at 0.3 years. One FB knee was reported as having detained bone cement that needed surgery to remove the cement segment.
Significant difference was observed in the mean time for reoperation between the two groups, the number favoured FB prosthesis (P = 0.016). The frequencies for aseptic loosening, persistent pain, progression of arthritis or overall reoperation between the two groups were not significantly different. However, the differences in frequency of bearing dislocation and polyethylene wear were statistically significant between the two groups (Fig. 2).

Forest plot for reoperations following UKAs
Three studies addressing MB and FB UKAs reported survival rates of 80–97 %, with a mean follow-up ranging from 3.6 to 17.2 years [16, 51, 67] (Table 2). These studies suggested that no significant difference in implant survivorship occurred between the two groups. However, Bhattacharya et al. [3] compared the survival of the two implants using the Cox regression analysis model, showing that the FB prosthesis has the worse survivorship (P < 0.05).
Publication bias
Publication bias was assessed with funnel plots, which demonstrate the relationship between the study sample size and the precision in estimating the treatment effect. The funnel plot visually demonstrated mild asymmetry, suggesting minimal evidence of publication bias (Fig. 3).

Funnel plot demonstrating minimal publication bias from reoperation outcome
Discussion
The most important finding of the present study was that the two designs in UKAs did not differ in the following: (1) knee score; (2) quality of life; (3) radiographic outcomes; and (4) incidence of reoperation. However, their differences have been noted in their modes and timing of failures. Early failures are related to the risk of bearing dislocation in the mobile-bearing design. In contrast, later failures are related to the risk of polyethylene wear in the fixed-bearing design.
In the current study, the frequency of RLL was higher in the MB group than the FB group. However, the difference was not significant. Periprosthetic RLLs following UKAs have been described as inclusive of two subtypes (physiological and pathological), but their etiological significances remain unclear [28]. Many authors found that the presence of RLLs is not associated with lower knee scores or higher revision rates in mid- and long-term follow-up study [23, 51, 55, 67]. Price et al. [55] followed-up 89 patients with 114 medial Oxford UKAs. They reported a 15-year survivorship of up to 92 % with complete RLLs in 96 % of the cases around the tibial component. Whittaker et al. [67] found that patients with non-progressive RLLs continue to function well without symptoms and subsidence. Parratte et al. [51] reported a high incidence of RLLs in MB and FB prostheses (69 and 24 %, respectively) at a minimum follow-up of 15 years. Survivorship for patients with or without RLLs did not differ. Although the sensitivity and specificity of RLLs using standard radiographs appear to be acceptable, their intraobserver and interobserver reliabilities were poor [28]. If a non-parallel X-ray beam obscures their characteristic features, the RLLs will be missed unless fluoroscopic control is used in the tibial component of Oxford UKA [23]. To improve the zonal reliability of the assessment of RLLs, some authors suggested that fluoroscopically guided radiographs may be used [23, 28].
Interestingly, the current research clearly demonstrated a lower incidence with polyethylene wear in MB design. One major goal of the MB design is to reduce the overall polyethylene wear by increasing the contact area and congruency while minimizing the constraint and maintaining the normal knee motion [29]. Retrieval studies reported low wear rates (0.01–0.043 mm/year) in well-functioning MB UKA through in vivo measurement [14, 29, 53]. The maximum linear penetration reported for MB UKA was an order of magnitude lower than that reported for FB UKA (0.15 mm/year) [2, 14]. Manson et al. [43] examined wear damage of three modern UKAs, including two FB and one MB design. They found that delamination and surface deformation are more common in FB designs. It should be noted, however, that in contrast to the above-mentioned studies, in vitro wear analysis found that fixed-bearing design is superior over mobile-bearing design. Brockett et al. [6] compared the wear performance of a low-conformity FB UKA with a conforming MB UKA using a physiological knee wear simulator. Under identical kinematic conditions, the relatively low-conforming FB prosthesis showed lower wear compared with the more conforming anterior–posterior sliding MB prosthesis. Another knee simulator study, limited to level walking, found that the MB design exhibits higher wear rates than the FB design [34].
Early UKAs from mid-term follow-up had a high failure rate of 15–28 % for aseptic loosening, polyethylene wear and progression of osteoarthritis [40, 42, 44, 48–50, 63]; however, recent clinical literature showed a steady improvement, with excellent mid- and long-term survivorship for both FB and MB UKAs [13, 16, 51, 54, 67]. Earlier data from a Swedish multicenter survival study showed that the MB UKA has twice the revision rate of the FB UKA [38]. Later arthroplasty registries comparing FB and MB UKAs did not confirm the superiority of one design over the other in knee function and survivorship [31, 32, 57, 58]. Some studies by surgeons, who have designed UKAs or are from specialized centres, tended to report more favourable outcomes [35, 55]. In a report from the Swedish Arthroplasty Registry, Robertsson et al. [57] found that revision rate is related to the annual surgical volume of Oxford UKA. They suggested greater learning curve and higher technical demands for the MB design, which could partially explain the difference in the reported outcomes. Given that excellent survivorship for a UKA has been documented, high-quality RCT with longer-term follow-up is required to assess the true differences in implant longevity of UKAs performed by experienced surgeons.
The design of the current study had several limitations. More than half of the studies reviewed were retrospective cohort studies. The retrospective nature of these studies, which is more susceptible to selection bias than prospective studies, precluded the ability of the present work to control confounding factors [20]. Additionally, publication bias may have affected the results; the present review did not search unpublished studies. However, the funnel plot demonstrated minimal evidence of publication bias.
Conclusion
In conclusion, both bearing designs have provided excellent knee function and survivorship in UKAs. The available evidence has shown similar performance of MB design in comparison with FB design in UKAs, regardless of the confounding factors that have been detected in the present study. The current review has not confirmed the superiority of one design over another in knee function, implant alignment and overall reoperation rate but has pointed out specific modes of failure.
References
Argenson JN, Komistek RD, Aubaniac JM, Dennis DA, Northcut EJ, Anderson DT, Agostini S (2002) In vivo determination of knee kinematics for subjects implanted with a unicompartmental arthroplasty. J Arthroplasty 17:1049–1154
Ashraf T, Newman JH, Desai VV, Beard D, Nevelos JE (2004) Polyethylene wear in a non-congruous unicompartmental knee replacement: a retrieval analysis. Knee 11:177–181
Bhattacharya R, Scott CE, Morris HE, Wade F, Nutton RW (2012) Survivorship and patient satisfaction of a fixed bearing unicompartmental knee arthroplasty incorporating an all-polyethylene tibial component. Knee 19:348–351
Bonutti PM, Dethmers DA (2008) Contemporary unicompartmental knee arthroplasty: fixed vs mobile bearing. J Arthroplasty 23(7 Suppl):24–27
Borus T, Thornhill T (2008) Unicompartmental knee arthroplasty. J Am Acad Orthop Surg 16:9–18
Brockett CL, Jennings LM, Fisher J (2011) The wear of fixed and mobile bearing unicompartmental knee replacements. Proc Inst Mech Eng H 225:511–519
Catani F, Benedetti MG, Bianchi L, Marchionni V, Giannini S, Leardini A (2012) Muscle activity around the knee and gait performance in unicompartmental knee arthroplasty patients: a comparative study on fixed- and mobile-bearing designs. Knee Surg Sports Traumatol Arthros 20:1042–1048
Catier C, Turcat M, Jacquel A, Baulot E (2011) The Unispacer™ unicompartmental knee implant: its outcomes in medial compartment knee osteoarthritis. Orthop Traumatol Surg Res 97:410–417
Confalonieri N, Manzotti A, Pullen C (2004) Comparison of a mobile with a fixed tibial bearing unicompartmental knee prosthesis: a prospective randomized trial using a dedicated outcome score. Knee 11:357–362
DerSimonian R, Laird N (1986) Meta-analysis in clinical trials. Control Clin Trials 7:177–188
Dervin GF, Carruthers C, Feibel RJ, Giachino AA, Kim PR, Thurston PR (2011) Initial experience with the Oxford unicompartmental knee arthroplasty. J Arthroplasty 26:192–197
Deschamps G, Chol C (2011) Fixed-bearing unicompartmental knee arthroplasty. Patients’selection and operative technique. Orthop Traumatol Surg Res 97:648–661
Deshmukh RV, Scott RD (2001) Unicompartmental knee arthroplasty: long-term results. Clin Orthop Relat Res 392:272–278
Eillison PJ, Traynor A, Casey BP, Collins SN (2011) Wear of a mobile bearing unicompartmental knee replacement prosthesis: a comparison of in vitro and in vivo wear rates. J ASTM Int 8:1–6
Emerson RH Jr, Head WC, Peters PC Jr (1992) Soft-tissue balance and alignment in medial unicompartmental knee arthroplasty. J Bone Joint Surg Br 74:807–810
Emerson RH, Hansborough T, Reitman RD, Rosenfeldt W, Higgins LL (2002) Comparison of a mobile with a fixed-bearing unicompartmental knee implant. Clin Orthop Relat Res 404:62–70
Felts E, Parratte S, Pauly V, Aubaniac JM, Argenson JN (2010) Function and quality of life following medial unicompartmental knee arthroplasty in patients 60 years of age or younger. Orthop Traumatol Surg Res 96:861–867
Foote JA, Smith HK, Jonas SC, Greenwood R, Weale AE (2010) Return to work following knee arthroplasty. Knee 17:19–22
Furnes O, Espehaug B, Lie SA, Vollset SE, Engesaeter LB, Havelin LI (2007) Failure mechanisms after unicompartmental and tricompartmental primary knee replacement with cement. J Bone Joint Surg Am 89:519–525
Geneletti S, Richardson S, Best N (2009) Adjusting for selection bias in retrospective, case-control studies. Biostatistics 10:17–31
Gleeson RE, Evans R, Ackroyd CE, Webb J, Newman JH (2004) Fixed or mobile bearing unicompartmental knee replacement? A comparative cohort study. Knee 11:379–384
Goodfellow JW, Tibrewal SB, Sherman KP, O’Connor JJ (1987) Unicompartmental Oxford Meniscal knee arthroplasty. J Arthroplasty 2:1–9
Gulati A, Chau R, Pandit HG, Gray H, Price AJ, Dodd CA, Murray DW (2009) The incidence of physiological radiolucency following Oxford unicompartmental knee replacement and its relationship to outcome. J Bone Joint Surg Br 91:896–902
Heyse TJ, Khefacha A, Peersman G, Cartier P (2012) Survivorship of UKA in the middle-aged. Knee 19:585–591
Higgins JP, Thompson SG, Deeks JJ, Altman DG (2003) Measuring inconsistency in meta-analyses. BMJ 327:557–560
Jeer PJ, Cossey AJ, Keene GC (2005) Haemoglobin levels following unicompartmental knee arthroplasty: influence of transfusion practice and surgical approach. Knee 12:358–361
Johnson S, Jones P, Newman JH (2007) The survivorship and results of total knee replacements converted from unicompartmental knee replacements. Knee 14:154–157
Kalra S, Smith TO, Berko B, Walton NP (2011) Assessment of radiolucent lines around the Oxford unicompartmental knee replacement: sensitivity and specificity for loosening. J Bone Joint Surg Br 93:777–781
Kendrick BJ, Longino D, Pandit H, Svard U, Gill HS, Dodd CA, Murray DW, Price AJ (2010) Polyethylene wear in Oxford unicompartmental knee replacement: a retrieval study of 47 bearings. J Bone Joint Surg Br 92:367–373
Kennedy WR, White RP (1987) Unicompartmental arthroplasty of the knee. Postoperative alignment and its influence on overall results. Clin Orthop Relat Res 221:278–285
Koskinen E, Eskelinen A, Paavolainen P, Pulkkinen P, Remes V (2008) Comparison of survival and cost-effectiveness between unicondylar arthroplasty and total knee arthroplasty in patients with primary osteoarthritis: a follow-up study of 50,493 knee replacements from the Finnish Arthroplasty Register. Acta Orthop 79:499–507
Koskinen E, Paavolainen P, Eskelinen A, Pulkkinen P, Remes V (2007) Unicondylar knee replacement for primary osteoarthritis: a prospective follow-up study of 1,819 patients from the Finnish Arthroplasty Register. Acta Orthop 78:128–135
Kozinn SC, Scott R (1989) Unicondylar knee arthroplasty: current concepts review. J Bone Joint Surg Am 71:145–150
Kretzer JP, Jakubowitz E, Reinders J, Lietz E, Moradi B, Hofmann K, Sonntag R (2011) Wear analysis of unicondylar mobile bearing and fixed bearing knee systems: a knee simulator study. Acta Biomater 7:710–715
Labek G, Sekyra K, Pawelka W, Janda W, Stöckl B (2011) Outcome and reproducibility of data concerning the Oxford unicompartmental knee arthroplasty: a structured literature review including arthroplasty registry data. Acta Orthop 82:131–135
Laurencin CT, Zelicof SB, Scott RD, Ewald FC (1991) Unicompartmental versus total knee arthroplasty in the same patient. A comparative study. Clin Orthop Relat Res 273:151–156
Levine WN, Ozuna RM, Scott RD, Thornhill TS (1996) Conversion of failed modern unicompartmental arthroplasty to total knee arthroplasty. J Arthroplasty 11:797–801
Lewold S, Goodman S, Knutson K, Robertsson O, Lidgren L (1995) Oxford meniscal bearing knee versus the Marmor knee in unicompartmental arthroplasty for arthrosis. A Swedish multicenter survival study. J Arthroplasty 10:722–731
Li MG, Yao F, Ioppolo J, Nivbrant B, Wood D (2006) Mobile vs. fixed bearing unicondylar knee arthroplasty: a randomized study on short-term clinical outcomes and knee kinematics. Knee 13:365–370
Lindstrand A, Stenström A, Lewold S (1992) Multicenter study of unicompartmental knee revision. PCA, Marmor, and St Georg compared in 3,777 cases of arthrosis. Acta Orthop Scand 63:256–259
Lisowski LA, van den Bekerom MP, Pilot P, van Dijk CN, Lisowski AE (2011) Oxford Phase 3 unicompartmental knee arthroplasty: medium-term results of a minimally invasive surgical procedure. Knee Surg Sports Traumatol Arthrosc 19:277–284
Maduekwe UI, Zywiel MG, Bonutti PM, Johnson AJ, Delanois RE, Mont MA (2010) Scientific evidence for the use of modern unicompartmental knee arthroplasty. Expert Rev Med Devices 7:219–239
Manson TT, Kelly NH, Lipman JD, Wright TM, Westrich GH (2010) Unicondylar knee retrieval analysis. J Arthroplasty 25(6 Suppl):108–111
McEwen HM, Barnett PI, Bell CJ, Farrar R, Auger DD, Stone MH, Fisher J (2005) The influence of design, materials and kinematics on the in vitro wear of total knee replacements. J Biomech 38:357–365
McEwen HM, Fisher J, Goldsmith AA, Auger DD, Hardaker C, Stone MH (2001) Wear of fixed bearing and rotating platform mobile bearing knees subjected to high levels of internal and external tibial rotation. J Mater Sci Mater Med 12:1049–1052
Newman JH, Ackroyd CE, Shah NA (1998) Unicompartmental or total knee replacement? Five-year results of a prospective, randomised trial of 102 osteoarthritic knees with unicompartmental arthritis. J Bone Joint Surg Br 80:862–865
Newman J, Pydisetty RV, Ackroyd C (2009) Unicompartmental or total knee replacement: the 15-year results of a prospective randomised controlled trial. J Bone Joint Surg Br 91:52–57
Palmer SH, Morrison P, Ross AC (1998) Early catastrophic tibial component wear after unicompartmental knee arthroplasty. Clin Orthop Relat Res 350:143–148
Pandit H, Jenkins C, Gill HS, Smith G, Price AJ, Dodd CA, Murray DW (2011) Unnecessary contraindications for mobile-bearing unicompartmental knee replacement. J Bone Joint Surg Br 93:622–628
Panni AS, Vasso M, Cerciello S, Felici A (2012) Unicompartmental knee replacement provides early clinical and functional improvement stabilizing over time. Knee Surg Sports Traumatol Arthrosc 20:579–585
Parratte S, Pauly V, Aubaniac JM, Argenson JN (2012) No long-term difference between fixed and mobile medial unicompartmental arthroplasty. Clin Orthop Relat Res 470:61–68
Patil S, Colwell CW Jr, Ezzet KA, D’Lima DD (2005) Can normal knee kinematics be restored with unicompartmental knee replacement? J Bone Joint Surg Am 87:332–338
Price AJ, Short A, Kellett C, Beard D, Gill H, Pandit H, Dodd CA, Murray DW (2005) Ten-year in vivo wear measurement of a fully congruent mobile bearing unicompartmental knee arthroplasty. J Bone Joint Surg Br 87:1493–1497
Price AJ, Svard U (2011) A second decade lifetable survival analysis of the Oxford unicompartmental knee arthroplasty. Clin Orthop Relat Res 469:174–179
Price AJ, Waite JC, Svard U (2005) Long-term clinical results of the medial Oxford unicompartmental knee arthroplasty. Clin Orthop Relat Res 435:171–180
Robertsson O, Borgguist L, Knutson K, Lewold S, Lidgren L (1999) Use of unicompartmental instead of tricompartmental prostheses for unicompartmental arthrosis in the knee is a cost-effective alternative. 15,437 primary tricompartmental prostheses were compared with 10,624 primary medial or lateral unicompartmental prostheses. Acta Orthop Scand 70:170–175
Robertsson O, Knutson K, Lewold S, Lidgren L (2001) The Swedish Knee Arthroplasty Register 1975–1997: an update with special emphasis on 41,223 knees operated on in 1988–1997. Acta Orthop Scand 72:503–513
Robertsson O, Lidgren L (2008) The short-term results of 3 common UKA implants during different periods in Sweden. J Arthroplasty 23:801–807
Saenz CL, McGrath MS, Marker DR, Seyler TM, Mont MA, Bonutti PM (2010) Early failure of a unicompartmental knee arthroplasty design with an all-polyethylene tibial component. Knee 17:53–56
Saldanha KA, Keys GW, Svard UC, White SH, Rao C (2007) Revision of Oxford medial unicompartmental knee arthroplasty to total knee arthroplasty: results of a multicentre study. Knee 14:275–279
Sathasivam S, Walker PS, Campbell PA, Rayner K (2001) The effect of contact area on wear in relation to fixed bearing and mobile bearing knee replacements. J Biomed Mater Res 58:282–290
Schallberger A, Jacobi M, Wahl P, Maestretti G, Jakob RP (2011) High tibial valgus osteotomy in unicompartmental medial osteoarthritis of the knee: a retrospective follow-up study over 13–21 years. Knee Surg Sports Traumatol Arthrosc 19:122–127
Smith TO, Hing CB, Davies L, Donell ST (2009) Fixed versus mobile bearing unicompartmental knee replacement: a meta-analysis. Orthop Traumatol Surg Res 95:599–605
Soohoo NF, Sharifi H, Kominski G, Lieberman JR (2006) Cost-effectiveness analysis of unicompartmental knee arthroplasty as an alternative to total knee arthroplasty for unicompartmental osteoarthritis. J Bone Joint Surg Am 88:1975–1982
Sun PF, Jia YH (2012) Mobile bearing UKA compared to fixed bearing TKA: a randomized prospective study. Knee 19:103–106
W-Dahl A, Robertsson O, Lidgren L, Miller L, Davidson D, Graves S (2010) Unicompartmental knee arthroplasty in patients aged less than 65. Acta Orthop 81:90–94
Whittaker JP, Naudie DD, McAuley JP, McCalden RW, MacDonald SJ, Bourne RB (2010) Does bearing design influence midterm survivorship of unicompartmental arthroplasty? Clin Orthop Relat Res 468:73–81
Wright JG, Swiontkowski MF, Heckman JD (2003) Introducing levels of evidence to the journal. J Bone Joint Surg Am 85:1–3
Conflict of interest
No benefits or funds were received in support of the study.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Cheng, T., Chen, D., Zhu, C. et al. Fixed- versus mobile-bearing unicondylar knee arthroplasty: are failure modes different?. Knee Surg Sports Traumatol Arthrosc 21, 2433–2441 (2013). https://doi.org/10.1007/s00167-012-2208-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00167-012-2208-y