
Abstract
Purpose
To determine the prevalence of DSM-IV psychiatric disorders in a representative sample of children and adolescents living in Santiago, Chile, as part of a national sample.
Method
Subjects aged 4–18 were selected using a stratified multistage design. First, ten municipalities/comunas of Santiago were selected; then the blocks, homes, and child or adolescent to be interviewed were chosen. Psychology graduate students administered the Spanish-language, computer-assisted version of DISC-IV that estimated DSM-IV 12-month prevalence.
Results
A total of 792 children and adolescents were evaluated, with a participation rate of 76.7%. The most stringent impairment DSM-IV DISC algorithm for psychiatric disorders revealed a prevalence of 25.4% (20.7% for boys and 30.3% for girls). The majority of the diagnoses corresponded to anxiety and affective disorders. Prevalence was higher in children aged 4–11 (31.9%) than in adolescents aged 12–18 (18.2%). This difference was mainly accounted for by disruptive disorders in the younger age group. Anxiety disorders had the highest prevalence, although impairment was low. In contrast, most children and adolescents with affective disorders were impaired.
Conclusions
In Santiago, the prevalence of psychiatric disorders in children and adolescents was high. This study helps raise awareness of child and adolescent mental health issues in Spanish-speaking Latin America and serves as a basis for improving mental health services.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Introduction
The purpose of this study was to determine the prevalence of psychiatric disorders in a representative sample of children and adolescents from a Chilean population. This initial report presents the prevalence of disorders found in the capital city of Santiago, where 54.5% of the nation’s children and adolescents reside (N = 1,150,270). The complete survey, once all data are available, will include Santiago, one city in northern Chile, and two cities in southern Chile. These cities were selected using socioeconomic, ethnic, and demographic criteria; the same cities were used for a previous epidemiological study of the adult population [1].
The World Health Organization (WHO) has stated that psychiatric disorders with onset in childhood and adolescence should be a matter of concern in terms of public health. In the USA, the Epidemiological Catchment Area Survey of adult populations retrospectively showed that the age of onset for core psychiatric disorders was earlier than formerly believed [2]. The National Comorbidity Survey-Replication study recently confirmed these findings [3].
Prospective follow-up studies of cohorts of children born in the 1960s have identified two groups of disorders: those with onset in childhood and those with onset in adolescence [4, 5]. Even so, prevalence data on children and adolescent mental health remain limited. Indeed, the mental health needs of children and adolescents are not fully met, even in developed countries [6, 7], and research in child and adolescent psychiatry is grossly underfunded. Other studies have shown that biological and psychosocial factors in childhood increase the risk of later medical and psychiatric disorders [8–10]. Despite the demonstrated efficacy of many interventions used for child and adolescent psychiatric disorders and evidence-based measures for prevention and the promotion of a healthy environment, many children do not receive the necessary services. The chance of receiving specialized care for depression is 14 times greater in adults than in children. Eighty-nine percent of mental health spending in the USA goes to adults [11].
The WHO emphasizes that the first step in mental health planning is the collection of relevant information. The Atlas Project of Mental Health Resources was developed to address this deficit, and its findings confirmed a paucity of available information on child and adolescent mental health, especially in the developing world. All the data collected showed a significant gap in resources between children and adults [12, 13].
A meta-analysis of 52 studies done using standardized interviews between 1980 and 1996 found child and adolescent prevalence rates ranging from 1 to 51%, depending on the instrument used to measure psychiatric disorders: Rutter’s criteria yielded 12% prevalence, the Schedule for Affective Disorders and Schizophrenia for Children (K-SADS) 14%, and the Diagnostic Interview Schedule for Children (DISC) 20–25% [11, 14]. Caveats in these earlier studies included problems with sampling, case definitions, data analysis, and presentation [14]. Since 1990, impairment criteria have been included in prevalence studies such as the Quebec Child Mental Health Survey (using DISC and both parents and teachers as informants) [15] and the Great Smoky Mountains Study [16] (using the Child and Adolescent Psychiatric Assessment, or CAPA, interview and the Children’s Global Assessment Scale, or C-GAS, as a measure of impairment) [17]. Three reviews of studies done in the past four decades found prevalence rates of 5–22% for psychiatric disorders among children and adolescents [7, 11, 14].
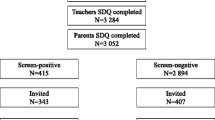
Table 1 summarizes selected psychiatric epidemiological studies conducted in the past decade, including the few carried out in South America. Most studies reported in the literature were based on four instruments: Developmental and Well-Being Assessment (DAWBA) [18], CAPA [19], DISC [20], and the Composite Diagnostic Interview (CIDI-A), which has been used more recently among adolescents [21]. Many of these diagnostic studies relied on a two-stage design with a screening instrument, and only a small sample (all the positives and a percentage of the negatives) received a diagnostic interview. The informants also varied across studies, as did the impairment criteria and sampling design. Given these methodological differences, caution should be exercised when interpreting differences between cross-national studies.
In an earlier study done in Santiago, Chile, child psychiatry fellows applied non-standardized, semi-structured, clinical interviews to schoolchildren (N = 372 from 1597) in grades 1 and 6 utilizing ICD-10 criteria [22]. This study used a two-phase design and found an overall prevalence rate of 45.7% for psychiatric disorders, a rate that fell to 15.7% when impairment criteria were considered. A preliminary report based on the first study site (Cautin, n = 254) of our national survey found a DSM-IV prevalence of 28.1% using the DISC-IV, with impairment of 16.8% [23].
Information on the prevalence of child and adolescent mental health in South America is clearly lacking. The present study is the first carried out in a Spanish-speaking country of Latin America south of Mexico to use standardized diagnostic instruments, and even the Mexican study that did so was limited to adolescents [24]. In Latin America, community-based methods rather than school-based studies are needed. In this region, relying on school-based sampling rather than household sampling may omit many of the most vulnerable children, who might not attend school even though it is compulsory.
The objective of this study was to provide data that would be useful for addressing the mental health service needs of children in Chile. This study also helps raise awareness of child and adolescent mental health issues in Spanish-speaking South America.
Methods
Participants
The sample was representative of children aged 4–18 in Santiago, Chile, in the Metropolitan Region. The target sample size was determined based on the probability of obtaining a sample with a prevalence of psychiatric disorders of 18%, according to the DISC-IV study from Puerto Rico, with a 95% confidence interval and maximum standard error of 1.75 [25].
In Santiago, ten municipalities/comunas (of a total of 32) were selected to represent the range of socioeconomic levels in the region. Within each municipality, random blocks were identified and the number of households on each block was counted. Based on the 2002 census, 12 homes were selected per block and five were surveyed. Homes were designated starting with the northeast corner and moving in a counterclockwise direction. The child or adolescent whose birth date was closest to the interview date was selected for the study. In the event of a tie (i.e., if more than one child had the same birth date), a coin was tossed and, in the event of more than one tie, a Kish table was used. The targeted sample was 1,008 subjects, representative of the 1,150,270 individuals aged 4–18 residing in the city of Santiago, according to the age and gender distribution of the 2002 census. Of these, 792 participated in the study.
Instruments
Psychiatric disorders were measured using the Spanish-language computer-assisted version of DISC-IV [20, 26], which had been previously adapted and validated for Chile [27]. The parent version was administered to primary caretakers of children aged 4–11. Adolescents aged 12 and older were interviewed directly using the youth version of the DISC-IV. Psychology graduate students trained in the use of the instrument conducted the interviews in the home. The psychiatric disorders selected for evaluation were: social phobia, separation anxiety disorder (SAD), generalized anxiety disorder (GAD), eating disorder, major depressive disorder (MDD), schizophrenia, attention-deficit hyperactivity disorder (ADHD), oppositional-defiant disorder (ODD), conduct disorder, alcohol use disorders, marijuana use disorders, nicotine dependence, and other substance use disorders.
The four algorithms contained in the DISC-IV interview ascertained impairment according to the extent to which symptoms in six domains had stressed the child or affected his or her school achievement or relationships with caretakers, family, friends, or teachers. For impairment criterion A, at least one of the impairments must be rated intermediate or severe (sometimes or many times; bad or very bad); for criterion B, at least two impairments must be rated intermediate or severe; for criterion C, at least one impairment must fall within the severe category; and criterion D was determined by the presence of either criterion B or C (i.e., at least two intermediate or one severe rating). Herein, criterion D was used as the measure of impairment.
Upon completion, the research team reviewed each interview independently, and discrepancies were discussed with the interviewers to obtain clarification or corrections. The field coordinator verified interviews with respondents by telephone. A smaller sample of respondents was revisited. Refusals were telephoned or visited by the field coordinator in an attempt to encourage participation. If rejected a second time, a senior member of the research team visited them before they were classified as a true refusals. Homes refusing participation were not replaced; replacements were only used for those homes in which no child or adolescent resided.
Statistical analysis
Data not obtained using the DISC computer-assisted version were entered in an SPSS database, using double digitation for error control. DISC-IV yields 12-month DSM-IV diagnoses. Estimates of prevalence rates and the corresponding standard errors were obtained using STATA 11.0 to take into account the complex sample design. First-order Taylor series linearization was used to calculate odds ratios, 95% confidence intervals, and p values.
Samples were weighted for selection probabilities at each stage of the sampling: municipality, block, home, and child. In addition, a post-stratification adjustment for gender and age ensured that the data analysis was based on the population from the 2002 census.
Written informed consent was obtained from the adults responsible for each child. To assure confidentiality, the data analysis team did not have access to any identifying information. The adult responsible for each child and the adolescent participants were offered the opportunity to receive their diagnostic results based on the DISC-IV via certified letter. Treatment in the local mental health network was recommended for cases of identified disorders. Unfortunately, treatment was not guaranteed, as it depended on the caretaker’s or the adolescent’s behavior and the availability of mental health resources. The ethical research committees of the University of Concepcion and the funding institution approved the study.
Results
The final sample (n = 792) was representative of the ten selected municipalities. The overall response rate was 77.6%. This rate was somewhat lower in the two municipalities with the highest socioeconomic levels.
The 12-month prevalence rate of psychiatric disorders without adjusting for impairment in children and adolescents (aged 4–18) was 42.4%. The prevalence rate dropped to 25.4% when impairment was considered. Prevalence was higher in girls than boys, with or without impairment. This difference was accounted for by anxiety and affective disorders (Tables 2, 3). Although higher in girls, disruptive disorders showed no statistically significant gender difference. Prevalence was higher in children (aged 4–11) than adolescents (aged 12–18). These differences were primarily due to disruptive disorders. Substance use disorders were present only among adolescents.
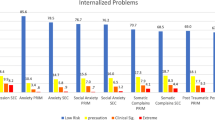
Prevalence rates for anxiety disorders were 20% (unadjusted) and 9% (adjusted for impairment). Anxiety disorders were more frequent in girls. More specifically, girls had higher prevalence rates for social phobia [excluding impairment: OR = 3.7, 95% (1.6, 8.6); including impairment: OR = 5.7, 95% (1.9, 17.6)], SAD [excluding impairment: OR = 2.7, 95% (1.6, 4.6); including impairment: OR = 2.5, 95% (1.2, 5.4)], and GAD including impairment: OR = 5.6, 95% CI (1.3, 23.8)] but not for GAD excluding impairment. The most prevalent anxiety disorder among children was SAD, whereas GAD was the most prevalent in adolescents. There was no statistically significant difference in rates of anxiety disorders between the two age groups.
The prevalence of any affective disorder was slightly reduced (from 6.5 to 5.4%) when considering impairment criteria. Most affective disorder diagnoses were due to MDD, whereas rates for dysthymia were very low and not associated with impairment. MDD was more frequent in girls at all ages [excluding impairment: OR = 2.9, 95% (1.1, 8.0)], but not statistically significant when impairment was taken into account. MDD was significantly more prevalent in adolescents than in children when impairment was excluded [OR = 2.6, 95% (1.2, 5.9)], but this was not appreciable when impairment was included.
The population showed a very high prevalence of any disruptive disorder: 26.0% without impairment and 17.9% with impairment. Among the disruptive disorders, ADHD was the most prevalent (12.6%), followed by ODD (6.4%) and conduct disorder (2.5%) when using impairment criteria. For both ADHD and ODD, prevalence rates were higher in girls, whereas conduct disorder was more prevalent in boys; however, none of these differences were statistically significant. According to the age distribution, prevalence rates for ADHD [excluding impairment: OR = 0.2, 95% CI (0.1, 0.4); including impairment: OR = 0.3, 95% (0.1, 0.6)] and ODD were lower in adolescents than in children [excluding impairment: OR = 0.4, 95% CI (0.2, 0.9); including impairment: OR = 0.3, 95% CI (0.1, 0.6)]. When not considering impairment, conduct disorder was significantly more prevalent in adolescents [OR = 5.0, 95% CI (2.4, 10.6)].
Substance use disorders were found in 5.1% of the population and in 1.5% with impairment. No cases of substance abuse or dependence were found among children. The most abused substance was alcohol (1.8% without and 0.5% with impairment). Cannabis abuse appeared only in the adolescent group when impairment criteria were not considered (Table 4).
Table 3 provides the odds ratios and confidence intervals of the demographic correlates for anxiety, affective, and substance use disorders by age, gender, and socioeconomic status (SES). In Chile, SES is traditionally stratified into five groups based on family income: group 1 represents the 20% of the population living under the poverty line and group 5 the wealthiest 20% of the population. Only anxiety disorders showed a statistically significant (inverse) relationship with SES. Substance use disorders were less common among those in the lowest SES groups.
Discussion
Structured, internationally validated instruments for child and adolescent psychiatric epidemiology using established methodology have now been used in four countries or territories of Latin America and the Caribbean. Although comparisons across countries should be interpreted with caution, Santiago, Chile, has one of the highest reported rates of child and adolescent disorders. Nearly all the DAWBA studies used a two-stage procedure with several caveats: it may have been overly selective, it already incorporated severity criteria and required appraisal by a clinician, and it combined information from more than one informant. The CAPA and Mexico City CIDI-A studies incorporated severity criteria, and their rates were consistent with the impaired rates in Chile. When compared with other DISC studies, the rates for Santiago appeared to be elevated.
Using the impairment algorithm of the DISC-IV, the prevalence rate for disorders in Santiago was reduced by 40% (from 42.4 to 25.4%). Canino suggested considering an external measure of impairment such as the C-GAS rather than relying exclusively on the DISC impairment measures, which are specific for each diagnosis. An external measure of impairment permits identifying children who may be impaired but do not have a diagnosis [25].
Interestingly, the high rates found in Santiago were not observed in Cautin, southern Chile, the other site where the national survey was completed [24]. In Cautin, the total rate for DSM-IV disorders was 28.1%; this also decreased by 40% when impairment criteria were applied. It should be noted that the rates obtained in Santiago may be accurate, as our results for children closely coincide with an earlier school-based study limited to children [22].
Similar to more recent psychiatric epidemiological studies that included adolescent groups [24, 67], we relied only on the adolescent respondent. The high rates obtained in Santiago raise an interesting issue not fully addressed in the literature: would incorporating a parent interview improve diagnostic reliability or inhibited responses given by the adolescents?
Upon examining specific diagnoses in Santiago, ADHD was the most prevalent disorder among children. However, in Cautin, SAD was the most prevalent disorder observed. The ADHD rates were higher than expected in Santiago (12.6% with impairment) considering that a review of the world prevalence indicated a rate of 5.3%. However, reported ADHD rates vary greatly [28]. In general, ADHD rates in South America do not differ statistically from those in North America or Europe, and the high rates of ADHD in Santiago should be explored further.
Although powerful arguments have been made for the role of SES in childhood behavioral problems [29, 30], such findings were not robust in the Santiago study. A number of studies published since 2000 have found a relationship between overall psychopathology in children or adolescents and parental income [31, 32], whereas a few studies have found no association [25, 33]. However, a weak association with family income was also noted earlier in the Ontario Child Health Study, which only found correlations among selected disorders [34]. Since 2000, several studies have noted a relationship only with internalizing disorders or anxiety disorders, as occurred in Santiago [35–39]. However, earlier studies reported stronger associations for externalizing rather than internalizing disorders [34, 38]. Interestingly, the Mexican CIDI-A study found only an association with substance misuse (lower rates in the lowest income group), a finding also noted in Santiago [24]. Environment-related stressors have been found to partially mediate associations between mental health problems and SES [39]. This paper limited the examination of SES to family income; however, other measure of SES should be considered as well.
In Santiago, girls were found to have higher rates of nearly all disorders for which statistical differences were noted. Although not statistically significant, girls in Santiago were found to have higher rates of ADHD (a ratio of 1.3:1) and ODD (1.4:1). ADHD and externalizing disorders in general are almost universally higher in boys [40, 41]. In Cautin, girls had rates of 3.2% compared with 6.7% in boys [23]. Interestingly, the Mexican CIDI-A study [24] and a Brazilian ADHD school-based investigation [42] reported higher, although not statistically significant, rates for impulse control disorders (including ADHD) among girls. A prevalence study of ADHD in Venezuela of 1141 school children also reported higher rates among girls [43]. However, two Colombian school-based studies found higher rates in boys [44, 45]. The reasons behind the elevated ADHD rates in girls or nearly equal rates with boys found in a number of Latin American epidemiological studies merit further research.
Child and adolescent psychiatric epidemiology is still evolving in Latin America. Research from a number of countries, including Chile, is beginning to produce data that call attention to the need to better address childhood mental health issues in the region. This is particularly an issue in Santiago, which has high rates of child and adolescent mental health disorders.
References
Vicente B, Kohn R, Rioseco S, Saldivia S, Levav I, Torres S (2006) Lifetime and 12-month prevalence of DSM-III-R disorders in the Chile psychiatric prevalence study. Am J Psychiatry 163(8):1362–1370
Burke KC, Burke JD Jr, Regier DA, Rae DS (1990) Age at onset of selected mental disorders in 5 community populations. Arch Gen Psychiatry 47(6):511–518
Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE (2005) Lifetime prevalence and age of onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry 62(6):593–602
Rutter M, Sroufe LA (2000) Developmental psychopathology: concepts and challenges. Dev Psychopathol 12(3):265–296
Costello E, Foley DL, Angold A (2006) 10-year research update review: the epidemiology of child and adolescent psychiatric disorders: II. developmental epidemiology. J Am Acad Child Adolesc Psychiatry 45(1):8–25
Leckman JF, Leventhal BL (2008) Editorial: a global perspective on child and adolescent mental health. J Child Psychol Psychiatr 49(3):221–225
Patel V, Flischer AJ, Hetrick S, McGorry P (2007) Mental health of young people: a global public health challenge. Lancet 369(9569):1302–1313
Barker DJ (2003) The developmental origins of adult disease. Eur J Epidemiol 18(8):733–736
Mäntymaa M, Puura K, Luoma I, Salmelin R, Davis H, Tsiantis J, Ispanovic-Radojkovic V, Paradisiotou A, Tamminen T (2003) Infant-mother interaction as a predictor of child′s chronic health problems. Child Care Health Dev 29(3):181–191
Brown AS, Sussex ES (2002) In utero infection and adult schizophrenia. Ment Retard Dev Disabil Res Rev 8(1):51–57
O’Connell ME, Boat T, Warner KE (eds) (2009) Preventing mental, emotional, and behavioral disorders among young people: progress and possibilities. The National Academies Press, Washington, DC, pp 191–220
World Health Organization (2005) Atlas child and adolescent mental health resources global concerns: implications for the future. World Health Organization, Geneva
Belfer ML (2008) Child and adolescent mental disorders: the magnitude of the problem across the globe. J Child Psychol Psychiatr 49(3):226–236
Roberts RE, Attkinson CC, Rosenblatt A (1998) Prevalence of psychopathology among children and adolescents. Am J Psychiatry 155(6):715–725
Breton J, Bergeron L, Valla JP, Berthiaume C, Gaudet N, Lambert J, St-Georges M, Houde L, Lépine S (1999) Quebec child mental health survey: prevalence of DSM-II-R mental health disorders. J Child Psychol Psychiat 40(3):375–384
Costello EJ, Angold A, Burns BJ, Stangl DK, Tweed DL, Erkanli A, Worthman CM (1996) The Great Smoky Mountains Study of Youth: goals, design, methods and the prevalence of DSM-III-R disorders. Arch Gen Psychiatry 53(12):1129–1136
Shaffer D, Gould MS, Brasic J, Ambrosini PJ, Fisher PW, Bird HR, Aluwahlia S (1983) A children’s global assessment scale (CGAS). Arch Gen Psychiatry 40(11):1228–1231
Goodman R, Ford T, Richards H, Meltzer H, Gatward R (2000) The development and well-being assessment: description and initial validation of an integrated assessment of child and adolescent psychopathology. J Child Psychol Psychiatry 41(5):645–657
Angold A, Prendergast M, Cox A, Harrington R, Simonoff E, Rutter M (1995) The Child and Adolescent Psychiatric Assessment (CAPA). Psychol Med 25(4):739–753
Shaffer D, Fischer P, Lucas CP, Dulcan MK, Schwab-Stone ME (2000) NIMH Diagnostic Interview Schedule for Children Version IV (NIMH DISC-IV): description, differences from previous versions, and reliability of some common diagnoses. J Am Acad Child Adolesc Psychiatry 39(1):28–38
Merikangas K, Avenevoli S, Costello J, Koretz D, Kessler RC (2009) National comorbidity survey replication adolescent supplement (NCS-A): I. Background and measures. J Am Acad Child Adolesc Psychiatry 48(4):367–369
de la Barra F, Toledo V, Rodríguez J (2004) Estudio de salud mental en dos cohortes de niños escolares de Santiago Occidente. IV: desórdenes psiquiátricos, diagnóstico psicosocial y discapacidad. Rev Chil Neuro-Psiquiat 42(4):259–272
Vicente B, Saldivia S, Rioseco P, de la Barra F, Valdivia M, Melipillan R, Zùñiga M, Escobar B, Pihan R (2010) Epidemiología de trastornos mentales infanto-juveniles en la Provincia de Cautín. Rev Med Chile 138:965–973
Benjet C, Borges G, Medina-Mora ME, Zambrano J, Aguilar-Gaxiola S (2009) Youth mental health in a populous city of the developing world: results from the Mexican Adolescent Mental Health Survey. J Child Psychol Psychiatry 50(4):386–395
Canino G, Shrout P, Rubio-Stipec M, Bird HR, Bravo M, Ramirez R, Chavez L, Alegria M, Bauermeister JJ, Hohmann A, Ribera J, Garcia P, Martinez-Taboas A (2004) The DSM-IV rates of child and adolescent disorders in Puerto Rico: prevalence, correlates, service use, and the effects of impairment. Arch Gen Psychiatry 61(1):85–93
Bravo M, Ribera J, Rubio-Stipeck M, Rubio-Stipec M, Canino G, Shrout P, Ramírez R, Fábregas L, Chavez L, Alegría M, Bauermeister JJ, Martínez Taboas A (2001) Test-retest reliability of the Spanish version of the Diagnostic Interview Schedule for Children (DISC-IV). J Abnorm Child Psychol 29(5):433–444
Saldivia S, Vicente B, Valdivia M, Zúñiga M, Llorente C, Condeza MI (2008) Validación de la entrevista diagnóstica estructurada DISC-IV para la identificación de trastornos psicopatológicos en niños y adolescentes chilenos. Rev Chil Neuro-Psiquiat 62:86
Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 164(6):942–948
Leventhal T, Brooks-Gunn J (2000) The neighborhoods they live in: the effects of neighborhood residence on child and adolescent outcomes. Psychol Bull 126(2):309–337
Ayer L, Hudziak JJ (2009) Socioeconomic risk for psychopathology: the search for causal mechanisms. J Am Acad Child Adolesc Psychiatry 48(10):982–983
Costello EJ, Angold A, Burns BJ, Erkanli A, Stangl DK, Tweed DL (1996) The Great Smoky Mountains Study of Youth. Functional impairment and serious emotional disturbance. Arch Gen Psychiatry 53(12):1137–1143
Vostanis P, Graves A, Meltzer H, Goodman R, Jenkins R, Brugha T (2006) Relationship between parental psychopathology, parenting strategies and child mental health—findings from the GB national study. Soc Psychiatry Psychiatr Epidemiol 41(7):509–514
Goodman R, Slobodskaya H, Knyazev G (2005) Russian child mental health: a cross-sectional study of prevalence and risk factors. Eur Child Adolesc Psychiatry 14(1):28–33
Lipman EL, Offord DR, Boyle MH (1996) What if we could eliminate child poverty? The theoretical effect on child psychosocial morbidity. Soc Psychiatry Psychiatr Epidemiol 31(5):303–307
Carter AS, Wagmiller RJ, Gray SA, McCarthy KJ, Horwitz SM, Briggs-Gowan MJ (2010) Prevalence of DSM-IV disorder in a representative, healthy birth cohort at school entry: sociodemographic risks and social adaptation. J Am Acad Child Adolesc Psychiatry 49(7):686–698
Roberts RE, Roberts CR, Xing Y (2007) Rates of DSM-IV psychiatric disorders among adolescents in a large metropolitan area. J Psychiatr Res 41(11):959–967
Farbstein I, Mansbach-Kleinfeld I, Levinson D, Goodman R, Levav I, Vograft I, Kanaaneh R, Ponizovsky AM, Brent DA, Apter A (2010) Prevalence and correlates of mental disorders in Israeli adolescents: results from a national mental health survey. J Child Psychol Psychiatry 51(5):630–639
McLoyd VC (1998) Socioeconomic disadvantage and child development. Am Psychol 53(2):185–204
Amone-P’Olak K, Ormel J, Huisman M, Verhulst FC, Oldehinkel AJ, Burger H (2009) Life stressors as mediators of the relation between socioeconomic position and mental health problems in early adolescence: the TRAILS study. J Am Acad Child Adolesc Psychiatry 48(10):1031–1038
Polanczyk G, Rohde LA (2007) Epidemiology of attention-deficit/hyperactivity disorder across the lifespan. Curr Opin Psychiatry 20(4):386–392
Skounti M, Philalithis A, Galanakis E (2007) Variations in prevalence of attention deficit hyperactivity disorder worldwide. Eur J Pediatr 166(2):117–123
Rohde LA, Biederman J, Busnello EA, Zimmermann H, Schmitz M, Martins S, Tramontina S (1999) ADHD in a school sample of Brazilian adolescents: a study of prevalence, comorbid conditions, and impairments. J Am Acad Child Adolesc Psychiatry 38(6):716–722
Montiel-Nava C, Peña JA, López M, Salas M, Zurga JR, Montiel-Barbero I, Pirela D, Cardozo JJ (2002) Estimations of the prevalence of attention deficit hyperactivity disorder in Marabino children. Rev Neurol 35(11):1019–1024
Cornejo JW, Osío O, Sánchez Y, Carrizosa J, Sánchez G, Grisales H, Castillo-Parra H, Holguín J (2005) Prevalence of attention deficit hyperactivity disorder in Colombian children and teenagers. Rev Neurol 40(12):716–722
Pineda D, Ardila A, Rosselli M, Arias BE, Henao GC, Gomez LF, Mejia SE, Miranda ML (1999) Prevalence of attention-deficit/hyperactivity disorder symptoms in 4- to 17-year-old children in the general population. J Abnorm Child Psychol 27(6):455–462
Ford T, Goodman R, Meltzer H (2003) The British Child and Adolescent Mental Health Survey 1999: the prevalence of DSM-IV disorders. J Am Acad Child Adolesc Psychiatry 42(10):1203–1211
Fleitlich-Bilyk B, Goodman R (2004) Prevalence of child and adolescent psychiatric disorders in southern Brazil. J Am Acad Child Adolesc Psychiatry 43(6):727–734
Goodman R, Neves dos Santos D, Robatto Nunes AP, Pereira de Miranda D, Fleitlich-Bilyk B, Almeida Filho N (2005) The Ilha de Maré study: a survey of child mental health problems in a predominantly African-Brazilian rural community. Soc Psychiatry Psychiatr Epidemiol 40(1):11–17
Mullick MS, Goodman R (2005) The prevalence of psychiatric disorders among 5–10 year olds in rural, urban and slum areas in Bangladesh: an exploratory study. Soc Psychiatry Psychiatr Epidemiol 40(8):663–671
Heiervang E, Stormark KM, Lundervold AJ, Heimann M, Goodman R, Posserud MB, Ullebø AK, Plessen KJ, Bjelland I, Lie SA, Gillberg C (2007) Psychiatric disorders in Norwegian 8- to 10-year-olds: an epidemiological survey of prevalence, risk factors, and service use. J Am Acad Child Adolesc Psychiatry 46(4):438–447
Pillai A, Patel V, Cardozo P, Goodman R, Weiss HA, Andrew G (2008) Non-traditional lifestyles and prevalence of mental disorders in adolescents in Goa, India. Br J Psychiatry 192(1):45–51
Alyahri A, Goodman R (2008) The prevalence of DSM-IV psychiatric disorders among 7–10 year old Yemeni schoolchildren. Soc Psychiatry Psychiatr Epidemiol 43(3):224–230
Frigerio A, Rucci P, Goodman R, Ammaniti M, Carlet O, Cavolina P, De Girolamo G, Lenti C, Lucarelli L, Mani E, Martinuzzi A, Micali N, Milone A, Morosini P, Muratori F, Nardocci F, Pastore V, Polidori G, Tullini A, Vanzin L, Villa L, Walder M, Zuddas A, Molteni M (2009) Prevalence and correlates of mental disorders among adolescents in Italy: the PrISMA study. Eur Child Adolesc Psychiatry 18(4):217–226
Anselmi L, Fleitlich-Bilyk B, Menezes AM, Araújo CL, Rohde LA (2010) Prevalence of psychiatric disorders in a Brazilian birth cohort of 11-year-olds. Soc Psychiatry Psychiatr Epidemiol 45(1):135–142
Wacharasindhu A, Panyyayong B (2002) Psychiatric disorders in Thai school-aged children: I Prevalence. J Med Assoc Thai 85(Suppl 1):S125–S136
Angold A, Erkanli A, Farmer EM, Fairbank JA, Burns BJ, Keeler G, Costello EJ (2002) Psychiatric disorder, impairment, and service use in rural African American and white youth. Arch Gen Psychiatry 59(10):893–901
Costello EJ, Mustillo S, Erkanli A, Keeler G, Angold A (2003) Prevalence and development of psychiatric disorders in childhood and adolescence. Arch Gen Psychiatry 60(8):837–844
McKelvey RS, Sang DL, Baldassar L, Davies L, Roberts L, Cutler N (2002) The prevalence of psychiatric disorders among Vietnamese children and adolescents. Med J Aust 177(8):413–417
Srinath S, Girimaji SC, Gururaj G, Seshadri S, Subbakrishna DK, Bhola P, Kumar N (2005) Epidemiological study of child & adolescent psychiatric disorders in urban & rural areas of Bangalore, India. Indian J Med Res 122(1):67–79
Roberts RE, Roberts CR, Xing Y (2006) Prevalence of youth-reported DSM-IV psychiatric disorders among African, European, and Mexican American adolescents. J Am Acad Child Adolesc Psychiatry 45(11):1329–1337
Leung PW, Hung SF, Ho TP, Lee CC, Liu WS, Tang CP, Kwong ST (2008) Prevalence of DSM-IV disorders in Chinese adolescents and the effects of an impairment criterion: a pilot community study in Hong Kong. Eur Child Adolesc Psychiatry 17(7):452–461
Merikangas KR, He JP, Brody D, Fisher PW, Bourdon K, Koretz DS (2010) Prevalence and treatment of mental disorders among US children in the 2001–2004 NHANES. Pediatrics 125(1):75–81
Kroes M, Kalff AC, Kessels AG, Steyaert J, Feron FJ, van Someren AJ, Hurks PP, Hendriksen JG, van Zeben TM, Rozendaal N, Crolla IF, Troost J, Jolles J, Vles JS (2001) Child psychiatric diagnoses in a population of Dutch school children aged 6 to 8 years. J Am Acad Child Adolesc Psychiatry 40(12):1401–1409
Gau SS, Chong MY, Chen TH, Cheng A (2005) A 3-year panel study of mental disorders among adolescents in Taiwan. Am J Psychiatry 162(7):1344–1350
Eapen V, Jakka ME, Abou-Saleh MT (2003) Children with psychiatric disorders: the Al Ain Community Psychiatric Survey. Can J Psychiatry 48(6):402–407
Petersen DJ, Bilenberg N, Hoerder K, Gillberg C (2006) The population prevalence of child psychiatric disorders in Danish 8- to 9-year-old children. Eur Child Adolesc Psychiatry 15(2):71–78
Merikangas KR, He JP, Burstein M, Swanson SA, Avenevoli S, Cui L, Benjet C, Georgiades K, Swendsen J (2010) Lifetime prevalence of mental disorders in U.S. adolescents: results from the National Comorbidity Survey Replication-Adolescent Supplement (NCS-A). J Am Acad Child Adolesc Psychiatry 49(10):980–989
Acknowledgments
This study was funded by the National Science and Technology Research Fund (FONDECYT), Grant No. 1070519.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Vicente, B., de la Barra, F., Saldivia, S. et al. Prevalence of child and adolescent psychiatric disorders in Santiago, Chile: a community epidemiological study. Soc Psychiatry Psychiatr Epidemiol 47, 1099–1109 (2012). https://doi.org/10.1007/s00127-011-0415-3
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00127-011-0415-3