
Abstract
This study was designed to assess the prevalence of psychiatric disorders and the impact of impairment criteria on rates of diagnoses in a representative sample of elementary school children from a country in a region. We sampled 419 primary school children by using a one-stage design in Izmir, Turkey. The response rate was 99.5 % and 417 cases were assessed using the Schedule for Affective Disorders and Schizophrenia for School-Age Children Present and Lifetime Version and a scale to assess the impairment criterion. The results showed that 36.7 % of the sample met DSM-IV criteria independent of impairment and that 14.1 % of the population had one or more DSM-IV disorders when a measure of impairment specific to each diagnosis was considered. The most prevalent disorders were attention-deficit/hyperactivity disorder and anxiety disorders. This study provided the first estimates of the prevalence of specific DSM-IV-defined psychiatric disorders in Turkish population of children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Childhood is a period in which profound changes occur in physical, social and cognitive development. Additionally, this is a time period in which mental disorders first develop. Psychiatric disorder during the childhood period can disrupt a young person’s normal development. The prevention, detection, and treatment of these problems are important not only to relieve current distress but also to improve adult functioning and prevent the perpetuation of disadvantage into the next generation [1]. Epidemiologic data are essential for planning health services and implementing strategies of detection and early intervention, with substantial possible benefits for public health [2]. In the literature, childhood psychiatric disorders are estimated at prevalence rates ranging from 10 to 20 % [3]. Variations in estimated prevalence may be explained, in part, by the varying reasons the studies were conducted—for example, developmental perspectives, patterns of symptoms, and studies of prevalence—and by the purposes for which their estimates were to be used. The methodology of study populations has also differed among such studies. Studies have applied several diagnoses of disorders obtained from numerous reports and measures. They have incorporated variations of reports based on structured interviews from different informants and data combining two or more sources. Moreover, their use of the term “functional impairment” also has varied [4]. In previous studies [5–9], it has been reported that the application of an impairment criterion leads to a reduction of prevalence estimates. In China, using the impairment algorithm of the Diagnostic Interview Schedule for Children, Version IV (DISC-IV), the prevalence rate for disorders was reduced by 57 % (from 38.4 to 16.4 %) [8]. A recent study in Chile reported the 12-month prevalence rate of psychiatric disorders was 38.3 % without impairment and 22.5 % when impairment was taken into account in a stratified household sample representative of the country’s children aged 4–18 [9]. Additionally, Vicente et al. [10] reported that the prevalence rate for disorders in Santiago was reduced by 40 % (from 42.4 to 25.4 %) upon adding an impairment criterion. Another study by Roberts et al. [11] reported the prevalence estimates of DSM-IV disorders in youths aged 11–17 years from households enrolled in large health maintenance organizations as 17.1 % when not considering impairment, 11 % when considering only DISC impairment and 5.3 % when only using the Child Global Assessment Scale (CGAS).
To our knowledge, the prevalence of childhood psychiatric disorders has not previously been extensively studied in investigations in Turkey or neighboring countries, such as Greece and Iran, but there are many studies employing questionnaires—e.g., the Child Behavior Checklist (CBCL), Teacher Report Form (TRF) and Achenbach’s Child Behavior Checklist (ACBC) [12–16]. Despite their well-established psychometric properties, these questionnaires are not diagnostic tools, and their results do not necessarily map onto formal psychiatric diagnoses. The few studies that have provided a diagnosis have only examined attention-deficit/hyperactivity disorder (ADHD) and oppositional defiant disorder (ODD) [17].
The present study was carried out to obtain the prevalence of specific DSM-IV childhood psychiatric disorders, the impact of impairment criteria on rates of diagnoses and also to examine the association between psychiatric disorders and relevant sociodemographic factors in a non-referred representative sample in Turkey, a country for which no previous rates are available except ADHD and ODD.
Methods
Sample
This study was conducted in Izmir province—that which includes the third largest city in Turkey. There are 66 public schools in the Izmir province, which has a population of 405.580. The total number of children from 1st to 5th grade is 27.080: A total of 5.581 of them are in first grade, 5.018 of them are in second grade, 5.226 of them are in third grade, 5.751 of them are in fourth grade and 5.504 of them are in fifth grade. Twelve schools out of 66 total were targeted with a randomized sampling method with regard to the low/middle/high socioeconomic class categorization defined by the Ministry of National Education Izmir Provincial Directorate. The sample consisted of 419 randomly selected primary school children with a 5 % margin of error, had an alpha (t) of 1 % and assumed a psychiatric disorder prevalence of approximately 20 %. Among these 12 schools, 419 cases were selected from a per-year list, again using a randomized sampling method. Written informed consents were obtained from the parents of all children participating in the study together with the necessary legal approvals and the Ege University Ethical Committee’s approval. Our study included a broad range of children (6–14 years). Four hundred and seventeen subjects were interviewed, for a total response rate of 99.5 %. Subjects were assessed using the K-SADS-PL and for levels of functionality using the impairment criterion scale.
Instruments and Measures
Kiddie-SADS-Lifetime Version (KSADS-PL)
KSADS-PL is a highly reliable semi-structured interview for the assessment of a wide range of psychiatric disorders in children and adolescents according to DSM-III-R and DSM-IV criteria [18]. A Turkish reliability and validity study of K-SADS was conducted by Gökler et al. [19].
Impairment
In the evaluation of impairment criteria, first, parents were interviewed, and four areas were assessed, including the children’s relationships with their siblings and friends, their homework execution and their general adjustment at home. In ınterviews with teachers, four domains were again assessed: whether the child was problematic or not, his or her relationships with friends at school, his or her general success in subjects and, last, the self-esteem level of the child. These questions were asked of teachers in semi-structured interviews.
All items were rated using the anchors no problem at all (0), a little problematic (1), and very problematic (2). A case was considered to be impaired if he or she was rated as very problematic in at least one area or a little problematic in two or more areas. Similar approaches have previously been used in other epidemiologic studies [20, 21].
Diagnostic Procedures
Four hundred and seventeen cases completed the clinical assessment, which included a psychiatric evaluation using the K-SADS-PL. The interview was administered by one child and adolescent psychiatry resident trained for the administration of the interview, first with the primary caretaker and then with the child. Training on K-SADS-PL administration was given only by the Turkish Association of Child and Adolescent Psychiatry in Turkey, which provided uniform and efficient training to the evaluators. Another child and adolescent psychiatry resident carried out an interview with the parents and teachers for the purpose of evaluating the impairment criterion. A “best estimate procedure” was used to determine the final diagnosis [22]. A “best estimate procedure” provides a diagnosis for a patient after all assessments of teacher and parent scales, semi-structured interviews conducted with parents and children (K-SADS-PL), and evaluations of the impairment criterion by an independent interviewer have been separately conducted.
Data Analysis
The data were analyzed using the Statistical Package for the Social Sciences-Windows, version 16.0. Confidence intervals for the estimated prevalence of disorders were calculated using a binominal approximation method. For the statistical analyses, Chi square tests for categorical variables were used. p values less than 0.05 were considered to be statistically significant.
Results
Prevalence Rates and the Impact of Impairment
A total of 417 school-age children were interviewed, for a response rate of 99.5 %. The mean age of subjects was 9.1 years (SD = 1.4), and the sample included 225 boys (54 %) and 192 girls (46 %). The age range of the subjects was 6–14 years. The mean age of girls was 9.0 years (SD = 1.5), and the mean age of boys was 9.2 years (SD = 1.4).
The results showed that 36.7 % of the sample met DSM-IV criteria when not considering impairment and 25.6 and 14.1 % of the population had one or more DSM-IV disorders when a measure of moderate (parent or teacher) and severe (parent and teacher) impairment specific to each diagnosis was considered, respectively.
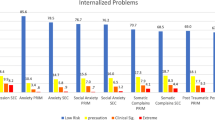
Table 1 presents the prevalence of DSM-IV disorders, both considering and irrespective of impairment, as assessed using the K-SADS-PL. Total rates of specific disorders were 21.8 % for ADHD, 1.9 % for conduct disorder, 2.4 % for oppositional defiant disorder, 13.9 % for anxiety disorders (1.7 % for generalized anxiety disorder [GAD], 0.5 % for post-traumatic stress disorder [PTSD], 11 % for phobia, 0.7 % for obsessive compulsive disorder [OCD], and 1 % for separation anxiety disorder [SAD]), and 2.9 % for mood disorders (2.6 % for major depressive disorder [MDD] and 0.3 % for dysthymic disorder [DD]). For most disorders, rates were reduced by nearly a half through the application of the “severe” impairment criterion (reported by parents and teachers). Rates of ADHD decreased from 21.8 to 12.7 %, and rates of conduct disorder decreased from 2.1 to 1.7 %. There were greater reductions in mood disorders (from 2.9 to 1.4 %) and anxiety disorders (from 13.9 to 2.6 %) compared to other disorders.
Socio-demographic Correlates
Table 2 presents the prevalence of disorders by gender. Boys had significantly higher rates of overall disorder compared with girls, primarily because of the high rates of male-predominant ADHD, whose difference in prevalence between genders was statistically significant (p < 0.05). Girls had slightly higher rates of mood and anxiety disorders, but these differences were not statistically significant (p = 0.123 and p = 0.141, respectively).
Table 3 presents the results of an analysis of the association between socio-demographic characteristics and mental disorders. With respect to parental characteristics, the prevalence rates of ADHD (p < 0.05) and ODD (p < 0.05) were higher in children whose parents were divorced or separated relative to respondents of currently married parents. No statistically significant differences were found between children whose parents were divorced compared to currently married parents with respect to mood disorders (p = 0.129), CD (p = 0.398) and anxiety disorders (p = 0.337).
Children whose mothers had low educational status were at increased risk for ADHD (p < 0.05) and CD (p < 0.05). However, there were not statistically significant differences between educational statuses of the mothers in the cases of ODD (p = 0.730), MD (p = 0.469) or AD (p = 0.677). Moreover, there was no association between the educational statuses of fathers and the prevalence of ODD (p = 0.447), CD (p = 0.357), MD (p = 0.525) or AD (p = 0.372). Only the prevalence of ADHD (p < 0.05) was higher for fathers who had low levels of education.
Discussion
This was the first study to investigate, using a state-of-the-art methodology, the prevalence of frequently observed disorders in pediatric psychiatry in Turkish elementary school children when both considering and disregarding impairment. As stated by Polanczyk and Jensen [2], epidemiologic data are essential for planning health services and implementing strategies of detection and early intervention, with possible substantial benefits for public health. Today, because most of epidemiologic data are obtained from Western countries, it is necessary to obtain accurate and reliable information from all over the world, especially from regions in which epidemiologic data are lacking. Turkey has a geostrategic importance by its neighborhood with European, Asian and Middle Eastern countries, but no epidemiological study about the pediatric psychiatric diseases has been conducted, and this is the first epidemiological study of this kind that conducted in Turkish population. In this study, semi-structured face-to-face interviews were carried out using a one-stage evaluation method (K-SADS); dropout cases were included in the study by considering the lists of the students who started at the school. We assessed the importance of including an impairment criterion by determining frequencies both with and without such a criterion.
In our study, of 417 children, 36.7 % met at least one DSM-IV diagnosis, and 14.1 % had severe functional impairment. This was similar to the results of other DSM-based studies that did not consider impairment, which have found prevalence rates of 38.3 % in Chile [9] and 38.4 % in Hong Kong [8]; these findings were higher than those reported in Canino et al.’s study from Puerto Rico (19,8 %) [7]. Our overall prevalence estimate of 14.1 % with impairment was close to those reported by Leung et al. (16.4 %) and Canino et al. [7] (16.4 %), whereas Vicente et al. [9] reported higher rates (22.5 %). According to literature, differences in the reported prevalence of psychiatric disorders may be the result of different methodologies being used in epidemiological studies [23–25].
Again, these variations may result from differences in sampling (e.g., different age ranges and clinical sampling vs. school sampling), and culturally some disorders may be observed to have different frequencies depending on ethnic group, although this has not been shown to have a significant effect [26]. Methodological features that affect findings include one-versus two-setting designs, diagnostic system (ICD, DSM-III-R or DSM-IV) and a clinical impairment evaluation [27–32]. These kinds of variations in methodologies were also present in our reference studies. In the studies by Canino et al. [7] and Vicente et al. [9], a stratified cluster sampling from the households were used, but Leung et al. [8] used a school sampling like our study. Also, the scales used in the studies were also varied; DISC-IV (Diagnostic Interview Schedule for Children-Version 4) and PIC-GAS (Parent Interview–Children’s Global Assessment Scale) were used in Puerto Rico study [7]; DISC-IV, CBCL (Child Behavior Checklist), and YSR (Youth Self Report) were used in Chinese study [8]; and DISC-IV and SACA (Service Assessment for Children and Adolescents) were used in the Chilean study [9], whereas KSADS-PL was used in our study. Given such methodological diversity, our research was the first cross-sectional study to have met most of the criteria proposed for epidemiological studies, and the findings from this study provided the first estimates of the prevalence of DSM-IV-defined psychiatric disorders in a school-age child population in Turkey. The most common disorder in our study was ADHD (21.8 %), followed by anxiety disorders (13.9 %), mood disorders (2.9 %), and ODD (2.4 %). In contrast to ADHD, anxiety and mood disorder rates were substantially similar to previous reports [7, 33, 34]. ODD and CD rates were lower than those reported in other prevalence studies of mental disorders in children [35]. Previous studies [7, 8] also have reported a reduction in prevalence estimates when an impairment criterion is applied. In our study, ADHD, ODD, anxiety disorders and mood disorders are most affected, whereas CD was the least affected, as a result of considering impairment criteria. It is well-known that rates are much more strongly influenced by impairment [31]. Considering diagnostic criteria alone, diagnostic rates of ADHD are high, as has been reported by other studies. Canino et al. [7] reported ADHD prevalence with and without impairment at 8.9 and 3.7 %, respectively. Similarly, ODD rates are affected by impairment. Likewise, we found significantly different outcomes of pre-and post-impairment ODD rates in a study conducted by our group in Turkey [17]. But, CD was not likely to be affected by the presence of impairment. Similar to previous studies, with the addition of an impairment criteria, we found significant decreases in the frequencies of mood disorders and anxiety disorders [7, 8]. The prevalence of mood disorder reported by Canino et al. [7] (3.4 %) was close to that of our study (2.9 %). Our mood disorder prevalence estimate of 1.4 % with impairment was close to those of Canino et al.’s study (1.7 %). The authors found the frequency of anxiety disorders to be 6.9 % without impairment, whereas we found a rate of 13.9 %. However, they reported a prevalence of anxiety disorders of 2.9 % with the impairment criteria, and this result was similar to ours (2.6 %). Leung et al. [8] reported the frequency of anxiety disorders as 30.2 % without an impairment criteria and 6.9 % with an impairment criteria, and 1.3 and 1.7 % for mood disorder without and with impairment criteria, respectively. As in our study, they found a similar pronounced decrease in the prevalence of anxiety disorders after the addition of impairment criteria. The frequency of mood disorders was similar to the findings of our study when considering impairment (1.4 %). As reported in previous studies, adverse family factors were found to be associated with psychiatric disorders [36, 37]. In contrast to the literature, in their study, Roberts et al. [11] did not find a correlation between socioeconomic status and psychiatric disorders. Similar to other data from the literature [38], a study by Eapen et al. [3] found no relationship among the child’s age, family size, socioeconomic status, parental education level, parental marital status and the child’s psychiatric illness. We found in our study that ADHD and CD were more prevalent at lower socio-economic levels; however, socio-economic level was not associated with ODD or anxiety disorders. Children whose mothers and fathers had low levels of education were at increased risk for ADHD. The prevalence rates of ADHD and ODD were higher in children whose parents were divorced or separated compared to the respondents who had currently married parents.
In a study with a large sample size which indicated that, in 2003, approximately 4.4 million children aged 4–17 years were reported to have a history of ADHD diagnosis, ADHD was reported to occur in boys 2.5 times more than girls [39], whereas in a meta-analysis of 102 studies with 171,756 subjects conducted between 1978 and 2005, ADHD prevalence for boys was demonstrated to be 2.4-fold higher than for girls [31]. Likewise, our study found the incidence of ADHD to be 2.8-fold higher for boys than for girls, and there was a statistically significant difference between both genders. Impairment is more common in boys than in girls during the period before puberty. The gender ratio becomes balanced after puberty [35, 40]. Although not statistically significant, in this study, the prevalence of ODD was more common in boys than girls. The boy/girl ratio was found to be 3:2 when excluding impairment, whereas this ratio was 4:1 when considering the impairment criterion. It has been found that the subtype beginning in the childhood period more frequently occurs in boys than the subtype beginning in the adolescence period, whereas conduct problems increase in girls in the period before puberty [41, 42]. In our study, impairment was more common in boys than girls, and the boy/girl ratio was 7:1. Although not statistically significant, anxiety and depressive disorders are reported in the literature to be more common in girls [11, 23]. Consistent with the literature, in this study, girls had slightly higher rates of mood and anxiety disorders, but there were no statistically significant differences for either mood or anxiety disorders.
This study has several strengths. It provides the first estimates of the prevalence of specific DSM-IV-defined psychiatric disorders in a Turkish population of children. We obtained information from children, parents and teachers. Information that supplemented the diagnostic data in this study included ratings of the clinical significance of the disorders through the inclusion of systematic information on different levels of functional impairment.
Limitations
There were number of limitations to this study. First, there was a relatively small sample size and a broad range in ages, from 6 to 14 years; consequently, our sample size was inadequate for determining age- and sex-specific prevalence. Second, the issues of comorbidity and mental health service use rates were not addressed. Another limitation that should be considered are the cultural factors, which may have a role on the parents’ perceptions about the functions of their children, and the possibility that they may minimize the effect of disabilities, and impairment.
Summary
Few epidemiologic studies have aimed at estimating the prevalence, incidence and associated risk factors of psychiatric disorders for children and adolescents in developing countries, as is the case in Turkey. Using state-of-the-art methodology, this study was designed to assess the prevalence of psychiatric disorders and the impact of impairment criteria on rates of diagnoses in a representative sample of elementary school children from a country in a region where no rates were previously available. We sampled 419 primary school children by using a one-stage design in. The response rate was 99.5 % and 417 cases were extensively assessed using K-SADS-PL and a scale to assess the impairment criterion. For the statistical analyses, Chi square tests for categorical variables were used. p values less than 0.05 were considered to be statistically significant. The results showed that 36.7 % of the sample met DSM-IV criteria independent of impairment and that 14.1 % of the population had one or more DSM-IV disorders when a measure of impairment specific to each diagnosis was considered. The most prevalent disorders were ADHD and anxiety disorders. This study provided the first estimates of the prevalence of specific DSM-IV-defined psychiatric disorders in a Turkish population of children. Upon the inclusion of diagnosis-specific impairment criteria, all rates of psychiatric disorders slightly decreased except for Conduct Disorder (CD), which is consistent with the previous literature. The results from this study should be confirmed by further studies conducted in other regions of Turkey.
References
Ford T, Goodman R, Meltzer H (2003) The British child and adolescent mental health survey 1999: the prevalence of DSM-IV disorders. J Am Acad Child Adolesc Psychiatry 42:1203–1211
Polanczyk G, Jensen P (2008) Epidemiologic considerations in attention deficit hyperactivity disorder: a review and update. Child Adolesc Psychiatr Clin N Am 17:245–260
Eapen V, Jakka ME, Abou-Saleh MT (2003) Children with psychiatric disorders: the A1 Ain community psychiatric survey. Can J Psychiatry 48:402–407
Brauner CB, Stephens CB (2006) Estimating the prevalence of early childhood serious emotional/behavioral disorders: challenges and recommendations. Public Health Rep 121:303–310
Romano E, Tremblay RE, Vitaro F, Zoccolillo M, Pagani L (2001) Prevalence of psychiatric diagnoses and the role of perceived impairment: findings from an adolescent community sample. J Child Psychol Psychiatry 42:451–461
McArdle P, Prosser J, Kolvin I (2004) Prevalence of psychiatric disorder: with and without psychosocial impairment. Eur Child Adolesc Psychiatry 13:347–353
Canino G, Shrout PE, Rubio-Stipec M, Bird HR, Bravo M, Ramirez R et al (2004) The DSM-IV rates of child and adolescent disorders in Puerto Rico: prevalence, correlates, service use, and the effects of impairment. Arch Gen Psychiatry 61:85–93
Leung PW, Hung SF, Ho TP, Lee CC, Liu WS, Tang CP et al (2008) Prevalence of DSM-IV disorders in Chinese adolescents and the effects of an impairment criterion: a pilot community study in Hong Kong. Eur Child Adolesc Psychiatry 17:452–461
Vicente B, Saldivia S, de la Barra F, Kohn R, Pihan R, Valdivia M et al (2012) Prevalence of child and adolescent mental disorders in Chile: a community epidemiological study. J Child Psychol Psychiatry 53:1026–1035
Vicente B, de la Barra F, Saldivia S, Kohn R, Rioseco P, Melipillan R (2011) Prevalence of child and adolescent psychiatric disorders in Santiago, Chile: a community epidemiological study. Soc Psychiatry Psychiatr Epidemiol 47:1099–1109
Roberts RE, Roberts CR, Xing Y (2007) Rates of DSM-IV psychiatric disorders among adolescents in a large metropolitan area. J Psychiatr Res 41:959–967
Motti-Stefanidi F, Tsiantis J, Richardson SC (1993) Epidemiology of behavioural and emotional problems of primary schoolchildren in Greece. Eur Child Adolesc Psychiatry 2:111–118
Roussos A, Karantanos G, Richardson C, Hartman C, Karajiannis D, Kyprianos S et al (1999) Achenbach’s Child Behavior Checklist and Teacher’s Report Form in a normative sample of Grek children 6–12 years old. Eur Child Adolesc Psychiatry 8:165–172
Minaei A (2005) Manual of ASEBA school-age forms for Iranian children. Research Institute for Tehran: Exceptional Children
Erol N, Kilic C, Ulusoy M, Kececi M, Simsek Z (1997) Mental health profiles in Turkey: a preliminary report. Aydogdu, Ankara, pp 12–33
Simşek Z, Erol N, Oztop D, Ozer Ozcan O (2008) Epidemiology of emotional and behavioral problems in children and adolescents reared in orphanages: a national comparative study. Turk Psikiyatr Derg 19:235–246
Ercan ES, Kandulu R, Uslu E, Ardic UA, Yazici KU, Basay BK et al (2013) Prevalence and diagnostic stability of ADHD and ODD in Turkish children: a 4-year longitudinal study. Child Adolesc Psychiatry Ment Health 7:30
Kaufman J, Birmaher B, Brent D, Rao U, Flynn C, Moreci P et al (1997) Schedule for affective disorders and schizophrenia for school-age children-present and lifetime version (KSADS-PL): initial reliability and validity data. J Am Acad Child Adolesc Psychiatry 36:980–988
Gökler B, Ünal F, Pehlivantürk B, Çengel Kültür E, Akdemir D, Taner Y (2004) Okul Çağı Çocukları İçin Duygulanım Bozuklukları ve Şizofreni Görüşme Çizelgesi-Şimdi ve Yaşam Boyu Şekli-Türkçe Uyarlamasının Geçerlik ve Güvenirliği. Çocuk ve Gençlik Ruh Sağlığı Dergisi 11:109–116
Brotman MA, Schmajuk M, Rich BA, Dickstein DP, Guyer AE, Costello EJ et al (2006) Prevalence, clinical correlates, and longitudinal course of severe mood dysregulation in children. Biol Psychiatry 60:991–997
Cho SC, Kim BN, Kim JW, Rohde LA, Hwang JW, Chungh DS et al (2009) Full syndrome and subthreshold attention-deficit/hyperactivity disorder in a Korean community sample: comorbidity and temperament findings. Eur Child Adolesc Psychiatry 18:447–457
Leckman JF, Sholomskas D, Thompson WD, Belanger A, Weissman MM (1982) Best estimate of lifetime psychiatric diagnosis: a methodological study. Arch Gen Psychiatry 39:879–883
Costello EJ, Mustillo S, Keller G, Angold A (2004) Prevalence of psychiatric disorders in childhood and adolescence. In: Levin BL, Petrila J, Hennessy KD (eds) Mental health services: a public health perspective. Oxford University Press, New York, pp 111–1282
Roberts RE, Attkisson CC, Rosenblatt A (1998) Prevalence of psychopathology among children and adolescents. Am J Psychiatry 155:715–725
Lahey BB, Miller TL, Gordon RA, Riley AW (1999) Developmental epidemiology of the disruptive behavior disorders. In: Quay HC, Hogan AE (eds) Handbook of disruptive behavior disorders, vol 99. Kluwer, New York, pp 23–48
Roberts RE, Roberts CR, Xing Y (2006) Prevalence of youth-reported DSM-IV psychiatric disorders among African, European, and Mexican American adolescents. J Am Acad Child Adolesc Psychiatry 45:1329–1337
Shaffer D, Fisher P, Dulcan MK, Davies M, Piacentini J, Schwab-Stone ME et al (1996) The NIMH diagnostic interview schedule for children version 2.3 (DISC-2.3): description, acceptability, prevalence rates, and performance in the MECA study: methods for the epidemiology of child and adolescent mental disorders study. J Am Acad Child Adolesc Psychiatry 35:865–877
Costello EJ, Angold A, Burns BJ, Stangl DK, Tweed DL, Erkanli A et al (1996) The Great Smoky Mountains Study of youth. Goals, design, methods, and the prevalence of DSM-III-R disorders. Arch Gen Psychiatry 53:1129–1136
Narrow WE, Regier DA, Goodman SH, Rae DS, Roper MT, Bourdon KH et al (1998) A comparison of federal definitions of severe mental illness among children and adolescents in four communities. Psychiatr Serv 49:1601–1608
Cartwright-Hatton S, McNicol K, Doubleday E (2006) Anxiety in a neglected population: prevalence of anxiety disorders in pre-adolescent children. Clin Psychol Rev 26:817–833
Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA (2007) The worldwide prevalence of ADHD: a systematic review and metaregression analysis. Am J Psychiatry 164:942–948
Skounti M, Philalithis A, Galanakis E (2007) Variations in prevalence of attention deficit hyperactivity disorder worldwide. Eur J Pediatr 166:117–123
Merikangas KR, Nakamura EF, Kessler RC (2009) Epidemiology of mental disorders in children and adolescents. Dialogues Clin Neurosci 11:7–20
Costello EJ, Egger H, Angold A (2005) 10-year research update review: the epidemiology of child and adolescent psychiatric disorders: I. Methods and public health burden. J Am Acad Child Adolesc Psychiatry 44:972–986
Canino G, Polanczyk G, Bauermeister JJ, Rohde LA, Frick PJ (2010) Does the prevalence of CD and ODD vary across cultures? Soc Psychiatry Psychiatr Epidemiol 45:695–704
Gureje O, Omigbodun OO (1995) Children with mental disorders in primary care: functional status and risk factors. Acta Psychiatr Scand 92:310–314
Eapen V, Al-Gazali L, Bin-Othman S, Abou-Saleh MT (1998) Mental health problems among schoolchildren in United Arab Emirates: prevalence and risk factors. J Am Acad Child Adolesc Psychiatry 37:880–886
Ghubash R, Hamdi E, Bebbington P (1992) The Dubai community psychiatric survey: I. Prevalence and socio-demographic correlates. Soc Psychiatry Psychiatr Epidemiol 27:53–61
Centers for Diseases Control and Prevention (CDC) (2005) Mental health in the United States. Prevalance of diagnosis and medication treatment for attention-deficit/hyperactivity disorder-United States, 2003. MMWR Morb Mortal Wkly Rep 54:842–847
Loeber R, Burke J, Pardini DA (2009) Perspectives on oppositional defiant disorder, conduct disorder, and psychopathic features. J Child Psychol Psychiatry 50:133–142
August GJ, Realmuto GM, Joyce T, Hektner JM (1999) Persistence and desistance of oppositional defiant disorder in a community sample of children with ADHD. J Am Acad Child Adolesc Psychiatry 38:1262–1270
Maughan B, Rowe R, Messer J, Goodman R, Meltzer H (2004) Conduct disorder and oppositional defiant disorder in a national sample: developmental epidemiology. J Child Psychol Psychiatry 45:609–621
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Ercan, E.S., Bilaç, Ö., Uysal Özaslan, T. et al. Prevalence of Psychiatric Disorders Among Turkish Children: The Effects of Impairment and Sociodemographic Correlates. Child Psychiatry Hum Dev 47, 35–42 (2016). https://doi.org/10.1007/s10578-015-0541-3
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10578-015-0541-3