
Abstract
The choices for blood vessels to undergo angiogenesis or stay quiescent are mostly determined by the status of tissue oxygenation. A major link between tissue hypoxia and active angiogenesis is the accumulation of hypoxia-inducible factor (HIF)-α subunits which play a major role in the transcriptional activation of genes encoding angiogenic factors. HIF-α abundance is negatively regulated by a subfamily of dioxygenases referred to as prolyl hydroxylase domain-containing proteins (PHDs) which use O2 as a substrate to hydroxylate HIF-α subunits and hence tag them for rapid degradation. Under hypoxic conditions, HIF-α subunits accumulate due to reduced hydroxylation efficiency and form transcriptionally active heterodimers with HIF-1ß to activate the expression of angiogenic factors and other proteins important for cellular adaptation to hypoxia. Angiogenesis is regulated by a combination of at least two different mechanisms. The paracrine mechanism is mediated by non-endothelial expression of angiogenic factors such as vascular endothelial growth factor (VEGF)-A, which in turn interact with endothelial cell surface receptors to initiate angiogenic activities. In the autocrine mechanism, endothelial cell themselves are induced to express VEGF-A, which collaborate with the paracrine mechanism to support angiogenesis and protect vascular integrity. Because of critical roles of PHDs and HIFs in regulating angiogenic activities, studies are underway to assess their candidacy as targets for angiogenesis therapies.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
In most normal adult tissues, the endothelium is quiescent, and blood vessels do not undergo significant growth. Such a status is conditional to adequate tissue oxygenation, which varies between 30 ~ 50 mmHg (4 ~ 6.5% of one atmospheric pressure) depending on specific tissue types [29, 99]. These values are significantly below the normal oxygen partial pressure in ambient room air and hence are often referred to as physiological hypoxia. Tissue oxygen content may fall further below physiological hypoxia levels for a variety of reasons. For example, oxygen consumption outpaces supply in rapidly expanding embryonic tissues, thus leading to developmental hypoxia which plays a key role in the development of the vascular system. In adult tissues, occlusion of coronary arteries results in cardiac tissue hypoxia and heart attack. While physiological hypoxia does not typically promote vascular growth, a further reduction in tissue oxygen tension may trigger angiogenesis.
Expression of angiogenic molecules in oxygen deficient tissues is mostly due to the accumulation of hypoxia-inducible factors (HIFs), which are heterodimeric transcription factors of α and ß subunits. HIFs activate the transcription of a long list of genes encoding a diverse set of proteins, such as glycolytic enzymes, erythropoietin, and VEGF-A. Oxygen-dependent regulation of HIF-α abundance is mediated by a subfamily of dioxygenases, including PHD1, PHD2, and PHD3 (prolyl hydroxylase domain-containing proteins) [6, 23, 42], and a polyubiquitination and proteasomal degradation mechanism that rapidly degrades hydroxylated HIF-α [44, 46, 72]. Since molecular oxygen is a substrate to prolyl hydroxylase domain-containing proteins (PHDs), reduced oxygen content in a hypoxic environment favors HIF-α accumulation due to poor hydroxylation reactions.
This review focuses on the regulation of angiogenesis by changes in tissue oxygen levels. Specifically, the following topics will be discussed: (1) how fluctuations in tissue oxygen levels are detected by intracellular mechanisms; (2) how tissue hypoxia regulates the expression of angiogenic molecules; (3) mouse models for the study of oxygen sensing mechanisms and angiogenesis; and (4) oxygen sensing and pathological angiogenesis.
Oxygen sensing mechanisms
Prolyl hydroxylase domain-containing proteins
PHDs form a subfamily of 2-oxoglutarate (2-OG)/Fe(II)-dependent dioxygenases that are evolutionarily conserved from worms to mammals [6, 23]. While Caenorhabditis elegans or Drosophila melanogaster each has a single PHD enzyme, three PHD isoforms, including PHD1, PHD2, and PHD3, are present in mammalian cells [6, 23]. PHDs are often referred to as egg laying nine (EGL-9 or EGLN) due to the fact that the PHD prototype was first discovered as a protein encoded by the EGL-9 locus in C. elegans; they are also called "HIF prolyl hydroxylases (HPH)" or "proline-4 hydroxylases for HIF-α (P4H-HIF)" based on their main functions [37]. A fourth HIF-α hydroxylase, P4H-TM, has also been identified recently [51]. However, this enzyme is distinct from PHDs in two respects: (1) it is a transmembrane protein in the endoplasmic reticulum, whereas all three PHDs are soluble enzymes and (2) P4H-TM amino acid sequence is more closely related to collagen hydroxylase than to PHDs, although its substrate specificity is more similar to PHDs and does not hydroxylate collagen [51].
PHDs hydroxylate specific proline residues in the so-called oxygen-dependent degradation (ODD) domain of HIF-α, which encompasses a region of about 200 amino acid residues in the C-terminal half [40]. However, the ODD domain contains two separate prolyl hydroxylation sites (e.g., P402 and P564 in human HIF-1α), each of which is present in the conserved sequence motif LXXLAP and is hydroxylated independently [70].
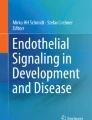
The PHD hydroxylase activities are mostly controlled by the availability of co-factors and substrates, including Fe(II), O2 and 2-OG [23, 37, 80, 95]. Because cytosolic concentrations of these molecules are influenced by a variety of cellular events, it is not surprising that PHD hydroxylase activities are also regulated by multiple mechanisms (Fig. 1). For example, reactive oxygen species (ROS), which often originate from dysfunctional mitochondria, may oxidize Fe(II) to Fe(III) and inhibit hydroxylase activity [80]. Similarly, lack of ascorbate (vitamin C) may also suppress PHD hydroxylase activity due to the essential role of ascorbate in reducing Fe(III) to Fe(II). Increased cytosolic presence of 2-OG analogs such as succinate, often due to defective mitochondrial functions, may also reduce PHD activity by inhibiting normal interaction between 2-OG and PHDs [95]. Mitochondria also inhibit PHD activities by consuming large amounts of O2 and therefore reducing cytosolic O2 concentration [7, 31, 33, 47].

Regulatory mechanisms of PHD hydroxylase activities. Factors or processes with positive effects on PHD hydroxylase activities are shown in green, whereas those with inhibitory effects are shown in red
The oxygen concentrations in normal tissues fluctuate around 60 μM [29, 99], which is far below the Km values of all three PHDs (230 ~ 250 μM) [37], suggesting that PHDs are only partially active even in normal tissues. The fact that physiological O2 concentration is far below Km values ensures that PHD activity is sensitive to fluctuations in O2 concentrations. Consequently, any further decreases in O2 concentration from physiological values would effectively suppress PHD hydroxylase activities and trigger significant HIF-α accumulation.
Factor inhibiting HIF
Factor inhibiting HIF (FIH) is also a dioxygenase that contributes to intracellular oxygen sensing. Instead of regulating HIF-α abundance, FIH inhibits the transcriptional activity of HIF-α by oxygen-dependent hydroxylation of a specific asparagine residue in HIF-α transcription activation domain [53, 64, 102]. For example, hydroxylation at Asn 851 in human HIF-1α prevents its interaction with CBP/p300, a transcriptional coactivator important for HIF activity [53, 64]. Although Asn 851 hydroxylation does not affect the formation of HIF-αß heterodimers, lack of CBP/p300 interaction inactivates HIF transcription activity.
Hypoxia-inducible factors
Hypoxia-inducible factors are heterodimers between an α subunit and HIF-1ß [22, 46]. Of note, HIF-1ß also plays a role in the nuclear translocation of aryl hydrocarbon receptor (AhR) which is important for detoxification of aryl hydrocarbon compounds, a function that has no apparent relevance to hypoxia signaling [90]. For its role in heterodimerization with and nuclear translocation of AhR, HIF-1ß is also referred to as aryl hydrocarbon receptor nuclear translocator (ARNT).
While HIF-1ß is insensitive to oxygen, HIF-1α and HIF-2α are rapidly degraded via PHD catalyzed hydroxylation. Initial siRNA mediated knockdown of different PHD isoforms indicated that HIF-1α hydroxylation was mostly mediated by PHD2, but subsequent studies indicated that this preference was at least partially due to the fact that PHD2 was more abundantly expressed than other PHD isoforms [3, 4]. Nonetheless, partial substrate selectivity does exist, wherein HIF-1α is more efficiently hydroxylated by PHD2 whereas HIF-2α is a better substrate for PHD1 and PHD3 [3].
Although hydroxylated HIF-α subunits undergo VHL-dependent polyubiquitination and proteasomal degradation [44, 72], at least two conditions ensure that there is a basal level presence of HIF-α in normal tissues: (1) HIF-1α and HIF-2α are constitutively transcribed and translated, while activation of several signaling pathways may further boost their expression levels [55, 108, 118] and (2) PHDs are only partially active in normal adult tissues due to below suboptimal cytosolic O2 concentrations. The persistence of basal level HIF-α proteins may be important for normal physiological logical functions.
Different HIF-α genes are differentially transcribed in different cell types, although their expression profiles are partially overlapping. In general, HIF-1α mRNA is broadly present throughout most tissues, although protein accumulation is subject to regulation by local oxygen levels [58]. In contrast, HIF-2α is mostly expressed in endothelial cells during embryonic development, and for this reason it is also referred to as endothelial PAS domain protein [22]. In adult tissues, HIF-2α expression is also more restricted than HIF-1α, although it is expressed in a number of non-endothelial cell types as well, including hepatocytes, lung epithelial cells and kidney interstitial cells [12, 88, 93].
The broad expression pattern of HIF-1α is consistent with a role in mediating the paracrine mechanism of angiogenesis. In brief, HIF-1α accumulation in non-endothelial cells triggers the expression of angiogenic factors such as VEGF-A, which initiate angiogenesis by interacting with their endothelial cell receptors. In contrast, HIF-2α is more predominantly expressed in endothelial cells in most tissues, suggesting that HIF-2α plays a major role in adapting ECs to tissue hypoxia. There is, however, no absolute division between the roles of HIF-1α and HIF-2α. HIF-1α may also play roles in endothelial cells, at least under certain conditions, whereas HIF-2α may also play a role in paracrine signaling during angiogenesis [50, 88].
Much less is known about HIF-3α. In contrast to HIF-1α and HIF-2α, HIF-3α is upregulated by hypoxia at the transcriptional level [34]. HIF-3α protein can be hydroxylated by PHDs and undergoes VHL-dependent polyubiquitination, but oxygen-dependent degradation has not been directly demonstrated [73]. The heterodimer between HIF-3α and HIF-1ß only has very low transcriptional activity and is not known to be involved in angiogenesis. In addition, alternative splicing of HIF-3α primary transcript generates several variants, some of which lack the transcriptional activation domain and form transcriptionally inactive heterodimers with HIF-1ß [65, 66]. Thus, HIF-3α alternative splicing isoforms may act as competitive inhibitors that block heterodimer formation between HIF-1ß with other α isoforms.
Interesting, there is a negative feedback mechanism wherein HIF-1α limits its own accumulation under hypoxia by upregulating the expression of PHD2 and PHD3 [16, 17, 74, 101]. This mechanism may be important to prevent excessive HIF-α accumulation under hypoxia, but is also thought to play a crucial role in allowing rapid clearance of HIF-α upon tissue reoxygenation [16]. The relationship between PHDs, HIFs, and the expression of angiogenic molecules is schematically explained in Fig. 2.

Relationship between oxygen availability and the expression of angiogenic molecules (VEGF-A and VEGF receptor-2 as examples). HIF-1α, HIF-2α and HIF-1ß are shown as half ovals, and corresponding heterodimers are shown as their combinations. Oxygen induces HIF-1α and HIF-2α degradation by PHD dependent hydroxylation, followed by VHL-mediated recruitment of hydroxylated HIF-α subunits E3 polyubiquitin ligase complex and subsequent degradation in proteasomes. HIF-α escapes degradation due to hypoxia, they form heterodimers and activate the transcription of VEGF-A and VEGF receptors. Both HIF-1 and HIF-2 contribute to VEGF-A expression, but only HIF-2 is known to activate the expression of VEGFR-2
Regulated expression of angiogenic molecules
HIF-1α and HIF-2α both activate the expression of genes important for angiogenesis as well as other processes, but some level of selectivity does exist. While both can activate the expression of target genes important for angiogenesis and erythropoiesis, only HIF-1α activates the expression of glycolytic genes [39]. On the other hand, HIF-2α but not HIF-1α activates the expression of Oct-4 which is important for the maintenance of pluripotency of stem cells during development [15]. Discussion in this section will focus on angiogenic genes (Table 1).
Among hypoxia-induced angiogenic genes, some are bona fide HIF target genes and are regulated by direct interactions between HIF and a DNA sequence motif on HIF target genes referred to as hypoxia response elements (HRE). Examples of these genes include VEGF-A [26], VEGFR-1/Flt-1[27, 105], erythropoietin (EPO) [75, 96], and eNOS [14, 117]. However, there are also many HIF-inducible genes that are not known to contain HRE. Examples in this category include fibroblast growth factor (FGF) 2, placental growth factor (PLGF), platelet-derived growth factor (PDGF)-B, angiopoietin (ANGPT)-1 and 2, and ANGPT receptor Tie-2 [18, 49]. While some of these genes may carry yet unidentified HRE and therefore are actually direct HIF targets, others are probably indirectly induced by transcription factors which themselves are directly or indirectly HIF-induced.
HIF-1α and HIF-2α display some selectivity over different angiogenic target genes. For example, while VEGF-A expression can be induced by both HIF-1 and HIF-2, upregulation of VEGFR-2/Flk-1 appears to be mediated by HIF-2α but not HIF-1α [48]. HIF-2α dependence might be due to the presence of HIF-2 binding site (HBS) in Flk-1 promoter instead of a typical HRE found in most HIF-1 responsive genes [48]. The dependence of Flk-1 expression on HIF-2α may have physiological relevance, because both HIF-2α and Flk-1 are most abundantly expressed in endothelial cells (although with a few exceptions such as hepatocytes which expresses HIF-2α but not Flk-1). In addition to differential HIF-1α and HIF-2α expression in different cell types, the accumulation of the same HIF-α isoform in different cell types may also have differential regulatory effects. For example, HIF-1α accumulation in retinal tissues led to increased expression of VEGF-A, PDGF-B, PLGF, ANGPT (angiopoietin)-1 and 2, but similar HIF-1α accumulation in cardiomyocytes only increased the expression of VEGF-A and PLGF [49].
Effects of hypoxia on vascular cells
Endothelial cells
Hypoxia may have complicated effects on cultured endothelial cells (ECs). Moderate hypoxia (e.g., 5% oxygen) promotes proliferation, survival, migration, and vascular network formation via increased expression of VEGF-A, eNOS, and other angiogenic molecules [77, 85]. On the other hand, more severe hypoxia may cause increased EC apoptosis, partly due to NFκB-dependent suppression of Bcl-2 expression and stabilization of p53 [71, 100]. In living tissues, hypoxia both directly affects ECs by modulating endothelial gene expression and indirectly by paracrine mechanisms wherein expression of angiogenic factors in non-endothelial cells regulates EC functions [56, 68]. It is interesting to note that EC-derived VEGF-A plays a unique role by activating intracellular VEGFR-2 signaling before it is secreted [56]. Intracellular VEGF-A/VEGFR-2 signaling plays a critical role in maintaining EC viability and vascular integrity, a conclusion supported by the finding that EC-specific knockout of VEGF-A resulted in EC apoptosis and loss of vascular integrity [56].
Vascular smooth muscle cells
Moderate hypoxia induces vascular smooth muscle cells (VSMCs) proliferation, in part by inducing the expression of cyclooxygenase (COX)-2 and PDGF-ß receptor [54, 97], but severe hypoxia causes apoptosis [61]. Besides altered proliferation and survival properties, VSMCs exposed to hypoxia may be less adhesive to extracellular matrix proteins, a change that is associated with HIF-1α-mediated inhibition of FAK phosphorylation [13]. Reduced VSMC adhesion to extracellular proteins in the basement membrane may favor angiogenesis, because disassociation of VSMCs (or other mural cells such as pericytes) from the basement membrane is thought to be a necessary condition to allow the protrusion of the underlying ECs to form new sprouts. VSMC properties are also regulated by a list of molecules whose relationships to the oxygen sensing mechanism are yet unclear. One example of these molecules is Ephrin B2, which support the association of VSMC-like mural cells to endothelial cells [25].
Macrophages
Hypoxic tissues express a number of extracellular factors that are capable of recruiting monocytes, including chemoattractant protein-1 (MCP-1) [8], colony-stimulating factor (CSF)-1 [11], tumor necrosis factor-α (TNF-α) [36], stromal-derived factor (SDF)-1 [110], and VEGF-A [19]. Once recruited to hypoxic tissues, monocytes differentiate into macrophages and promote angiogenesis by several mechanisms: (1) secretion of metalloproteases, which degrade extracellular matrix proteins and activate latent angiogenic factors such matrix bound VEGF-A by proteolytic cleavage [45]; (2) expression and secretion of angiogenic factors; and (3) amplification of hypoxia responses by secreting a short peptide of 39 amino acid residues (PR39) which enters cytoplasm of resident cells and interferes with HIF-α degradation [59].
Regulation of angiogenesis by oxygen sensing mechanisms
Role of HIF-1 and HIF-2 in vascular development
In mouse embryos, sites of HIF-1α protein accumulation correlates with VEGF-A expression, suggesting a role of HIF-1α in embryonic expression of VEGF-A [58]. Mouse embryos lacking HIF-1α or ARNT do not survive beyond embryonic days 9.5 to 10.5 due to poor angiogenesis, defective neural tube development, and death of mesenchymal cells [43, 67, 91]. The association of multiple defects with HIF-1α or ARNT deficiency was consistent with the requirement of HIF-1α and ARNT in many different cell types. The consequences of HIF-2α knockout varied depending on mouse strains. In 129 SvJ background, loss of HIF-2α interfered with the progression of the initial embryonic vascular network into mature vascular trees [18, 81]. However, in other strain backgrounds, HIF-2α knockout does not result in obvious vascular defects [12, 92, 107].
Unlike HIF-1α and HIF-2α, HIF-3α only has low transcriptional activity, and is not known to have a proangiogenic role [115, 116]. Mice lacking HIF-3α are viable, although a number of post-natal defects were found including enlarged right ventricle and defective lung remodeling [116]. In fact, HIF-3α may inhibit angiogenesis because some alternative splicing isoforms lack transcriptional activation domain and compete against HIF-1α and HIF-2α for HIF-1ß heterodimerization. In the cornea, for example, a truncated HIF-3α isoform (inhibitor of PAS, or IPAS) has a demonstrated role as an angiogenic inhibitor and is critical to the maintenance of the avascular status of the cornea [65]. Since the HIF-3α promoter is upregulated by hypoxia, the avascular (and hence hypoxic) nature of the cornea sustains itself by upregulating the transcription of the HIF-3α gene [66].
Consequences of HIF-α stabilization
Oxygen-insensitive HIF-1α, engineered by proline to alanine/glycine mutations in the ODD domain, have been expressed in mouse tissues by different approaches including transgene expression of mutant cDNA or infection with adenoviral expression vectors [21, 35, 49, 79, 111]. When expressed in the dermis, retina, myocardium, or skeletal muscles, stabilized HIF-1α accumulated to high levels, significantly increased VEGF-A expression, and led to active angiogenesis [21, 35, 79, 111]. Increased angiogenesis was also induced by transgenic overexpression of similarly mutated HIF-2α in dermal and hepatic tissues, but concurrent overexpression of both HIF-1α and HIF-2α was more effective in activating angiogenesis than by either of them [50].
While transgenic overexpression or delivery of exogenous VEGF-A often leads to the formation of unstable and leaky blood vessels that fail to recruit pericytes and VSMCs, blood vessels induced by the expression of stabilized HIF-α were apparently normal, even though HIF-α accumulation upregulated VEGF-A levels [21, 79, 111]. It is not known for certainty why HIF-α accumulation did not prevent VSMC recruitment; however, one possible explanation is that HIF-α also induces the expression of a repertoire of angiogenic factors in addition to VEGF-A, including factors that promote VSMC/pericyte recruitment such as angiopoietins and PDGF-B [49]. Another possible reason is HIF-α accumulation induces all different VEGF-A isoforms whereas transgenic overexpression or delivery of exogenous VEGF-A typically involves VEGF-A165 isoform alone.
Role of VHL and PHDs in angiogenesis
VHL or PHD2 deficient embryos die in utero during midgestation due to placental defects [28, 104]. In contrast, PHD1 and PHD3 knockout embryos are apparently normal. Differential requirements for different PHDs are consistent with the fact that PHD2 is much more abundantly expressed than other PHD isoforms. PHD2 or VHL null embryos do not display apparently increased angiogenic activity, even though HIF-1α and HIF-2α levels are significantly elevated [28, 104]. One probable reason is that angiogenesis is already happening at a near maximal pace during normal embryogenesis so that any additional HIF-α accumulation has relatively insignificant impact. In contrast to embryonic phenotypes, VHL or PHD2 deficiency in adult mice led to significantly increased angiogenesis [32, 87, 103]. These findings suggest that VHL or PHD2 play essential roles in maintaining the quiescent nature of adult blood vessels.
Role of tissue hypoxia in pathological angiogenesis
Angiogenesis due to tissue expansion
During the development of atherosclerotic plaques, rapid proliferation of VSMCs and accumulation of macrophages increase metabolic demand and oxygen consumption, resulting in local tissue hypoxia within plaques [41]. These conditions induce angiogenic growth of microvessels from vasa vasorum into plaques, forming a vicious cycle wherein plaque expansion induces angiogenesis but vascularization of the plaque further exacerbates its expansion by facilitating the infiltration of macrophages through newly formed blood vessels [76]. Consistent with a role of HIF-1α and VEGF-A in plaque angiogenesis, these proteins were found to be co-localized in atherosclerotic plaques [112].
Hypoxia in arthritis synovium is mostly caused by the high metabolic rate associated with tissue expansion and the presence of large numbers of infiltrated leukocytes. As in other hypoxic tissues, high levels of HIF-1α in arthritis synovium activate the expression of various proangiogenic genes and induce angiogenesis [38, 84]. It has been proposed that inhibition of angiogenesis in arthritic tissues may reduce metabolic activities and therefore shrink the synovium tissue mass [24].
Angiogenesis in tumor tissues is induced by tumor tissue hypoxia as well as high level expression of angiogenic growth factors directly contributed by oncogenic activation of various signaling pathways. HIF-α accumulation in tumors is triggered not only by hypoxia, but also by a number of other mechanisms including transcriptional and translational upregulation in response to oncogenic activation of various signaling pathways [60]. In addition, hypoxia-independent HIF-α stabilization also occurs, often due to loss of p53 or accumulation of succinate [89, 95]. Thus, in addition to hypoxia, various other oncogenic alterations may also directly contribute to tumor angiogenesis. Details of the role of hypoxia in tumor angiogenesis are reviewed in another article in this issue.
Angiogenesis due to poor perfusion
Wounded tissues are typically hypoxic and actively express angiogenic factors. Besides resident cells, infiltrated neutrophils, mast cells, lymphocytes, and macrophages also express high levels of angiogenic factors and promote angiogenesis [69]. Applications of PHD inhibitors L-mimosine (L-Mim) and N-carboxymethylamid (S956711) or competitive peptides corresponding to the conserved HIF-α hydroxylation sites were found to stimulate angiogenesis [113, 114]. Delivery of stabilized HIF-1α to dermal wounds by a peptide-based technology also effectively enhanced angiogenesis and vascular maturation [109].
In another example of angiogenesis induced by poor tissue perfusion, rupture of atherosclerotic plaques in coronary arteries leads to the formation of thrombi which clog coronary circulation and cause myocardial ischemia and infarction. HIF-1α accumulation and VEGF-A expression are both increased in the early phase of ischemia or infarction development [57]; however, persistent oxygen deficiency may result in widespread cell deaths and therefore hinder the expression of angiogenic factors. Several studies demonstrated that introduction of HIF-1α overexpression vectors into myocardial tissues or inhibition of HIF-1α degradation by RP39 promoted angiogenesis and facilitated cardiac repair [59, 98].
Re-vascularization of ischemic myocardial tissues may occur by a combination of two mechanisms. One is angiogenic sprouting from bordering healthy cardiac tissues, and the other is the recruitment of myeloid-derived circulating endothelial cell progenitors [52, 78]. In addition, myeloid-derived cells in the circulation may also provide a source to pericytes that help stabilizing newly formed microvessels. Recent studies indicate that the recruitment of endothelial and pericyte progenitors from the circulation may be mediated by VEGF-A and SDF-1/CXCL12, respectively [30].
Poor perfusion also contributes to retinopathy of prematurity (ROP). ROP is a side effect resulting from oxygen therapy for premature infants and starts with rapid obliteration of retinal microvessels upon oxygen exposure. When patients are returned to ambient room air, poor perfusion resulting from significant microvessel losses leads to retinal tissue hypoxia and activates angiogenesis. However, both the quality and spatial location of the resultant microvessels are abnormal: they are unstable and leaky due to failed recruitment of pericytes, and are often present as protrusions into the vitreous cavity. These abnormalities suggest that even though hypoxia can be an inducer of normal angiogenesis, it can also be an inducer of abnormal neoangiogenesis. The exact reasons behind these differential effects are not well understood, but different levels of oxygen deficiency and specific tissue environments might be contributing factors.
The mechanisms underlying ROP have been studied extensively in mice. Excessive induction of VEGF-A expression is undoubtedly important [2, 86], but erythropoietin also plays a significant role [75]. Recently, it has been shown that suppression of PHD activities with chemical inhibitors may reduce capillary loss during oxygen treatment [94]. Another promising approach is to promote the recruitment of circulatory endothelial progenitor cells during oxygen treatment, so that capillary damage by oxygen can be repaired in a timely fashion. In mouse ROP models, delivery of exogenous insulin-like growth factor (IGF)-binding protein (IGFBP)-3 protected retinal vessels by pericyte recruitment [10], whereas knockout of the Igfbp-3 gene worsened capillary loss in the retina [62].
Angiogenesis due to other genetic and pathological events
Individuals carrying germline mutation in one of the VHL alleles are highly susceptible to a second VHL mutation in somatic cells, resulting in the development of benign vascular tumors such as hemangioblastomas in the central nervous system [63]. Although vascular tumors are generally benign, excessive proliferation of leaky retinal blood vessels can lead to blindness. In addition to vascular tumors, VHL deficiency is associated with several other tumor types such as renal cell carcinoma and pheochromocytoma, which are highly malignant [63]. VHL point mutation is also associated with polycythemia [63]. Vascular diseases due to PHD mutation have not been reported; however, PHD2 mutation is also associated with polycythemia [82, 83].
Hyperglycemia in diabetic patients also significantly modifies vascular properties and trigger retinopathy. Initially, microvessel damages occur due to hyperglycemia-induced apoptosis of capillary pericytes and endothelial cells, resulting in poor perfusion and retinal tissue hypoxia [20]. Large amounts of vasoactive molecules such as VEGF-A are induced by HIFs which accumulate in hypoxic retinal tissues and initiate angiogenesis, resulting in the formation of abnormal microvessels that are leaky and tortuous due to lack of pericyte association [1].
The relationship between diabetes and angiogenesis is complicated. Even though hyperglycemia may trigger neoangiogenesis by first damaging existing blood vessels and therefore result in tissue hypoxia, elevated levels of reactive oxygen species under diabetic conditions may hinder angiogenesis by disruptive modification of HIF-1α [5, 9]. Such complications may contribute to poor angiogenesis in diabetic foot ulcers.
Concluding remarks
PHD-dependent hydroxylation of HIF-α subunits and their consequent degradation is probably the most fundamental mechanism responsible for the maintenance of the quiescent status of adult blood vessels. A corollary of this statement is that HIF-α accumulation due to reduced PHD hydroxylase activity in hypoxic tissues is probably the most common trigger of angiogenesis. These conclusions are supported by a large number of studies indicating that HIF deficiency significantly interferes with angiogenesis whereas excessive accumulation of HIF-α due to PHD2 deficiency promotes angiogenesis. Different PHD and HIF-α isoforms are differentially involved in angiogenesis. Among all three PHDs, PHD2 is most critically involved in angiogenesis due to the fact that it is the most abundantly expressed isoform. On the other hand, conditions other than PHD hydroxylase activity, such as loss of p53, may also promote HIF-α accumulation and angiogenesis. As with PHD isoforms, different HIF-α isoforms may also have non-identical roles, although partially overlapping functions are also likely. HIF-1α is the most broadly expressed isoform and has a major role in mediating paracrine mechanisms of angiogenesis, whereas HIF-2α plays a major role in endothelial cells by activating the expression of endothelial cell receptors for angiogenic factors. However, roles of HIF-2α in non-endothelial cells and role of HIF-1α in endothelial cells have also been reported [88, 106]. Another level of complication is differential consequences of HIF-α accumulation in different tissues, with the formation of normal and healthy blood vessels in some tissues but unstable and leaky vessels in others. Thus, detailed investigation for the role of HIF-α in different tissues will be important to aid the development of effective angiogenesis (or anti-angiogenesis) therapies.
References
Aiello LP, Avery RL, Arrigg PG, Keyt BA, Jampel HD, Shah ST, Pasquale LR, Thieme H, Iwamoto MA, Park JE et al (1994) Vascular endothelial growth factor in ocular fluid of patients with diabetic retinopathy and other retinal disorders. N Engl J Med 331:1480–1487
Aiello LP, Pierce EA, Foley ED, Takagi H, Chen H, Riddle L, Ferrara N, King GL, Smith LE (1995) Suppression of retinal neovascularization in vivo by inhibition of vascular endothelial growth factor (VEGF) using soluble VEGF-receptor chimeric proteins. Proc Natl Acad Sci U S A 92:10457–10461
Appelhoff RJ, Tian YM, Raval RR, Turley H, Harris AL, Pugh CW, Ratcliffe PJ, Gleadle JM (2004) Differential function of the prolyl hydroxylases PHD1, PHD2, and PHD3 in the regulation of hypoxia-inducible factor. J Biol Chem 279:38458–38465
Berra E, Benizri E, Ginouves A, Volmat V, Roux D, Pouyssegur J (2003) HIF prolyl-hydroxylase 2 is the key oxygen sensor setting low steady-state levels of HIF-1alpha in normoxia. Embo J 22:4082–4090
Botusan IR, Sunkari VG, Savu O, Catrina AI, Grunler J, Lindberg S, Pereira T, Yla-Herttuala S, Poellinger L, Brismar K et al (2008) Stabilization of HIF-1alpha is critical to improve wound healing in diabetic mice. Proc Natl Acad Sci U S A 105:19426–19431
Bruick RK, McKnight SL (2001) A conserved family of prolyl-4-hydroxylases that modify HIF. Science 294:1337–1340
Brunelle JK, Bell EL, Quesada NM, Vercauteren K, Tiranti V, Zeviani M, Scarpulla RC, Chandel NS (2005) Oxygen sensing requires mitochondrial ROS but not oxidative phosphorylation. Cell Metab 1:409–414
Burke-Gaffney A, Brooks AV, Bogle RG (2002) Regulation of chemokine expression in atherosclerosis. Vascul Pharmacol 38:283–292
Ceradini DJ, Yao D, Grogan RH, Callaghan MJ, Edelstein D, Brownlee M, Gurtner GC (2008) Decreasing intracellular superoxide corrects defective ischemia-induced new vessel formation in diabetic mice. J Biol Chem 283:10930–10938
Chang KH, Chan-Ling T, McFarland EL, Afzal A, Pan H, Baxter LC, Shaw LC, Caballero S, Sengupta N, Li Calzi S et al (2007) IGF binding protein-3 regulates hematopoietic stem cell and endothelial precursor cell function during vascular development. Proc Natl Acad Sci U S A 104:10595–10600
Clinton SK, Underwood R, Hayes L, Sherman ML, Kufe DW, Libby P (1992) Macrophage colony-stimulating factor gene expression in vascular cells and in experimental and human atherosclerosis. Am J Pathol 140:301–316
Compernolle V, Brusselmans K, Acker T, Hoet P, Tjwa M, Beck H, Plaisance S, Dor Y, Keshet E, Lupu F et al (2002) Loss of HIF-2alpha and inhibition of VEGF impair fetal lung maturation, whereas treatment with VEGF prevents fatal respiratory distress in premature mice. Nat Med 8:702–710
Corley KM, Taylor CJ, Lilly B (2005) Hypoxia-inducible factor 1alpha modulates adhesion, migration, and FAK phosphorylation in vascular smooth muscle cells. J Cell Biochem 96:971–985
Coulet F, Nadaud S, Agrapart M, Soubrier F (2003) Identification of hypoxia-response element in the human endothelial nitric-oxide synthase gene promoter. J Biol Chem 278:46230–46240
Covello KL, Kehler J, Yu H, Gordan JD, Arsham AM, Hu CJ, Labosky PA, Simon MC, Keith B (2006) HIF-2alpha regulates Oct-4: effects of hypoxia on stem cell function, embryonic development, and tumor growth. Genes Dev 20:557–570
D'Angelo G, Duplan E, Boyer N, Vigne P, Frelin C (2003) Hypoxia up-regulates prolyl hydroxylase activity: a feedback mechanism that limits HIF-1 responses during reoxygenation. J Biol Chem 278:38183–38187
del Peso L, Castellanos MC, Temes E, Martin-Puig S, Cuevas Y, Olmos G, Landazuri MO (2003) The von Hippel Lindau/hypoxia-inducible factor (HIF) pathway regulates the transcription of the HIF-proline hydroxylase genes in response to low oxygen. J Biol Chem 278:48690–48695
Duan LJ, Zhang-Benoit Y, Fong GH (2005) Endothelium-intrinsic requirement for Hif-2alpha during vascular development. Circulation 111:2227–2232
Dvorak HF, Brown LF, Detmar M, Dvorak AM (1995) Vascular permeability factor/vascular endothelial growth factor, microvascular hyperpermeability, and angiogenesis. Am J Pathol 146:1029–1039
Ejaz S, Chekarova I, Ejaz A, Sohail A, Lim CW (2008) Importance of pericytes and mechanisms of pericyte loss during diabetes retinopathy. Diabetes Obes Metab 10:53–63
Elson DA, Thurston G, Huang LE, Ginzinger DG, McDonald DM, Johnson RS, Arbeit JM (2001) Induction of hypervascularity without leakage or inflammation in transgenic mice overexpressing hypoxia-inducible factor-1alpha. Genes Dev 15:2520–2532
Ema M, Taya S, Yokotani N, Sogawa K, Matsuda Y, Fujii-Kuriyama Y (1997) A novel bHLH-PAS factor with close sequence similarity to hypoxia-inducible factor 1alpha regulates the VEGF expression and is potentially involved in lung and vascular development. Proc Natl Acad Sci U S A 94:4273–4278
Epstein AC, Gleadle JM, McNeill LA, Hewitson KS, O'Rourke J, Mole DR, Mukherji M, Metzen E, Wilson MI, Dhanda A et al (2001) C. elegans EGL-9 and mammalian homologs define a family of dioxygenases that regulate HIF by prolyl hydroxylation. Cell 107:43–54
Firestein GS (1999) Starving the synovium: angiogenesis and inflammation in rheumatoid arthritis. J Clin Invest 103:3–4
Foo SS, Turner CJ, Adams S, Compagni A, Aubyn D, Kogata N, Lindblom P, Shani M, Zicha D, Adams RH (2006) Ephrin-B2 controls cell motility and adhesion during blood-vessel-wall assembly. Cell 124:161–173
Forsythe JA, Jiang BH, Iyer NV, Agani F, Leung SW, Koos RD, Semenza GL (1996) Activation of vascular endothelial growth factor gene transcription by hypoxia-inducible factor 1. Mol Cell Biol 16:4604–4613
Gerber HP, Condorelli F, Park J, Ferrara N (1997) Differential transcriptional regulation of the two vascular endothelial growth factor receptor genes. Flt-1, but not Flk-1/KDR, is up-regulated by hypoxia. J Biol Chem 272:23659–23667
Gnarra JR, Ward JM, Porter FD, Wagner JR, Devor DE, Grinberg A, Emmert-Buck MR, Westphal H, Klausner RD, Linehan WM (1997) Defective placental vasculogenesis causes embryonic lethality in VHL-deficient mice. Proc Natl Acad Sci U S A 94:9102–9107
Goetze JP, Gore A, Moller CH, Steinbruchel DA, Rehfeld JF, Nielsen LB (2004) Acute myocardial hypoxia increases BNP gene expression. Faseb J 18:1928–1930
Grunewald M, Avraham I, Dor Y, Bachar-Lustig E, Itin A, Jung S, Chimenti S, Landsman L, Abramovitch R, Keshet E (2006) VEGF-induced adult neovascularization: recruitment, retention, and role of accessory cells. Cell 124:175–189
Guzy RD, Hoyos B, Robin E, Chen H, Liu L, Mansfield KD, Simon MC, Hammerling U, Schumacker PT (2005) Mitochondrial complex III is required for hypoxia-induced ROS production and cellular oxygen sensing. Cell Metab 1:401–408
Haase VH, Glickman JN, Socolovsky M, Jaenisch R (2001) Vascular tumors in livers with targeted inactivation of the von Hippel–Lindau tumor suppressor. Proc Natl Acad Sci U S A 98:1583–1588
Hagen T, Taylor CT, Lam F, Moncada S (2003) Redistribution of intracellular oxygen in hypoxia by nitric oxide: effect on HIF1alpha. Science (New York, N. Y.) 302:1975–1978
Heidbreder M, Frohlich F, Johren O, Dendorfer A, Qadri F, Dominiak P (2003) Hypoxia rapidly activates HIF-3alpha mRNA expression. Faseb J 17:1541–1543
Heinl-Green A, Radke PW, Munkonge FM, Frass O, Zhu J, Vincent K, Geddes DM, Alton EW (2005) The efficacy of a 'master switch gene' HIF-1alpha in a porcine model of chronic myocardial ischaemia. Eur Heart J 26:1327–1332
Heinrich SA, Messingham KA, Gregory MS, Colantoni A, Ferreira AM, Dipietro LA, Kovacs EJ (2003) Elevated monocyte chemoattractant protein-1 levels following thermal injury precede monocyte recruitment to the wound site and are controlled, in part, by tumor necrosis factor-alpha. Wound Repair Regen 11:110–119
Hirsila M, Koivunen P, Gunzler V, Kivirikko KI, Myllyharju J (2003) Characterization of the human prolyl 4-hydroxylases that modify the hypoxia-inducible factor. J Biol Chem 278:30772–30780
Hitchon C, Wong K, Ma G, Reed J, Lyttle D, El-Gabalawy H (2002) Hypoxia-induced production of stromal cell-derived factor 1 (CXCL12) and vascular endothelial growth factor by synovial fibroblasts. Arthritis Rheum 46:2587–2597
Hu CJ, Wang LY, Chodosh LA, Keith B, Simon MC (2003) Differential roles of hypoxia-inducible factor 1alpha (HIF-1alpha) and HIF-2alpha in hypoxic gene regulation. Mol Cell Biol 23:9361–9374
Huang LE, Gu J, Schau M, Bunn HF (1998) Regulation of hypoxia-inducible factor 1alpha is mediated by an O2-dependent degradation domain via the ubiquitin-proteasome pathway. Proc Natl Acad Sci U S A 95:7987–7992
Isner JM (1999) Cancer and atherosclerosis: the broad mandate of angiogenesis. Circulation 99:1653–1655
Ivan M, Haberberger T, Gervasi DC, Michelson KS, Gunzler V, Kondo K, Yang H, Sorokina I, Conaway RC, Conaway JW et al (2002) Biochemical purification and pharmacological inhibition of a mammalian prolyl hydroxylase acting on hypoxia-inducible factor. Proc Natl Acad Sci U S A 99:13459–13464
Iyer NV, Kotch LE, Agani F, Leung SW, Laughner E, Wenger RH, Gassmann M, Gearhart JD, Lawler AM, Yu AY et al (1998) Cellular and developmental control of O2 homeostasis by hypoxia-inducible factor 1 alpha. Genes Dev 12:149–162
Jaakkola P, Mole DR, Tian YM, Wilson MI, Gielbert J, Gaskell SJ, Kriegsheim A, Hebestreit HF, Mukherji M, Schofield CJ et al (2001) Targeting of HIF-alpha to the von Hippel-Lindau ubiquitylation complex by O2-regulated prolyl hydroxylation. Science 292:468–472
Jansen PL, Rosch R, Jansen M, Binnebosel M, Junge K, Alfonso-Jaume A, Klinge U, Lovett DH, Mertens PR (2007) Regulation of MMP-2 gene transcription in dermal wounds. J Invest Dermatol 127:1762–1767
Jiang BH, Rue E, Wang GL, Roe R, Semenza GL (1996) Dimerization, DNA binding, and transactivation properties of hypoxia-inducible factor 1. J Biol Chem 271:17771–17778
Kaelin WG Jr (2005) ROS: really involved in oxygen sensing. Cell Metab 1:357–358
Kappel A, Ronicke V, Damert A, Flamme I, Risau W, Breier G (1999) Identification of vascular endothelial growth factor (VEGF) receptor-2 (Flk-1) promoter/enhancer sequences sufficient for angioblast and endothelial cell-specific transcription in transgenic mice. Blood 93:4284–4292
Kelly BD, Hackett SF, Hirota K, Oshima Y, Cai Z, Berg-Dixon S, Rowan A, Yan Z, Campochiaro PA, Semenza GL (2003) Cell type-specific regulation of angiogenic growth factor gene expression and induction of angiogenesis in nonischemic tissue by a constitutively active form of hypoxia-inducible factor 1. Circ Res 93:1074–1081
Kim WY, Safran M, Buckley MR, Ebert BL, Glickman J, Bosenberg M, Regan M, Kaelin WG Jr (2006) Failure to prolyl hydroxylate hypoxia-inducible factor alpha phenocopies VHL inactivation in vivo. Embo J 25:4650–4662
Koivunen P, Tiainen P, Hyvarinen J, Williams KE, Sormunen R, Klaus SJ, Kivirikko KI, Myllyharju J (2007) An endoplasmic reticulum transmembrane prolyl 4-hydroxylase is induced by hypoxia and acts on hypoxia-inducible factor alpha. J Biol Chem 282:30544–30552
Koponen JK, Kekarainen T, Heinonen SE, Laitinen A, Nystedt J, Laine J, Yla-Herttuala S (2007) Umbilical cord blood-derived progenitor cells enhance muscle regeneration in mouse hindlimb ischemia model. Mol Ther 15:2172–2177
Lando D, Peet DJ, Gorman JJ, Whelan DA, Whitelaw ML, Bruick RK (2002) FIH-1 is an asparaginyl hydroxylase enzyme that regulates the transcriptional activity of hypoxia-inducible factor. Genes Dev 16:1466–1471
Lanner MC, Raper M, Pratt WM, Rhoades RA (2005) Heterotrimeric G proteins and the platelet-derived growth factor receptor-beta contribute to hypoxic proliferation of smooth muscle cells. Am J Respir Cell Mol Biol 33:412–419
Laughner E, Taghavi P, Chiles K, Mahon PC, Semenza GL (2001) HER2 (neu) signaling increases the rate of hypoxia-inducible factor 1alpha (HIF-1alpha) synthesis: novel mechanism for HIF-1-mediated vascular endothelial growth factor expression. Mol Cell Biol 21:3995–4004
Lee S, Chen TT, Barber CL, Jordan MC, Murdock J, Desai S, Ferrara N, Nagy A, Roos KP, Iruela-Arispe ML (2007) Autocrine VEGF signaling is required for vascular homeostasis. Cell 130:691–703
Lee SH, Wolf PL, Escudero R, Deutsch R, Jamieson SW, Thistlethwaite PA (2000) Early expression of angiogenesis factors in acute myocardial ischemia and infarction. N Engl J Med 342:626–633
Lee YM, Jeong CH, Koo SY, Son MJ, Song HS, Bae SK, Raleigh JA, Chung HY, Yoo MA, Kim KW (2001) Determination of hypoxic region by hypoxia marker in developing mouse embryos in vivo: a possible signal for vessel development. Dev Dyn 220:175–186
Li J, Post M, Volk R, Gao Y, Li M, Metais C, Sato K, Tsai J, Aird W, Rosenberg RD et al (2000) PR39, a peptide regulator of angiogenesis. Nat Med 6:49–55
Lim JH, Lee ES, You HJ, Lee JW, Park JW, Chun YS (2004) Ras-dependent induction of HIF-1alpha785 via the Raf/MEK/ERK pathway: a novel mechanism of Ras-mediated tumor promotion. Oncogene 23:9427–9431
Loberg RD, Vesely E, Brosius FC 3rd (2002) Enhanced glycogen synthase kinase-3beta activity mediates hypoxia-induced apoptosis of vascular smooth muscle cells and is prevented by glucose transport and metabolism. J Biol Chem 277:41667–41673
Lofqvist C, Chen J, Connor KM, Smith AC, Aderman CM, Liu N, Pintar JE, Ludwig T, Hellstrom A, Smith LE (2007) IGFBP3 suppresses retinopathy through suppression of oxygen-induced vessel loss and promotion of vascular regrowth. Proc Natl Acad Sci U S A 104:10589–10594
Maher ER, Kaelin WG Jr (1997) von Hippel–Lindau disease. Medicine (Baltimore) 76:381–391
Mahon PC, Hirota K, Semenza GL (2001) FIH-1: a novel protein that interacts with HIF-1alpha and VHL to mediate repression of HIF-1 transcriptional activity. Genes Dev 15:2675–2686
Makino Y, Cao R, Svensson K, Bertilsson G, Asman M, Tanaka H, Cao Y, Berkenstam A, Poellinger L (2001) Inhibitory PAS domain protein is a negative regulator of hypoxia-inducible gene expression. Nature 414:550–554
Makino Y, Uenishi R, Okamoto K, Isoe T, Hosono O, Tanaka H, Kanopka A, Poellinger L, Haneda M, Morimoto C (2007) Transcriptional up-regulation of inhibitory PAS domain protein gene expression by hypoxia-inducible factor 1 (HIF-1): a negative feedback regulatory circuit in HIF-1-mediated signaling in hypoxic cells. J Biol Chem 282:14073–14082
Maltepe E, Schmidt JV, Baunoch D, Bradfield CA, Simon MC (1997) Abnormal angiogenesis and responses to glucose and oxygen deprivation in mice lacking the protein ARNT. Nature 386:403–407
Marti HH, Risau W (1998) Systemic hypoxia changes the organ-specific distribution of vascular endothelial growth factor and its receptors. Proc Natl Acad Sci U S A 95:15809–15814
Martin P, Leibovich SJ (2005) Inflammatory cells during wound repair: the good, the bad and the ugly. Trends Cell Biol 15:599–607
Masson N, Willam C, Maxwell PH, Pugh CW, Ratcliffe PJ (2001) Independent function of two destruction domains in hypoxia-inducible factor-alpha chains activated by prolyl hydroxylation. Embo J 20:5197–5206
Matsushita H, Morishita R, Nata T, Aoki M, Nakagami H, Taniyama Y, Yamamoto K, Higaki J, Yasufumi K, Ogihara T (2000) Hypoxia-induced endothelial apoptosis through nuclear factor-kappaB (NF-kappaB)-mediated bcl-2 suppression: in vivo evidence of the importance of NF-kappaB in endothelial cell regulation. Circ Res 86:974–981
Maxwell PH, Wiesener MS, Chang GW, Clifford SC, Vaux EC, Cockman ME, Wykoff CC, Pugh CW, Maher ER, Ratcliffe PJ (1999) The tumour suppressor protein VHL targets hypoxia-inducible factors for oxygen-dependent proteolysis. Nature 399:271–275
Maynard MA, Qi H, Chung J, Lee EH, Kondo Y, Hara S, Conaway RC, Conaway JW, Ohh M (2003) Multiple splice variants of the human HIF-3 alpha locus are targets of the von Hippel-Lindau E3 ubiquitin ligase complex. J Biol Chem 278:11032–11040
Metzen E, Stiehl DP, Doege K, Marxsen JH, Hellwig-Burgel T, Jelkmann W (2005) Regulation of the prolyl hydroxylase domain protein 2 (phd2/egln-1) gene: identification of a functional hypoxia-responsive element. Biochem J 387:711–717
Morita M, Ohneda O, Yamashita T, Takahashi S, Suzuki N, Nakajima O, Kawauchi S, Ema M, Shibahara S, Udono T et al (2003) HLF/HIF-2alpha is a key factor in retinopathy of prematurity in association with erythropoietin. Embo J 22:1134–1146
Moulton KS, Vakili K, Zurakowski D, Soliman M, Butterfield C, Sylvin E, Lo KM, Gillies S, Javaherian K, Folkman J (2003) Inhibition of plaque neovascularization reduces macrophage accumulation and progression of advanced atherosclerosis. Proc Natl Acad Sci U S A 100:4736–4741
Murohara T, Witzenbichler B, Spyridopoulos I, Asahara T, Ding B, Sullivan A, Losordo DW, Isner JM (1999) Role of endothelial nitric oxide synthase in endothelial cell migration. Arterioscler Thromb Vasc Biol 19:1156–1161
Nahrendorf M, Swirski FK, Aikawa E, Stangenberg L, Wurdinger T, Figueiredo JL, Libby P, Weissleder R, Pittet MJ (2007) The healing myocardium sequentially mobilizes two monocyte subsets with divergent and complementary functions. J Exp Med 204:3037–3047
Pajusola K, Kunnapuu J, Vuorikoski S, Soronen J, Andre H, Pereira T, Korpisalo P, Yla-Herttuala S, Poellinger L, Alitalo K (2005) Stabilized HIF-1alpha is superior to VEGF for angiogenesis in skeletal muscle via adeno-associated virus gene transfer. Faseb J 19:1365–1367
Pan Y, Mansfield KD, Bertozzi CC, Rudenko V, Chan DA, Giaccia AJ, Simon MC (2007) Multiple factors affecting cellular redox status and energy metabolism modulate hypoxia-inducible factor prolyl hydroxylase activity in vivo and in vitro. Mol Cell Biol 27:912–925
Peng J, Zhang L, Drysdale L, Fong GH (2000) The transcription factor EPAS-1/hypoxia-inducible factor 2alpha plays an important role in vascular remodeling. Proc Natl Acad Sci U S A 97:8386–8391
Percy MJ, Furlow PW, Beer PA, Lappin TR, McMullin MF, Lee FS (2007) A novel erythrocytosis-associated PHD2 mutation suggests the location of a HIF binding groove. Blood 110:2193–2196
Percy MJ, Zhao Q, Flores A, Harrison C, Lappin TR, Maxwell PH, McMullin MF, Lee FS (2006) A family with erythrocytosis establishes a role for prolyl hydroxylase domain protein 2 in oxygen homeostasis. Proc Natl Acad Sci U S A 103:654–659
Peters CL, Morris CJ, Mapp PI, Blake DR, Lewis CE, Winrow VR (2004) The transcription factors hypoxia-inducible factor 1alpha and Ets-1 colocalize in the hypoxic synovium of inflamed joints in adjuvant-induced arthritis. Arthritis Rheum 50:291–296
Phillips PG, Birnby LM, Narendran A (1995) Hypoxia induces capillary network formation in cultured bovine pulmonary microvessel endothelial cells. Am J Physiol 268:L789–L800
Pierce EA, Avery RL, Foley ED, Aiello LP, Smith LE (1995) Vascular endothelial growth factor/vascular permeability factor expression in a mouse model of retinal neovascularization. Proc Natl Acad Sci U S A 92:905–909
Rankin EB, Higgins DF, Walisser JA, Johnson RS, Bradfield CA, Haase VH (2005) Inactivation of the arylhydrocarbon receptor nuclear translocator (Arnt) suppresses von Hippel–Lindau disease-associated vascular tumors in mice. Mol Cell Biol 25:3163–3172
Rankin EB, Rha J, Unger TL, Wu CH, Shutt HP, Johnson RS, Simon MC, Keith B, Haase VH (2008) Hypoxia-inducible factor-2 regulates vascular tumorigenesis in mice. Oncogene 27:5354–5358
Ravi R, Mookerjee B, Bhujwalla ZM, Sutter CH, Artemov D, Zeng Q, Dillehay LE, Madan A, Semenza GL, Bedi A (2000) Regulation of tumor angiogenesis by p53-induced degradation of hypoxia-inducible factor 1alpha. Genes Dev 14:34–44
Reisz-Porszasz S, Probst MR, Fukunaga BN, Hankinson O (1994) Identification of functional domains of the aryl hydrocarbon receptor nuclear translocator protein (ARNT). Mol Cell Biol 14:6075–6086
Ryan HE, Lo J, Johnson RS (1998) HIF-1 alpha is required for solid tumor formation and embryonic vascularization. Embo J 17:3005–3015
Scortegagna M, Ding K, Oktay Y, Gaur A, Thurmond F, Yan LJ, Marck BT, Matsumoto AM, Shelton JM, Richardson JA et al (2003) Multiple organ pathology, metabolic abnormalities and impaired homeostasis of reactive oxygen species in Epas1-/- mice. Nat Genet 35:331–340
Scortegagna M, Ding K, Zhang Q, Oktay Y, Bennett MJ, Bennett M, Shelton JM, Richardson JA, Moe O, Garcia JA (2005) HIF-2alpha regulates murine hematopoietic development in an erythropoietin-dependent manner. Blood 105:3133–3140
Sears JE, Hoppe G, Ebrahem Q, Anand-Apte B (2008) Prolyl hydroxylase inhibition during hyperoxia prevents oxygen-induced retinopathy. Proc Natl Acad Sci U S A 105:19898–19903
Selak MA, Armour SM, MacKenzie ED, Boulahbel H, Watson DG, Mansfield KD, Pan Y, Simon MC, Thompson CB, Gottlieb E (2005) Succinate links TCA cycle dysfunction to oncogenesis by inhibiting HIF-alpha prolyl hydroxylase. Cancer Cell 7:77–85
Semenza GL, Wang GL (1992) A nuclear factor induced by hypoxia via de novo protein synthesis binds to the human erythropoietin gene enhancer at a site required for transcriptional activation. Mol Cell Biol 12:5447–5454
Sheares KK, Jeffery TK, Long L, Yang X, Morrell NW (2004) Differential effects of TGF-beta1 and BMP-4 on the hypoxic induction of cyclooxygenase-2 in human pulmonary artery smooth muscle cells. Am J Physiol Heart Circ Physiol 287:L919–L927
Shyu KG, Wang MT, Wang BW, Chang CC, Leu JG, Kuan P, Chang H (2002) Intramyocardial injection of naked DNA encoding HIF-1alpha/VP16 hybrid to enhance angiogenesis in an acute myocardial infarction model in the rat. Cardiovasc Res 54:576–583
Smith LM, Golub AS, Pittman RN (2002) Interstitial PO(2) determination by phosphorescence quenching microscopy. Microcirculation 9:389–395
Stempien-Otero A, Karsan A, Cornejo CJ, Xiang H, Eunson T, Morrison RS, Kay M, Winn R, Harlan J (1999) Mechanisms of hypoxia-induced endothelial cell death. Role of p53 in apoptosis. J Biol Chem 274:8039–8045
Stiehl DP, Wirthner R, Koditz J, Spielmann P, Camenisch G, Wenger RH (2006) Increased prolyl 4-hydroxylase domain proteins compensate for decreased oxygen levels. Evidence for an autoregulatory oxygen-sensing system. J Biol Chem 281:23482–23491
Stolze IP, Tian YM, Appelhoff RJ, Turley H, Wykoff CC, Gleadle JM, Ratcliffe PJ (2004) Genetic analysis of the role of the asparaginyl hydroxylase factor inhibiting hypoxia-inducible factor (HIF) in regulating HIF transcriptional target genes. J Biol Chem 279:42719–42725
Takeda K, Cowan A, Fong GH (2007) Essential role for prolyl hydroxylase domain protein 2 in oxygen homeostasis of the adult vascular system. Circulation 116:774–781
Takeda K, Ho VC, Takeda H, Duan LJ, Nagy A, Fong GH (2006) Placental but not heart defects are associated with elevated hypoxia-inducible factor alpha levels in mice lacking prolyl hydroxylase domain protein 2. Mol Cell Biol 26:8336–8346
Takeda N, Maemura K, Imai Y, Harada T, Kawanami D, Nojiri T, Manabe I, Nagai R (2004) Endothelial PAS domain protein 1 gene promotes angiogenesis through the transactivation of both vascular endothelial growth factor and its receptor, Flt-1. Circ Res 95:146–153
Tang N, Wang L, Esko J, Giordano FJ, Huang Y, Gerber HP, Ferrara N, Johnson RS (2004) Loss of HIF-1alpha in endothelial cells disrupts a hypoxia-driven VEGF autocrine loop necessary for tumorigenesis. Cancer Cell 6:485–495
Tian H, Hammer RE, Matsumoto AM, Russell DW, McKnight SL (1998) The hypoxia-responsive transcription factor EPAS1 is essential for catecholamine homeostasis and protection against heart failure during embryonic development. Genes Dev 12:3320–3324
Treins C, Giorgetti-Peraldi S, Murdaca J, Semenza GL, Van Obberghen E (2002) Insulin stimulates hypoxia-inducible factor 1 through a phosphatidylinositol 3-kinase/target of rapamycin-dependent signaling pathway. J Biol Chem 277:27975–27981
Trentin D, Hubbell J, Hall H (2005) Non-viral gene delivery for local and controlled DNA release. J Control Release 102:263–275
van Weel V, Seghers L, de Vries MR, Kuiper EJ, Schlingemann RO, Bajema IM, Lindeman JH, Delis-van Diemen PM, van Hinsbergh VW, van Bockel JH et al (2007) Expression of vascular endothelial growth factor, stromal cell-derived factor-1, and CXCR4 in human limb muscle with acute and chronic ischemia. Arterioscler Thromb Vasc Biol 27:1426–1432
Vincent KA, Shyu KG, Luo Y, Magner M, Tio RA, Jiang C, Goldberg MA, Akita GY, Gregory RJ, Isner JM (2000) Angiogenesis is induced in a rabbit model of hindlimb ischemia by naked DNA encoding an HIF-1alpha/VP16 hybrid transcription factor. Circulation 102:2255–2261
Vink A, Schoneveld AH, Lamers D, Houben AJ, van der Groep P, van Diest PJ, Pasterkamp G (2007) HIF-1alpha expression is associated with an atheromatous inflammatory plaque phenotype and upregulated in activated macrophages.
Warnecke C, Griethe W, Weidemann A, Jurgensen JS, Willam C, Bachmann S, Ivashchenko Y, Wagner I, Frei U, Wiesener M et al (2003) Activation of the hypoxia-inducible factor-pathway and stimulation of angiogenesis by application of prolyl hydroxylase inhibitors. Faseb J 17:1186–1188
Willam C, Masson N, Tian YM, Mahmood SA, Wilson MI, Bicknell R, Eckardt KU, Maxwell PH, Ratcliffe PJ, Pugh CW (2002) Peptide blockade of HIFalpha degradation modulates cellular metabolism and angiogenesis. Proc Natl Acad Sci U S A 99:10423–10428
Yamashita T, Ohneda K, Nagano M, Miyoshi C, Kaneko N, Miwa Y, Yamamoto M, Ohneda O, Fujii-Kuriyama Y (2008) Hypoxia-inducible transcription factor-2alpha in endothelial cells regulates tumor neovascularization through activation of ephrin A1. J Biol Chem 283:18926–18936
Yamashita T, Ohneda O, Nagano M, Iemitsu M, Makino Y, Tanaka H, Miyauchi T, Goto K, Ohneda K, Fujii-Kuriyama Y et al (2008) Abnormal heart development and lung remodeling in mice lacking the hypoxia-inducible factor-related basic helix-loop-helix PAS protein NEPAS. Mol Cell Biol 28:1285–1297
Zhao X, Lu X, Feng Q (2002) Deficiency in endothelial nitric oxide synthase impairs myocardial angiogenesis. Am J Physiol Heart Circ Physiol 283:H2371–2378
Zhong H, Chiles K, Feldser D, Laughner E, Hanrahan C, Georgescu MM, Simons JW, Semenza GL (2000) Modulation of hypoxia-inducible factor 1alpha expression by the epidermal growth factor/phosphatidylinositol 3-kinase/PTEN/AKT/FRAP pathway in human prostate cancer cells: implications for tumor angiogenesis and therapeutics. Cancer Res 60:1541–1545
Acknowledgment
The cost for the preparation of this manuscript was partially supported by grants from the American Heart Association and March of Dimes Foundation.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Fong, GH. Regulation of angiogenesis by oxygen sensing mechanisms. J Mol Med 87, 549–560 (2009). https://doi.org/10.1007/s00109-009-0458-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00109-009-0458-z