
Abstract
Purpose
Dysphagia is one of the most important treatment-related side effects in head and neck cancer (HNC), as it can lead to severe life-threating complications such as aspiration pneumonia and malnutrition. Intensity-modulated radiotherapy (IMRT) could reduce swallowing dysfunction by producing a concave dose distribution and reducing doses to the swallowing-related organs at risk (SWOARs). The aim of this study was to review the current literature in order to compare swallowing outcomes between IMRT and three-dimensional conformal radiotherapy (3DCRT).
Methods
A search was conducted in the PubMed and Embase databases to identify studies on swallowing outcomes, both clinically and/or instrumentally assessed, after 3DCRT and IMRT. Dysphagia-specific quality of life and objective instrumental data are summarized and discussed.
Results
A total of 262 papers were retrieved from the searched databases. An additional 23 papers were retrieved by hand-searching the reference lists. Ultimately, 22 papers were identified which discussed swallowing outcomes after 3DCRT and IMRT for HNC. No outcomes from randomized trials were identified.
Conclusion
Despite several methodological limitations, reports from the current literature seem to suggest better swallowing outcomes with IMRT compared to 3DCRT. Further improvements are likely to result from the increased use of IMRT plans optimized for SWOAR sparing.
Zusammenfassung
Hintergrund
Dysphagie ist eine der wichtigsten Nebenwirkungen bei der Behandlung von Kopf-Hals-Tumoren (HNC), da sie zu lebensbedrohlichen Komplikationen wie Aspirationspneumonien und Mangelernährung führen kann. Durch Erzeugung konkaver Dosisverteilungen und durch die Reduzierung der Dosis an schluckrelevanten Strukturen (SWOAR) kann die IMRT Schluckstörungen möglicherweise vermindern. Ziel dieser Studie war es, die gegenwärtige Literaturlage hinsichtlich der Schluckfunktion nach IMRT und konformaler dreidimensionaler Strahlentherapie (3DCRT) systematisch zu überprüfen.
Material und Methoden
Studien, die die Schluckfunktion nach 3DCRT und IMRT klinisch und/oder instrumentell untersuchten, wurden durch eine Datenbankrecherche in PubMed und Embase identifiziert. Schluckbezogene Lebensqualität und objektiv instrumentell erhobene Daten wurden zusammengefasst und diskutiert.
Ergebnisse
Insgesamt wurden 262 Manuskripte aus den Datenbanken extrahiert. Weitere 23 Manuskripte wurden durch manuelle Suche in den Literaturlisten ermittelt. Schließlich wurden 22 Arbeiten identifiziert, welche die Schluckfunktion nach 3DCRT und IMRT zum Gegenstand hatten. Darunter waren keine randomisierten Studien.
Schlussfolgerung
Trotz methodisch bedingter Einschränkungen der Aussagekraft dieser Analyse legt die gegenwärtige Literaturlage bessere Ergebnisse hinsichtlich der Schluckfunktion nach IMRT im Vergleich zu 3DCRT nahe. Weitere Verbesserungen werden wahrscheinlich durch die gezielte Optimierung von IMRT-Plänen hinsichtlich der SWOAR resultieren.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Due to the tumor location at the aerodigestive crossroad, patients frequently suffer from swallowing dysfunction and its potentially life-threating complications (i. e., aspiration pneumonia and malnutrition), which are caused by both primary cancer (baseline dysphagia) and cancer therapies (treatment-related dysphagia) [3,4,5].
Over the past decades, several organ-preservation protocols using a combination of chemotherapy (CT) and radiotherapy (RT) have been investigated. These have shown comparable oncologic results to radical surgery (i. e., total laryngectomy) but are associated with a high rate of treatment-related dysphagia [6, 7]. In fact, the recent publication of 10-year results of the Radiation Therapy Oncology Group (RTOG) 91-11 trial [8, 9] has revealed that concomitant radio-chemotherapy (RTCT) results in better locoregional control and laryngeal preservation than induction chemotherapy followed by RT alone, despite being hampered by a relevant rate (17 to 24%) of swallowing dysfunction that compromises patient nutritional status and quality of life. Historically, RT has always been burdened by a high rate of radiation-related dysphagia occurring in more than 50% of patients and often leading to aspiration pneumonia, pharyngo-esophageal strictures, and malnutrition status with long-term percutaneous endoscopic gastrostomy (PEG) tube dependence [3, 10,11,12]. Compared to three-dimensional conformal RT (3DCRT), several studies have suggested that intensity-modulated RT (IMRT) reduces the probability of swallowing dysfunction due to the fact that it can produce concave dose distributions with better avoidance of several critical dose-limiting structures, such as swallowing organs at risk (SWOARs), which might lead to better functional outcomes [13,14,15,16]. Swallowing disorders can be both clinically and/or instrumentally assessed. In this regard, clinical evaluation is usually performed using patient-reported questionnaires such as the M.D. Anderson Dysphagia Inventory (MDADI)—the sole questionnaire validated to specifically assess oropharyngeal dysphagia (OPD) [17]—and/or observer-rated toxicity scales such as the Common Toxicity Criteria for Adverse Events (CTCAE) or RTOG scales [18, 19]. Finally, objective instrumental assessment is usually provided using the videofluoroscopic swallowing study (VFSS) and/or fiberoptic endoscopic evaluation of swallowing (FEES) [20].
Unfortunately, the current data are inhomogeneous in terms of swallowing outcome due to several methodological issues as well as the different radiation techniques used (3DCRT and IMRT). Thus, the aim of this study was to review the current literature on posttreatment swallowing function in order to compare outcomes between 3DCRT and IMRT. For this purpose, we distinguished clinical and instrumental swallowing outcomes to allow a more homogeneous comparison of results.
Methods
A search of the PubMed and Embase databases for original articles published between 2000 and 2016 was performed. The Medical Subject Headings (MeSH) terms used were “head and neck cancer,” “squamous cell carcinoma,” “radiotherapy,” “radio-chemotherapy,” “intensity and modulated radiotherapy,” “swallowing dysfunction,” and “deglutition dysfunction.” Additional search terms included swallowing function, deglutition function, and dysphagia. Only English-language articles were included. The review articles retrieved were not included in the study but the reference lists in these articles, as well as those from other papers, were hand-searched for additional relevant publications. Two investigators (SU and DM) reviewed all the titles and abstracts for inclusion into the study. The review was performed systematically according to the PICO questions-based methodology as follows: P (population) = squamous head and neck cancers; I (intervention) = RT, RTCT, or RT-biotherapy with IMRT; C (comparison) = 3DCRT; O (outcome) = swallowing dysfunction [21].
The inclusion criteria were 1) prospective (presence of a baseline swallowing assessment) or retrospective (absence of a baseline swallowing assessment) studies which evaluated dysphagia after RT in HNC; 2) nasophaynx, oropharynx, larynx, hypopharynx, and oral cavity as primary sites; 3) RT, RTCT, or RT plus cetuximab with curative intent (±induction chemotherapy); 4) 3DCRT or IMRT treatment techniques; 5) clinical swallowing evaluation using dysphagia-specific quality of life measures and/or “gold-standard” objective instrumental assessment (VFSS and/or FEES) both early (within 3 months) and/or late (over 3 months) after treatment.
Papers were excluded if 1) prospective or retrospective trials were focused exclusively on patients who complained of dysphagia after treatment; 2) primary sites were different from the inclusion criteria; 3) postoperative or palliative RT or RTCT was performed; 3) surrogate or composite endpoints to evaluate dysphagia were used; 4) two-dimensional radiotherapy (2DRT) or hadrontherapy was performed; 4) non-English language. We also considered studies that included patients treated with both 3DCRT and IMRT (mixed treatment population); subsequently, these papers were excluded if it was not possible to analyze them separately and compare the swallowing outcomes between the two different techniques. Papers dealing with both clinical and instrumental assessment of dysphagia were analyzed separately for the different endpoints. Finally, papers where the swallowing outcomes were incompletely or partially reported because they were part of a wider acute or late toxicity category or health-related quality of life study were not considered.
This review was performed using studies with the primary aim of specifically assessing the oropharyngeal swallowing function (both clinically and/or instrumentally) after 3DCRT and/or IMRT.
Results
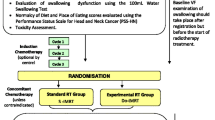
A total of 262 papers were retrieved from the search database. Of these, 172 papers were excluded based on their abstract and title. All 90 remaining full-text papers were retrieved and an additional 23 papers were retrieved by hand-searching relevant review articles. Thereafter, 91 papers were excluded based on the inclusion criteria and a total of 22 papers (eight 3DCRT, 11 IMRT, and three mixed 3DCRT/IMRT) were included in the final analysis (Fig. 1). All the included studies were published between 2000 and 2016. No randomized controlled trials were identified. All the reported trials were single-center experiences. Only three studies [22,23,24] focusing on a mixed-treatment population (3DCRT/IMRT) were included because it was possible to analyze the data separately and compare results on swallowing outcomes. Among the 22 studies included for the purpose of this review, 11 used only the instrumental swallowing assessment [25,26,27,28,29,30,31,32,33,34,35], three used only the clinical swallowing assessment [24, 36, 37], and eight combined clinical and instrumental assessments [22, 38,39,40,41,42,43,44]. Indeed, four of the 11 instrumental studies provided a combined clinical and instrumental swallowing assessment [29, 31, 32, 34], but their data on clinical evaluation were not considered for the purpose of this review because the questionnaires were inadequate in their reporting or inconsistent with our inclusion criteria. Of the 19 studies that provided an instrumental evaluation (both exclusively or combined with clinical questionnaires), all used VFSS except for three studies that used only FEES [38,39,40] and one study that combined VFSS and FEES [35].

Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of included studies. RT radiotherapy
Patient demographics
The total number of patients, patient age, gender, overall stage according to the American Joint Committee on Cancer, and swallowing evaluation method were extracted from the papers, where available, and are summarized in Table 1.
Median sample size was 24.5 patients (range 7–112; mean 38) for 3DCRT studies and 55 patients (range 7–300; mean 71) for IMRT; this difference was statistically significant (p < 0.0001).
Subjective clinical outcomes (intervention vs. comparison)
Among the 11 studies that reported a clinical assessment of OPD, four performed 3DCRT, five performed IMRT, and two performed mixed 3DCRT/IMRT treatments. Three out of the four 3DCRT studies (75%) as well as four out of the five IMRT studies (80%) provided a prospective evaluation of swallowing function; therefore, in both groups, only one study reported results on retrospective evaluation. A total of 143 patients (mean: 36; range: 14–71) were accrued in 3DCRT studies compared to 267 patients (mean: 53.4; range: 18–116) in IMRT studies. None of the 3DCRT studies were focused on a specific subsite, whereas four of the five IMRT studies were focused on a single subsite; overall, the oropharynx was the most frequently investigated subsite as it was included in eight out of the nine studies (89%). The MDADI was the most frequently used questionnaire, as it was employed in five of the nine studies with clinical assessment of OPD (two in the 3DCRT and three in the IMRT studies); in the other four studies, the use of dysphagia-reported questionnaires was extremely variable.
Results of the clinical swallowing assessment studies for 3DCRT are reported in Table 2.
A significant reduction of the MDADI composite score from pretreatment to 3 months posttreatment (76.6 vs. 59.4; p < 0.01) without a subsequent improvement from 3 months to 6 and 12 months was reported by Patterson et al. [39].
Contrastingly, data reported by Cartmill et al. [44] revealed a significant reduction of global and functional MDADI domain scores soon after treatment (4–6 weeks), followed by a subsequent significant improvement by 6 months in the global domain (p = 0.03). A similar pattern, although not statistically significant (p = 0.08), was reported for the other domains (especially for the functional and physical domains); no statistically significant difference resulted between baseline and 6‑months posttreatment scores. The study by Goguen et al. [43] reported an overall reduction in mean score for the swallowing-related questions of the FACT-H&N questionnaire. The retrospective data by Jensen et al. [40] on 35 patients reported an overall 83% pattern of some degree of dysphagia using European Organization Radiation Treatment Cancer (EORTC) H&N35 swallowing questionnaires.
Results of the clinical swallowing assessment studies for IMRT are reported in Table 3.
As shown in the study by Goepfert et al. [37], a significant reduction in the MDADI composite score was reported from baseline to 6 months posttreatment (from 88.3 to 73.8; p < 0.0001), followed by a slight subsequent improvement at 12 (73.8 vs. 78.6; p = 0.006) and 24 months (78.6 vs. 83.3; p < 0.0001), although at 2 years the score remained significantly decreased compared to baseline (p < 0.001). In addition, the authors reported a similar trend for MDADI subscale scores, which remained statistically reduced at 24 months compared to baseline values (emotional p = 0.008, functional p = 0.006, physical p < 0.001). In the prospective study by Lazaurus et al. [36], an overall significant worsening of swallowing function using MDADI, Eating Assessment Tool-10 (EAT-10), EORTC H&N, and Performance Status Scale for Head & Neck Cancer Patients (PSS-HN) questionnaires was reported. Similar to results reported by previous studies, the MDADI scores were found to be significantly reduced at 3 months (81.9 vs. 74.67), followed by a subsequent slight recovery at 6 months (74.67 vs. 79.28). Moreover, also for the EAT-10 questionnaire was the score found to be significantly higher at 3 months compared to pretreatment (4.39 vs. 11.18; p < 0.001), with a subsequent slight reduction at 6 months (11.18 vs. 7.18; p = 0.011), as it was for EORTC H&N scores (from 11.36 at baseline to 20.92 and 15.84 at 3 and 6 months, respectively; p = 0.057). For PSS-HN, there was an approximately 18 (p < 0.001) and 14% (p = 0.002) reduction in normalcy of diet domain from baseline to 3 and 6 months, respectively, whereas for the eating in public domain there was not a statistically significant difference at any of the time points (p = 0.270 and p = 0.326, respectively). Similarly, Schwartz et al. [42] reported significantly lower MDADI composite and global scores from baseline to all posttreatment intervals (p < 0.001), showing a significant reduction of values at 6 months (89.7 vs. 76.5 and 89.1 vs. 75.6, respectively), a slight recovery at 12 months (76.5 vs. 82.6 and 75.6 vs. 81.5, respectively), and an approximate stabilization at 24 months (82.6 vs. 84.8 and 81.5 vs. 82.4, respectively). Likewise, a similar trend was observed for the PSS-HN normalcy of diet subscale. Feng et al. [41] reported an acute worsening at 1 month posttreatment both for the Head and Neck Quality of Life Questionnaire (HNQOL) eating domain and University Washington Head and Neck Quality of Life Questionnaire (UWQOL) swallowing scores (10 vs. 43 and 8 vs. 39, respectively; p < 0.001), followed by a significant improvement over time at 6–12 months (p < 0.001) and then a stabilization at 24 months (p = 0.57). Finally, in the retrospective study by Patterson et al. [38], moderate swallowing impairment or activity restriction was reported in 27.8 and 11.1% of patients, respectively.
Data resulting from the 3DCRT/IMRT mixed population studies are shown in Table 4.
In the study by Kraaijenga et al. [22], patients treated with IMRT showed a significantly better swallowing function compared to 3DCRT for Swallowing Quality of Life Questionnaire (SWAL-QOL) scores, especially on the domains of food selection (p = 0.043), eating desire (p = 0.050), communication (p = 0.014), mental health (p = 0.014), and social function (p = 0.017). Similar results were reported by Kerr et al. [24] for PSS-HN scores, showing a significant difference in favor of IMRT and predicting no restriction vs. any restriction (100 vs. <75; odds ratio, OR, 0.164; p < 0.001). Regarding the eating in public domain at 12 and 24 months, 83 and 82% of IMRT survivors had no restrictions compared to 49 and 64% of 3DCRT survivors, respectively, whereas for the normalcy of diet domain, a difference in favor of IMRT was observed at 12 and 24 months, with 22 and 25% in the IMRT group without restriction compared to 7 and 5% in the 3DCRT group, respectively.
Objective instrumental outcomes (intervention vs. comparison)
Results of the instrumental swallowing assessment studies for the different radiation treatment techniques are reported in Table 5 and 6. Among the 19 studies that reported an instrumental assessment of OPD, eight performed 3DCRT, nine IMRT, and two mixed 3DCRT/IMRT treatments. Seven out of the eight 3DCRT studies (87.5%) provided a prospective evaluation of the swallowing function compared to five out of the nine IMRT studies (55.5%). A total of 214 patients (mean: 26.75; range: 12–71) were accrued in 3DCRT studies compared with a total of 707 patients (mean: 74.5; range: 14–300) in IMRT studies. In the 3DCRT studies, the oropharynx was the most frequently investigated subsite as it was enrolled in six out of eight studies (75%), followed by the hypopharynx and larynx that were enrolled in five studies (62.5%), and the nasopharynx and oral cavity in three studies (37.5%). In the IMRT studies, the oropharynx was the most frequently investigated subsite as it was enrolled in nine out of 11 studies (82%), followed by the nasopharynx and oral cavity in four studies (36%), and larynx and hypopharynx in three studies (27%).
Only one study [44] in both groups reported differentiated swallowing outcomes at different times of evaluation or for administration of different bolus consistencies.
Almost all the studies reported the postradiation swallowing outcome as the pattern of penetration and/or aspiration. Several also reported the percentage of pharyngeal residue [27, 28, 30, 35, 38, 40], whereas only few studies [34, 41,42,43] reported data on OPSE or SPSS videofluoroscopy-based scores. An overall range of 5–78% and 7–75% was reported for aspiration and penetration, respectively, in the 3DCRT studies, compared to a range of 2.6–26% and 11–35%, respectively, in the IMRT studies. Moreover, a rate of 2–88% of pharyngeal residue was reported after 3DCRT compared to 10–63% after IMRT. Finally, only four studies (one on 3DCRT and three on IMRT) reported data on specific swallowing rating tools such as SPSS or OPSE. As shown in Table 5 and 6, in the 3DCRT study [43], a mean SPSS score of 5 (indicating moderate dysfunction that required a modified diet and swallowing precautions to minimize risk of aspiration) was reported, compared to a score of 4 (indicating mild/moderate dysfunction) or 78% of patients with an SPSS score <3 (indicating normal swallowing or mild dysfunction) in the IMRT studies [34, 41, 43]. Additionally, the only study that used OPSE reported a reduction of 13.2 points after IMRT [42].
Data resulting from the mixed 3DCRT/IMRT population are presented in Table 4. As shown in the prospective study by Paulosky et al. [26], a statistically significant better swallowing outcome measured using the OPSE score was reported with IMRT compared to 3DCRT, both after liquid and paste bolus administration (p = 0.0003 and 0.018, respectively), as well as in terms of the percentage of pharyngeal residue (p = 0.005). Similarly, a lower pattern of aspirations (30 vs. 83%) was observed after IMRT compared with 3DCRT in the retrospective study by Kraaijenga et al. [22].
Discussion
This systematic review aimed to establish what evidence is currently available on better swallowing outcomes using IMRT rather than 3DCRT as part of a multidisciplinary organ-preservation treatment strategy in HNC patients. To our knowledge, this is the only review specifically focused on comparing the swallowing outcomes of these two treatment techniques. Previous reviews only aimed at exploring the potential effects of IMRT on swallowing performance and some concluded that there is limited evidence on this topic [45, 46].
Nevertheless, the rationale for using IMRT as a strategy to reduce posttreatment dysphagia has been well acknowledged based on the relationship between swallowing functional status and the pattern of radiation dose received by the swallowing related structures (SWOARs) such as pharyngeal constrictor muscles (superior, medium, and inferior), supraglottic and glottis larynx, and the esophageal inlet [47,48,49,50]. In addition, several authors [13, 51] have already discussed the potential for significant dosimetric improvements when SWOARs are explicitly considered in the IMRT plan optimization process (SWOAR-sparing IMRT) compared to standard IMRT, in order to maximally reduce irradiation of these structures and to achieve better swallowing outcomes. In this regard, computed tomography (CT)-based guidelines for delineation of the main swallowing structures have recently been published by Christianen et al. [52], to assist radiation oncologists in clinical practice as well as to facilitate comparison of results between different clinical studies. Therefore, we identified 22 papers (for a total of 1311 patients), heterogeneously in favor of IMRT but homogeneous in terms of the method of evaluation, which were relevant according to our inclusion criteria.
In almost all prospective clinical evaluation studies analyzed in this review, an overall worsening of the swallowing function from baseline to after treatment was shown, regardless of the RT techniques and questionnaires used. In the IMRT studies, a greater number of evaluation steps were performed compared to the situation with 3DCRT. These evaluation steps reported a significant swallowing impairment soon after treatment (between 1 to 3 months), followed by an improvement or stabilization (6 months), and a subsequent gradual recovery (between 12 to 24 months), although there was a persistence of values at levels lower than baseline. Indeed, a statistically significant benefit in favor of IMRT emerged from a direct comparison in the two mixed population studies, highlighting its ameliorative role in reducing subjectively reported swallowing impairment compared to standard techniques.
Regarding the instrumental evaluation studies, the results were extremely variable and difficult to compare, mainly due to the lack of well-defined and standardized score parameters, which made it difficult to draw firm conclusions.
Penetration and aspiration were the most frequently used parameters to measure the severity of posttreatment dysphagia, although results were rarely reported according to the standardized penetration-aspiration scale (PAS) [53]. Sometimes the authors did not distinguish between these occurrences (i. e., reporting a global rate of penetration/aspiration), making it difficult to interpret the data as their clinical relevance is different (“ab ingestis” pneumonia is associated with the occurrence of aspiration rather than penetration). Even so, the pattern of aspiration seemed to be significantly lower after IMRT than after 3DCRT, as most papers specifically reported a rate of 2.6–7% from IMRT compared to 7–78% after 3DCRT. Some studies reported results using pharyngeal residue, although the absence of standardized scores to quantify the amount of bolus retained in the pharynx limited the possibility to compare the effects of the two different techniques. In this regard, we do believe that pharyngeal residue, if properly quantified and combined with the pattern of aspiration, is a useful tool to assess postradiation dysphagia. It has been well recognized by previous authors [4, 54] that the greater the amount of bolus retention in the pharynx after the swallowing act (post-swallowing residue), the higher the probability of aspiration (post-swallowing aspiration). Nevertheless, similar to clinical studies, a significant benefit in favor of IMRT clearly emerged from the direct comparison of the two different techniques, both in terms of aspiration and pharyngeal residue, and in terms of functional parameters such as OPSE.
Overall, despite our strict inclusion criteria, the heterogeneity of the population studied (many studies focused on more than two HNC subsites), the different clinical swallowing questionnaires used, and the lack of standardized objective instrumental parameter scores, as well as the lack of standardization of the amount and consistency of the bolus administered and the high variability in the timings of the evaluations, were the major limitations for the comparison of the results. However, a considerable benefit of IMRT in preserving the swallowing function emerged in this review and we believe that its positive impact is likely to increase as radiation oncologists will be more and more encouraged to optimize treatment plans for the swallowing-related structures in their clinical practice.
Among the 13 IMRT studies that we considered for the intent of this review, seven performed only parotid-sparing [22, 26, 34, 38, 42], whereas six performed SWOAR-sparing IMRT [25, 31,32,33, 35, 41], though only few [33, 35, 41] clearly reported dosimetric constraints for swallowing-related structures in their protocol study. In this regard, authors mostly referred to previous studies [3, 49, 55] that retrospectively correlated the dose to SWOARs to the occurrence of life-threating dysphagia-related complications (i. e., aspiration pneumonia), and generally suggested mean doses to the constrictor muscles below 55 Gy and to the larynx below 48 Gy.
In our opinion, the study by the University of Michigan [41] best investigated the impact of an “intent-SWOAR-sparing IMRT,” albeit in a highly selected population (oropharyngeal cancers without infiltration of posterior pharyngeal wall and without lateral retropharyngeal node involvement), in terms of locoregional recurrence rates and functional preservation. These authors reported the safety of dose reduction to these structures together with a mild to moderate dysfunction (SPSS score 4) at 12 months after treatment. In this study, dosimetric goals for the swallowing structures were arbitrarily set at a maximum dose of 50 Gy outside the planning target volume (PTV) [47]. Hereafter, the subsequent dosimetric analysis on the same population by Eisbruch et al. [56] found a significant correlation between the dose received by the SWOARs and the occurrence of VFS-based aspirations, reporting a 50 and 25% risk for doses of 63 Gy and 56 Gy to the pharyngeal constrictors, and for doses of 56 Gy and 39 Gy to the supraglottic and glottic larynx, respectively.
From these studies, a recent group analysis on long-term (median follow-up 6.5 years) health-related quality of life in 40 oropharyngeal cancer patients (97.5% human papillomavirus, HPV, positive) reported no significant change of patient-reported dysphagia measured by both HNQOL and UWQOL swallowing questions compared with the assessment at 24 months after treatment [57]. Thus, further potential improvements are warranted and likely to be achieved with more rigorous application of the published CT SWOAR delineation guidelines by Christianen et al. [52].
Conclusion
The maximum benefit of IMRT in swallowing function preservation has still to be thoroughly investigated, such that well-designed prospective trials specifically focused on this relevant endpoint are strongly encouraged by a panel of experts [58]. These trials should provide a good RT quality control protocol for dose reduction to SWOARs and homogeneous clinical inclusion criteria based on the tumor subsite (i. e., in the superiorly sited tumors, the upper and middle constrictor muscles receive higher doses, whereas larynx and inferior muscle are more exposed to higher doses in the inferiorly sited tumors), together with an accurate dysphagia assessment protocol providing a clinical and/or uniform standardized instrumental evaluation itemizing the different consistencies and the amount of the bolus used in order to facilitate comparison of results.
As far as we know, the DARS trial [59] is the only ongoing multicenter randomized controlled trial to determine whether SWOAR-sparing IMRT will led to an improvement in long-term swallowing function compared with standard IMRT in locally advanced oropharyngeal cancers after RTCT, using the difference in mean MDADI composite score as the primary endpoint of the study.
In the meantime, we suggest taking the SWAORs into consideration in the plan optimization process, to maximally reduce irradiation without compromising target coverage, and to refer patients (mostly HPV-positive patients who are candidates for a RTCT curative treatment with a bilateral neck irradiation) to deglutologists for management and prevention of swallowing dysfunction, as recommended by current guidelines [60,61,62].
References
Marur S, Forastiere AA (2008) Head and neck cancer: changing epidemiology, diagnosis, and treatment. Mayo Clin Proc 83:489–501
Stambuk HE, Karimi S, Lee N, Patel SG (2007) Oral cavity and oropharynx tumors. Radiol Clin North Am 45:1–20
Caudell JJ, Schaner PE, Meredith RF, Locher JL, Nabell LM, Carroll WR et al (2009) Factors associated with long-term dysphagia after definitive radiotherapy for locally advanced head-and-neck cancer. Int J Radiat Oncol Biol Phys 73:410–415
Rosenthal DI, Lewin JS, Eisbruch A (2006) Prevention and treatment of dysphagia and aspiration after chemoradiation for head and neck cancer. J Clin Oncol 24:2636–2643
Robbins KT (2002) Barriers to winning the battle with head-and-neck cancer. Int J Radiat Oncol Biol Phys 53:4–5
Machtay M, Moughan J, Farach A, Martin-O’Meara E, Galvin J, Garden AS et al (2012) Hypopharyngeal dose is associated with severe late toxicity in locally advanced head-and-neck cancer: an RTOG analysis. Int J Radiat Oncol Biol Phys 84:983–989
Pignon JP, Bourhis J, Domenge C, Designé L (2000) Chemotherapy added to locoregional treatment for head and neck squamous-cell carcinoma: three meta-analyses of updated individual data. MACH-NC Collaborative Group. Meta-Analysis of Chemotherapy on Head and Neck Cancer. Lancet 355:949–955
Forastiere AA, Zhang Q, Weber RS, Maor MH, Goepfert H, Pajak TF et al (2013) Long-term results of RTOG 91–11: a comparison of three nonsurgical treatment strategies to preserve the larynx in patients with locally advanced larynx cancer. J Clin Oncol 31:845–852
Ward MC, Adelstein DJ, Bhateja P, Nwizu TI, Scharpf J, Houston N et al (2016) Severe late dysphagia and cause of death after concurrent chemoradiation for larynx cancer in patients eligible for RTOG 91–11. Oral Oncol 57:21–26
Nguyen NP, Sallah S, Karlsson U, Antoine JE (2002) Combined chemotherapy and radiation therapy for head and neck malignancies: quality of life issues. Cancer 94:1131–1141
Nguyen NP, Moltz CC, Frank C, Vos P, Smith HJ, Karlsson U et al (2004) Dysphagia following chemoradiation for locally advanced head and neck cancer. Ann Oncol 15:383–388
Batth SS, Caudell JJ, Chen AM (2014) Practical considerations in reducing swallowing dysfunction following concurrent chemoradiotherapy with intensity-modulated radiotherapy for head and neck cancer. Head Neck 36:291–298
Eisbruch A, Schwartz M, Rasch C, Vineberg K, Damen E, Van As CJ et al (2004) Dysphagia and aspiration after chemoradiotherapy for head-and-neck cancer: which anatomic structures are affected and can they be spared by IMRT? Int J Radiat Oncol Biol Phys 60:1425–1439
Mazzola R, Ferrera G, Alongi F, Mannino M, Abbate B, Cucchiara T et al (2015) Organ sparing and clinical outcome with step-and-shoot IMRT for head and neck cancer: a mono-institutional experience. Radiol Med 120:753–758
Levendag PC, Teguh DN, Voet P, van der Est H, Noever I, de Kruijf WJM et al (2007) Dysphagia disorders in patients with cancer of the oropharynx are significantly affected by the radiation therapy dose to the superior and middle constrictor muscle: a dose-effect relationship. Radiother Oncol 85:64–73
Bhide SA, Gulliford S, Kazi R, El-Hariry I, Newbold K, Harrington KJ et al (2009) Correlation between dose to the pharyngeal constrictors and patient quality of life and late dysphagia following chemo-IMRT for head and neck cancer. Radiother Oncol 93:539–544
Chen AY, Frankowski R, Bishop-Leone J, Hebert T, Leyk S, Lewin J et al (2001) The development and validation of a dysphagia-specific quality-of-life questionnaire for patients with head and neck cancer: the M. D. Anderson dysphagia inventory. Arch Otolaryngol Head Neck Surg 127:870–876
Cox JD, Stetz J, Pajak TF (1995) Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 31:1341–1346
Trotti A, Colevas AD, Setser A, Rusch V, Jaques D, Budach V et al (2003) CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 13:176–181
Speyer R (2013) Oropharyngeal dysphagia: screening and assessment. Otolaryngol Clin North Am 46:989–1008
Stone PW (2002) Popping the (PICO) question in research and evidence-based practice. Appl Nurs Res 15:197–198
Kraaijenga SAC, Oskam IM, van der Molen L, Hamming-Vrieze O, Hilgers FJM, van den Brekel MWM (2015) Evaluation of long term (10-years+) dysphagia and trismus in patients treated with concurrent chemo-radiotherapy for advanced head and neck cancer. Oral Oncol 51:787–794
Pauloski BR, Rademaker AW, Logemann JA, Lazarus CL, Newman L, Hamner A et al (2002) Swallow function and perception of dysphagia in patients with head and neck cancer. Head Neck 24:555–565
Kerr P, Myers CL, Butler J, Alessa M, Lambert P, Cooke AL (2015) Prospective functional outcomes in sequential population based cohorts of stage III/IV oropharyngeal carcinoma patients treated with 3D conformal vs. intensity modulated radiotherapy. J Otolaryngol Head Neck Surg 44:17
MD Anderson Head and Neck Cancer Symptom Working Group (2016) Beyond mean pharyngeal constrictor dose for beam path toxicity in non-target swallowing muscles: Dose-volume correlates of chronic radiation-associated dysphagia (RAD) after oropharyngeal intensity modulated radiotherapy. Radiother Oncol 118:304–314
Pauloski BR, Rademaker AW, Logemann JA, Discekici-Harris M, Mittal BB (2015) Comparison of swallowing function after intensity-modulated radiation therapy and conventional radiotherapy for head and neck cancer. Head Neck 37:1575–1582
Kotz T, Costello R, Li Y, Posner MR (2004) Swallowing dysfunction after chemoradiation for advanced squamous cell carcinoma of the head and neck. Head Neck 26:365–372
Maruo T, Fujimoto Y, Ozawa K, Hiramatsu M, Suzuki A, Nishio N et al (2014) Laryngeal sensation and pharyngeal delay time after (chemo)radiotherapy. Eur Arch Otorhinolaryngol 271:2299–2304
Ku PK, Yuen EH, Cheung DM, Chan BY, Ahuja A, Leung SF et al (2007) Early swallowing problems in a cohort of patients with nasopharyngeal carcinoma: Symptomatology and videofluoroscopic findings. Laryngoscope 117:142–146
Eisbruch A, Lyden T, Bradford CR, Dawson LA, Haxer MJ, Miller AE et al (2002) Objective assessment of swallowing dysfunction and aspiration after radiation concurrent with chemotherapy for head-and-neck cancer. Int J Radiat Oncol Biol Phys 53:23–28
Starmer HM, Tippett D, Webster K, Quon H, Jones B, Hardy S et al (2014) Swallowing outcomes in patients with oropharyngeal cancer undergoing organ-preservation treatment. Head Neck 36:1392–1397
Van der Molen L, Heemsbergen WD, de Jong R, van Rossum MA, Smeele LE, Rasch CRN et al (2013) Dysphagia and trismus after concomitant chemo-Intensity-Modulated Radiation Therapy (chemo-IMRT) in advanced head and neck cancer; dose-effect relationships for swallowing and mastication structures. Radiother Oncol 106:364–369
Kumar R, Madanikia S, Starmer H, Yang W, Murano E, Alcorn S et al (2014) Radiation dose to the floor of mouth muscles predicts swallowing complications following chemoradiation in oropharyngeal squamous cell carcinoma. Oral Oncol 50:65–70
Mortensen HR, Jensen K, Aksglæde K, Behrens M, Grau C (2013) Late dysphagia after IMRT for head and neck cancer and correlation with dose-volume parameters. Radiother Oncol 107:288–294
Ursino S, Seccia V, Cocuzza P, Ferrazza P, Briganti T, Matteucci F et al (2016) How does radiotherapy impact swallowing function in nasopharynx and oropharynx cancer? Short-term results of a prospective study. Acta Otorhinolaryngol Ital 36:174–184
Lazarus CL, Husaini H, Hu K, Culliney B, Li Z, Urken M et al (2014) Functional outcomes and quality of life after Chemoradiotherapy: baseline and 3 and 6 months post-treatment. Dysphagia 29:365–375
Goepfert RP, Lewin JS, Barrow MP, Fuller CD, Lai SY, Song J et al (2016) Predicting two-year longitudinal MD Anderson Dysphagia Inventory outcomes after intensity modulated radiotherapy for locoregionally advanced oropharyngeal carcinoma. Laryngoscope 127(4):842–848
Patterson M, Brain R, Chin R, Veivers D, Back M, Wignall A et al (2014) Functional swallowing outcomes in nasopharyngeal cancer treated with IMRT at 6 to 42 months post-radiotherapy. Dysphagia 29:663–670
Patterson JM, McColl E, Carding PN, Hildreth AJ, Kelly C, Wilson JA (2014) Swallowing in the first year after chemoradiotherapy for head and neck cancer: Clinician-and patient-reported outcomes. Head Neck 36:352–358
Jensen K, Lambertsen K, Grau C (2007) Late swallowing dysfunction and dysphagia after radiotherapy for pharynx cancer: frequency, intensity and correlation with dose and volume parameters. Radiother Oncol 85:74–82
Feng FY, Kim HM, Lyden TH, Haxer MJ, Worden FP, Feng M et al (2010) Intensity-modulated chemoradiotherapy aiming to reduce dysphagia in patients with oropharyngeal cancer: clinical and functional results. J Clin Oncol 28:2732–2738
Schwartz DL, Hutcheson K, Barringer D, Tucker SL, Kies M, Holsinger FC et al (2010) Candidate dosimetric predictors of long-term swallowing dysfunction following Oropharyngeal IMRT. Int J Radiat Oncol Biol Phys 78:1356–1365
Goguen LA, Posner MR, Norris CM, Tishler RB, Wirth LJ, Annino DJ et al (2006) Dysphagia after sequential chemoradiation therapy for advanced head and neck cancer. Otolaryngol Head Neck Surg 134:916–922
Cartmill B, Cornwell P, Ward E, Davidson W, Porceddu S (2012) A prospective investigation of swallowing, nutrition, and patient-rated functional impact following altered fractionation radiotherapy with concomitant boost for oropharyngeal cancer. Dysphagia 27:32–45
Roe JWG, Carding PN, Dwivedi RC, Kazi RA, Rhys-Evans PH, Harrington KJ et al (2010) Swallowing outcomes following Intensity Modulated Radiation Therapy (IMRT) for head & neck cancer – a systematic review. Oral Oncol 46:727–733
Frowen JJ, Perry AR (2006) Swallowing outcomes after radiotherapy for head and neck cancer: a systematic review. Head Neck 28:932–944
Feng FY, Kim HM, Lyden TH, Haxer MJ, Feng M, Worden FP et al (2007) Intensity-modulated radiotherapy of head and neck cancer aiming to reduce dysphagia: early dose-effect relationships for the swallowing structures. Int J Radiat Oncol Biol Phys 68:1289–1298
Dornfeld K, Simmons JR, Karnell L, Karnell M, Funk G, Yao M et al (2007) Radiation doses to structures within and adjacent to the larynx are correlated with long-term diet- and speech-related quality of life. Int J Radiat Oncol Biol Phys 68:750–757
Caglar HB, Tishler RB, Othus M, Burke E, Li Y, Goguen L et al (2008) Dose to larynx predicts for swallowing complications after intensity-modulated radiotherapy. Int J Radiat Oncol Biol Phys 72:1110–1118
Mendenhall WM, Amdur RJ, Morris CG, Kirwan JM, Li JG (2010) Intensity-modulated radiotherapy for oropharyngeal squamous cell carcinoma1. Laryngoscope 120:2218–2222
van der Laan HP, Christianen MEMC, Bijl HP, Schilstra C, Langendijk JA (2012) The potential benefit of swallowing sparing intensity modulated radiotherapy to reduce swallowing dysfunction: An in silico planning comparative study. Radiother Oncol 103:76–81
Christianen MEMC, Langendijk JA, Westerlaan HE, van de Water TA, Bijl HP (2011) Delineation of organs at risk involved in swallowing for radiotherapy treatment planning. Radiother Oncol 101:394–402
Rosenbek JC, Robbins JA, Roecker EB, Coyle JL, Wood JL (1996) A penetration-aspiration scale. Dysphagia 11:93–98
Hutcheson KA, Lewin JS, Barringer DA, Lisec A, Gunn GB, Moore MWS et al (2012) Late dysphagia after radiotherapy-based treatment of head and neck cancer. Cancer 118:5793–5799
Levendag PC, Teguh DN, Voet P, van der hest H, Noever I, de Kruijif WJM et al (2007) Dysphagia disorders in patients with cancer of the oropharynx are significantly affected by the radiation therapy dose to the superior and middle constrictor muscle: A dose-effect relationship. Radiother Oncol 85:64–73
Eisbruch A, Kim HM, Feng FY, Lyden TH, Haxer MJ, Feng M et al (2011) Chemo-IMRT of oropharyngeal cancer aiming to reduce dysphagia: Swallowing organs late complication probabilities and dosimetric correlates. Int J Radiat Oncol Biol Phys 81:e93–9
Vainshtein JN, Moon DH, Feng FY, Chepeha DB, Eisbruch A, Stenmark MH (2015) Long-term quality of life after swallowing and salivary-sparing chemo-intensity modulated radiation therapy in survivors of human Papillomavirus-related oropharyngeal cancer. Int J Radiat Oncol Biol Phys 91:925–933
Lefebvre JL, Ang KK (2009) Larynx preservation clinical trial design: key issues and recommendations – a consensus panel summary. Int J Radiat Oncol 73:1293–1303
Pektar I, Rooney K, Roe JWG, Patterson JM, Bernstein D, Tyler JM et al (2016) DARS: a phase III randomized multicentre study of dysphagia-optimised intensity-modulated radiotherapy (Do-IMRT) versus standard intensity-modulated radiotherapy (S-IMRT) in head and neck cancer. BMC Cancer 16:770
Russi EG, Corvò R, Merlotti A, Alterio D, Franco P, Pergolizzi S et al (2012) Swallowing dysfunction in head and neck cancer patients treated by radiotherapy: Review and recommendations of the supportive task group of the Italian Association of Radiation Oncology. Cancer Treat Rev 38:1033–1049
Schindler A, Denaro N, Russi EG, Pizzorni N, Bossi P, Merlotti A et al (2015) Dysphagia in head and neck cancer patients treated with radiotherapy and systemic therapies: Literature review and consensus. Crit Rev Oncol Hematol 96:372–384
NCCN Clinical Practice Guidelines in Oncology n. d. https://www.nccn.org/professionals/physician_gls/f_guidelines.asp#head-and-neck. Accessed 10.06.2017
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
S. Ursino, E. D’Angelo, R. Mazzola, A. Merlotti, R. Morganti, A. Cristaudo, F. Paiar, D. Musio, D. Alterio, A. Bacigalupo, and E.G. FRussiand. Lohr declare that they have no competing interests.
Rights and permissions
About this article

Cite this article
Ursino, S., D’Angelo, E., Mazzola, R. et al. A comparison of swallowing dysfunction after three-dimensional conformal and intensity-modulated radiotherapy. Strahlenther Onkol 193, 877–889 (2017). https://doi.org/10.1007/s00066-017-1160-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-017-1160-7