
Abstract
Concomitant chemoradiotherapy provides organ preservation for those patients with head and neck cancer. We report the results of a prospective study that examined functional outcomes and quality of life (QOL) after chemoradiotherapy over the first 6 months post-treatment (tx). Twenty-nine patients with head and neck cancer were treated with chemoradiotherapy. All were seen baseline and 3 and 6 months post-tx. Assessments included the performance status scale (PSS), Karnofsky performance status scale, tongue strength, jaw opening, and saliva weight. QOL was patient-rated using the eating assessment tool (EAT-10), MD Anderson dysphagia inventory, speech handicap index (SHI), and the EORTC H&N35 scale. Repeated-measures ANOVAs were used, with significance at p < 0.05. PSS scores were significantly different across time points. Tongue strength, jaw range of motion (ROM), and saliva weight were significantly lower at 3 and 6 months than at baseline. QOL was significantly worse after tx, although it improved by 6 months as rated with the EAT-10 and the SHI scores were significantly worse at 3 and 6 months. EORTC domains of swallowing, senses, speech, dry mouth, and sticky saliva were significantly worse at 3 and 6 months. Concomitant chemoradiotherapy for treatment of head and neck tumors can result in impaired performance outcomes and QOL over the first 6 months post-tx. However, performance status, tongue strength, jaw ROM, and eating QOL were only mildly impaired by 6 months post-tx. Saliva production and speech QOL remained significantly impaired at 6 months post-treatment. Current studies are examining outcomes at 12 and 24 months post-treatment to better predict outcomes over time in this population.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Patients undergoing primary chemoradiotherapy have been found to suffer from various oral complications after treatment that can include xerostomia, pain, mucositis, trismus, and reduced or altered taste sensation [1–3]. These impairments can result in reduced chewing ability, increased meal time, weight loss, dysphagia, aspiration, and reduced ability to eat a normal diet after treatment [4–6]. Oral impairments and their sequelae have been found to negatively affect quality of life [7–10]. Lingual strength has been found to be reduced after chemoradiotherapy to the head and neck, which can have a negative impact on the oral phase of swallowing and the ability to eat by mouth [11–13]. Speech and voice quality of life can become impaired following chemoradiotherapy to the head and neck [14–16]. Quality of life has been found to improve over the first 6 months post-treatment, although not to baseline levels of functioning [17, 18]. Oral outcomes of tongue strength, saliva production, and jaw range of motion (ROM) have been found to correlate with performance status and patient-rated quality of life in surgically treated oral cancer patients [19]. Specifically, higher tongue strength measures correlated with better performance status in terms of diet type and ability to eat in public on the performance status scale (PSS) [20] and overall level of functioning/impairment on the Karnofsky performance status scale [21]. Tongue strength also correlated with patient-rated quality of life for swallowing, as examined with the eating assessment tool (EAT-10) [22] and the MD Anderson Dysphagia Inventory (MDADI) [23], and for speech, as examined with the SHI [24]. Tongue strength correlated with the domains of pain, swallowing, and speech on the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Head and Neck module (QLQ-H&N35) [25]. No study to date has examined how oral outcomes correlate with performance status and patient-rated quality of life in patients who have undergone definitive chemoradiotherapy for head and neck cancer treatment. This study examined oral outcomes, performance status, and patient-rated quality of life at baseline and 3 and 6 months post-treatment in a group of patients who had undergone definitive chemoradiotherapy for head and neck cancer. We hypothesized that oral outcomes would correlate with performance status and patient-rated quality of life in this population. We further hypothesized that outcomes would improve over time in this cohort of patients.
Patients and Methods
Subjects
Twenty-nine patients who underwent chemoradiotherapy (CXRT) treatment for head and neck cancer at various sites were included in this study. Patients were accrued between January 2010 and April 2012. Subjects included 23 males and 6 females (mean age = 58.52 ± 9.2, range = 41–78). Table 1 gives complete demographic information. The majority of patients (n = 18) were treated for oropharyngeal tumors (63 %), and the next largest group had cancer of the larynx (n = 5; 18 %). The majority of patients (n = 21) had Stage IV disease. Sample size estimation was not performed for this study as it was a pilot study and there are few data regarding oral outcome variables in this population. Therefore, we selected all of the patients in our database who met our inclusion criteria for this study. Patients were consecutively referred by their medical or radiation oncologist for functional assessment by the speech pathologist prior to commencement of CXRT. As part of our usual protocol, the speech pathologist follows patients at the following time points: baseline (before CXRT) and 1, 3, 6, and 12 months post-CXRT (Fig. 1) [19].This study was approved by the Institutional Review Board and all subjects provided informed consent. Eligibility criteria included patients over 21 years of age who were to undergo primary CXRT for newly diagnosed head and neck cancer. Patients with any history of neurologic deficits, spine surgery, or previous head and neck cancer treatment that might adversely affect cognition, tongue function, or swallowing were excluded from this study.

Standard assessment protocol
Assessments
All patients underwent functional assessment of oral outcome variables, including tongue strength, jaw ROM, and saliva weight. In addition, all patients were administered the PSS, a clinician-administered scale that includes the domains Normalcy of Diet, Eating in Public, and Understandability of Speech, and the Karnofsky Performance Scale (KPS), a clinician-administered scale that assesses overall functional impairment. The PSS and KPS were scored by the clinician, based on patient questioning. The PSS was administered as a speech- and swallow-related PSS, whereas the KPS was administered to glean overall functional performance (i.e., ability to carry on normal activity, work, take care of personal needs, etc.). Subjects were also asked to complete QOL questionnaires, including (1) the EAT-10, (2) The MDADI, (3) the SHI, and (4) the EORTC H&N35. All patients were assessed at baseline and 3 and 6 months post-treatment.
Tongue Strength Assessment
Tongue strength was assessed with the Iowa Oral Performance Instrument (IOPI), an instrument that measures oral tongue pressures [26]. Maximum tongue strength (P max) in kilopascals (kPa) was measured. During tongue function measurement, subjects were seated with the tongue pressure bulb positioned behind the central incisors or behind the alveolar ridge in the edentulous patient. Subjects were instructed to press up on the bulb with the tongue and squeeze the bulb against the roof of the mouth as hard as possible for 3 s. Three maximum pressure measurements were obtained for each subject, with the highest maximum pressure used as the subject’s maximal tongue strength [26]. A bite block was not used during this task, as data support having the jaw unconstrained during tongue strength assessment [27]. A 2-min rest was allowed between trials. Although swallowing is a submaximal task, maximal tongue strength has been found to correlate with oral phase swallow functioning as well as airway protection (i.e., aspiration) [11, 13, 28].
Jaw ROM Assessment
Jaw ROM was assessed using TheraBite® jaw ROM measurement discs (Atos Medical AB, Hörby, Sweden), which have a ruler (in mm) to measure the mouth opening. For this task, subjects were asked to open their mouth as wide as possible and the disc was placed between the central incisors, or the gums in the midline in the case of edentulous patients. In the latter case, 19 mm was subtracted from the score to take into account the lack of dentition [29].
Salivary Flow Assessment
Stimulated saliva flow production was assessed to determine the degree of hyposalivation in these patients. The subject’s stimulated saliva production was quantified using the Saxon test [30], a reliable and validated test to assess stimulated saliva production by taking the difference of the weight of a 4 × 4 folded sterile piece of gauze before and after having been chewed. Subjects were asked to chew on the gauze for 2 min and then spit it into a cup for reweighing. The liquid crystal display (LCD) electronic top-loading balance (Cole-Palmer model 11320-00) was used for the xerostomia assessment. Saliva production was examined in relation to the scores on the PSS and QOL questionnaires.
Performance Status Assessment
The PSS [20] was administered to determine diet type (i.e., normalcy of diet domain), speech understandability (i.e., understandability of speech domain) and impact of CXRT treatment on ability to eat socially (i.e., eating in public domain). All three domains are scaled from 0 to 100, with a higher score indicating better functioning. In addition, the Karnofsky performance scale index (KPS) [21], a clinician-rated scale of overall functional impairment was administered. Both scales were administered and scored by the clinician, based on patient responses to questions.
Quality-of-Life Assessment
Subjects completed four QOL questionnaires: (1) the EAT-10, a 10-item self-administered symptom-specific outcome instrument for dysphagia that uses a Likert scale from 0 to 4, with 0 being a normal score and higher scores indicating poorer functioning [22]; (2) the MDADI, a 30-point self-administered symptom-specific outcome instrument for dysphagia specific to the head and neck cancer population that uses a Likert scale, with higher scores indicating better functioning [23]; (3) the SHI, a 30-point self-administered symptom-specific outcome instrument for speech that incorporates a Likert scale from 0 to 4, with 0 being a normal score and 4 indicating the most abnormal functioning [24]; and (4) the EORTC H&N35, a 35-item self-administered symptom-specific outcome instrument that assesses symptoms encountered specifically by patients with head and neck cancer [25]. This measure has 18 symptom scales that record pain, swallowing, senses, speech, social eating, social contact, sexuality, teeth, mouth opening, dry mouth, sticky saliva, coughing, felt ill, painkillers, feeding tube, nutritional supplements, weight gain, and weight loss. This instrument incorporates a Likert scale from 1 to 4, with higher scores indicating poorer functioning. We report on only nine symptom scales for this article (Table 5). These nine symptoms were chosen as they relate most closely to the oral outcomes assessed and described earlier in this article. Both the EAT-10 and the MDADI were administered since the EAT-10 examines specific swallow-related impairments (e.g., swallowing liquids/solids/pills takes extra effort, food sticks in throat, coughing when eating, etc. [22]), whereas the MDADI taps into additional domains of the emotional aspects of swallowing impairment (i.e., embarrassed by eating, feeling self-conscious, being upset, etc. [23]).
Statistical Analysis
Means and standard deviations were used to describe the oral outcome variables and the PSS, KPS, and QOL scores. A repeated-measures ANOVA was completed to compare patients at baseline and at 3 and 6 months post-treatment. This analysis was performed to assess oral outcome measures, performance status measures, and QOL measures over time (baseline (BS) and 3 and 6 months post-treatment). The Mann–Whitney test of mean differences was completed to compare oral outcome variables, performance status, and patient-rated QOL by tumor site and stage of disease. Statistical analyses were conducted with SPSS ver. 20 (SPSS, Inc., Chicago, IL, USA).
Results
Oral Outcome Variables
Tongue strength was found to be statistically different at all three time points (p = 0.000). On post hoc analyses it was seen that there was approximately a 12.19 % (p = 0.003) and an 8.98 % (p = 0.002) significant reduction in tongue strength from baseline to 3 and 6 months post-treatment, respectively (Table 2A and B; Fig. 2). However, despite these statistically significant differences across time points, mean tongue strength at all time points was within the range seen in the healthy population (i.e., 50–60 kPa) [31–33].

Tongue strength and jaw opening at baseline and 3 and 6 months post-treatment
Jaw ROM was also found to be statistically different at all three time points (p = 0.000) (Table 2A and B). Further post hoc analyses revealed the jaw ROM to be marginally but significantly reduced from baseline to 3 months (8.80 % reduction, p = 0.000) and 6 months (9.42 % reduction, p = 0.000). In addition, despite these differences, the jaw ROM was within the range seen in healthy individuals at all time points (i.e., 36-mm opening) [14].
Saliva weight followed a similar trend and was also statistically significantly different at all three time points (p = 0.000) (Table 2A and B). On post hoc analyses it was seen that there was an approximately 58 % (p = 0.000) and 49 % (p = 0.00) significant reduction in saliva weight from baseline to 3 and 6 months, respectively (Table 2; Fig. 3). In contrast to the other oral outcome measures, saliva weight was grossly within the range seen in healthy individuals only at baseline (i.e., 4.76 g) [34]. Saliva weight was lower than that seen in healthy individuals at both 3 and 6 months.

Saliva weight at baseline and 3 and 6 months post-treatment
When examining oral outcome variables over time by site (i.e., oropharynx vs. other sites combined) and by tumor stage (i.e., Stage I–III vs. Stage IV), no significant differences were found for any variable at any time point (Table 2A and B).
Performance Status Scores
Normalcy of diet was found to be statistically different at all three time points (p = 0.000). On post hoc analyses it was seen that there was an approximately 18 % (p = 0.000) and 14 % (p = 0.002) significant reduction in normalcy of diet from baseline to 3 and 6 months, respectively (Table 3A and B; Fig. 4).Eating in Public and Understandability of Speech were not statistically different at all three time points (p = 0.270 and p = 0.326, respectively). When examining performance status by site (i.e., oropharynx vs. other sites combined), it was significantly higher for the normalcy of diet domain for the oropharynx group at all three time points compared to the other sites combined (Table 3A). For the Eating in Public domain, the oropharynx group scored significantly higher at the baseline and 3-month time points and marginally significantly higher at the 6-month time point than the Other sites group (Table 3A). No significant differences were found between the two groups for the Understandability of Speech domain (Table 3A). When comparing performance status by tumor stage (i.e., Stage I–III vs. Stage IV), the group with Stage I-III disease demonstrated significantly higher normalcy of diet scores at baseline and 3 months post-treatment, but lower scores at 6 months post-treatment (Table 3B). The Stage I-III group performed worse on eating in public at baseline and 6 months post-treatment but slightly better at 3 months post-treatment. (Table 3B). There were no differences in Understandability of Speech by tumor stage across time points (Table 3B).

Performance status scale at baseline and 3 and 6 months post-treatment
Patient-rated Quality-of-Life Scores
All patients reported a mean EAT-10 score of >3, which indicates impairment in eating ability prior to commencement of treatment [22]. The EAT-10 score was found to be statistically different at all three time points (p = 0.000). On post hoc analyses it was further seen that scores at baseline were significantly higher than those at 3 months (11.18 vs. 4.39, p = 0.000) (Table 4A and B; Fig. 5) It was also noted that EAT-10 scores significantly decreased from 3 months to 6 months post-treatment (11.18 vs. 7.18, p = 0.011).This indicated a continued moderate impairment (between 3.1 and 20 on the EAT-10 severity scale) in eating ability (from baseline to 6 months) [35]. A similar pattern was seen across time when taking tumor site and stage of disease into consideration (Table 4A and B). When comparing by site of disease, the oropharynx group performed better at all three time points than the other sites group (Table 4A). When examining by tumor stage, the Stage I–III group performed better than the Stage IVA group across time points (Table 4B).

Eating assessment tool (EAT-10) and speech handicap index (SHI) at baseline and 3 and 6 months post-treatment
The MDADI score was also found to be different at all three time points (p = 0.202). According to Chen et al. [36], MDADI has been categorized by degree of disability (0–20 = profound, 21–40 = severe, 41–60 = moderate, 61–80 = mild, 81–100 = minimal), and, thus, we observed that patients in this study went from being minimally impaired at baseline to mildly impaired at 3 and 6 months (Table 4; Fig. 6). When examining the data by site, the oropharynx group performed better than the Other sites group across time points (Table 4A). The Stage I–III group performed worse at baseline and 6 months post-treatment but better at 3 months post-treatment than the Stage IVA group (Table 4B).

MD Anderson Dysphagia Inventory (MDADI) at baseline and 3 and 6 months post-treatment
All patients reported a mean SHI score of >6, which indicates speech problems in daily life prior to commencement of treatment. The SHI was found to be marginally statistically different at all three time points (p = 0.055). On post hoc analyses it was further seen that scores increased (i.e., worsened) significantly from baseline to 6 months (8.50 vs. 17.79, p = 0.041) (Table 4A and B; Fig. 5). When examining SHI scores by site of disease, the oropharynx group scored marginally significantly higher at baseline and significantly higher at 3 and 6 months post-treatment (Table 4A). When examining by tumor stage, the Stage I–III group performed worse at baseline and 6 months post-treatment than the Stage IVA group.
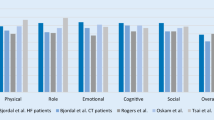
On the EORTC H&N35, scores of symptom scales such as Swallowing (p = 0.057), Senses (p = 0.000), Speech (p = 0.082), Dry mouth (p = 0.000), and Sticky saliva (p = 0.000) were found to be different at all three time points. On post hoc analyses it was further seen that the Dry mouth scores significantly increased from baseline to 3 months (15.92 vs. 71.96, p = 0.000) and 6 months (15.92 vs. 65.32, p = 0.000) (Table 5). For Speech, post hoc analyses revealed that scores significantly increased from baseline to 6 months (11.13 vs. 14.87, p = 0.046). For Sticky saliva, post hoc analyses revealed that scores significantly increased from baseline to 3 months (9.67 vs. 49.92, p = 0.000) and 6 months (9.67 vs. 49.96, p = 0.000). Similarly, for the symptom scale of Senses (taste and smell), post hoc analyses revealed that scores significantly increased from baseline to 3 months (2.00 vs. 27.40, p = 0.000) and 6 months (2.00 vs. 23.28, p = 0.000) (Fig. 7).

EORTC H&N 35 domains at baseline and 3 and 6 months post-treatment
At baseline, when the EORTC domains’ scores were compared by site, statistically significant differences were noted for dry mouth only (oropharynx group: 8.31 vs. other sites group: 29.80; p = 0.032). Statistically significant differences were observed for the domain of swallowing (oropharynx group: 2.31 vs. other sites group: 24.70; p = 0.050) but not for speech (oropharynx group: 4.75 vs. other sites group: 23.67; p = 0.064), social eating (oropharynx group: 2.75 vs. other sites group: 27; p = 0.075), social contact (oropharynx group: 1.44 vs. other sites group: 10.70; p = 0.059), and sticky saliva (oropharynx group: 4.13 vs. other sites group: 18.44; p = 0.054), For the EORTC domain of pain, we found statistically significant differences when comparing stage of cancer (Stage I–III: 3.33 vs. Stage IVA: 24.26; p = 0.000).
At 3 months, the EORTC Pain domain was statistically significantly different between different sites (oropharynx group: 24.35 vs. other sites group: 10.36; p = 0.024). When grouped by stage, there were no statistically significant differences.
At 6 months, EORTC domains were not statistically significantly different by site or stage.
Discussion
Patients in this study demonstrated poorer functioning in oral outcomes, performance status, and quality of life after completion of chemoradiotherapy compared to pretreatment. Poorer performance status post-treatment agrees with that found in the literature. However, several outcomes examined in this study were within normal or acceptable limits following treatment. Specifically, although the oral outcomes of tongue strength and jaw opening declined following chemoradiotherapy, the values for both lingual strength and jaw opening were still within the normal limits seen in healthy individuals [14, 32]. Salivary flow was the only oral outcome that was significantly lower than normal at both 3 and 6 months post-treatment, thus, contributing to the poorer QOL scores for the sticky saliva and dry mouth domains on the EORTC H&N35. Connor et al. [18] found similar decrements in salivary flow that persisted at 6 months post-treatment. However, others have found improved salivary function over 12–24 months in patients treated with intensity-modulated radiotherapy (IMRT) [37, 38], with a similar improvement in xerostomia-related QOL over a 12-month period [38]. All patients received IMRT. Twenty-four patients received bilateral radiotherapy to the neck and five patients received unilateral radiotherapy to the neck. No statistically significant differences were seen in terms of oral outcome variables, performance status, and quality-of-life measures between these two groups at baseline and 3 and 6 months. Two of the 29 patients also received induction chemotherapy. Again, no statistically significant differences were seen in terms of oral outcome variables, performance status, and QOL measures between those who had induction chemotherapy and those who did not at baseline and 3 and 6 months. Furthermore, no significant differences were found when examining oral outcomes by tumor site or stage.
When examining performance status in these patients, normalcy of diet was lowest at 3 months and improved by 6 months. Despite the statistically significant decrease in diet, the mean score of 86 at 6 months post-treatment indicates that these patients were able to eat anything other than peanuts or they could take a regular diet but needed to wash their food down with liquids; both situations would rate a score of 90 (the next lower score of 80 includes all meats). When examining performance status by tumor site, significant differences were found for normalcy of diet and eating in public, with better functioning in the oropharynx group than in the other sites group. However, results were mixed when the outcomes were analyzed by stage of disease. Others have found that swallowing returned to pretreatment levels [18]. Follow-up for up to 12 months after chemoradiotherapy has shown that there was improvement in diet and reduction in the need for nonoral supplementation [12]. Harrison et al. [39, 40] have found performance status to be quite high in terms of eating in public and diet type in patients with BOT cancer treated with primary radiotherapy, with a mean follow-up of 5 years post-treatment. However, it remains to be seen whether the addition of chemotherapy will result in worsening of outcomes in these patients over time.
Across QOL scales, ratings were poorest at 3 months and improved at 6 months post-treatment, although not to pretreatment levels. This trend held true when examining outcomes by tumor site and by stage of disease. This trend also agrees with QOL outcomes after chemoradiotherapy found by others [18]. Longer follow-up, specifically 5 years, has yielded excellent QOL in BOT patients treated with primary radiotherapy to the oropharynx as compared to a comparable group treated with surgery [39, 40]. It is interesting that the patients in our study rated themselves as impaired on the SHI post-treatment, despite being completely understandable, as found on the PSS understandability of speech subscale. When queried further, patients reported that dry mouth seemed to have a negative impact on their speech. This report coincides with the worsening of both salivary flow and SHI scores from 3 to 6 months post-treatment in these patients. All of these patients demonstrated normal speech function and none demonstrated lingual neuropathy. This QOL scale is probably best administered further out from treatment, as cranial nerve deficits resulting in dysarthria may not be appreciated until long after completion of treatment.
Late changes in swallow function have been found in irradiated head and neck cancer patients, with development of tissue fibrosis, neuropathy, trismus, and osteoradionecrosis, which can affect chewing ability, bolus propulsion, and pharyngeal phase function of swallowing, the latter including reduced pharyngeal constrictor motion, reduced tongue base motion, reduced laryngeal elevation, and closure for swallowing [41–43]. Clearly, these patients should be followed long term to monitoring their swallow function. In addition, there is evidence to support the use of prophylactic swallow exercises during treatment in this population [44–49]. All of the patients in this cohort were assigned prophylactic swallow exercises at the onset of the concomitant chemoradiotherapy, focusing on maximizing jaw, tongue, tongue base, pharyngeal constrictor, and laryngeal ROM and strength in order to maintain the oral and pharyngeal phases of swallowing during treatment. All patients were given written instructions on how to perform these exercises at home. Formal therapy was not provided during chemoradiotherapy. However, patients were seen halfway through their treatment for review of the exercises and to monitor swallowing, and as otherwise needed during treatment. Although not specifically examined in this study, there was only fair compliance by the patients with this exercise program during treatment. We are currently examining the utility of exercise logs to improve adherence to this exercise program. In addition, we are following patients to 24 months, with 12- and 24-month evaluations to look for any swallowing changes as well as changes in oral outcomes and QOL.
Conclusion
Patients who underwent chemoradiotherapy for head and neck cancer performed worse in oral outcomes, performance status, and quality of life after treatment. However, the level of functioning for some oral outcomes was still grossly within normal limits and performance status was normal to mildly reduced. Quality of life did not reach pretreatment levels in these patients but was only mildly impaired, except for speech and domains related to xerostomia, which did not improve over time. Current studies are examining functional outcomes and QOL functioning further out from treatment to help predict function over time. The question of when and how completely function will return is commonly asked by patients who are about to undergo organ preservation treatment for head and neck cancer. Future studies with larger numbers of patients that assess functioning further out from treatment should help answer this question. Furthermore, the effects of prophylactic exercise regimens on functional outcomes and QOL is currently being examined, as is adherence to these regimens.
References
Cooper JS, et al. Late effects of radiation therapy in the head and neck region. Int J Radiat Oncol Biol Phys. 1995;31(5):1141–64.
Treister N, Sonis S. Mucositis: biology and management. Curr Opin Otolaryngol Head Neck Surg. 2007;15(2):123–9.
Ruo Redda MG, Allis S. Radiotherapy-induced taste impairment. Cancer Treat Rev. 2006;32(7):541–7.
Eisbruch A, et al. Dysphagia and aspiration after chemoradiotherapy for head-and-neck cancer: which anatomic structures are affected and can they be spared by IMRT? Int J Radiat Oncol Biol Phys. 2004;60(5):1425–39.
Logemann JA, et al. Swallowing disorders in the first year after radiation and chemoradiation. Head Neck. 2008;30(2):148–58.
Newman LA, et al. Swallowing and speech ability after treatment for head and neck cancer with targeted intra-arterial versus intravenous chemoradiation. Head Neck. 2002;24(1):68–77.
de Graeff A, et al. A prospective study on quality of life of laryngeal cancer patients treated with radiotherapy. Head Neck. 1999;21(4):291–6.
Hammerlid E, et al. A prospective quality of life study of patients with laryngeal carcinoma by tumor stage and different radiation therapy schedules. Laryngoscope. 1998;108(5):747–59.
List MA, et al. Quality of life and performance in advanced head and neck cancer patients on concomitant chemoradiotherapy: a prospective examination. J Clin Oncol. 1999;17(3):1020–8.
Oates JE, et al. Prospective evaluation of quality of life and nutrition before and after treatment for nasopharyngeal carcinoma. Arch Otolaryngol Head Neck Surg. 2007;133(6):533–40.
Lazarus CL, et al. Swallowing and tongue function following treatment for oral and oropharyngeal cancer. J Speech Lang Hear Res. 2000;43(4):1011–23.
Lazarus C, et al. Effects of radiotherapy with or without chemotherapy on tongue strength and swallowing in patients with oral cancer. Head Neck. 2007;29(7):632–7.
Clark HM, et al. Relationships among subjective and objective measures of tongue strength and oral phase swallow impairments. Am J Speech Lang Pathol. 2003;12:40–50.
Weber C, et al. Limited mouth opening after primary therapy of head and neck cancer. Oral Maxillofac Surg. 2010;14(3):169–73.
Carrara-de Angelis E, et al. Voice and swallowing in patients enrolled in a larynx preservation trial. Arch Otolaryngol Head Neck Surg. 2003;129(7):733–8.
Fung K, et al. Voice and swallowing outcomes of an organ-preservation trial for advanced laryngeal cancer. Int J Radiat Oncol Biol Phys. 2005;63(5):1395–9.
Cartmill B, et al. A prospective investigation of swallowing, nutrition, and patient-rated functional impact following altered fractionation radiotherapy with concomitant boost for oropharyngeal cancer. Dysphagia. 2012;27(1):32–45.
Connor NP, et al. Impact of conventional radiotherapy on health-related quality of life and critical functions of the head and neck. Int J Radiat Oncol Biol Phys. 2006;65(4):1051–62.
Lazarus CL, Husaini H, Anand SM, Jacobson AS, Mojica JK, Buchbinder D, Urken ML. Tongue strength as a predictor of functional outcomes and quality of life after tongue cancer surgery. Ann Otol Rhinol Laryngol. 2013;122(6):386–97.
List MA, Ritter-Sterr C, Lansky SB. A performance status scale for head and neck cancer patients. Cancer. 1990;66(3):564–9.
Schag CC, Heinrich RL, Ganz PA. Karnofsky performance status revisited: reliability, validity, and guidelines. J Clin Oncol. 1984;2(3):187–93.
Belafsky PC, et al. Validity and reliability of the eating assessment tool (EAT-10). Ann Otol Rhinol Laryngol. 2008;117(12):919–24.
Chen AY, et al. The development and validation of a dysphagia-specific quality-of-life questionnaire for patients with head and neck cancer: the M. D. Anderson dysphagia inventory. Arch Otolaryngol Head Neck Surg. 2001;127(7):870–6.
Rinkel RN, et al. Speech Handicap Index in patients with oral and pharyngeal cancer: better understanding of patients’ complaints. Head Neck. 2008;30(7):868–74.
Sherman AC, et al. Assessing quality of life in patients with head and neck cancer: cross-validation of the European Organization for Research and Treatment of Cancer (EORTC) Quality of Life Head and Neck module (QLQ-H&N35). Arch Otolaryngol Head Neck Surg. 2000;126(4):459–67.
Robin DA, et al. Tongue strength and endurance: relation to highly skilled movements. J Speech Hear Res. 1992;35(6):1239–45.
Solomon NP, Munson B. The effect of jaw position on measures of tongue strength and endurance. J Speech Lang Hear Res. 2004;47(3):584–94.
Robbins J, et al. The effects of lingual exercise in stroke patients with dysphagia. Arch Phys Med Rehabil. 2007;88(2):150–8.
Magne P, Gallucci GO, Belser C. Anatomic crown width/length ratios of unworn and worn maxillary teeth in white subjects. J Prosthet Dent. 2003;89(5):453–61.
Kohler PF, Winter ME. A quantitative test for xerostomia. The Saxon test, an oral equivalent of the Schirmer test. Arthritis Rheum. 1985;28(10):1128–32.
Robbins J, et al. Age effects on lingual pressure generation as a risk factor for dysphagia. J Gerontol A Biol Sci Med Sci. 1995;50(5):M257–62.
Nicosia MA, et al. Age effects on the temporal evolution of isometric and swallowing pressure. J Gerontol A Biol Sci Med Sci. 2000;55(11):M634–40.
Stierwalt JA, Youmans SR. Tongue measures in individuals with normal and impaired swallowing. Am J Speech Lang Pathol. 2007;16(2):148–56.
Navazesh M, Christensen CM. A comparison of whole mouth resting and stimulated salivary measurement procedures. J Dent Res. 1982;61(10):1158–62.
Husaini H et al. Feasibility of developing a severity rating scale for the Eating Assessment Tool (Eat-10) in head and neck cancer patients. Presented at the Annual Dysphagia Research Society Meeting 2013, Seattle, WA.
Chen PH, et al. Prevalence of perceived dysphagia and quality-of-life impairment in a geriatric population. Dysphagia. 2009;24(1):1–6.
Eisbruch A, et al. Xerostomia and its predictors following parotid-sparing irradiation of head-and-neck cancer. Int J Radiat Oncol Biol Phys. 2001;50(3):695–704.
Lin A, et al. Quality of life after parotid-sparing IMRT for head-and-neck cancer: a prospective longitudinal study. Int J Radiat Oncol Biol Phys. 2003;57(1):61–70.
Harrison LB, et al. Detailed quality of life assessment in patients treated with primary radiotherapy for squamous cell cancer of the base of the tongue. Head Neck. 1997;19(3):169–75.
Harrison LB, et al. Performance status after treatment for squamous cell cancer of the base of tongue—a comparison of primary radiation therapy versus primary surgery. Int J Radiat Oncol Biol Phys. 1994;30(4):953–7.
Lazarus CL. Effects of radiation therapy and voluntary maneuvers on swallow functioning in head and neck cancer patients. Clin Commun Disord. 1993;3(4):11–20.
Hutcheson KA, Lewin JS, Barringer DA, Lisec A, Gunn GB, Moore MW, Holsinger FC. Late dysphagia after radiotherapy-based treatment of head and neck cancer. Cancer. 2012;118:5793–9.
Pauloski BR, et al. Speech and swallowing in irradiated and nonirradiated postsurgical oral cancer patients. Otolaryngol Head Neck Surg. 1998;118(5):616–24.
Kotz T, et al. Prophylactic swallowing exercises in patients with head and neck cancer undergoing chemoradiation: a randomized trial. Arch Otolaryngol Head Neck Surg. 2012;138(4):376–82.
Kulbersh BD, et al. Pretreatment, preoperative swallowing exercises may improve dysphagia quality of life. Laryngoscope. 2006;116(6):883–6.
Carroll WR, et al. Pretreatment swallowing exercises improve swallow function after chemoradiation. Laryngoscope. 2008;118(1):39–43.
van der Molen L, et al. A randomized preventive rehabilitation trial in advanced head and neck cancer patients treated with chemoradiotherapy: feasibility, compliance, and short-term effects. Dysphagia. 2011;26(2):155–70.
Carnaby-Mann G, et al. “Pharyngocise”: randomized controlled trial of preventative exercises to maintain muscle structure and swallowing function during head-and-neck chemoradiotherapy. Int J Radiat Oncol Biol Phys. 2012;83(1):210–9.
Hutcheson KA, et al. Eat and exercise during radiotherapy or chemoradiotherapy for pharyngeal cancers: use it or lose it. JAMA Otolaryngol Head Neck Surg. 2013;139(11):1127–34.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lazarus, C.L., Husaini, H., Hu, K. et al. Functional Outcomes and Quality of Life After Chemoradiotherapy: Baseline and 3 and 6 Months Post-Treatment. Dysphagia 29, 365–375 (2014). https://doi.org/10.1007/s00455-014-9519-8
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00455-014-9519-8