
Abstract
Background
Anal fissure is one of the most common proctological complaints. If the fissure persists for more than 6–8 weeks, it is termed a chronic fissure and will most likely need surgical intervention. Surgical partial transection of the internal sphincter muscle, lateral internal sphincterotomy (LIS), is still seen as the gold standard procedure for chronic anal fissure in many parts of the world, especially in the Anglo-American community. In contrast, the German-speaking surgical community favors fissurectomy ± application of Botox, as some studies report high postoperative incontinence rates after LIS.
Objective
This paper aims to give an overview of the literature on LIS and its outcomes and answer the question, “Is LIS still the gold standard surgical approach for chronic anal fissure?”
Material and methods
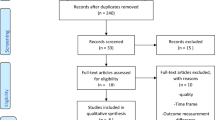
A literature search for “sphincterotomy,” “internal sphincter,” and “anal fissure” was performed in PubMed. For the purpose of this overview article, randomized controlled trials (RCTs), meta-analyses, up-to-date guidelines, and retrospective cohort studies were taken into account.
Results and conclusion
LIS produces excellent rates of fissure healing (~95%), quick symptom relief, and high patient satisfaction. Incontinence after LIS is mostly described as mild and transient. In the authors’ view, open LIS is therefore rightfully still the gold standard procedure for treatment of chronic anal fissure in the majority of patients. A conservative approach with limited division of internal sphincter muscle is preferred. For patients with preexisting sphincter weakness and an increased risk of incontinence, further preoperative diagnostic assessment (anal manometry, endoanal ultrasound) is recommended. In this high-risk group, alternative surgical options might be preferred.
Zusammenfassung
Hintergrund
Die Analfissur ist eine der häufigsten proktologischen Diagnosen. Besteht sie länger als 6–8 Wochen wird sie zur chronischen Fissur, welche in der Regel eine operative Intervention benötigt. Vor allem im englischsprachigen Raum wird die chirurgische Durchtrennung eines Teils des internen Sphinktermuskels, die laterale Internus Sphinkterotomie (LIS), nach wie vor als „Goldstandard“ in der chirurgischen Behandlung angesehen. Dies steht im Kontrast zur deutschsprachigen chirurgischen Gemeinschaft, welche der Fissurektomie ± Botoxinjektion den Vorzug gibt, da nach LIS zum Teil eine hohe Inkontinenzrate beschriebenen wird.
Ziel
Aufbereitung der aktuellen Literatur rund um LIS – ist der Status von LIS als Goldstandard-Therapie in der chronischen Analfissur nach wie vor vertretbar?
Material und Methoden
Aktuelle Literatur rund um LIS wurde in „pubmed“ identifiziert. Dabei wurden sowohl RCT, Metaanalysen, aktuelle Guidelines, sowie retrospektive Kohortenstudien berücksichtigt.
Ergebnisse und Diskussion
Die Vorteile von LIS bestehen in einer ausgezeichneten Heilungsrate (~95 %), einer prompten Symptomlinderung und dementsprechend hoher Patientenzufriedenheit. Postoperative Inkontinenz nach LIS wird meist als mild und transient beschrieben. Die Autoren vertreten daher die Meinung, dass eine offene, laterale Sphinkterotomie nach wie vor dem „Gold Standard“ der chirurgischen Fissurbehandlung entspricht. Dabei wird ein „konservativer Approach“ mit limitierter Muskeldurchtrennung bevorzugt. Bei Patienten mit Verdacht auf bereits bestehende Sphinkterschwäche werden weitergehende präoperative Abklärungen (Manometrie, endoanaler Ultraschall) empfohlen. Bei dieser „Risikogruppe“ kann ein Ausweichen auf alternative chirurgische Techniken sinnvoll sein.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Anal fissure is a common proctological complaint, with a lifetime risk of 11% [1]. It most often affects young adults and is a cause of morbidity and loss of time from work. Anal fissures are categorized into acute and chronic. Acute fissures are usually amenable to medical treatment, which includes a combination of stool softeners, bulking agents, and topical ointments (glyceral trinitrate, GTN; diltiazem; etc.). If an acute fissure fails to heal within 6–8 weeks, it is said to be chronic in nature and usually requires surgical intervention [2].
The pathophysiology underlying chronic anal fissure is believed to involve spasm of the internal anal sphincter secondary to mucosal injury and inflammation, giving rise to high sphincter pressures and local ischemia, which in turn inhibits mucosal healing. Surgical treatments aim to break this vicious cycle by causing temporary (Botox) or permanent (sphincterotomy) relief of internal sphincter spasm.
A trial of medical therapy is usually advocated for patients with chronic anal fissure, but if this fails, the surgical options include Botox injection into the internal anal sphincter, fissurectomy with/without Botox, anodermal advancement flap, or lateral internal sphincterotomy (LIS). There is disagreement in the colorectal community about which should be the preferred method. The German-speaking community has practically “banned” LIS, due to reports of unacceptably high postoperative incontinence rates [3], whereas LIS is still the preferred option in many other Western countries, because of excellent healing rates and high patient satisfaction ([4]; Fig. 1; Table 1).

UK algorithm for anal fissure treatment. GTN glyceral trinitrate
This paper attempts to unravel the evidence behind the treatment of chronic anal fissure and make the case for LIS as a good option in the majority of patients.
First-line surgical strategy for chronic anal fissure
Why LIS?
During LIS, the internal sphincter is divided to relieve muscle spasm, thereby increasing blood flow to the chronic mucosal ulcer and stimulating healing. The open lateral technique was first described by Eisenhammer in 1959 [10] and further propagated in the 1960s by Parks, after whom the technique was named [11]. The closed technique was advocated by Notaras in 1971 [12]. The predecessor of LIS, posterior sphincterotomy, has been abandoned due to frequent development of a “keyhole deformation” at the 6 o’clock sphincterotomy site rendering patients more prone to incontinence [13, 14].
Many national treatment guidelines still recommend LIS as first-line treatment in chronic anal fissure (Table 1). The advantages of LIS are well described in the literature, including high rates of fissure healing (~95%) with rapid pain relief and high patient satisfaction (Table 2). Two recent meta-analyses have confirmed these findings, with healing rates of 93% documented by Ebinger et al. [15], and superior healing rates as compared to other treatments (topical nitroglycerin, botulinum toxin A injection, oral nifedipine) published by Nelson et al. [14].
Fissurectomy vs. lateral internal sphincterotomy
In the German-speaking community, fissurectomy is the preferred surgical fissure treatment. The chronically inflamed mucosal ulcer and any sentinel skin tags are excised, leaving a well-vascularized tissue bed to facilitate healing and an intact internal sphincter muscle to preserve continence [21].
Although the theory behind fissurectomy is sound, the evidence supporting its benefit over LIS is limited. Randomized controlled trials (RCTs) comparing fissurectomy with LIS are scarce. Hancke et al. compared two groups of 30 patients undergoing either fissurectomy alone or fissurectomy + LIS. The success rates were similar in each treatment group, with no significant difference in postoperative incontinence. The authors concluded that addition of sphincterotomy to fissurectomy was unnecessary [21].
Another RCT published by Mousavi et al. compared fissurectomy with LIS. In this group of 60 patients, both fissurectomy and LIS showed excellent healing rates. Whereas patients in the fissurectomy group experienced a slow, gradual improvement in symptoms, patients in the LIS group benefited from immediate symptom relief, which was reflected in a higher patient satisfaction score (LIS 96.6% vs. fissurectomy 87.5%). After a median follow-up of 22 months, 2 patients reported incontinence for flatus in the fissurectomy group, but none in the LIS group. The authors conclude that LIS should be the preferred surgical technique for chronic anal fissure [16]. In a meta-analysis by Nelson et al., LIS was less likely to result in treatment failure as compared to fissurectomy. Additionally, there was no significant difference in continence disturbance between the two techniques [4].
Incontinence after LIS
The elephant in the room?
The reporting of postoperative incontinence after LIS is inconsistent. The meta-analysis by Ebinger et al. documented an overall incontinence rate after LIS of 9.4%. It included studies with incontinence rates varying widely between 0 and 44%, suggesting differences in surgical technique and/or patient selection. The impact of incontinence on patient satisfaction and quality of life was not assessed, nor was the duration of incontinence (transient or permanent) [15]. A US study investigated the outcomes of LIS with particular regard to fecal incontinence (FI) [18]. Five hundred patients were evaluated by questionnaire after LIS, with a medium follow-up of 72 months. The fissure healing rate was excellent at 96%, with symptom relief achieved on average by 3 weeks, and a recurrence rate of only 8%. However, 45% of patients reported some form of incontinence during the postoperative period. In long-term follow-up, the incontinence rate dropped, with 6% suffering incontinence to flatus, 8% minor fecal soiling, and 1% incontinence to solid stool, indicating that incontinence was mostly transient and minor. Accordingly, only 3% of patients reported a negative impact on quality of life.
Another study by Hasse et al. analyzed short- and long-term outcomes of 209 patients undergoing LIS matched to a control group with no previous proctological history. In the LIS group, 15% of patients reported some degree of incontinence at 12 weeks postoperatively. Incontinence was classified as mild in 11%, moderate in 6.9%, and severe in only about 1%. Patient satisfaction after 12 weeks was high, at 95%. In longer-term follow-up (median of 124 months), however, the number of patients affected by incontinence increased, as did its severity (7.7% mild, 9.6% moderate, 4.3% severe), and patient satisfaction dropped to 73%. The follow-up data of the control group revealed an overall incontinence rate of only 3.8%, with 2.4% classified as mild, 1.4% as moderate, and 0% as severe. The authors concluded that LIS should serve as a “salvage procedure,” with fissurectomy recommended as the first-line treatment in chronic anal fissure [17].
A recent meta-analysis evaluating the outcomes of around 4500 patients who had undergone either open or closed LIS, with a follow-up ranging from 24 to 124 months, reported continence disturbance in up to 48% of patients. Incontinence was mostly minor (flatus incontinence/seepage) and transient, with frank incontinence to stool being reported in only 1% of patients [22].
A recent study from Turkey undertook a retrospective analysis of 417 patients treated with LIS for chronic anal fissure. Only 8 patients (1.9%) developed incontinence problems. Interestingly, 7 affected patients were females who had undergone previous vaginal delivery; the 1 male patient suffering incontinence had undergone prior anorectal surgery. In 5 patients, incontinence resolved completely, with 3 patients continuing to suffer incontinence to liquid stool after 4 months [19].
Nelson et al. conclude in their meta-analysis that the risk for incontinence after LIS is around 5% and is mostly minor (incontinence to flatus). They argue that operative procedures have improved, with the overall incontinence risk now lower than reported in older studies [4].
Several groups have focused on the effect that incontinence after LIS has on quality of life. Hyman followed 35 patients after LIS over a period of 2 years. The Fecal Incontinence Severity Index was measured pre- and postoperatively. Only 3 patients showed a deterioration in continence score, with only 1 patient reporting a deterioration in quality of life [23]. Another study analyzed quality of life in 244 patients after open LIS. Some degree of incontinence was reported in 8 and 3% of patients after 2 and 12 months follow-up, respectively. The Gastrointestinal Quality of Life score improved regardless of complications or continence disturbances. Only 1.2% of patients reported a deterioration in the Fecal Incontinence Quality of Life score [24].
Taking an overview of the above data, one can conclude that incontinence symptoms are suffered by a minority of patients undergoing LIS. A small proportion of patients, however, will experience continence disturbance, but this tends to be minor and transient. This suggests that there is a small subset of patients for whom LIS should be recommended only after appropriate counselling. In the majority of patients with chronic anal fissure, LIS is a safe and effective first-line treatment option.
Groups at risk
Most studies did not assess patients’ preoperative continence levels. Some authors argue that certain patient groups are at a higher risk of postoperative incontinence after LIS than others. For example, Nyam et al. concluded that females were more likely to develop incontinence after a sphincterotomy (females: 53 incontinence vs. males: 33% incontinence), especially after previous vaginal deliveries [18]. As previously mentioned, all 8 patients suffering from incontinence after LIS in Acars’ study either had previous vaginal deliveries or previous anorectal surgery [19]. Elsebea states that LIS could be more invasive than intended in females, because their anal canal is much shorter than in males. He recommends the use of LIS with caution in females who have undergone vaginal deliveries [25]. Several of the national guidelines that favor LIS (Table 1) do so with certain caveats. The Italian guidelines recommend LIS with caution in elderly patients, multiparous women, and patients with previous proctological surgery. The American guidelines exclude patients with previous documented sphincter injuries, anorectal operations, and patients with irritable bowel disease (IBD) from their 1a recommendation for LIS in chronic anal fissure treatment. The UK guidelines recommend preoperative anorectal manometry in these “high-risk” groups, and advocate alternative surgical treatment such as anal advancement flap if anal sphincter pressures are low (Fig. 1).
Practical aspects of LIS
Open vs. closed
Routine administration of preoperative antibiotics and bowel preparation is not usually necessary. According to patient and surgeon’s preferences, LIS can be performed under local, regional, or general anesthesia. Patient positioning is usually in the lithotomy position, but the procedure can also be performed in the lateral decubitus or prone jack-knife position. The operation usually begins with a careful rectal examination and inspection of the anal canal using a retractor. Some authors regularly excise the fissure and occasional secondary hemorrhoids; others leave the fissure itself untouched.
LIS can be performed using either the open or the closed technique. In the open technique, the anoderm is incised over the intersphincteric groove, usually aided by tension applied to the anal canal using a retractor, and the internal sphincter muscle is divided under direct vision. The sphincterotomy is usually performed in the 3’o clock position using a knife or diathermy, but can be performed on either side of the anal canal. In the closed technique, a blade is introduced into the intersphincteric groove and the muscle divided without direct visualization, although often aided by a digit in the anal canal to detect a palpable deficiency in the internal sphincter muscle. Local anesthetic infiltration can be used to facilitate postoperative pain relief in both techniques (Fig. 2).

Graphic illustration of lateral internal sphincterotomy
Comparing the open and closed technique for LIS, the available literature does not suggest significant differences in outcomes so far. In the meta-analysis by Nelson et al., no significant difference between the two techniques was found for fissure healing or incontinence rates [14]. A similar finding was reported by Wiley et al., who randomized 79 patients to either open or closed LIS [26].
Classical, conservative, or tailored LIS?
During a classical LIS, the internal sphincter muscle is divided along the entire length of the anal canal, or at least up to, if not beyond, the dentate line. In recent years, a more conservative approach has been advocated, whereby the internal anal sphincter muscle is divided to a level coinciding with the apex of the fissure. Another option, the so-called tailored sphincterotomy, involves division of the muscle by either 20, 40, or 60% according to preoperative manometric findings, thus allowing the sphincterotomy to be limited to the region of sphincter hypertension [27].
Mentes et al. investigated the effect of classical sphincterotomy in comparison to conservative sphincterotomy. A total of 76 patients were randomized into a classical group (division of muscle up to dentate line or higher) and a conservative group with muscle division up to the fissure apex only. The classical group experienced statistically significantly quicker fissure healing and a 100% healing rate after 12 months, whereas the conservative group showed 13.2% of patients experiencing treatment failure after 12 months (one non-healing, four recurrences). The changes between pre- and postoperative anal incontinence scores were not significantly different between groups; however, a significant change in anal incontinence scores (AIS) compared to baseline could only be observed in the classical group [28]. Some authors have reported lower fissure healing rates with the conservative approach, whilst others have shown a comparable success rate. For example, Garcea et al. demonstrated a 97% healing rate in 60 patients at 6 weeks following conservative sphincterotomy [29]. In their meta-analysis, Nelson et al. reported higher healing rates following classical LIS, with no difference in incontinence rates as compared to conservative sphincterotomy [4].
The tailored or “calibrated” sphincterotomy consists of individualizing sphincterotomy for each patient, depending on the extent of sphincter hypertension. In the study of Rosa et al., 388 patients underwent tailored sphincterotomy over a 5-year period. Whereas 122 patients were lost to follow-up, of the remaining 261, 97% had fissure healing after 8 months. Only 1 patient reported disturbance of continence [27].
Although there is merit in attempting to modify the extent of sphincterotomy to reduce continence disturbance, at least for high-risk patients, the accuracy by which muscle division can be aligned to sphincter hypertension is, in the authors’ opinion, questionable.
Posterolateral vs. lateral internal sphincterotomy
Alawady et al. [30] have recently described the concept of posterolateral sphincterotomy, whereby the sphincterotomy is performed at the 5 o’clock position as opposed to the 3 o’clock position in classical LIS. The hypothesis behind this approach is that a greater reduction in sphincter pressure is achieved by sphincterotomy at a posterolateral position, due to higher resting pressures in this region of the internal sphincter []. Forty-nine patients were randomized to either posterolateral sphincterotomy at 5 o’clock or classical sphincterotomy, whereby the same amount of internal sphincter muscle (8–10 mm) was divided in each group. There was a significantly shorter healing time and lower postoperative pain score in the posterolateral group, as well as a greater reduction in anal pressure as measured by manometry. The incidence of continence disturbance was lower in the posterolateral group, but did not reach statistical significance.
Conclusion
A view from a UK proctology practice
The text below comprises a summary of the authors’ practice, derived from experience in a tertiary referral coloproctology unit in the UK and based on the above evidence and national guidelines.
Although the focus of discussion has been on LIS, there is a place for examination under anesthesia (EUA) and Botox in chronic anal fissure. EUA confirms the diagnosis and permits exclusion of other proctological conditions. Botox injection is easy and safe, and, if successful, spares the patient unnecessary sphincterotomy. In patients who relapse following Botox, there is a logical rationale for proceeding with a permanent sphincterotomy. For these reasons, the majority of patients with chronic anal fissure receive a trial of Botox injection prior to proceeding to LIS in our institution.
Open LIS is the procedure of choice in the majority of patients with chronic anal fissure, but this is usually restricted to a conservative rather than a classical sphincterotomy, aiming to minimize the risk of postoperative incontinence. In the authors’ opinion, open sphincterotomy is far superior to closed sphincterotomy in terms of the accuracy of muscle division—failure to complete the sphincterotomy will lead to fissure recurrence. The authors’ question the accuracy of mapping the extent of sphincterotomy to the degree of high anal canal pressure, and therefore the validity of the tailored sphincterotomy.
As regards fissurectomy, the authors are skeptical that simply “freshening” the mucosal ulcer is sufficient to bring about fissure healing, because it fails to address the underlying sphincteric hypertension, and believe that fissure recurrence is a too frequent outcome. Similarly, anodermal advancement flap is rarely practiced because of the propensity for anodermal wounds to become infected and breakdown, often leaving the patient in a worse condition.
The authors accept that LIS is not a panacea for all chronic anal fissures. There is clearly a small proportion of patients with existing anal sphincter weakness in whom further muscle division will lead to continence disturbance, even if minor and transient. They therefore take the view articulated in the Association of Coloproctology of Great Britain and Ireland (ACPGBI) guidelines, that any patient with suspected sphincter weakness should be investigated preoperatively by anal manometry and endoanal ultrasound (Fig. 1). Evidence of existing sphincter weakness should be a signal to proceed to sphincterotomy with caution, with consideration given to alternative treatments that leave the internal anal sphincter intact.
References
Cross KL, Massey EJ, Fowler AL, Monson JR (2008) The management of anal fissure: ACPGBI position statement. Colorectal Dis 10(Suppl3):1–7
Dykes SL, Madoff RD (2007) Benign anorectal: anal fissure. In: The ASCRS textbook of colon and rectal surgery. Springer, New York, pp 178–191
Aigner F (2008) Letter to the editor: fissurectomy for treatment of anal fissures. Dis Colon Rectum 51:1163
Nelson RL et al (2011) Operative procedures for fissure in ano. Cochrane Database Syst Rev. https://doi.org/10.1002/14651858.CD002199.pub4
Alonso-Coello P et al (2008) Guia de practica clinica sobre el manejo de la fisura anal. Gastroenterol Hepatol 31(10):668–681
Altomare et al (2011) The management of patients with primary chronic anal fissure: a position paper. Tech Coloproctol 15:135–141
Raulf F et al (2008) AWMF, Leitlinien der Deutschen Gesellschaft für Koloproktologie
American Society of Colon and Rectal Surgeons, Stewart D et al (2017) Clinical practice guidelines for the management of anal fissures. Dis Colon Rectum 60:7–14
Wald A et al (2014) ACG clinical guideline: management of benign anorectal disorders. Am J Gastroenterol 109:1141–1157
Eisenhammer S (1959) The evaluation of the internal anal sphincterotomy operation with special reference to anal fissure. Surg Gynecol Obstet 109:583–590
Parks AG (1967) The management of fissure in ano. Hosp Med 1:737
Notaras MJ (1969) Lateral subcutaneous sphincterotomy for anal fissure: a new technique. Proc R Soc Med 62:713
Memon AS, Siddiqui FG, Hamad A (2010) Fissurectomy with posterior midline sphincterotomy for management of chronic anal fissure. J Coll Physicians Surg Pak 20(4):229–223
Nelson RL et al (2017) A systematic review and meta-analysis of the treatment of anal fissure. Tech Coloproctol 21(8):605–625
Ebinger et al (2017) Operative and medical treatment of chronic anal fissures—a review and network meta-analysis of randomized controlled trials. J Gastroenterol 52:663–676
Mousavi S, Sharifi M, Mhedikha Z (2009) A comparison between the results of fissurectomy and lateral internal sphincterotomy in the surgical management of chronic anal fissure. J Gastrointest Surg 13:1279–1282
Hasse et al (2004) Lateral partial sphincter myotomy as therapy of chronic anal fissure: long term outcome of an epidemiological cohort study. Chirurg 75:160–167
Nyam DC, Pemberton JH (1999) Long-term results of lateral internal sphincterotomy for chronic anal fissure with particular reference to incidence of fecal incontinence. Dis Colon Rectum 42(10):1306–1310
Acar T et al (2019) Treatment of chronic anal fissure: is lateral open sphincterotomy a safe and adequate option? Asian J Surg 42:628–633
Vaithianathan R, Panneerselvam S (2015) Randomised Prospective Controlled Trial of Topical 2% Diltiazem Versus Lateral Internal Sphincterotomy for the Treatment of Chronic Fissure in Ano. Indian Surg 77(Suppl 3):1484–1487
Hancke E, Schwaner S (2003) Chronische Analfissur – Operative Behandlung mit Analdilatation, Exzision der Analfissur versus laterale Sphinkterotomie. coloproctology 25:95–105
Garg P, Garg M, Menon G (2013) Long-term continence disturbance after LIS for chronic anal fissure: a systematic review and meta-analysis. Colorectal Dis 15:e104–e117
Hyman N (2004) Incontinence after lateral internal sphincterotomy: a prospective study and quality of life assessment. Dis Colon Rectum 47(1):35–38
Mentes et al (2006) Results of lateral internal sphincterotomy for chronic anal fissure with particular reference to quality of life. Dis Colon Rectum 49(7):1045–1051
Elsebae M (2007) A study of fecal incontinence in patients with chronic anal fissure: prospective, randomized, controlled trial of the extent of internal anal sphincter division during lateral sphincterotomy. World J Surg 31:2052–2057
Wiley et al (2004) Open vs. closed lateral internal sphincterotomy for idiopathic fissure-in-ano: a prospective, randomized, controlled trial. Dis Colon Rectum 47(6):847–852
Rosa et al (2005) Calibrated LIS for chronic anal fissure. Tech Coloproctol 9(2):127–131
Mentes et al (2005) Extent of lateral internal sphincerotomy: up to the dentate line or up to the fissure apex. Dis Colon Rectum 48(2):365–370
Garcea G et al (2003) Results following conservative lateral sphincterotomy for the treatment of chronic anal fissures. Colorectal Dis 5(4):311–314
Alawady M, Emile S, Abdelnaby M, Elbanna H, Farid M (2018) Posterolateral versus lateral internal anal sphincterotomy in the treatment of chronic anal fissure: a randomized controlled trial. Int J Colorectal Dis 33:1461–1467
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
M. Holzgang and D. Jayne declare that they have no competing interests.
For this article no studies with human participants or animals were performed by any of the authors. All studies performed were in accordance with the ethical standards indicated in each case.
Rights and permissions
About this article

Cite this article
Holzgang, M., Jayne, D. Lateral internal sphincterotomy (LIS)—still top gun in chronic anal fissure treatment?. coloproctology 42, 478–484 (2020). https://doi.org/10.1007/s00053-020-00454-9
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00053-020-00454-9
Keywords
- Postoperative incontinence
- Conservative sphincterotomy
- Anorectal surgery
- Fissurectomy
- Botulinum toxin injection