
Abstract
Background
Anal fissure has a very large number of treatment options. The choice is difficult. To assist in this choice, presented herein is a summary of a systematic review and meta-analysis of all published treatments for anal fissure that have been studied in randomized controlled trials up through 2016.
Methods
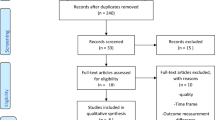
The review is divided into those studies that compared two or more surgical procedures and those that had at least one arm that was nonsurgical. Studies were further categorized by the specific interventions and comparisons. The outcome assessed was the inverse of sustained cure of the fissure, i.e., treatment failure. In addition, the harms of treatment assessed were headache and anal incontinence. Risk of bias was assessed for each study and the strength of the evidence of each comparison was assessed using Grading of Recommendations, Assessment, Development and Evaluations (GRADE).
Results
A total of 148 eligible trials were found and assessed, 31 in the surgical group (2606 patients) and 117 in the nonsurgical group (9456 patients). There were 14 different operations described in the surgical group and 29 different nonsurgical treatments in the nonsurgical group along with partial lateral internal sphincterotomy (LIS). There were 61 different comparisons. Of these, 47 were reported in two or fewer studies, usually with quite small populations. The largest single comparison was glyceryl trinitrate (GTN) versus control with 19 studies. GTN was more effective than control in terms of sustained cure (odds ratio = 0.68; 95% confidence interval = 0.63–0.77) but the quality of evidence was very poor due to severe heterogeneity and risk of bias due to inadequate clinical follow-up. The only comparison to have a high GRADE quality of evidence was a subgroup analysis of LIS versus any medical therapy, with outcome of treatment failure (0.12; 0.07–0.21) and mild incontinence (4.41; 1.97–9.87) assessed after at least 6 months from surgery. There were 12 studies in this analysis, the medical therapy being GTN in 6, Botox in 5, and calcium channel blocker (CCB) in 1. Most of the other analyses were downgraded in GRADE due to imprecision, i.e., too few or too small studies, and significant heterogeneity in almost all other comparisons with more than six studies.
Conclusion
LIS is superior to nonsurgical therapies in achieving sustained cure of fissure with an increased risk of mild incontinence, usually meaning flatus. CCBs were more effective than GTN and had less risk of headache, but with only a low quality of evidence. Anal incontinence, once thought to be a frequent risk with LIS, was found in various subgroups in this review to have a risk between 3.4 and 4.4%. Among the surgical studies, manual anal stretch (Lord procedure) performed worse than LIS in the treatment of chronic anal fissure in adults. For those patients requiring surgery for anal fissure, open LIS and closed LIS appear to be equally efficacious, with a moderate GRADE quality of evidence. Most other GRADE evaluations of procedures were low to very low, due mostly to imprecision.
Zusammenfassung
Hintergrund
Die Behandlungsmöglichkeiten einer Analfissur sind zahlreich. Die Wahl ist schwierig. Um bei der zu treffenden Auswahl zu unterstützen, präsentiert der vorliegende Beitrag die Zusammenfassung eines systematischen Reviews und einer Metaanalyse aller Analfissurbehandlungen, die bis 2016 in randomisierten kontrollierten Studien untersucht wurden.
Methoden
Der Review differenziert zwischen jenen Studien, in denen 2 oder mehr chirurgische Eingriffe miteinander verglichen wurden, und solchen, bei denen mindestens eine Studiengruppe nichtchirurgisch behandelt wurde. Die Studien wurden durch die spezifischen Interventionen und Vergleiche weiterkategorisiert. Untersucht wurde das Gegenteil der anhaltenden Heilung der Fissur – das Therapieversagen. Zusätzlich wurden Kopfschmerzen und Stuhlinkontinenz als Komplikation der Behandlung analysiert. Das Verzerrungspotenzial wurde für jede Studie bewertet, und die Stärke der Evidenz jedes Vergleichs wurde unter Verwendung des Grading of Recommendations, Assessment, Development and Evaluations (GRADE) beurteilt.
Ergebnisse
Es wurden 148 auswertbare Studien identifiziert und bewertet, 31 in der chirurgischen Gruppe (2606 Patienten) und 117 in der nichtchirurgischen Gruppe (9456 Patienten). In der chirurgischen Gruppe wurden 14 verschiedene Operationen und in der nichtchirurgischen Gruppe 29 verschiedene nichtchirurgische Behandlungen sowie die partielle laterale interne Sphinkterotomie (LIS) beschrieben. Es wurden 61 Vergleiche durchgeführt. Davon gab es zu 47 Vergleichen nur 2 oder weniger Studien, normalerweise mit relativ kleinen Studienpopulationen. Die größte Analyse umfasste 19 Studien und verglich Glyceryltrinitrat (GTN) gegen Placebo bzw. herkömmliche Therapie. Glyceryltrinitrat war bezüglich anhaltender Heilung wirksamer („odds ratio“ [OR] = 0,68; 95 %-Konfidenzintervall [95 %-KI] 0,63–0,77), aber die Evidenzqualität war aufgrund schwerer Heterogenität und des Risikos einer Verzerrung aufgrund unzureichender klinischer Nachsorge sehr schlecht. Der einzige Vergleich, der einen GRADE-Qualität hoher Evidenz „high“ aufwies, war eine Untergruppenanalyse von LIS im Vergleich zu einer medizinischen Therapie. Dieser ergab eine OR für Therapieversagen von 0,12 (95 %-KI: 0,07–0,21) und für milde Inkontinenz von 4,41 (95 %-KI: 1,97–9,87), nach einer Nachbeobachtungszeit von mindestens 6 Monaten. Diese Analyse umfasste 12 Studien, wobei die medizinische Therapie in 6 Studien die GTN-, in 5 Studien die Botox- und in einer Studie die Kalziumkanalblocker(CCB)-Anwendung betraf. Die meisten anderen Analysen wurden in der GRADE-Bewertung aufgrund von Ungenauigkeit, d. h. zu wenige, zu kleine Studien, und/oder aufgrund signifikanter Heterogenität herabgestuft. Letzteres fand sich in fast allen anderen Vergleichen mit mehr als 6 Studien und war meistens auf unvollständige Nachkontrolluntersuchungen zurückzuführen.
Schlussfolgerungen
Die LIS ist nichtchirurgischen Therapien bezüglich der Effektivität der Analfissurbehandlung überlegen. Andererseits geht eine LIS mit einem höheren Risiko für eine anhaltende milde Stuhlinkontinenz einher, zumeist für Flatus. Kalziumkanalblocker waren wirksamer als GTN und mit einem geringeren Risiko für Kopfschmerzen assoziiert, bei jedoch nur geringer Evidenzqualität. Die Stuhlinkontinenz, die früher als häufige Komplikation nach LIS beschrieben wurde, wurde in dieser Metaanalyse in verschiedenen Untergruppen bei 3,4–4,4 % der Patienten festgestellt.
In der Analyse zum Vergleich der chirurgischen Therapien chronischer Analfissuren beim Erwachsenen ergaben sich für die manuelle Analdilatation (nach Lord) schlechtere Resultate als für die LIS. Die offene und die geschlossene LIS scheinen zur Behandlung der Analfissur gleichermaßen wirksam zu sein, bei mäßiger Evidenzqualität. Alle anderen GRADE-Bewertungen zu Vergleichen von operativen Verfahren waren niedrig bis sehr niedrig, hauptsächlich aufgrund von Ungenauigkeiten des Vergleichs.
Similar content being viewed by others

Avoid common mistakes on your manuscript.
Anal fissure and incontinence, a history
Anal fissure is rarely mentioned by any ancient author. Sushruta, Hippocrates, and Galen all write extensively about hemorrhoids and fistula, including surgical treatment. Usually, cauterization and ulcers are mentioned but never separated from hemorrhoids or fistula. Abū Bakr Muḥammad ibn Zakariyyā ar-Rāzī does specifically mention fissure but felt it was due to constipation and was treated with laxatives [3]. John of Arderne does mention fissuring associated with tenesmus but felt that it was secondary to piles rather than a specific diagnosis [19]. The treatment was nonsurgical.
It was not until the 19th century that fissure seems to have been recognized as a specific diagnosis and that surgical intervention was needed for its cure. The birth of sphincterotomy was attributed to Alexis Boyer’s eleven-volume Traitē des Maladies Chirurgicales published between 1818 and 1826 [4]. The operation described is slightly different from that which is performed today. The extent of sphincterotomy is not delineated, nor is it in most publications today. In a very thorough and fascinating book by Bodenhamer about just anal fissure published in 1868, it is stated that although fissure had been rarely described, Ambrose Pare may have described the same operation and Albucasis described a more conservative incisional approach at the end of the tenth century [4]. The number of surgeons actively involved in investigating the surgical treatment of fissure at that time (19th century) and communicating their results was outstanding. Not only efficacy in pain relief and healing were described, but also harms of the procedures including incontinence. The procedure of Boyer was regarded as too extensive and a lesser incision recommended, especially for continence preservation.
Another approach described in this book [4] is forced dilation as a method for relieving the outlet obstruction associated with fissure. One operation of some note was that of Maisonneuve, who inserted his whole hand and then closed his fist upon withdrawal. The risk of incontinence was obviously recognized with this procedure and so lesser dilatations were investigated, including a two-thumbs stretch to the ischial tuberosities. This was also found to have a high risk of incontinence and so there was, finally, description of just two index fingers being inserted until a release was palpated. All that these surgeons seem to have been lacking in their investigations were the statisticians. No numerical data were published.
In the 1920s a now old disease got a new name: pectenosis [2]. The previously described internal sphincter fibers were thought to have undergone fibrosis, they so were called a pectin band. The preferred method of treatment was to incise the fibers, apparently away from the fissure in most descriptions until the anus could accommodate a two-finger insertion—a much more conservative procedure than Maisonneuve’s or Boyer’s procedures. It was subsequently found that the presumed fibrosis was intact spastic internal sphincter fibers. By the late 1930s attention had shifted to the external sphincter, with injections or actual division of external fibers by Gabriel [6]. Kilbourne also raised the possibility that fissures could be caused by tuberculosis or syphilis at that time [12].
Then, in 1951, Eisenhammer described the partial lateral internal sphincterotomy (LIS), though he combined this with a rather liberal dilation of the anal canal after the sphincterotomy. He was, I believe, the first to list the number of patients treated by his method and states that none had any defecation difficulties afterwards [5]. This procedure was enthusiastically adopted by surgeons around the world. It was also thought by others that anal incontinence (AI) was not an issue [1, 20]. The first publication to quantify AI was in 1985 and it stated that of 306 patients who had had LIS at least 1 year earlier, only 15 suffered from any degree of AI, principally to flatus. In none was it severe enough for the patient to wear a pad [20].
However, in 1989, everything changed. Khubchandani published a large case series of follow-up after LIS in which 36% of the patients were incontinent to flatus and 5% to solid stool [13]. In 1996, in a new retrospective comparison of open vs. closed LIS, the University of Minnesota, which had reported such low incontinence rates in 1985 [20], found that 30.3% of their patients were incontinent to flatus and 11.8% to solid stool [7]. One report found that AI progressed over time in those with early AI after LIS [9]. The age of glyceryl trinitrate (GTN), Botox, and calcium channel blockers (CCBs) was born. In many countries it appears that LIS had been abandoned in favor of medical therapy [18]. Yet patient satisfaction with LIS has been reported to be high [10]. The often-crippling pain of fissure is almost immediately relieved by LIS. The rest of us wondered: “Where are all these incontinent patients?” American surgeons ask, “We are experts in AI too, and we do not see AI due to LIS in our clinics.” At a meeting of the American Society of Colorectal Surgeons in Chicago in 2008, a speaker asked the audience if any surgeon had performed an internal sphincter repair on a patient in whom he had performed a LIS? Could that person please stand up? Nobody stood up. I have never performed such a repair. Why do patient satisfaction studies of LIS show high satisfaction with the procedure [10]? How can there be such a large difference in AI seen in retrospective surveys and randomized trials?
Why has the risk of AI after LIS declined in the current century? There are several possibilities to consider. More haphazard ascertainment is unlikely, since the protocols of all randomized trials are carefully scrutinized by ethics committees. Might the operation have changed? I think this is likely only insofar as all surgeons are extremely aware of the risk of incontinence related to LIS. If anything, the extent of sphincterotomy (or concomitant dilation) has diminished without apparently diminishing efficacy. This is exactly what was described by Bodenhamer in the USA in the 1860s, wherein the LIS, which was quite extensive in the description of Boyer, was barely more than a mucosal incision with Bodenhamer, and he described good results [4]. The length of the sphincterotomy has been studied: either extending proximally to the dentate line or just to the level of the proximal margin of the fissure. The longer incision showed insignificantly better efficacy but slightly worse continence [15].
Or possibly different patients are receiving the surgery, which I also think is likely. There may be more careful selection of those patients with an obviously hypertrophied internal sphincter and stenotic anal orifice for surgery, and not just anybody with an anal fissure. Reasonable medical therapies are now available for most fissure patients. This also suggests that, for instance, patients with fissure but no hypertrophy or stenosis may have been more prone to postoperative incontinence and are now being treated medically. But these are both guesses.
Myths concerning fissure and incontinence
Posterior midline partial internal sphincterotomy is thought to leave a keyhole defect in the distal anal canal that results in incontinence of flatus (Fig. 1).

A keyhole defect after posterior partial internal sphincterotomy. (From: [21])
All LIS—open or closed, posterior or lateral—have been found in ultrasound examination to leave a keyhole defect and there are no data from randomized trials to suggest that either efficacy or incontinence are greater with any of the sphincterotomy locations [15].
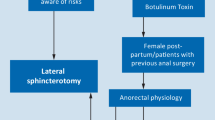
Acute anal fissure should never be operated upon. It is generally thought that chronic fissures arise from pre-existing acute fissures (of course) but that the hypertrophy and stenosis of the sphincter take time to develop. This will not happen in many acute fissure patients, and surgery need not be considered until this has happened. Fine. In order to defend the above statement, step one is for there to be general agreement as to what constitutes an acute anal fissure. Physical findings can certainly separate them. With many fissures there is no doubt that they are chronic, but there is no general agreement as to duration. Some very chronic fissures look very acute, and the published definition of chronicity varies from 2 weeks to 6 months. In today’s climate, most patients with an acute-looking fissure will be started on GTN and by the time it has failed, they have usually crossed the chronicity dateline. It seems prudent that LIS should still not be considered in these patients unless sphincter hypertrophy and anal stenosis are present and the appearance is otherwise not atypical. But clinical trials dealing with only acute fissure do exist and do not report horrible outcomes [15].
The most pernicious myth is that LIS causes permanent AI. This phrase introduces virtually every publication about medical treatment of anal fissure. There is no such thing as untreatable permanent AI, as anyone who has run an AI clinic knows. All forms of AI have treatments that are often very effective. And AI due to LIS should be eminently treatable—surgically or medically. It is much more likely, for instance, that AI in obstetric patients who have had vaginal delivery and subsequent AI pose greater problems. Or patients with inflammatory bowel disease. In postpartum women muscle repair is often ineffective, most likely due to pelvic floor nerve damage during pregnancy or delivery [16]. Nor have epidemiologic studies of AI reported LIS to be a risk factor [17], in spite of the findings of Hasse [9]. There is no pelvic nerve damage to cause the AI in anal fissure; just a simple controlled muscular division, easily repaired. But there are no published or registered clinical trials related to this procedure, although there is some anecdotal experience [14].
Medical therapy cannot lead to AI. See Table 1 of adverse events that can occur in the treatment of anal fissure (from the systematic review mentioned in the Abstract [15]).
Medical therapy cannot lead to AI
Medical therapy is highly effective in curing fissure. Not really. The studies with high cure rates had assessment of continence much too early after the treatment to establish cure. Fissures wax and wane both symptomatically and on physical examination. Very high recurrence rates have been reported in patients whose fissures were initially healed by GTN if they had 1 year of follow-up: 51% [11] and 67% [8].
Manual anal dilation is inferior to LIS, but recent small studies suggest that more controlled dilation, either pneumatic, by speculum, or by patients at home, is equally effective to LIS and with no incontinence risk. As stated in the abstract, these studies are crippled by random error due to small sample sizes in few studies [15].
Conclusion
The systematic review summarized in the Abstract covers a huge number of interventions, too many to fit in this paper. The History and Myths sections above attempt to further summarize those analyses by addressing questions raised in fissure therapy. It is unwise to tell a patient that LIS will result in permanent AI. It is similarly unwise to tell a patient that GTN or any of the alternatives are as good as surgery. Patients deserve an informed choice and to know that alternatives always exist. This is still fertile turf for clinical trials, with 28 new randomized trials published since 2015.
Abbreviations
- AI:
-
Anal incontinence
- Botox:
-
Botulinum toxin
- CCB:
-
Calcium channel blockers
- GTN:
-
Glyceryl trinitrate
- LIS:
-
Partial lateral internal sphincterotomy
References
Abcarian H (1980) Surgical correction of chronic anal fissure: results of lateral internal sphincterotomy vs. fissurectomy—midline sphincterotomy. Dis Colon Rectum 23(1):31–36
Abel AL (1932v) The pecten, pecten band, pectenosis and pectenotomy. Lancet 1(5666):714–718
AL-Humadi AH, Al-Samarrai S (2009) Treatment of anorectal diseases by al-Rāzī. J Indian Med Assoc 41:122–134
Bodenhamer W (1868) Practical observations on the aetiology, pathology, diagnosis and treatment of anal fissure. Wm Wood & Co, New York
Eisenhammer S (1951) The surgical correction of chronic internal anal (sphincteric) contracture. S Afr Med J 25:486–489
Gabriel WB (1939) Anal Fissure. Br Med J 1(4079):519–521
Garcia-Aguilar J, Belmonte C, Wong WD, Lowry AC, Madoff RD (1996) Open vs. closed sphincterotomy for chronic anal fissure: long-term results. Dis Colon Rectum 39(4):440–443
Graziano A, Svidler Lopez L, Lencinas S, Masciangioli G, Gualdrini U, Bisisio O (2001) Long-term results of topical nitroglycerin in the treatment of chronic anal fissures are disappointing. Tech Coloproctol 5(3):143–147
Hasse C, Brune M, Bachmann S, Lorenz W, Rothmund M, Sitter H (2004) Lateral, partial sphincter myotomy as therapy of chronic anal fissue. Long-term outcome of an epidemiological cohort study. Chirurg 75(2):160–167
Hyman N (2004) Incontinence after lateral internal sphincterotomy: a prospective study and quality of life assessment. Dis Colon Rectum 47:35–38
Jonas M, Lund JN, Scholefield JH (2002) Topical 0.2 % glyceryl trinitrate ointment for anal fissure: Long-term efficacy in routine clinical practice. Colorectal Dis 4(5):317–320
Kilbourne NJ (1931) The injection treatment of anal fissure. Cal West Med 35(5):384
Khubchandani IT, Reed JF (1989) Sequelae of internal sphincterotomy for chronic fissure in ano. Br J Surg 76(5):431–434
Najarian M (2006) Surgeons’ beliefs and experiences with the surgical treatment of anal fissure. Semin Colon Rectal Surg 17:116–119
Nelson RL, Manuel D, Gumienny C, Spencer B, Patel K, Schmitt K, Castillo D, Bravo A, Yeboah-Sampong A (2017) A systematic review and meta-analysis of the treatment of anal fissure. Tech Coloproctol 21(8):605–625. https://doi.org/10.1007/s10151-017-1664-2
Nelson RL, Go C, Darwish R, Gao J, Parikh R, Kang C, Mahajan A, Habeeb L, Zalavadiya P, Patnam M (2019) Cesarean delivery to prevent anal incontinence: a systematic review and meta-analysis. Tech Coloproctol 23(9):809–820. https://doi.org/10.1007/s10151-019-02029-3
Nelson RL (2017) Epidemiology of anal incontinence. In: Abrams P, Cardozo L, Wagg A, Wein A (eds) 6th Internatonal Consultation on Incontinence, 6th edn. ICS.2017.
Ommer A (2015) Management of complications of fissure and fistula surgery. Chirurg 86(8):734–740
Power D (ed) (1910) Treatises of Fistula m Ano Haemorrhoids, and Clysters, from an early fifteenth-century manuscript translation of John Arderne, Kegan Paul. Published for The Early English Text Society by the Oxford University Press, London, New York, Toronto
Walker WA, Rothenberger DA, Goldberg SM (1985) Morbidity of internal sphincterotomy for anal fissure and stenosis. Dis Colon Rectum 28(11):832–835
Nelson R (2017) Anal fissure. In: Abcarian H, Cintron J, Nelson R (eds) Complications of anorectal surgery. Springer, Cham
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author, R. Nelson, has no conflicts of interest related to anal fissure or any medication described in this manuscript.
For this article, no studies with human participants or animals were performed by any of the authors. All studies performed were in accordance with the ethical standards indicated in each case.
Rights and permissions
About this article

Cite this article
Nelson, R. Anal fissure and lateral internal sphincterotomy. coloproctology 42, 445–449 (2020). https://doi.org/10.1007/s00053-020-00479-0
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00053-020-00479-0