
Abstract
Introduction
Sepsis is a complex inflammatory disorder believed to originate from an infection by any types of microbes and/or their products. It is the leading cause of death in intensive care units (ICUs) throughout the globe. The mortality rates depend both on the severity of infection and the host’s response to infection.
Methods
Literature survey on pathobiology of sepsis in general and failure of more than hundred clinical trials conducted so far in search of a possible cure for sepsis resulted in the preparation of this manuscript.
Findings
Sepsis lacks a suitable animal model that mimics human sepsis. However, based on the results obtained in animal models of sepsis, clinical trials conducted so far have been disappointing. Although involvement of multiple mediators and pathways in sepsis has been recognized, only few components are being targeted and this could be the major reason behind the failure of clinical trials.
Conclusion
Inability to recognize a single critical mediator of sepsis may be the underlying cause for the poor therapeutic intervention of sepsis. Therefore, sepsis is still considered as a disease—in search of cure.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
“Small creatures, invisible to the eye, fill the atmosphere and breathed through the nose cause dangerous diseases”—a definition for Sepsis given by an ancient Roman scholar and writer—Marcus Terentius Varro (116 BC–27 BC) [1]. Today, the world’s human population has crossed seven billion and the technology in the field of healthcare to predict/manage diseases is also developed to a great extent. Despite such great advancements in science, human population is still susceptible to diseases caused by pathogenic microorganisms and one such disease/syndrome that has become a nightmare is “SEPSIS”—a condition of overwhelming systemic inflammation initiated in response to an infection by microbes and/or their released endotoxins leading to multiple organ dysfunction syndrome (MODS) and death [2, 3].
Sepsis accounts for high mortality rates standing at more severe than breast cancer, prostate cancer and HIV/AIDS combined [4], or Hepatitis [5] and continues to be a major life threatening condition, taking more and more lives. The causative agents/organisms behind this devastating syndrome are believed to be microbes [6, 7] and/or their products [8].
Hyperactivation of the inflammatory response is a remarkable feature of sepsis, which can be initiated at any site vastly by bacteria and/or its prime product—Lipopolysaccharide (LPS) [9]. However, targeting either whole bacteria [10] or LPS [11], their receptors [12] and the downstream pro-inflammatory mediators [11] involved in exaggerating the inflammation never lead to a fruitful outcome of reducing mortality. This indicates the involvement of other bacterial components such as membrane lipoproteins in exaggerating the inflammatory process, which are previously unappreciated.
Quantification of pro-inflammatory cytokines is an extensively employed method to determine the extent of inflammatory insult and this holds good in case of sepsis too [13]. Besides, few molecules are identified as the early mortality predictors, where their levels predict the early mortality of patients with severe sepsis [14–17]. Although these early mortality predictors are proven to be the best markers of severe sepsis, they need extensive validation for their use in clinical practice [18, 19].
With the failure of more than 100 clinical trials [20] and early-goal directed therapy (EGDT) formulated by the “Surviving Sepsis Campaign” (SSC) committee [21] in reducing the mortality of patients with severe sepsis and septic shock, researchers are now concentrating on several new strategies so as to come up with an efficient drug to overcome this devastating disease.
Although proven to be successful in animal models of sepsis, none of the drugs reached the market, clearing the hurdles of clinical trials. These unsatisfactory results obtained in translating the treatment options to bedside may be attributed to the disadvantages of each animal model employed in the studies [22]. Besides, development of new strategies employing modern technology for the identification of cause and disease progression, use of combination of drugs and identification of new markers which can predict the mortality of a patient have led to the better understanding of pathophysiology associated with the diseased state.
Definitions for sepsis
Although, the word ‘sepsis’ is under use for more than 2700 years [23], a perfect and universally agreeable definition was lacking to define sepsis and related disorders. To solve this issue, and to provide a conceptual and practical framework to define the systemic inflammatory response to an infection, the American College of Chest Physicians (ACCP) and the Society of Critical Care Medicine (SCCM) hosted a “Consensus Conference” in August 1991 [24] at Chicago, USA and designed various criteria for defining sepsis and related disorders (Fig. 1). These definitions served as the basis for designing inclusion criteria for various clinical trials and also helped in better understanding of the pathophysiology associated with sepsis and related disorders. Based on the subsequent understandings in the pathophysiology of sepsis, experts in the field decided to revisit and modify the earlier definition of sepsis so as to reflect the recent understandings in the pathophysiology of sepsis and related disorders. The “International Sepsis Definitions Conference—2001”, jointly organized by SCCM, The European Society of Intensive Care Medicine (ESICM), ACCP, the American Thoracic Society (ATS), and the Surgical Infection Society (SIS) in Washington D.C. USA [25], resulted in no new or better definitions, as there was no evidence in support of replacing the existing definitions for sepsis and related disorders and hence, the earlier definitions were retained (Fig. 1).

Classification of sepsis based on the severity of infection and criteria for defining each group
The SCCM in association with ESICM and the International Sepsis Forum (ISF) initiated “Surviving Sepsis Campaign” (SSC) in the year 2002. The goal was to understand the pathophysiology of sepsis and related disorders, designing appropriate definitions, improving diagnosis, and treatment options thereby to reduce the mortality rate due to severe sepsis and septic shock. To date the SSC committee has met four times and has successfully put forth the international guidelines for management of severe sepsis and septic shock in the SSC-2012 meeting [26]. A 7.5 year study as per SSC-2004 guidelines by Levy et al. [27] to determine the association of compliance with the SSC performance bundles and mortality indicates a 25 % relative risk reduction in mortality rate.
Epidemiology of sepsis
Sepsis and related disorders are the leading cause of death throughout the world accounting for 19 million cases each year [28] and 1,400 deaths each day [29]. In a developed country like United States alone, the incidence of sepsis is estimated to be 1,655,000 [30] resulting in more than 250,000 deaths each year [31]. This has become a major economic burden to United States that accounts for a total of $16.7 billion towards healthcare [29].
The result of a multicentre, prospective observational study of 5478 patients admitted at various Intensive Care Units (ICUs) in India shows 25 % of the patient admissions are due to SIRS and organ dysfunction. Out of all admissions the incidence of severe sepsis was 16.45 % and the mortality rate was 12.08 %, of which 59.26 % of patients died of severe sepsis [32].
What are the causes of sepsis?
Sepsis is a result of an infection from any microorganisms (Bacteria/Virus/Fungi) [33] with bacteria being the commonest (Table 1). It is estimated that there are ten bacteria for every human cell and human evolution occurred in parallel with bacteria [34], allowing them to symbiotically inhabit many vital organs such as buccal cavity, gastro-intestinal tract, skin and nasal linings of human body. However, many times, when our microbial neighbors penetrate previously negotiated boundaries, complications arise.
The infection, being the primary cause, can be initiated anywhere in the body, especially in the urinary tract [35], abdomen [36], blood stream [37] or lungs [38]. The microbial invasion activates the host immune system leading to the recruitment of first line of cells of innate immune system. These immune cells abrogate the further invasion and multiplication of microbes by phagocytosis and killing [39]. However, the results of two popular clinical trials [40, 41] using anti-microbial components as a possible cure for sepsis syndrome was in vain. This indicates whole bacteria are not a prerequisite for initiating sepsis. Even the fragmentation products produced after bacterial killing by phagocytic cells are probably more than sufficient to elicit a strong inflammatory response leading to sepsis, as evident from the negative blood cultures obtained in severe sepsis patients [42]. One such component of gram-negative bacterial membrane, widely employed as a surrogate endotoxin in research is the Lipopolysaccharide (LPS).
Lipopolysaccharide (LPS): the bacterial endotoxin
LPS is the major component of gram-negative bacterial membrane. It is under experimental research since its discovery in 1894 by a German Physician, Richard Friedrich Johannes Pfeiffer who coined the term “Endotoxin” [43]. It is estimated that each bacterial cell contains two-million LPS molecules [44], covering approximately 75 % of the membrane surface [45].
LPS is a complex molecule, comprised of an O-specific chain (O-antigen), core oligosaccharides and a covalently bound Lipid A moiety [46]. LPS is the most studied pathogen associated molecular pattern (PAMP) well known to elicit its actions through Toll-like receptor-4 (TLR4); a type of pattern recognizing receptor (PRR) expressed on the cells of innate immune system [47].
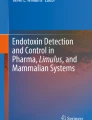
Activation of TLR4 by LPS is not a simple mechanism which involves many crucial molecules that carry LPS to TLR4. An acute phase protein produced in the liver, Lipopolysaccharide binding protein (LBP), mediates the decisive step of LPS recognition by binding to Lipid A moiety and forming a LPS-LBP complex [48]. This complex is then recognized by the Cluster of Differentiation 14 (CD14) receptor, a surface molecule that is also known to form a tertiary complex [49] helping in presenting LPS to TLR4 [50]. Once bound, the TLR4 undergoes dimerization with myeloid differentiation factor 2 (MD2) bringing their intracellular Toll/interleukin-1 receptor (TIR) domains together and allowing the binding of other adaptor proteins [51]. Recruitment and binding of adaptor proteins initiate the TLR4 signaling cascade ending up in the activation and nuclear translocation of NF-κB [51], which further leads to the upregulation of a battery of pro-inflammatory cytokines such as IL-1β, IL-6, IL-8, TNF-α (Fig. 2) along with other molecules such as, COX-2, E-Selectin, MCP-1 and iNOS [52–55].

Schematic representation of Toll-like receptor signaling pathway. TLRs specifically recognize bacteria and/or their products and their activation is mostly dependent on MyD88. Although activation of TLR4 & TLR2 initiates the pathway in a similar manner leading to the activation of NFκB, there are also notable differences in both the pathways and this schematic diagram represents their major differences. Interferon (α/β) genes are predominantly upregulated by the activation of TLR4, while Casapase 8 dependent apoptotic machinery is activated predominantly by the activation of TLR2. Tenascin C, a glycoprotein with a myriad of functions is recently known to be upregulated in response to TLR2 activation in in vitro model [59]. (The pathway was designed using ChemBioDraw Ultra 12.0 software). LBP lipopolysaccharide binding protein, TLR toll-like receptor, MD2 lymphocyte antigen 96, CD-14 cluster of Differentiation 14, TRAM toll-like receptor 4 adaptor protein, TIRAP toll-interleukin 1 receptor (TIR) domain containing adaptor protein, MyD88 myeloid differentiation factor 88, TRIF TIR-domain-containing adapter-inducing interferon-β, TRAF tumor necrosis factor receptor-associated factor, IFN interferon, IRAK interleukin-1 receptor-associated kinase, RIP2 receptor-interacting protein 2, FADD fas-associated death domain protein, PI3K phosphoinositide 3-kinase, NF-κB nuclear factor κB
However, strategies of using monoclonal antibodies and receptor antagonists against LPS and TLR4 to block the deleterious effects initiated by LPS have been in vain, suggesting that LPS is not the only component of bacterial membrane responsible for inducing all the lethal symptoms in patients with severe sepsis and septic shock. This hypothesis is also evident from the study conducted by Freudenberg et al. [56] where the mice strains having mutation in their Tlr4 gene (C3H/HeJ and C57BL/10ScCr) were resistant to LPS action, yet highly susceptible to gram-negative infection, suggesting the involvement of other components of bacterial membrane in eliciting inflammation.
Bacterial lipoproteins and peptides are equipotent as LPS
The probable reason behind the failure of vast number of clinical trials targeting LPS, its receptor TLR4 or downstream signaling molecules can be ascribed to the involvement of other components of bacteria. The lipoproteins and peptides of microbial origin possessing N-terminal lipid modifications are also shown to be potent inducers of inflammation like LPS [57–59]. However, wide use of LPS in sepsis research has made these components unappreciated. Bacterial proteins are known to elicit their inflammatory properties through TLR2 [60], a different but related receptor dedicated to recognizing PAMPs of microbial origin.
Braun lipoprotein (BLP) is the next most abundant component of bacterial membrane after LPS in E. coli. It is a low molecular weight lipoprotein with its N-terminal cysteine residue bearing three palmitoyl residues making the structure a triacylcysteinyl-modified peptide [61]. It is estimated that each bacterial cell is composed of 105 molecules of BLP [62]. Although purified and characterized as a structural component of bacterial membrane over 40 years ago [63], BLP has not gained much attention as an inflammatory component except for few reports describing its potent inflammatory roles in in vitro systems. BLP has been shown to activate macrophages [64], lymphocytes [65] and endothelial cells [57] as efficiently as LPS. The experiments conducted by us clearly indicate the potential pro-inflammatory roles of purified BLP in Swiss albino mice when administered intraperitoneally. The results show endotoxemia-like pathology, along with the upregulation of pro-inflammatory cytokines, while these effects were not observed in BLP-injected TLR2 knockout mice (Lakshmikanth et al., unpublished data). Researchers often use Pam3CSK4, a synthetic structural analogue of BLP while targeting various drugs against TLR2. However, Pam3CSK4 has been shown to be less potent when compared to intact BLP [57] and hence this aspect also needs to be considered while targeting TLR2.
Although activation of TLR4 and TLR2 leads to similar outcomes such as overproduction of pro-inflammatory mediators, there are quite a few differences. This is evident from the study conducted by Neilsen et al. [57] where, IFN-γ-inducible protein-10, a CC-chemokine was specifically upregulated by LPS (Fig. 2), but not by BLP. Similarly, a report by Barrenschee et al., [59] indicates Macrophage-activating lipopeptide-2 (MALP-2), a TLR2 agonist from Mycoplasma fermentas, uniquely upregulated by inflammatory marker, tenascin C but not by LPS (Fig. 2). Hence, despite targeting TLR4, TLR2 pathway should also be considered while attenuating sepsis and related inflammatory disorders.
Early mortality predictors of severe sepsis
Besides traditional inflammatory markers implicated in sepsis and related disorders [52–55], a variety of molecules have been identified as the predictors of early mortality. Macrophage migration inhibitory factor (MIF) released from white blood cells in response to their activation by bacterial components are known to exaggerate the inflammatory mechanisms [66]. An increase in serum levels of MIF is associated with an increased risk towards early mortality during severe sepsis [67]. Similarly, procalcitonin (PCT)—a peptide precursor of calcitonin is produced from the neuroendocrine cells of lungs and intestine in addition to its production from the thyroid gland. PCT levels increase in response to infection and is more specific for bacterial infections when compared with infections by other microbes [68]. The higher level of PCT is often observed in sepsis patients and the level of PCT depicts the severity of the diseased state [69]. Presepsin, a glycoprotein expressed on monocytes and macrophages has been shown to be superior over PCT in terms of specificity and its increased levels correlate with the in-hospital mortality rates of patients with sepsis [70]. Yet another useful component of serum which can be employed as a risk marker to predict mortality is lactate, as its levels are shown to be at the higher end in patients with sepsis and related disorders [71]. Although, serum lactate levels correlate with organ dysfunction [72], a study by Mikkelsen et al. [73] indicates the ability of initial serum lactate levels to predict mortality irrespective of organ dysfunction. Likewise, higher serum levels of soluble urokinase plasminogen activator receptor (suPAR), a marker of immune activation has also been found to be a marker of mortality risk prediction [74].
Strategies that failed in attenuating the severity of sepsis
Despite enormous advancements in understanding the pathophysiology of sepsis, the mortality rate has failed to show any major decrease as evident from the failure of more than 100 clinical trials [20]. The only drug which made an attempt to reach the market after FDA approval was ‘XIGRIS’ (activated Drotrecogin alfa), a recombinant form of activated protein C (rhAPC). Unfortunately, this was also pulled down from the market by Eli Lilly, Indianapolis, USA [75, 76] and that has left the critical care specialists with no choice of a single medication for the treatment of sepsis and related disorders. Out of all the molecules employed in clinical trials with an aim to reduce the severe mortality rates due to sepsis and related disorders, very few of them gained a lot of importance as they were successful in reducing the mortality in homogeneous population. They include corticosteroids [77], antibodies against LPS [78–80], antibodies against key cytokine mediator TNF-α [81–85], receptor antagonists for TLR4 [86, 87], interleukin-1 receptor (IL-1R) [88] and bradykinin receptor [89], blood coagulation pathway inhibitors [90, 91] and the agents that block platelet activating factor (PAF) mediated effects [92, 93]. However, none of them were successful in clearing the phase III clinical trials (Table 2).
Never ending failure of clinical trials made the SSC committee employ early-goal directed therapy (EGDT) to simplify complex processes while treating the patients with severe sepsis [26]. EGDT include bundles of tasks to be employed in the first 6 h of admission of patients at the hospital, some of which include: (1) obtaining blood cultures before treating with antibiotics and administering with broad spectrum antibiotics, (2) imaging studies to confirm the potential source of infection and their control with attention to the balance of risks and benefits, (3) measuring lactate levels as it is known to be increased (>4 mM/L) in severe sepsis cases due to various factors [71], (4) fluid resuscitation by administering crystalloids (30 ml/kg) for patients with hypotension and supplementing albumin to patients who continue to require substantial amounts of crystalloid to maintain adequate mean arterial pressure, and (5) applying vasopressors for persistent hypotension [26]. However, large, multicentre, randomized clinical trials conducted by protocol-based care for early septic shock (ProCESS) group [94], the Australasian Resuscitation in Sepsis Evaluation (ARISE) group [95] and Protocolised Management In Sepsis (ProMISe) group [96] employing EGDT protocols also resulted in no better outcomes. These failures have bound clinician’s hands when treating patients arriving at the emergency departments.
Animal models employed in sepsis research
Animal models play an important role in drug development by creating a replica of the diseased condition, and an ideal animal model should mimic and translate all the relevant information concerned with the progressive pathophysiology associated with the diseased state. Wide varieties of animal models of sepsis have been developed [22] and are categorized as surgical models and non-surgical models [97].
Despite being expensive and involving animal welfare issues, surgical models are the most relevant models of sepsis [97], since a significant amount of sepsis cases are a result of an acquired infection during invasive surgery [98, 99]. Based on the surgical procedure involved, the surgical models of sepsis are of two types [22], one being cecal ligation and puncture (CLP) model of sepsis—which involves ligation below the ileocecal valve followed by puncturing the cecum using a needle so as to leak the fecal matter into the peritoneal cavity [100] and the other being colon ascendens stent peritonitis (CASP) model of sepsis—which involves inserting a stent into the ascending colon so as to leak abdominal content [101]. Although, both CLP and CASP models are efficient in bringing up polymicrobial sepsis conditions mimicking clinical course of intra-abdominal sepsis, there are significant differences in bacterial load, generation of cytokines and the survival time [102]. CLP and CASP models also suffer from inconsistent results as the ligation distance, size of the needle used to puncture the cecum in CLP model and diameter of the stent used in CASP model are the major determining factors of mortality [22, 102, 103].
To overcome the disadvantages of CLP and CASP models of sepsis, a reliable and reproducible rodent model of sepsis—‘polymicrobial peritoneal contamination and infection (PCI) model’ has been developed [104, 105]. PCI involves the administration of human fecal matter into the peritoneal cavity of rodents to develop the classical symptoms of sepsis [104, 105]. In contrast to CLP and CASP models, the major advantage of PCI model is its simplicity in terms of sample preparation, injection and the ease of controlling the severity of infection by manipulating the amount of fecal matter to be injected [105]. With these advantages, PCI is now being employed in sepsis research [104, 106–109].
Yet another surgical model of sepsis is the ‘implantation model’ which involves implanting a fibrin clot impregnated with live bacteria into the peritoneal cavity through a major surgery [110]. Fibrin clots aid in the slow release of bacteria into the bloodstream. This model is an elegant one over others due to slow mortality and choice of organism based on the field of interest [97], thus allowing the researcher to design specific drugs based on the organism being used.
The non-surgical model is the widely used animal model of sepsis for mimicking pathophysiological conditions associated with sepsis syndrome as it is more advantageous in terms of cost and animal welfare issues [97]. It involves the administration of animals with pathogenic organisms either in live or heat-killed form or administration of endotoxins through various routes (i.p/i.v) depending on the experimental needs. Based on the component of injections the non-surgical model of sepsis has been categorized as infection model, which involves injecting live bacterium and intoxication model, which involves injecting non-infectious components such as heat-killed bacteria or bacterial endotoxin LPS [111].
The infection model involving administration of a live pathogenic organism of interest would induce sepsis [112, 113], however, the spreading of infection, the generation of inflammatory cytokines and the mortality rates are all determined by the route of administration [97] and the bacterial strains used in the experiments determine the hemodynamic responses [112].
The intoxication model known also as endotoxemia model of sepsis is the widely used model, since the administration of LPS mimics almost all the pathological consequences that occur during sepsis [114]. However, there are many disadvantages of using endotoxemia model, since the systemic clinical signs are initiated immediately after the administration of LPS. For example, the TNF-α level increases within an hour of LPS administration and the levels decline after 4 h. But, this is more unlikely to occur in human system and the inflammatory cytokine levels may raise based on the severity of infection [114]. The other major disadvantage of using endotoxemia model is that the concentration of LPS required to elicit strong inflammatory response is much higher in mice when compared to humans [115], indicating a variation in the sensitivity to LPS in different animal species [116]. In addition to differences in sensitivity among various animal models of different species, Yang et al. showed variation in sensitivity to LPS in murine models of sepsis. In this, the most widely used strains of mice, C57BL/6J strain, shows less sensitivity to LPS while BALB/c is more sensitive [117].
All animal models, irrespective of whether surgery is involved or not, possess disadvantages in addition to various advantages [118]. So, the researchers should consider all the disadvantages before opting for a particular animal model. Unfortunately, an ideal animal model of sepsis is yet to be developed.
Inclusion of antibiotics along with novel candidate drugs while treating sepsis
Strategies of targeting a single entity in clinical sepsis never lead to fruitful outcomes as evident from the failure of a vast number of clinical trials. Yet another strategy that could be employed while treating patients with severe sepsis is the use of antibiotics in combination with candidate drug molecule. Although very few reports suggests the beneficial effects of inclusion of antibiotics along with various drugs, the results of experiments using animal models of sepsis clearly demonstrate the potentially beneficial roles of combination therapy in reducing the mortality rates. Reports by Bauhofer et al. [104] and Aydin et al. [119] describe the positive effects of combination of antibiotics with Granulocyte colony stimulating factor (G-CSF)—a stimulator of bactericidal activity of granulocytes, in reducing the mortality of animals. Similarly, use of antibiotics in combination with Tumor Necrosis Factor Inhibitor and an endotoxin antagonist, E5531, significantly protected mice from lethality as reported by Fei et al. [120] and Christ et al. [121], respectively. With these beneficial effects, including antibiotics along with various drugs would improve the survival of sepsis patients.
Recent advancements in search of cure for sepsis
Technologies employed in delineating the cause of sepsis
Decades of struggle in sepsis research has lead to the better understanding of disease progression. Researchers are now involved in identifying the exact cause by employing various advanced technologies so as to treat the patients immediately in a more specific way. The particular pathogen behind the microbial infection is being analyzed by Polymerase Chain Reaction (PCR)-based assays, replacing the standard microbial culture methods [122, 123]. The disseminated intravascular coagulation is one of the major problems often observed in patients with severe sepsis and septic shock [124] and this defect can be quantified in vitro by modified thromboelastometry [125], a technique that measures the fibrinolytic activity in whole blood samples. Quantification of metabolic biomarkers is of great importance in diagnosing the worsened diseased state to initiate timely treatment options. For this purpose Garcia-Simon et al., have developed a 1H NMR based analysis protocol to quantify the metabolic markers in urine [126]. However, implementing the use of these techniques in clinical labs is only after their extensive validation and most importantly, depends on their cost effectiveness.
Strategies employed to attenuate cardiac dysfunction
With the failure of more than 100 randomized clinical trials [20], researchers are finding new avenues to block the severity of sepsis and related disorders. Of the organs most affected during severe sepsis and septic shock, heart plays a major role [127], as low cardiac output is often the major problem seen in cases of severe sepsis resulting in hypoperfusion and end-organ damage [72]. To circumvent the problems associated with low cardiac output, the ionotropic drug—Levosimendan, a calcium sensitizer, earlier shown to be effective in animal models [128, 129] and also to be superior over widely employed ionotropic drug Dobutamine [130], is now being employed in clinical trial to test its efficacy in improving the organ dysfunctions in septic shock patients [121]. Resuscitation using selepressin, a selective vasopressin type-1a receptor agonist involved in vasodilation has been shown to be effective in animal models of sepsis and is also shown to be more effective than vasopressin in blocking the vascular leakage [131, 132]. Selepressin is now under phase 2b/3 initiated by Ferring Pharmaceuticals for the treatment of septic shock. Trimetazidine (TMZ), an inhibitor of β-oxidation pathway, has been shown to possess anti-ischemic activities through extensive utilization of myocardial glucose and maintaining proper energy metabolism [133]. TMZ has recently shown to have protective roles by blocking LPS-induced myocardial dysfunction and apoptosis in experimental sepsis model [134, 135]. Hence, TMZ can also be a candidate drug molecule to alleviate the problems associated with heart.
Strategies to circumvent the problems associated with acute kidney injury
Acute kidney injury (AKI) following cardiac dysfunction is the frequent condition often observed in sepsis patients [136]. The severity of kidney dysfunction can be determined by quantifying the serum troponin I level as reported recently by Thiengo Dda et al. [137]. Administering the dephosphorylating enzyme, alkaline phosphatase to sepsis associated AKI patients has shown beneficial effects by reducing the urinary excretion of tubular injury biomarkers and plasma markers of inflammation [138]. Recent prospective, two-center, open-labeled randomized, controlled trials conducted by Abdul-Aziz et al. have shown the beneficial effects of continuous administration of β-lactam antibiotics in patients not undergoing renal replacement therapy [139].
Nuclear proteins as the marker of mortality due to sepsis
Histones, the component of eukaryotic cell nuclei involved in folding the DNA into nucleosomes [140] are now shown to have a role in inflammatory condition, where these nuclear components are released to the exterior by damaged and activated cells. They possess cytotoxic and pro-inflammatory effects which depict the severity of inflammation, thereby joining the list of damage associated molecular patterns (DAMPs) [141]. These released histones act through TLR2 and TLR4 and are responsible for cytokine release, endothelial dysfunction, end-organ damage and mortality in animal models of sepsis [142, 143]. Infusion of histones in mice has been shown to cause pulmonary vascular obstruction, induced right ventricular pressure increase and dilatation leading to cardiac injury [144]. These deleterious effects are shown to be attenuated by the use of heparin [145]. Extracellular histone levels are also shown to predict mortality in sepsis patients [146] and hence, targeting extracellular histones is of great importance so as to come up with an efficient drug to treat sepsis and related disorders.
High-mobility group protein B1 (HMGB1) are the abundant and ubiquitous chromatin-associated nuclear proteins [147, 148] belonging to the superfamily of high-mobility group (HMG) proteins [149]. Its presence is restricted to nucleus in naive cells because of the presence of two lysine-rich nuclear localization sequences [150]. However, it is released to the extracellular milieu by various cell types in response to their activation by various factors [151–157]. The released HMGB1 may act through TLR4 [158, 159] or through the receptor for advanced glycation endproducts (RAGE) [160, 161] leading to the activation of NF-κB resulting in the production of pro-inflammatory cytokines [162]. Recent report by Zheng et al. [163] shows the loss of vascular endothelial monolayer integrity in vitro induced by HMGB1 present in the sera of patients with sepsis. Use of Dabrafenib, a B-Raf inhibitor, ameliorated HMGB1-induced vascular permeability in addition to blocking HMGB1 release as reported by Jung et al. [164]. Anti-HMGB1 antibodies are shown to reduce the LPS-induced lethality in mouse model of endotoxemia [151] and are also shown to be beneficial in protecting the mice against endotoxin-induced acute lung inflammation [165]. Release of HMGB1 (late mediator) and its inflammatory properties might be the reason behind the failure of monoclonal antibody therapies directed against TNF-α or IL-1β (early mediators). Developing an efficient drug targeting HMGB1 and using it in conjugation with other drugs would be a wise idea to bring down the mortality rates associated with sepsis and related disorders.
Combination therapy as a new strategy to treat sepsis
Sepsis-induced organ damage is mediated by the involvement of multiple pathways [166] and hence, designing a single drug to block all the pathways simultaneously is not feasible. In this regard, researchers are now employing the use of a combination of drugs to attenuate the septic challenge in animal models of sepsis. A recent study by Kwon et al. [167] show the beneficial effect of combination of niacin and selenium in attenuating the severity of lung injury and mortality in endotoxemia and CLP models of sepsis. Besides, treating animals either with niacin or selenium individually failed to mount the similar response [167]. In a similar study, Lima et al. [168] have used monoclonal antibodies against the two major receptors TLR2 and TLR4 in combination with antibiotics to circumvent the adverse effects of polymicrobial sepsis. The results have shown a remarkable improvement in survival rate in addition to reduced neutrophil infiltration and cytokine production [168]. Although proven to be beneficial in experimental models of sepsis, the strategies of using combination of drugs have to undergo validation to reach clinical trials.
New cell-based therapies against sepsis
Mesenchymal stem cells (MSCs) are shown to be promising therapeutic options against various tissue injuries and immune disorders [169]. MSCs are shown to be protective in models of acute lung injury [170], cardiac dysfunction [171], renal failure [172] and hepatic injury [173]. Apart from this, MSCs therapeutic roles have been proved even in animal models of endotoxemia [174, 175] and polymicrobial sepsis [176, 177]. With all these beneficial roles, MSCs have not yet reached the phases of clinical trials for the treatment of sepsis [178].
Future perspectives in search of cure for sepsis
Since sepsis is a complex disease involving multimediators, targeting a single entity is unattainable as evident from the failure of clinical trials against LPS which throws light on the involvement of other possible components of bacterial membrane in the pathogenesis of sepsis. As observed by us (Unpublished data) and others [57], purified BLP is as potent as LPS in inducing severe inflammatory response both in vitro and in vivo. Hence, targeting several other components of bacteria like BLP along with LPS would be a good strategy in attenuating the severity of sepsis. In addition, researchers need to focus on blocking the deleterious effects mediated by the released nuclear proteins as they are shown to be the late mediators of sepsis. Another strategy would be to employ combination of drugs as they are proven to be beneficial in regulating the process of initiation and disease progression [168]. Similarly, inclusion of antibiotics in combination with other standard drugs would improve the survival rates of sepsis patients as shown in various animal models of sepsis. However, the strategy of employing a combination of drugs needs to be validated both in animal models of sepsis and clinical trials. Although very few reports suggest the beneficial roles of adjunct therapy using high-dose of IgM, enriched intravenous Ig, (IVIG) [179, 180], considering this option would be a good strategy for the treatment of patients with sepsis. As the use of MSCs have been proven to be beneficial in modulating the immune response and converting the macrophages and neutrophils to anti-inflammatory phenotype in animal models of sepsis [181], clinical trials may be carried out to bring MSCs to market as one of the therapeutic options.
Conclusion
Although, many of the molecular events occurring during sepsis are dissected, an appropriate single molecular entity that needs to be targeted is still a mystery. One can argue that, in a disease involving multimediators it is unlikely to have a single entity that can be targeted. Moreover, more than 100 clinical trials have been undertaken and have failed to identify a critical mediator for sepsis and related disorders [20]. Furthermore, this disease/syndrome also lacks a suitable and appropriate animal model as evident from the disadvantages of each model [118] and this may also be the reason behind the failure of so many clinical trials. Therefore, sepsis is still considered as a disease, in search of a cure. Hopefully, modern biology will come up with a suitable animal model or a molecular target so as to develop a magic bullet to treat this deadly disease soon.
References
Martin GS. Sepsis, severe sepsis and septic shock: changes in incidence, pathogens and outcomes. Expert Rev Anti Infect Ther. 2012;10:701–6.
Ma J, Chen C, Barth AS, Cheadle C, Guan X, Gao L. Lysosome and cytoskeleton pathways are robustly enriched in the blood of septic patients: a meta-analysis of transcriptomic data. Mediators Inflamm. 2015;2015:984825.
Rossaint J, Zarbock A. Pathogenesis of multiple organ failure in sepsis. Crit Rev Immunol. 2015;35:277–91.
Chaudhry N, Duggal AK. Sepsis associated encephalopathy. Adv Med 2014; 2014.
Organization WH. Global surveillance and control of hepatitis C. Report of a WHO Consultation organized in collaboration with the Viral Hepatitis Prevention Board, Antwerp, Belgium. J Viral Hepat. 1999;6:35–47.
Garciarena CD, McHale TM, Watkin RL, Kerrigan SW. Coordinated molecular cross-talk between staphylococcus aureus, endothelial cells and platelets in bloodstream infection. Pathogens. 2015;4:869–82.
Ribet D, Cossart P. How bacterial pathogens colonize their hosts and invade deeper tissues. Microbes Infect. 2015;17:173–83.
Van Kaer L, Parekh VV, Wu L. The response of CD1d-restricted invariant NKT cells to microbial pathogens and their products. Front Immunol. 2015;6:226.
Ramachandran G. Gram-positive and gram-negative bacterial toxins in sepsis: a brief review. Virulence. 2014;5:213–8.
Martin L, van Meegern A, Doemming S, Schuerholz T. Antimicrobial peptides in human sepsis. Front Immunol. 2015;6:404.
Riedemann NC, Guo RF, Ward PA. Novel strategies for the treatment of sepsis. Nat Med. 2003;9:517–24.
Tse MT. Trial watch: sepsis study failure highlights need for trial design rethink. Nat Rev Drug Discov. 2013;12:334.
Bozza FA, Salluh JI, Japiassu AM, Soares M, Assis EF, Gomes RN, et al. Cytokine profiles as markers of disease severity in sepsis: a multiplex analysis. Crit Care. 2007;11:R49.
Malmir J, Bolvardi E, Afzal Aghaee M. Serum lactate is a useful predictor of death in severe sepsis and septic shock. Rev Clin Med. 2014;1:97–104.
Masson S, Caironi P, Fanizza C, Thomae R, Bernasconi R, Noto A, et al. Circulating presepsin (soluble CD14 subtype) as a marker of host response in patients with severe sepsis or septic shock: data from the multicenter, randomized ALBIOS trial. Intensive Care Med. 2015;41:12–20.
Chuang TY, Chang HT, Chung KP, Cheng HS, Liu CY, Liu YC, et al. High levels of serum macrophage migration inhibitory factor and interleukin 10 are associated with a rapidly fatal outcome in patients with severe sepsis. Int J Infect Dis. 2014;20:13–7.
Donadello K, Scolletta S, Covajes C, Vincent JL. suPAR as a prognostic biomarker in sepsis. BMC Med. 2012;10:2.
Sandquist M, Wong HR. Biomarkers of sepsis and their potential value in diagnosis, prognosis and treatment. Expert Rev Clin Immunol. 2014;10:1349–56.
Donadello K, Scolletta S, Taccone FS, Covajes C, Santonocito C, Cortes DO, et al. Soluble urokinase-type plasminogen activator receptor as a prognostic biomarker in critically ill patients. J Crit Care. 2014;29:144–9.
Marshall JC. Why have clinical trials in sepsis failed? Trends Mol Med. 2014;20:195–203.
Marik PE. The demise of early goal-directed therapy for severe sepsis and septic shock. Acta Anaesthesiol Scand. 2015;59:561–7.
Rittirsch D, Hoesel LM, Ward PA. The disconnect between animal models of sepsis and human sepsis. J Leukoc Biol. 2007;81:137–43.
Vincent JL. Definition of sepsis and non-infectious SIRS. Sepsis and non-infectious systemic inflammation: from biology to critical care 2009; pp. 1–12.
Bone RC, Balk RA, Cerra FB, Dellinger RP, Fein AM, Knaus WA, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. The ACCP/SCCM Consensus Conference Committee. American College of Chest Physicians/Society of Critical Care Medicine. Chest. 1992;101:1644–55.
Levy MM, Fink MP, Marshall JC, Abraham E, Angus D, Cook D, et al. 2001 SCCM/ESICM/ACCP/ATS/SIS International Sepsis Definitions Conference. Crit Care Med. 2003;31:1250–6.
Dellinger RP, Levy MM, Rhodes A, Annane D, Gerlach H, Opal SM, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637.
Levy MM, Rhodes A, Phillips GS, Townsend SR, Schorr CA, Beale R, et al. Surviving Sepsis Campaign: association between performance metrics and outcomes in a 7.5-year study. Intensive Care Med. 2014;40:1623–33.
de Pablo R, Monserrat J, Prieto A, Alvarez-Mon M. Role of circulating lymphocytes in patients with sepsis. BioMed Res Int. 2014;2014:671087.
Perman SM, Goyal M, Gaieski DF. Initial emergency department diagnosis and management of adult patients with severe sepsis and septic shock. Scand J Trauma Resusc Emerg Med. 2012;20:41.
Schmidt GA, Mandel J, Parsons PE, Sexton DJ, Hockberger RS, Finlay G. Evaluation and management of severe sepsis and septic shock in adults. Uptodate com 2013.
Torres-Rosas R, Yehia G, Pena G, Mishra P, del Rocio Thompson-Bonilla M, Moreno-Eutimio MA, et al. Dopamine mediates vagal modulation of the immune system by electroacupuncture. Nat Med. 2014;20:291–5.
Todi S, Chatterjee S, Sahu S, Bhattacharyya M. Epidemiology of severe sepsis in India: an update. Crit Care. 2010;14:1.
Van Amersfoort ES, Van Berkel TJ, Kuiper J. Receptors, mediators, and mechanisms involved in bacterial sepsis and septic shock. Clin Microbiol Rev. 2003;16:379–414.
Chang AH, Parsonnet J. Role of bacteria in oncogenesis. Clin Microbiol Rev. 2010;23:837–57.
Widmeier K, Wesley K. Infection detection: identifying and understanding sepsis in the prehospital setting, part 1 of 2. JEMS. 2014;39:34–7.
Merrell RC. The abdomen as source of sepsis in critically ill patients. Crit Care Clin. 1995;11:255–72.
Hugonnet S, Sax H, Eggimann P, Chevrolet JC, Pittet D. Nosocomial bloodstream infection and clinical sepsis. Emerg Infect Dis. 2004;10:76–81.
Bewick T, Simmonds M, Chikhani M, Meyer J, Lim WS. Pneumonia in the context of severe sepsis: a significant diagnostic problem. Eur Respir J. 2008;32:1417–8.
Todar K. Immune defense against bacterial pathogens: innate immunity. Todar’s online textbook of bacteriology 2008.
Willatts SM, Radford S, Leitermann M. Effect of the antiendotoxic agent, taurolidine, in the treatment of sepsis syndrome: a placebo-controlled, double-blind trial. Crit Care Med. 1995;23:1033–9.
Levin M, Quint PA, Goldstein B, Barton P, Bradley JS, Shemie SD, et al. Recombinant bactericidal/permeability-increasing protein (rBPI21) as adjunctive treatment for children with severe meningococcal sepsis: a randomised trial. rBPI21 Meningococcal Sepsis Study Group. Lancet. 2000;356:961–7.
Phua J, Ngerng W, See K, Tay C, Kiong T, Lim H, et al. Characteristics and outcomes of culture-negative versus culture-positive severe sepsis. Crit Care. 2013;17:R202.
Fildes P. Richard Friedrich Johannes Pfeiffer. 1858–1945. Biogr Memoirs Fellows Royal Soc 1956; 2:237–247.
Nair SR, Geetha CS, Mohanan PV. Analysis of IL-1 beta release from cryopreserved pooled lymphocytes in response to lipopolysaccharide and lipoteichoic acid. BioMed Res Int. 2013;2013:689642.
Le Brun AP, Clifton LA, Halbert CE, Lin B, Meron M, Holden PJ, et al. Structural characterization of a model gram-negative bacterial surface using lipopolysaccharides from rough strains of Escherichia coli. Biomacromolecules. 2013;14:2014–22.
Rietschel ET, Kirikae T, Schade FU, Mamat U, Schmidt G, Loppnow H, et al. Bacterial endotoxin: molecular relationships of structure to activity and function. FASEB J Off Publ Feder Am Soc Exp Biol. 1994;8:217–25.
Kawasaki T, Kawai T. Toll-like receptor signaling pathways. Front Immunol. 2014;5:461.
Schumann RR, Leong SR, Flaggs GW, Gray PW, Wright SD, Mathison JC, et al. Structure and function of lipopolysaccharide binding protein. Science. 1990;249:1429–31.
Hailman E, Lichenstein HS, Wurfel MM, Miller DS, Johnson DA, Kelley M, et al. Lipopolysaccharide (LPS)-binding protein accelerates the binding of LPS to CD14. J Exp Med. 1994;179:269–77.
Takeda K, Akira S. Toll-like receptors in innate immunity. Int Immunol. 2005;17:1–14.
Lu YC, Yeh WC, Ohashi PS. LPS/TLR4 signal transduction pathway. Cytokine. 2008;42:145–51.
Geng Y, Zhang B, Lotz M. Protein tyrosine kinase activation is required for lipopolysaccharide induction of cytokines in human blood monocytes. J Immunol. 1993;151:6692–700.
Frost RA, Nystrom GJ, Lang CH. Lipopolysaccharide regulates proinflammatory cytokine expression in mouse myoblasts and skeletal muscle. Am J Physiol Regul Integr Comp Physiol. 2002;283:R698–709.
Nii T, Sonoda Y, Isobe N, Yoshimura Y. Effects of lipopolysaccharide on the expression of proinflammatory cytokines and chemokines and the subsequent recruitment of immunocompetent cells in the oviduct of laying and molting hens. Poult Sci. 2011;90:2332–41.
Birrell MA, McCluskie K, Wong S, Donnelly LE, Barnes PJ, Belvisi MG. Resveratrol, an extract of red wine, inhibits lipopolysaccharide induced airway neutrophilia and inflammatory mediators through an NF-kappaB-independent mechanism. FASEB J Off Publ Feder Am Soc Exp Biol. 2005;19:840–1.
Freudenberg MA, Galanos C. Tumor necrosis factor alpha mediates lethal activity of killed gram-negative and gram-positive bacteria in d-galactosamine-treated mice. Infect Immun. 1991;59:2110–5.
Neilsen PO, Zimmerman GA, McIntyre TM. Escherichia coli Braun lipoprotein induces a lipopolysaccharide-like endotoxic response from primary human endothelial cells. J Immunol. 2001;167:5231–9.
Ma Y, Weis JJ. Borrelia burgdorferi outer surface lipoproteins OspA and OspB possess B-cell mitogenic and cytokine-stimulatory properties. Infect Immun. 1993;61:3843–53.
Barrenschee M, Lex D, Uhlig S. Effects of the TLR2 agonists MALP-2 and Pam3Cys in isolated mouse lungs. PLoS One. 2010;5:e13889.
Mogensen TH. Pathogen recognition and inflammatory signaling in innate immune defenses. Clin Microbiol Rev. 2009;22:240–73 (Table of Contents).
Babu MM, Priya ML, Selvan AT, Madera M, Gough J, Aravind L, et al. A database of bacterial lipoproteins (DOLOP) with functional assignments to predicted lipoproteins. J Bacteriol. 2006;188:2761–73.
Vollmer W, Holtje JV. The architecture of the murein (peptidoglycan) in gram-negative bacteria: vertical scaffold or horizontal layer(s)? J Bacteriol. 2004;186:5978–87.
Braun V, Rehn K. Chemical characterization, spatial distribution and function of a lipoprotein (murein-lipoprotein) of the E. coli cell wall. The specific effect of trypsin on the membrane structure. Eur J Biochem. 1969;10:426–38.
Tamta H, Pugh ND, Balachandran P, Moraes R, Sumiyanto J, Pasco DS. Variability in in vitro macrophage activation by commercially diverse bulk echinacea plant material is predominantly due to bacterial lipoproteins and lipopolysaccharides. J Agric Food Chem. 2008;56:10552–6.
Bastian M, Braun T, Bruns H, Rollinghoff M, Stenger S. Mycobacterial lipopeptides elicit CD4 + CTLs in Mycobacterium tuberculosis-infected humans. J Immunol. 2008;180:3436–46.
Calandra T, Froidevaux C, Martin C, Roger T. Macrophage migration inhibitory factor and host innate immune defenses against bacterial sepsis. J Infect Dis. 2003;187:S385–90.
Chuang CC, Wang ST, Chen WC, Chen CC, Hor LI, Chuang YC. Increases in serum macrophage migration inhibitory factor in patients with severe sepsis predict early mortality. Shock. 2007;27:503–6.
Soni N, Samson D, Galaydick J, Vats V, Pitrak D, Aronson N. Procalcitonin-guided antibiotic therapy. Comparative Effectiveness Review No. 78. Effective Health Care Program AHRQ Publication, p. 13.
Meisner M, Tschaikowsky K, Palmaers T, Schmidt J. Comparison of procalcitonin (PCT) and C-reactive protein (CRP) plasma concentrations at different SOFA scores during the course of sepsis and MODS. Crit Care. 1999;3:45.
Ulla M, Pizzolato E, Lucchiari M, Loiacono M, Soardo F, Forno D, et al. Diagnostic and prognostic value of presepsin in the management of sepsis in the emergency department: a multicenter prospective study. Crit Care. 2013;17:R168.
Blomkalns AL. Lactate-a marker for sepsis and trauma. Emergency Medicine Cardiac Research and Education Group 2006; 2.
Koch T, Geiger S, Ragaller MJ. Monitoring of organ dysfunction in sepsis/systemic inflammatory response syndrome: novel strategies. J Am Soc Nephrol. 2001;12(Suppl 17):S53–9.
Mikkelsen ME, Miltiades AN, Gaieski DF, Goyal M, Fuchs BD, Shah CV, et al. Serum lactate is associated with mortality in severe sepsis independent of organ failure and shock*. Crit Care Med. 2009;37:1670–7.
Gustafsson A, Ljunggren L, Bodelsson M, Berkestedt I. The prognostic value of suPAR compared to other inflammatory markers in patients with severe sepsis. Biomarker Insights. 2012;7:39.
Williams SC. After Xigris, researchers look to new targets to combat sepsis. Nat Med. 2012;18:1001.
Focus on sepsis. Nat Med 2012; 18:997.
Sprung CL, Caralis PV, Marcial EH, Pierce M, Gelbard MA, Long WM, et al. The effects of high-dose corticosteroids in patients with septic shock. A prospective, controlled study. N Engl J Med. 1984;311:1137–43.
Calandra T, Glauser MP, Schellekens J, Verhoef J. Treatment of gram-negative septic shock with human IgG antibody to Escherichia coli J5: a prospective, double-blind, randomized trial. J Infect Dis. 1988;158:312–9.
Ziegler EJ, Fisher CJ Jr, Sprung CL, Straube RC, Sadoff JC, Foulke GE, et al. Treatment of gram-negative bacteremia and septic shock with HA-1A human monoclonal antibody against endotoxin. A randomized, double-blind, placebo-controlled trial. The HA-1A Sepsis Study Group. N Engl J Med. 1991;324:429–36.
Bone RC, Balk RA, Fein AM, Perl TM, Wenzel RP, Reines HD, et al. A second large controlled clinical study of E5, a monoclonal antibody to endotoxin: results of a prospective, multicenter, randomized, controlled trial. The E5 Sepsis Study Group. Crit Care Med. 1995;23:994–1006.
Abraham E, Wunderink R, Silverman H, Perl TM, Nasraway S, Levy H, et al. Efficacy and safety of monoclonal antibody to human tumor necrosis factor alpha in patients with sepsis syndrome. A randomized, controlled, double-blind, multicenter clinical trial. TNF-alpha MAb Sepsis Study Group. JAMA. 1995;273:934–41.
Cohen J, Carlet J. INTERSEPT: an international, multicenter, placebo-controlled trial of monoclonal antibody to human tumor necrosis factor-alpha in patients with sepsis. International Sepsis Trial Study Group. Crit Care Med. 1996;24:1431–40.
Fisher CJ Jr, Agosti JM, Opal SM, Lowry SF, Balk RA, Sadoff JC, et al. Treatment of septic shock with the tumor necrosis factor receptor: Fc fusion protein. The Soluble TNF Receptor Sepsis Study Group. N Engl J Med. 1996;334:1697–702.
Abraham E, Laterre PF, Garbino J, Pingleton S, Butler T, Dugernier T, et al. Lenercept (p55 tumor necrosis factor receptor fusion protein) in severe sepsis and early septic shock: a randomized, double-blind, placebo-controlled, multicenter phase III trial with 1342 patients. Crit Care Med. 2001;29:503–10.
Abraham E, Anzueto A, Gutierrez G, Tessler S, San Pedro G, Wunderink R, et al. Double-blind randomised controlled trial of monoclonal antibody to human tumour necrosis factor in treatment of septic shock. NORASEPT II Study Group. Lancet. 1998;351:929–33.
Opal SM, Laterre PF, Francois B, LaRosa SP, Angus DC, Mira JP, et al. Effect of eritoran, an antagonist of MD2-TLR4, on mortality in patients with severe sepsis: the ACCESS randomized trial. JAMA. 2013;309:1154–62.
Rice TW, Wheeler AP, Bernard GR, Vincent JL, Angus DC, Aikawa N, et al. A randomized, double-blind, placebo-controlled trial of TAK-242 for the treatment of severe sepsis. Crit Care Med. 2010;38:1685–94.
Opal SM, Fisher CJ Jr, Dhainaut JF, Vincent JL, Brase R, Lowry SF, et al. Confirmatory interleukin-1 receptor antagonist trial in severe sepsis: a phase III, randomized, double-blind, placebo-controlled, multicenter trial. The Interleukin-1 Receptor Antagonist Sepsis Investigator Group. Crit Care Med. 1997;25:1115–24.
Fein AM, Bernard GR, Criner GJ, Fletcher EC, Good JT Jr, Knaus WA, et al. Treatment of severe systemic inflammatory response syndrome and sepsis with a novel bradykinin antagonist, deltibant (CP-0127). Results of a randomized, double-blind, placebo-controlled trial. CP-0127 SIRS and Sepsis Study Group. JAMA. 1997;277:482–7.
Abraham E, Reinhart K, Opal S, Demeyer I, Doig C, Rodriguez AL, et al. Efficacy and safety of tifacogin (recombinant tissue factor pathway inhibitor) in severe sepsis: a randomized controlled trial. JAMA. 2003;290:238–47.
Vincent JL, Ramesh MK, Ernest D, LaRosa SP, Pachl J, Aikawa N, et al. A randomized, double-blind, placebo-controlled, Phase 2b study to evaluate the safety and efficacy of recombinant human soluble thrombomodulin, ART-123, in patients with sepsis and suspected disseminated intravascular coagulation. Crit Care Med. 2013;41:2069–79.
Dhainaut JF, Tenaillon A, Hemmer M, Damas P, Le Tulzo Y, Radermacher P, et al. Confirmatory platelet-activating factor receptor antagonist trial in patients with severe gram-negative bacterial sepsis: a phase III, randomized, double-blind, placebo-controlled, multicenter trial. BN 52021 Sepsis Investigator Group. Crit Care Med. 1998;26:1963–71.
Opal S, Laterre PF, Abraham E, Francois B, Wittebole X, Lowry S, et al. Recombinant human platelet-activating factor acetylhydrolase for treatment of severe sepsis: results of a phase III, multicenter, randomized, double-blind, placebo-controlled, clinical trial. Crit Care Med. 2004;32:332–41.
Yealy DM, Kellum JA, Huang DT, Barnato AE, Weissfeld LA, Pike F, et al. A randomized trial of protocol-based care for early septic shock. N Engl J Med. 2014;370:1683–93.
Peake SL, Delaney A, Bailey M, Bellomo R, Cameron PA, Cooper DJ, et al. Goal-directed resuscitation for patients with early septic shock. N Engl J Med. 2014;371:1496–506.
Mouncey PR, Osborn TM, Power GS, Harrison DA, Sadique MZ, Grieve RD, et al. Trial of early, goal-directed resuscitation for septic shock. N Engl J Med. 2015;372:1301–11.
Nemzek JA, Hugunin KM, Opp MR. Modeling sepsis in the laboratory: merging sound science with animal well-being. Comp Med. 2008;58:120–8.
deSa LA, Sathe MJ, Bapat RD. Factors influencing wound infection (a prospective study of 280 cases). J Postgrad Med. 1984;30:232–6.
Du Pont-Thibodeau G, Joyal JS, Lacroix J. Management of neonatal sepsis in term newborns. F1000prime reports 2014; 6:67.
Toscano MG, Ganea D, Gamero AM. Cecal ligation puncture procedure. J Vis Exp 2011.
Traeger T, Koerner P, Kessler W, Cziupka K, Diedrich S, Busemann A, et al. Colon ascendens stent peritonitis (CASP)–a standardized model for polymicrobial abdominal sepsis. J Vis Exp 2010.
Maier S, Traeger T, Entleutner M, Westerholt A, Kleist B, Huser N, et al. Cecal ligation and puncture versus colon ascendens stent peritonitis: two distinct animal models for polymicrobial sepsis. Shock. 2004;21:505–11.
Singleton KD, Wischmeyer PE. Distance of cecum ligated influences mortality, tumor necrosis factor-alpha and interleukin-6 expression following cecal ligation and puncture in the rat. Eur Surg Res. 2003;35:486–91.
Bauhofer A, Torossian A, Lorenz W, Middeke M, Plaul U, Schutz P, et al. Dependence of positive effects of granulocyte colony-stimulating factor on the antibiotic regimen: evaluation in rats with polymicrobial peritonitis. World J Surg. 2004;28:834–44.
Gonnert FA, Recknagel P, Seidel M, Jbeily N, Dahlke K, Bockmeyer CL, et al. Characteristics of clinical sepsis reflected in a reliable and reproducible rodent sepsis model. J Surg Res. 2011;170:e123–34.
Otto GP, Grunwald B, Geis C, Kothe S, Hurtado-Oliveros J, Chung HY, et al. Impact of antibiotic treatment intensity on long-term sepsis-associated kidney injury in a polymicrobial peritoneal contamination and infection model. Nephron. 2015;129:137–42.
Recknagel P, Gonnert FA, Halilbasic E, Gajda M, Jbeily N, Lupp A, et al. Mechanisms and functional consequences of liver failure substantially differ between endotoxaemia and faecal peritonitis in rats. Liver Int. 2013;33:283–93.
Randerath E, Randerath K, Reddy R, Lucier GW. Sexual dimorphism of the chromatographic profiles of I-compounds (endogenous deoxyribonucleic acid modifications) in rat liver. Endocrinology. 1991;129:3093–100.
Seidel M, Winning J, Claus RA, Bauer M, Losche W. Beneficial effect of clopidogrel in a mouse model of polymicrobial sepsis. J Thromb Haemost. 2009;7:1030–2.
Toky V, Sharma S, Arora BB, Chhibber S. Establishment of a sepsis model following implantation of Klebsiella pneumoniae-infected fibrin clot into the peritoneal cavity of mice. Folia Microbiol (Praha). 2003;48:665–9.
Warren HS. Editorial: mouse models to study sepsis syndrome in humans. J Leukoc Biol. 2009;86:199–201.
Dehring DJ, Crocker SH, Wismar BL, Steinberg SM, Lowery BD, Cloutier CT. Comparison of live bacteria infusions in a porcine model of acute respiratory failure. J Surg Res. 1983;34:151–8.
Xiang Y, Wang X, Yan C, Gao Q, Li SA, Liu J, et al. Adenosine-5’-triphosphate (ATP) protects mice against bacterial infection by activation of the NLRP3 inflammasome. PLoS One. 2013;8:e63759.
Remick DG, Newcomb DE, Bolgos GL, Call DR. Comparison of the mortality and inflammatory response of two models of sepsis: lipopolysaccharide vs. cecal ligation and puncture. Shock. 2000;13:110–6.
Copeland S, Warren HS, Lowry SF, Calvano SE, Remick D. Acute inflammatory response to endotoxin in mice and humans. Clin Diagn Lab Immunol. 2005;12:60–7.
Garrido AG, Figueiredo LFPd. Experimental models of sepsis and septic shock: an overview. Acta Cirurgica Brasileira. 2004;19:82–8.
Yang IV, Alper S, Lackford B, Rutledge H, Warg LA, Burch LH, et al. Novel regulators of the systemic response to lipopolysaccharide. Am J Respir Cell Mol Biol. 2011;45:393–402.
Doi K, Leelahavanichkul A, Yuen PS, Star RA. Animal models of sepsis and sepsis-induced kidney injury. J Clin Investig. 2009;119:2868–78.
Aydin S, Caylan R, Aydin K, Yulug E, Yenilmez E, Koksal I. The influence of G-CSF addition to antibiotic treatment of experimental sepsis on pulmonary tissue. J Natl Med Assoc. 2005;97:1489–95.
Fei Y, Wang W, Kwiecinski J, Josefsson E, Pullerits R, Jonsson IM, et al. The combination of a tumor necrosis factor inhibitor and antibiotic alleviates staphylococcal arthritis and sepsis in mice. J Infect Dis. 2011;204:348–57.
Christ WJ, Asano O, Robidoux AL, Perez M, Wang Y, Dubuc GR, et al. E5531, a pure endotoxin antagonist of high potency. Science. 1995;268:80–3.
Suberviola B, Marquez-Lopez A, Castellanos-Ortega A, Fernandez-Mazarrasa C, Santibanez M, Martinez LM. Microbiological diagnosis of sepsis: polymerase chain reaction system versus blood cultures. Am J Crit Care. 2016;25:68–75.
Plettig R, Nowak A, Balau V, Hahnenkamp K, Usichenko T. Prospective comparison of a PCR assay and a microbiological culture technique for identification of pathogens from blood and non-blood samples in septic patients. J Intensive Care. 2015;3:51.
Semeraro N, Ammollo CT, Semeraro F, Colucci M. Sepsis-associated disseminated intravascular coagulation and thromboembolic disease. Mediterr J Hematol Infect Dis. 2010;2:e2010024.
Kuiper GJ, Kleinegris MC, van Oerle R, Spronk HM, Lance MD, Ten Cate H, et al. Validation of a modified thromboelastometry approach to detect changes in fibrinolytic activity. Thromb J. 2016;14:1.
Garcia-Simon M, Morales JM, Modesto-Alapont V, Gonzalez-Marrachelli V, Vento-Rehues R, Jorda-Minana A, et al. Prognosis biomarkers of severe sepsis and septic shock by 1H NMR urine metabolomics in the intensive care unit. PLoS One. 2015;10:e0140993.
Merx MW, Weber C. Sepsis and the heart. Circulation. 2007;116:793–802.
Fries M, Ince C, Rossaint R, Bleilevens C, Bickenbach J, Rex S, et al. Levosimendan but not norepinephrine improves microvascular oxygenation during experimental septic shock. Crit Care Med. 2008;36:1886–91.
Garcia-Septien J, Lorente JA, Delgado MA, de Paula M, Nin N, Moscoso A, et al. Levosimendan increases portal blood flow and attenuates intestinal intramucosal acidosis in experimental septic shock. Shock. 2010;34:275–80.
Morelli A, Donati A, Ertmer C, Rehberg S, Lange M, Orecchioni A, et al. Levosimendan for resuscitating the microcirculation in patients with septic shock: a randomized controlled study. Crit Care. 2010;14:R232.
Maybauer MO, Maybauer DM, Enkhbaatar P, Laporte R, Wisniewska H, Traber LD, et al. The selective vasopressin type 1a receptor agonist selepressin (FE 202158) blocks vascular leak in ovine severe sepsis*. Crit Care Med. 2014;42:e525–33.
Boucheix OB, Milano SP, Henriksson M, Reinheimer TM. Selepressin, a new V1A receptor agonist: hemodynamic comparison to vasopressin in dogs. Shock. 2013;39:533–8.
Stanley WC, Marzilli M. Metabolic therapy in the treatment of ischaemic heart disease: the pharmacology of trimetazidine. Fundam Clin Pharmacol. 2003;17:133–45.
Tanoglu A, Yamanel L, Inal V, Ocal R, Comert B, Bilgi C. Appreciation of trimetazidine treatment in experimental sepsis rat model. Bratisl Lek Listy. 2015;116:124–7.
Chen J, Lai J, Yang L, Ruan G, Chaugai S, Ning Q, et al. Trimetazidine prevents macrophage mediated septic myocardial dysfunction via Sirt1. Br J Pharmacol 2015.
Peters E, Heemskerk S, Masereeuw R, Pickkers P. Alkaline phosphatase: a possible treatment for sepsis-associated acute kidney injury in critically ill patients. Am J Kidney Dis. 2014;63:1038–48.
Thiengo Dda A, Lugon JR, Graciano ML. Troponin I serum levels predict the need of dialysis in incident sepsis patients with acute kidney injury in the intensive care unit. J Bras Nefrol. 2015;37:433–8.
Pickkers P, Heemskerk S, Schouten J, Laterre P-F, Vincent J-L, Beishuizen A, et al. Alkaline phosphatase for treatment of sepsis-induced acute kidney injury: a prospective randomized double-blind placebo-controlled trial. Crit Care. 2012;16:R14.
Abdul-Aziz MH, Sulaiman H, Mat-Nor MB, Rai V, Wong KK, Hasan MS, et al. Beta-Lactam Infusion in Severe Sepsis (BLISS): a prospective, two-centre, open-labelled randomised controlled trial of continuous versus intermittent beta-lactam infusion in critically ill patients with severe sepsis. Intensive Care Med 2016.
Marino-Ramirez L, Kann MG, Shoemaker BA, Landsman D. Histone structure and nucleosome stability. Expert Rev Proteomics. 2005;2:719–29.
Chen R, Kang R, Fan XG, Tang D. Release and activity of histone in diseases. Cell Death Dis. 2014;5:e1370.
Xu J, Zhang X, Pelayo R, Monestier M, Ammollo CT, Semeraro F, et al. Extracellular histones are major mediators of death in sepsis. Nat Med. 2009;15:1318–21.
Xu J, Zhang X, Monestier M, Esmon NL, Esmon CT. Extracellular histones are mediators of death through TLR2 and TLR4 in mouse fatal liver injury. J Immunol. 2011;187:2626–31.
Alhamdi Y, Zi M, Abrams ST, Liu T, Su D, Welters I, et al. Circulating histone concentrations differentially affect the predominance of left or right ventricular dysfunction in critical illness. Crit Care Med 2015.
Iba T, Hashiguchi N, Nagaoka I, Tabe Y, Kadota K, Sato K. Heparins attenuated histone-mediated cytotoxicity in vitro and improved the survival in a rat model of histone-induced organ dysfunction. Intensive Care Med Exp. 2015;3:36.
Wildhagen KC, Wiewel MA, Schultz MJ, Horn J, Schrijver R, Reutelingsperger CP, et al. Extracellular histone H3 levels are inversely correlated with antithrombin levels and platelet counts and are associated with mortality in sepsis patients. Thromb Res. 2015;136:542–7.
Bustin M, Reeves R. High-mobility-group chromosomal proteins: architectural components that facilitate chromatin function. Prog Nucleic Acid Res Mol Biol. 1996;54:35–100.
Bianchi ME, Agresti A. HMG proteins: dynamic players in gene regulation and differentiation. Curr Opin Genet Dev. 2005;15:496–506.
Hock R, Furusawa T, Ueda T, Bustin M. HMG chromosomal proteins in development and disease. Trends Cell Biol. 2007;17:72–9.
Huang W, Tang Y, Li L. HMGB1, a potent proinflammatory cytokine in sepsis. Cytokine. 2010;51:119–26.
Wang H, Bloom O, Zhang M, Vishnubhakat JM, Ombrellino M, Che J, et al. HMG-1 as a late mediator of endotoxin lethality in mice. Science. 1999;285:248–51.
Gardella S, Andrei C, Ferrera D, Lotti LV, Torrisi MR, Bianchi ME, et al. The nuclear protein HMGB1 is secreted by monocytes via a non-classical, vesicle-mediated secretory pathway. EMBO Rep. 2002;3:995–1001.
Schierbeck H, Wahamaa H, Andersson U, Harris HE. Immunomodulatory drugs regulate HMGB1 release from activated human monocytes. Mol Med. 2010;16:343–51.
Tang D, Shi Y, Kang R, Li T, Xiao W, Wang H, et al. Hydrogen peroxide stimulates macrophages and monocytes to actively release HMGB1. J Leukoc Biol. 2007;81:741–7.
Pisetsky DS, Jiang W. Role of Toll-like receptors in HMGB1 release from macrophages. Ann N Y Acad Sci. 2007;1109:58–65.
Chen G, Li J, Ochani M, Rendon-Mitchell B, Qiang X, Susarla S, et al. Bacterial endotoxin stimulates macrophages to release HMGB1 partly through CD14- and TNF-dependent mechanisms. J Leukoc Biol. 2004;76:994–1001.
Dumitriu IE, Baruah P, Valentinis B, Voll RE, Herrmann M, Nawroth PP, et al. Release of high mobility group box 1 by dendritic cells controls T cell activation via the receptor for advanced glycation end products. J Immunol. 2005;174:7506–15.
Li M, Song L, Gao X, Chang W, Qin X. Toll-like receptor 4 on islet beta cells senses expression changes in high-mobility group box 1 and contributes to the initiation of type 1 diabetes. Exp Mol Med. 2012;44:260–7.
Zong M, Bruton JD, Grundtman C, Yang H, Li JH, Alexanderson H, et al. TLR4 as receptor for HMGB1 induced muscle dysfunction in myositis. Ann Rheum Dis. 2013;72:1390–9.
Qin YH, Dai SM, Tang GS, Zhang J, Ren D, Wang ZW, et al. HMGB1 enhances the proinflammatory activity of lipopolysaccharide by promoting the phosphorylation of MAPK p38 through receptor for advanced glycation end products. J Immunol. 2009;183:6244–50.
He ZW, Qin YH, Wang ZW, Chen Y, Shen Q, Dai SM. HMGB1 acts in synergy with lipopolysaccharide in activating rheumatoid synovial fibroblasts via p38 MAPK and NF-kappaB signaling pathways. Mediators Inflamm. 2013;2013:596716.
Schiraldi M, Raucci A, Munoz LM, Livoti E, Celona B, Venereau E, et al. HMGB1 promotes recruitment of inflammatory cells to damaged tissues by forming a complex with CXCL12 and signaling via CXCR4. J Exp Med. 2012;209:551–63.
Zheng YJ, Xu WP, Ding G, Gao YH, Wang HR, Pan SM. Expression of HMGB1 in septic serum induces vascular endothelial hyperpermeability. Mol Med Rep. 2016;13:513–21.
Jung B, Kang H, Lee W, Noh HJ, Kim YS, Han MS, et al. Anti-septic effects of dabrafenib on HMGB1-mediated inflammatory responses. BMB Rep 2015.
Abraham E, Arcaroli J, Carmody A, Wang H, Tracey KJ. HMG-1 as a mediator of acute lung inflammation. J Immunol. 2000;165:2950–4.
Dear JW, Yasuda H, Hu X, Hieny S, Yuen PS, Hewitt SM, et al. Sepsis-induced organ failure is mediated by different pathways in the kidney and liver: acute renal failure is dependent on MyD88 but not renal cell apoptosis. Kidney Int. 2006;69:832–6.
Kwon WY, Suh GJ, Kim KS, Jung YS, Kim SH, Kim JS, et al. Niacin and Selenium Attenuate Sepsis-Induced Lung Injury by Up-Regulating Nuclear Factor Erythroid 2-Related Factor 2 Signaling. Crit Care Med 2015.
Lima CX, Souza DG, Amaral FA, Fagundes CT, Rodrigues IP, Alves-Filho JC, et al. Therapeutic effects of treatment with anti-TLR2 and anti-TLR4 monoclonal antibodies in polymicrobial sepsis. PLoS One. 2015;10:e0132336.
Wei X, Yang X, Han ZP, Qu FF, Shao L, Shi YF. Mesenchymal stem cells: a new trend for cell therapy. Acta Pharmacol Sin. 2013;34:747–54.
Gupta N, Su X, Popov B, Lee JW, Serikov V, Matthay MA. Intrapulmonary delivery of bone marrow-derived mesenchymal stem cells improves survival and attenuates endotoxin-induced acute lung injury in mice. J Immunol. 2007;179:1855–63.
Lee C, Mitsialis SA, Aslam M, Vitali SH, Vergadi E, Konstantinou G, et al. Exosomes mediate the cytoprotective action of mesenchymal stromal cells on hypoxia-induced pulmonary hypertension. Circulation. 2012;126:2601–11.
Morigi M, Imberti B, Zoja C, Corna D, Tomasoni S, Abbate M, et al. Mesenchymal stem cells are renotropic, helping to repair the kidney and improve function in acute renal failure. J Am Soc Nephrol. 2004;15:1794–804.
Berardis S, Dwisthi Sattwika P, Najimi M, Sokal EM. Use of mesenchymal stem cells to treat liver fibrosis: current situation and future prospects. World J Gastroenterol. 2015;21:742–58.
Zhao Y, Yang C, Wang H, Li H, Du J, Gu W, et al. Therapeutic effects of bone marrow-derived mesenchymal stem cells on pulmonary impact injury complicated with endotoxemia in rats. Int Immunopharmacol. 2013;15:246–53.
Weil BR, Herrmann JL, Abarbanell AM, Manukyan MC, Poynter JA, Meldrum DR. Intravenous infusion of mesenchymal stem cells is associated with improved myocardial function during endotoxemia. Shock. 2011;36:235–41.
Nemeth K, Leelahavanichkul A, Yuen PS, Mayer B, Parmelee A, Doix K, et al. Bone marrow stromal cells attenuate sepsis via prostaglandin E(2)-dependent reprogramming of host macrophages to increase their interleukin-10 production. Nat Med. 2009;15:42–9.
Mei SH, Haitsma JJ, Dos Santos CC, Deng Y, Lai PF, Slutsky AS, et al. Mesenchymal stem cells reduce inflammation while enhancing bacterial clearance and improving survival in sepsis. Am J Respir Crit Care Med. 2010;182:1047–57.
Monsel A, Zhu YG, Gennai S, Hao Q, Liu J, Lee JW. Cell-based therapy for acute organ injury: preclinical evidence and ongoing clinical trials using mesenchymal stem cells. Anesthesiology. 2014;121:1099–121.
Rodriguez A, Rello J, Neira J, Maskin B, Ceraso D, Vasta L, et al. Effects of high-dose of intravenous immunoglobulin and antibiotics on survival for severe sepsis undergoing surgery. Shock. 2005;23:298–304.
Hamano N, Nishi K, Onose A, Okamoto A, Umegaki T, Yamazaki E, et al. Efficacy of single-dose intravenous immunoglobulin administration for severe sepsis and septic shock. J Intensive Care. 2013;1:4.
Lombardo E, van der Poll T, DelaRosa O, Dalemans W. Mesenchymal stem cells as a therapeutic tool to treat sepsis. World J Stem Cells. 2015;7:368–79.
Bone RC, Fisher CJ Jr, Clemmer TP, Slotman GJ, Metz CA, Balk RA. A controlled clinical trial of high-dose methylprednisolone in the treatment of severe sepsis and septic shock. N Engl J Med. 1987;317:653–8.
Bone RC, Fisher CJ Jr, Clemmer TP, Slotman GJ, Metz CA. Early methylprednisolone treatment for septic syndrome and the adult respiratory distress syndrome. Chest. 1987;92:1032–6.
Bone RC, Fisher CJ Jr, Clemmer TP, Slotman GJ, Metz CA, Balk RA. Sepsis syndrome: a valid clinical entity. Methylprednisolone Severe Sepsis Study Group. Crit Care Med. 1989;17:389–93.
McCloskey RV, Straube RC, Sanders C, Smith SM, Smith CR. Treatment of septic shock with human monoclonal antibody HA-1A. A randomized, double-blind, placebo-controlled trial. CHESS Trial Study Group. Ann Intern Med. 1994;121:1–5.
The French National Registry of HA-1A (Centoxin) in septic shock. A cohort study of 600 patients. The National Committee for the Evaluation of Centoxin. Arch Intern Med. 1994;154:2484–91.
Dhainaut JF, Tenaillon A, Le Tulzo Y, Schlemmer B, Solet JP, Wolff M, et al. Platelet-activating factor receptor antagonist BN 52021 in the treatment of severe sepsis: a randomized, double-blind, placebo-controlled, multicenter clinical trial. BN 52021 Sepsis Study Group. Crit Care Med. 1994;22:1720–8.
Panacek EA, MacArthur RD, Johnson SB, Albertson TE, Maki D, Tobias J, et al. Results of a phase III clinical trial of the human monoclonal antibody mab-t88 versus placebo in gram negative sepsis. Crit Care Med. 1995;23:A170.
Abraham E, Glauser MP, Butler T, Garbino J, Gelmont D, Laterre PF, et al. p55 Tumor necrosis factor receptor fusion protein in the treatment of patients with severe sepsis and septic shock. A randomized controlled multicenter trial. Ro 45-2081 Study Group. Jama. 1997;277:1531–8.
Christopher TA, Ma XL, Gauthier TW, Lefer AM. Beneficial actions of CP-0127, a novel bradykinin receptor antagonist, in murine traumatic shock. Am J Physiol. 1994;266:H867–73.
Bernard GR, Wheeler AP, Russell JA, Schein R, Summer WR, Steinberg KP, et al. The effects of ibuprofen on the physiology and survival of patients with sepsis. The Ibuprofen in Sepsis Study Group. N Engl J Med. 1997;336:912–8.
Angus DC, Birmingham MC, Balk RA, Scannon PJ, Collins D, Kruse JA, et al. E5 murine monoclonal antiendotoxin antibody in gram-negative sepsis: a randomized controlled trial. E5 Study Investigators. Jama. 2000;283:1723–30.
Suputtamongkol Y, Intaranongpai S, Smith MD, Angus B, Chaowagul W, Permpikul C, et al. A double-blind placebo-controlled study of an infusion of lexipafant (Platelet-activating factor receptor antagonist) in patients with severe sepsis. Antimicrob Agents Chemother. 2000;44:693–6.
Vincent JL, Spapen H, Bakker J, Webster NR, Curtis L. Phase II multicenter clinical study of the platelet-activating factor receptor antagonist BB-882 in the treatment of sepsis. Crit Care Med. 2000;28:638–42.
Abraham E, Naum C, Bandi V, Gervich D, Lowry SF, Wunderink R, et al. Efficacy and safety of LY315920Na/S-5920, a selective inhibitor of 14-kDa group IIA secretory phospholipase A2, in patients with suspected sepsis and organ failure. Crit Care Med. 2003;31:718–28.
Abraham E, Reinhart K, Opal S, Demeyer I, Doig C, Rodriguez AL, et al. Efficacy and safety of tifacogin (recombinant tissue factor pathway inhibitor) in severe sepsis: a randomized controlled trial. Jama. 2003;290:238–47.
Watson D, Grover R, Anzueto A, Lorente J, Smithies M, Bellomo R, et al. Cardiovascular effects of the nitric oxide synthase inhibitor NG-methyl-L-arginine hydrochloride (546C88) in patients with septic shock: results of a randomized, double-blind, placebo-controlled multicenter study (study no. 144-002). Crit Care Med. 2004;32:13–20.
Abraham E, Laterre P, Garg R, Levy H, Talwar D, Trzaskoma B, et al. Administration of Drotrecogin Alfa (Activated) in Early Stage Severe Sepsis (ADDRESS) Study Group Drotrecogin alfa (activated) for adults with severe sepsis and a low risk of death. N Engl J Med. 2005;353:1332–41.
Zeiher BG, Steingrub J, Laterre PF, Dmitrienko A, Fukiishi Y, Abraham E. LY315920NA/S-5920, a selective inhibitor of group IIA secretory phospholipase A2, fails to improve clinical outcome for patients with severe sepsis. Crit Care Med. 2005;33:1741–8.
Annane D, Sebille V, Bellissant E. Effect of low doses of corticosteroids in septic shock patients with or without early acute respiratory distress syndrome. Crit Care Med. 2006;34:22–30.
Nadel S, Goldstein B, Williams M, Dalton H, Peters M, Macias W, et al. REsearching severe Sepsis and Organ dysfunction in children: a gLobal perspective (RESOLVE) study group: Drotrecogin alfa (activated) in children with severe sepsis: A multicentre phase III randomised controlled trial. Lancet. 2007;369:836–43.
Sprung CL, Annane D, Keh D, Moreno R, Singer M, Freivogel K, et al. Hydrocortisone therapy for patients with septic shock. N Engl J Med. 2008;358:111–24.
Dellinger RP, Tomayko JF, Angus DC, Opal S, Cupo MA, McDermott S, et al. Efficacy and safety of a phospholipid emulsion (GR270773) in Gram-negative severe sepsis: results of a phase II multicenter, randomized, placebo-controlled, dose-finding clinical trial. Crit Care Med. 2009;37:2929–38.
Tidswell M, Tillis W, Larosa SP, Lynn M, Wittek AE, Kao R, et al. Phase 2 trial of eritoran tetrasodium (E5564), a toll-like receptor 4 antagonist, in patients with severe sepsis. Crit Care Med. 2010;38:72–83.
Ranieri VM, Thompson BT, Barie PS, Dhainaut JF, Douglas IS, Finfer S, et al. Drotrecogin alfa (activated) in adults with septic shock. N Engl J Med. 2012;366:2055–64.
Vincent JL, Privalle CT, Singer M, Lorente JA, Boehm E, Meier-Hellmann A, et al. Multicenter, randomized, placebo-controlled phase III study of pyridoxalated hemoglobin polyoxyethylene in distributive shock (PHOENIX)*. Crit Care Med. 2015;43:57–64.
Acknowledgements
The authors acknowledge University Grants Commission for financial support. University Grants Commission Basic Science Research fellowship [F.7-366/2012]—to LCL; University Grants Commission Non-NET Fellowship [F. 87-1-2012(SU-1)2]—to SPJ; UGC-Major Research Project [F. No: 41-128/2012-13 (SR)]—to GMK, Vision Group of Science and Technology (VGST) [VGST/K-FIST (2010-11)/GRD-36/2013-14], Government of Karnataka and UGC-Special Assistance Program (UGC-SAP) [F3-14/2012 (SAP II)].
Author information
Authors and Affiliations
Corresponding author
Additional information
Responsible Editor: Artur Bauhofer.
Rights and permissions
About this article

Cite this article
Lakshmikanth, C.L., Jacob, S.P., Chaithra, V.H. et al. Sepsis: in search of cure. Inflamm. Res. 65, 587–602 (2016). https://doi.org/10.1007/s00011-016-0937-y
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00011-016-0937-y