
Abstract
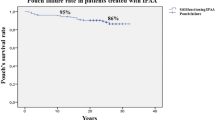
INTRODUCTION: The aim of this study is to report ten-year results of ileal pouch-anal anastomosis in selected patients with colorectal Crohn's disease for whom coloproctectomy and definitive end ileostomy was the only alternative. METHODS: 41 patients (22 females/19 males) with a mean age of 36 ± 13 (range, 16–72) years underwent ileal pouch-anal anastomosis for colorectal Crohn's disease between 1985 to 1998. None had past or present history of anal manifestations or evidence of small-bowel involvement. Diagnosis of Crohn's disease was established preoperatively in 26 patients, on the resected specimen after ileal pouch-anal anastomosis, or after occurrence of Crohn's disease-related complication in 15 patients. RESULTS: Follow-up was 113 ± 37 months, (18–174) 20 patients having been followed for more than 10 years. There was no postoperative death. Eleven (27 percent) patients experienced Crohn's disease-related complications, 47 ± 34 months (8–101) after ileal pouch-anal anastomosis: 2 had persistent anal ulcerations with pouchitis and granulomas on pouch biopsy and were treated medically; 2 experienced extrasphincteric abscesses and 7 presented pouch-perineal fistulas which were treated surgically. Among them, 3 patients with persistent perineal fistula despite surgery required definitive end-ileostomy. Of the 20 patients followed for more than 10 years, 7 (35 percent) experienced Crohn's disease-related complications which required pouch excision in 2 (10 percent). CONCLUSIONS: Ten years after ileal pouch-anal anastomosis for colorectal Crohn's disease, rates of Crohn's disease-related complications and pouch excision were 35 and 10 percent, respectively. These good long-term results justify for us to propose ileal pouch-anal anastomosis in selected patients with colorectal Crohn's disease (i.e., no past or present history of anal manifestations and no evidence of small-bowel involvement) for whom the only alternative is definitive end ileostomy.
Similar content being viewed by others


References
Deutsch AA, McLeod RS, Cullen J, Cohen Z. Results of the pelvic-pouch procedure in patients with Crohn's disease. Dis Colon Rectum 1991;34:475–7.
Scammell BE, Andrews H, Allan RN, Alexander-Williams J, Keighley MR. Results of proctocolectomy for Crohn's disease. Br J Surg 1987;74:671–4.
Grobler SP, Hosie KB, Affie E, Thompson H, Keighley MR. Outcome of restorative proctocolectomy when the diagnosis is suggestive of Crohn's disease. Gut 1993;34:1384–8.
Hyman NH, Fazio VW, Tukson WB, Lavery IC. Consequences of ileal pouch-anal anastomosis for Crohn's colitis. Dis Colon Rectum 1991;34:653–7.
Koltun WA, Schoetz DJ Jr, Roberts PL, Murray JJ, Coller JA, Veidenheimer MC. Indeterminate colitis predisposes to perineal complications after ileal pouch-anal anastomosis. Dis Colon Rectum 1991;34:857–60.
Pezim ME, Pemberton JH, Beart RW,et al. Outcome of “indeterminant” colitis following ileal pouch-anal anastomosis. Dis Colon Rectum 1989;32:653–8.
Panis Y, Poupard B, Nemeth J, Lavergne A, Hautefeuille P, Valleur P. Ileal pouch-anal anastomosis for Crohn's disease. Lancet 1996;347:854–7.
Lennard-Jones J. Classification of inflammatory bowel disease. Scand J Gastroenterol 1989;170:2–6.
Bernell O, Lapidus A, Hellers G. Risk factors for surgery and postoperative recurrence in Crohn's disease. Ann Surg 2000;231:38–45.
Panis Y, Bonhomme N, Hautefeuille P, Valleur P. Ileal pouch-anal anastomosis with mesorectal excision for rectal cancer complicating familial adenomatous polyposis. Eur J Surg 1996;162:817–21.
Berrebi W, Chaussade S, Bruhl AL,et al. Treatment of Crohn's disease recurrence after ileoanal anastomosis by azathioprine. Dig Dis Sci 1993;38:1558–60.
Benoist S, Panis Y, Berdah S, Hautefeuille P, Valleur P. New treatment for ileal pouch-anal or coloanal anastomotic stenosis. Dis Colon Rectum 1998;41:935–7.
Fazio VW, Ziv Y, Church JM,et al. Ileal pouch-anal anastomoses complications and function in 1005 patients. Ann Surg 1995;222:120–7.
Sagar PM, Dozois RR, Wolff BG. Long-term results of ileal pouch-anal anastomosis in patients with Crohn's disease. Dis Colon Rectum 1996;39:893–8.
Gorenstein L, Boyd JB, Ross TM. Gracilis muscle repair of rectovaginal fistula after restorative proctocolectomy: report of two cases. Dis Colon Rectum 1988;31:730–4.
Fazio VW, Tjandra JJ. Pouch advancement and neoileoanal anastomosis for anastomotic stricture and anovaginal fistula complicating restorative proctocolectomy. Br J Surg 1992;79:694–6.
Ozuner G, Hull T, Lee P, Fazio VW. What happens to a pelvic pouch when fistula develops? Dis Colon Rectum 1997;40:543–7.
Ricart E, Panaccione R, Loftus EV, Tremaine WJ, Sandborn WJ. Successful management of Crohn's disease of the ileoanal pouch with infliximab. Gastroenterology 1999;117:429–32.
Phillips RS. Ileal pouch-anal anastomosis for Crohn's disease. Gut 1998;43:303–4.
Author information
Authors and Affiliations
About this article
Cite this article
Regimbeau, J.M., Panis, Y., Pocard, M. et al. Long-term results of ileal pouch-anal anastomosis for colorectal Crohn's disease. Dis Colon Rectum 44, 769–776 (2001). https://doi.org/10.1007/BF02234693
Issue Date:
DOI: https://doi.org/10.1007/BF02234693