
Abstract
Aspergillus species are ubiquitous fungal saprophytes found in diverse ecological niches worldwide. Among them, Aspergillus fumigatus is the most prevalent and is largely responsible for the increased incidence of invasive aspergillosis with high mortality rates in some immunocompromised hosts. Azoles are the first-line drugs in treating diseases caused by Aspergillus spp. However, increasing reports in A. fumigatus azole resistance, both in the clinical setting and in the environment, are threatening the effectiveness of clinical and agricultural azole drugs. The azole target is the 14-α sterol demethylase encoded by cyp51A gene and the main mechanisms of resistance involve the integration of tandem repeats in its promoter and/or single point mutations in this gene. In A. fumigatus, azole resistance can emerge in two different scenarios: a medical route in which azole resistance is generated during long periods of azole treatment in the clinical setting and a route of resistance derived from environmental origin due to extended use of demethylation inhibitors in agriculture. The understanding of A. fumigatus azole resistance development and its evolution is needed in order to prevent or minimize its impact. In this article, we review the current situation of azole resistance epidemiology and the predominant molecular mechanisms described based on the resistance acquisition routes. In addition, the clinical implications of A. fumigatus azole resistance and future research are discussed.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
1 Introduction
The incidence of fatal fungal diseases is escalating due to an increased population at risk in developed countries: patients who suffer from immuno-deficiencies or predisposing factors, such as hematological malignancies, solid organ transplant recipients, and those suffering from chronic obstructive pulmonary disease and receiving high-dose and continued corticosteroid therapy [1–5]. Patients in intensive care units and those infected with HIV are also sometimes classified as high risk [6, 7].
The genus Aspergillus is relatively unique among fungi in that they cause a wide range of infections such as chronic pulmonary and allergic pulmonary aspergillosis, saprophytic colonization, asthma with fungal sensitization and most severely invasive aspergillosis (IA) [3, 8–10]. Affected individuals will develop a specific form of aspergillosis depending on numerous host factors, but mainly based on underlying immune status [11]. In immunocompromised hosts, A. fumigatus represents a major cause of morbidity and mortality, in part because of the difficulty in diagnosis and late initiation of antifungal therapy.
Treatment options are limited to three antifungal drug classes: polyenes (amphotericin B), azole drugs and echinocandins. Among them, only three specific triazole agents (itraconazole, voriconazole and posaconazole) are recommended for the treatment and prophylaxis of aspergillosis [12, 13]. The antifungal action of azole drugs was first reported in 1944. Since then many azole compounds have been introduced including imidazoles, followed by triazoles [14]. Within the triazoles, fluconazole and itraconazole were introduced for clinical use during 1990s, followed by a second generation, including voriconazole (2002) and posaconazole (2006) [15]. More recently, isavuconazole has been described as a new extended-spectrum triazole, and its activity against Aspergillus has been proven [16]. At present, voriconazole remains the primary treatment for IA and liposomal amphotericin B (L-AMB) is recommended as an alternative therapy [12, 13, 17]. Azoles are the only class of mold-active agents that can be administrated orally and intravenously so that they can be given in outpatient settings and they are used for both the evidence-based treatment and prevention of Aspergillus spp. infections [12, 13, 17]. However, azoles are generally fungistatic in vitro against yeast-like fungi and show species and strain-dependent fungicidal activity against Aspergillus species [18, 19].
Emerging resistance to existing antifungals is a current problem and a poor response to them has been described in infections caused by azole-resistant A. fumigatus [18, 20, 21]. Drug selection pressure due to the use of antifungal drugs, in medical centers and as pesticides in agriculture, is an important factor for resistance emergence and spread. Currently, the link between extensive use of azoles in the environment and the emergence of azole resistance among human fungal pathogens is subject of intensive research [22, 23]. Understanding the origin and development of A. fumigatus azole resistance is needed to minimize its global spread and to prolong the effectiveness of currently available antifungals [22].
2 Evolving Epidemiology
The incidence and prevalence of azole-resistant strains isolated from blood cultures, respiratory and deep tissue samples have been reviewed by several authors [20, 24–31]. Although the prevalence of mold isolation is low, the most frequently isolated genus is Aspergillus spp., ranging between 51–86% of the total number of isolates [25, 28, 30]. Among them, A. fumigatus is the most frequently isolated species, accounting for more than half of the total isolates in most of the studies [24, 26, 28, 30, 32]. Other species, in order of frequency, are A. flavus or A. terreus, A. niger and A. tubingensis [21, 24, 28, 30]. The cryptic Aspergillus species are probably underestimated, as their identification is more difficult; some studies have shown prevalence of up to 12% [28, 33]. This is an important issue as antifungal resistance among Aspergillus cryptic species can reach up to 40% of the isolates [28, 34–36].
Along with the expanding use of antifungal drugs globally, an increase in the number of Aspergillus triazole-resistant isolates has been reported. In the case of A. fumigatus, the prevalence of azole resistance is quite high within Europe with variable percentages observed in the rest of the world (Table 1). The prevalence of azole-resistant A. fumigatus infections also appears to vary between individual hospitals [37, 38]. Although surveillance of unselected clinical cultures provides resistance rates at a national level and offers information about the epidemiology of resistance mechanisms, recent studies show the need to determine the frequency of azole resistance at the hospital level and within different patient groups or departments [37, 38]. The high prevalence of resistance (20–30%) in clinical isolates of high-risk patients recently reported in the Netherlands and Germany highlights the need for rapid detection of azole resistance to initiate the appropriate therapy earlier [31, 39].
3 Azole Drugs Resistance Mechanisms
Triazole drugs inhibit the 14-α sterol demethylase (Cyp51) that catalyzes a key step in the ergosterol biosynthesis. This is a cytochrome P-450 enzyme containing a heme moiety in its active site and catalyzes the oxidative removal of the 14α-methyl group from cyclized sterol precursors (eburicol or lanosterol) by a three-step reaction [40]. Azole drugs act as competitive Cyp51 inhibitors through the interaction of the N-3 (imidazoles) or N-4 (triazoles) position of the aromatic ring with the iron atom of the heme moiety, which prevents oxygen activation, necessary for lanosterol/eburicol demethylation [41]. The basic heterocyclic nitrogen coordinates to the P450 heme iron, sharing its lone pair of electrons and blocking binding of molecular oxygen, whereas the non-ligated portion of the inhibitor molecule forms multiple contacts with the protein moiety, shaping the protein-ligand surface interface that largely defines the strength of the inhibition [41]. This interaction leads to the accumulation of various 14-α methyl sterols and ergosterol depletion that alters the fungal membrane and affects the cell wall integrity with consequent fungal growth impairment [42]. Specificity of azole compounds depends on the interaction between side groups of the azole compound and the Cyp51 protein [43, 44].
Aspergillus fumigatus has two Cyp51 isoenzymes, Cyp51A and Cyp51B [45], and both can fulfill the role of 14-α sterol demethylase in vitro with no significant differences [46, 47]. Growth is suppressed in the absence of both isoenzymes, but not in the absence of only one of them [46, 47]. Some research has indicated that A. fumigatus Cyp51A confers intrinsic fluconazole resistance [46]. Also, most studies conclude that mutations in cyp51A gene (promoter, coding region or both) are responsible for the great majority of the described azole resistance mechanisms [48]. In contrast, the role of Cyp51B in the susceptibility to azoles is still unclear [49].
Aspergillus fumigatus has different azole resistance mechanisms that can be classified in different categories; the most commonly described are (1) target (cyp51A) modifications, although recently (2) cyp51A-independent mechanisms have been described.
3.1 Aspergillus fumigatus Azole Target (cyp51) Modifications
Azole-resistant A. fumigatus isolates of clinical origin exhibit different mutations that are responsible for the increase in minimum inhibitory concentrations (MIC) to one, or more triazoles [48]. The main mechanisms accounting for triazole resistance in A. fumigatus are point mutations in the cyp51A gene. About 30 different mutations have been described in cyp51A gene, although not all mutations are responsible for an azole-resistant phenotype [5, 44, 50]. Based on cyp51A modifications, azole resistance mechanisms can be classified.
3.1.1 Hot-Spot Single Point Mutations
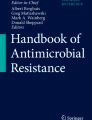
The three most commonly described single-point mutations that appear in A. fumigatus are Cyp51A amino acid substitutions at G54, M220 and G448, and all are thought to have arisen in the clinical setting where azoles are used as therapy (Fig. 1).

Azole target (cyp51A) modifications and susceptibility profiles. Cyp51A hot spot single point mutations (a–c) and Cyp51A multiple point mutations (d). MICs minimum inhibitory concentrations, ITC itraconazole, POS posaconazole, VCZ voriconazole
One mutation is located at position glycine 54, including amino acid changes G54E, G54V, G54R, and G54W. Clinical strains with these mutations show resistance to itraconazole (ITC) and yield high posaconazole (POS) MICs but not voriconazole (VCZ) MICs [51, 52]. The second important single-point mutation is at methionine 220, including amino acid changes M220V, M220K, M220T and M220I [53, 54], which yield resistance to ITC and reduced susceptibility to POS and VCZ [53]. A third resistant mechanism is G448S with resistance to VCZ and reduced susceptibility to ITC and POS [55, 56]. This mutation has also been correlated with in vivo azole resistance [57].
Other less common mutations have also been described. The G138R substitution was described in an azole-resistant mutant generated in the laboratory [58] and afterwards, a multi-azole-resistant strain with a G138C substitution was reported from a patient under azole treatment showing high MICs to all azoles [59]. However, the mechanism involved in this multi-azole resistance phenotype remains to be fully clarified [60].
Protein structure modeling is an important tool in the study of drug action and resistance and has been used to create 3D homology models derived from Cyp51A protein sequences of azole-resistant A. fumigatus isolates. These models have been built to assess direct or indirect mutation effects on azole access or binding to the protein and conclude that M220 and G54 mutations have clear potential to block access to the azole entry channel, while G448S, located on the opposite side of the protein and near the heme group, is thought to disrupt its position within the protein [61]. This mutation reduces the ability of the azole to bind to the heme effectively and allows replacement by the substrate [61, 62].
In some cases, other single-point mutations (N22D, F165L, P216L, F219C, F219I, D262Y, A284T, Y431C, G432S and G434C, T440A, N479D, Y491H) have occasionally been described as related to azole resistance or associated with a reduced azole susceptibility profile, but further research needs to be done in order to confirm, or to exclude, their role in azole drug resistance [20, 25, 50, 60, 63–67].
3.1.2 Cyp51A Multiple Point Mutations
A combination of Cyp51A amino acid substitutions is frequently described among clinical strains isolated from patients who have been undergoing azole treatment. Basically, there are two combinations of amino acid substitutions: (1) a group of three (F46Y, M172V, and D255E) (2) or of five that included the three former ones (F46Y, M172V, N248T, D255E and E427K) (Fig. 1d). Both groups have been described with different profiles of azole susceptibility as azole susceptible or resistant, but in all cases, they have remarkably higher azole MICs than A. fumigatus wild-type strains [20, 21, 50, 65, 68–74]. Some authors described these substitutions as playing no role in azole resistance [65, 75]. However, a cyp51A deletion mutant showed an azole hyper-susceptible profile, suggesting that some of these changes could be responsible for the increased azole MICs of these strains [76], although their role in azole susceptibility in vivo remains to be clarified.
Finally, some substitutions have been described together because they are usually detected along other point mutations, such as H147Y with G448S [20], P394L with G54R [63], S393S with G54R [63], and S297T with F495I [22].
3.1.3 Multiple cyp51A Modifications Involving cyp51A Overexpression
Triazole resistance in Aspergillus spp. can evolve during therapy, but resistant isolates are also being detected in azole-naive patients, with evidence to suggest acquisition of resistant isolates from the environment. These isolates are characterized by having a particular genetic alteration consisting of a 34 bp tandem repeat (TR34) in the promoter, together with a point mutation L98H in the cyp51A target gene conferring multi-azole resistance [77] (Fig. 2a). First reported in Europe, this mechanism is now being described across the world (Table 1). This issue is further complicated by the emergence of a new resistance mechanism, TR46/Y121F/T289A in the cyp51A gene, responsible for VCZ resistance (Fig. 2b). First detected in 2009 in a Dutch patient [78] it has recently been reported in clinical and environmental isolates from Belgium, France, Denmark, Germany, Spain, China, India, Japan, USA, Colombia, Tanzania and Thailand [67, 79–89]. Interestingly, an environmental A. fumigatus strain harboring only the Y121F substitution has been reported recently. However, this mutation is responsible for high VCZ MICs and does not confer resistance to all azoles [90]. Another less common duplication in the cyp51A promoter (TR53) without other substitutions in the cyp51A gene has also been described [86, 91] (Fig. 2c).

Multiple cyp51A modifications involving cyp51A overexpression. Tandem repeats: 34 bp (a); 46 bp (b); 53 bp (c), and associated point mutations
3.2 Aspergillus fumigatus Azole Resistance Mechanisms cyp51A-Independent
Other cyp51A-independent mechanisms have been reported as contributing to azole resistance. One important resistance mechanism is the reduction of the intracellular concentration of azole by active efflux systems, such as ATP-binding cassette (ABC) transporters and transporters of the major facilitator superfamily (MFS) [92]. The association between azole resistance and transporter upregulation is less clear in A. fumigatus than in yeast, such as Candida albicans [93, 94], C. krusei [95], and C. glabrata [96]. In A. fumigatus, there are 45 ABC proteins and 275 MFS proteins (http://www.membranetransport.org). Some studies have demonstrated correlation between ABC transporter expression and azole resistance [54, 97, 98]. However, a functional connection between a specific ABC transporter, RNA level and the development of azole resistance is still elusive. For example, the upregulation of the ABC transporter atrF has been described in a clinical strain of azole-resistant A. fumigatus after ITC treatment but its implication in the ITC resistance has not been confirmed [97]. The same applies to AfuMDR4, which was strongly upregulated in several ITC-resistant laboratory derived mutants, but further experiments need to be done to confirm its participation in azole resistance [54]. Also, transcriptome analysis of A. fumigatus exposed to VCZ revealed a number of transporter genes that were induced: five ABC transporter genes (abcA-E) and three MFS (mfsA-C) were upregulated [98]. Among these genes, only abcB, renamed cdr1B, has been demonstrated to have a direct role in A. fumigatus resistance [99].
In addition, some transcription factors such as SrbA are known to play a role in A. fumigatus azole resistance. SrbA is a transcriptional regulator belonging to the sterol regulatory element binding protein (SREBP) family and is important in A. fumigatus azole resistance. Disruption of srbA produces increased susceptibility to fluconazole, possibly due to the decreased expression of cyp51A [100]. The possibility that SrbA mutants are able to increase their activity and might elevate azole MICs has not been described at present [101]. Also, a P88L substitution in another transcription factor, HapE, leads to an increased azole resistance phenotype due to the induction of cyp51A expression in the mutant strains [102]. Just recently, the link between SrbA and HapE has been demonstrated. Gsaller et al. [103] have shown that the azole resistance exhibited by isolates with the HapEP88L modification is linked to an inability of the modified CCAAT binding complex to bind effectively to its recognition site in the cyp51A promoter, leading to increased expression. Interestingly, the growth phenotype exhibited by a strain with the HapEP88L mutation is less severe than that of the HapE null, suggesting only a partial loss of function, all together will strongly suggest that targeting SrbA would provide an effective avenue for therapeutic intervention for resistant strains.
Recently, a probable role of mitochondrial complex I in fungal drug resistance via alteration in membrane dynamics or composition has been suggested. A mutation leading to an E180D amino acid change in the 29.9 KD subunit has been strongly associated with clinical A. fumigatus azole-resistant isolates [104]. Finally, the modification of AfYap1 (homolog of Saccharomyces cerevisiae Yap1), a basic region-leucine zipper transcription factor with nuclear location and regulated by oxidative stress [105], has been shown to increase resistance to VCZ but not to ITC [106].
3.3 Azole Resistance in Other Aspergillus Species
Although the main etiologic agent of invasive aspergillosis is A. fumigatus, there are increasing reports of fungal infections caused by other species of this genus [107].
Aspergillus section Fumigati has been studied using phylogenetic analysis of different targets (mainly β-tubulin gene) and is found to be composed of 63 species [108, 109]. Some of these species, usually called sibling or cryptic, have been reported to have higher MICs to a range of antifungal agents compared to A. fumigatus [28, 110–113]. Among them, A. lentulus shows high VCZ and ITC MICs, compared to those of POS [110, 112], and good response to isavuconazole [114]; these higher azole MICs have been linked to the amino acid sequence of the Cyp51A target [115, 116]. Other species within the section, such as A. fumigatiaffinis and Neosartorya pseudofischeri, have high triazoles MICs while N. udagawae exhibit higher VCZ MICs than ITC or POS [35, 110, 112, 117]. However, isavuconazole displays good activity against some of these species [114]. Aspergillus viridinutans has high VCZ and ITC MICs but lower POS MICs [35, 113] whereas, A. hiratsukae and A. fumisynnematus are susceptible to all drugs tested [110].
In Aspergillus section Nigri, A. niger and A. tubingensis are the most frequent species found in clinical settings, and have a variable susceptibility profiles depending on the isolate [112]. Within Aspergillus section Flavi, A. flavus and A. alliaceus, are the most remarkable species with variable azole susceptibility profiles [112]. In Aspergillus section Terrei, A. terreus has reduced susceptibility to azoles while A. citrinoterreus is more susceptible to them [118]. Finally, within Aspergillus section Usti, A. ustus and A. calidoustus are known for their high MICs for all antifungals and are considered multi-resistant species [119, 120].
4 Development of Azole Resistance
Azoles are the only class of compounds that are used both in agriculture and in clinical medicine [121].
Generally, two different routes of azole resistance development in A. fumigatus have been described: (1) a medical route in which azole resistance is generated during long periods of azole treatment in clinical settings and (2) another route of resistance derived from environmental origin due to extended use of demethylation inhibitors (DMIs) in agriculture (http://www.frac.info/publications; FRAC Code List 2016) (Fig. 3). Although azole resistance is acquired by selective pressure in both cases, the result of this selection generates different resistance mechanisms and different azole susceptibility patterns.

Routes of Aspergillus fumigatus azole resistance acquisition. a Patient route: the patient is infected by A. fumigatus azole susceptible and after azole treatment there is a selection of A. fumigatus strains with point mutations at Cyp51A. b Environmental route: patients are infected by A. fumigatus azole resistant previously to treatment, and these strains have combined azole resistance mechanisms. DMI demethylation inhibitors
-
1.
In the first case, acquired azole resistance may develop in patients who have been treated long-term with prolonged azole exposure due to a chronic form of aspergillosis, for example patients with aspergilloma, cystic fibrosis or allergic bronchopulmonary aspergillosis. In these patients, isolation of resistant strains is almost always linked to previous azole exposure and the responsible mechanism can change over the course of infection [122]. Despite the fact that patient-to-patient transmission of resistant Aspergillus is uncommon, it would mean an important risk at patient level [32, 123]. These patients are initially infected by a susceptible A. fumigatus strain that evolves to a resistant phenotype under azole treatment pressure. Genotypic analysis of serial A. fumigatus isolates from patients with aspergillosis has revealed that the initial susceptible isolates and the later resistant ones had the same genotype [25, 124–126]. The underlying resistance mechanism normally involves single-point mutations in the cyp51A gene (G54, M220 and G448), which implies that the fungus is capable of rapidly adapting to azole drugs in patients exposed to long-term azole therapy [127].
-
2.
In the agricultural setting, azoles are the most important group of fungicides due to their great efficiency in the field and the remarkable resistance of fungi to other classes of compounds [128]. Agricultural fungicides are used variably throughout the year, depending on the location, crop type and the risk of fungal infestation [128]. They are classified according to their biochemical mode of action as sterol biosynthesis inhibitors (SBIs) of class I, particularly DMIs. Some azoles used in crop protection (imidazoles and triazoles) have a similar molecule structure to medical triazoles and induction of cross-resistance between them has been demonstrated [129].
The resistance mechanisms associated with this route consist of tandem repeat integrations of different size in the cyp51A promoter followed by point mutations in the coding gene (TR34/L98H and TR46/Y121F/T289A). In plant-pathogenic molds treated with DMIs both mechanisms have been found but independently, either as integrations of different sequences in the cyp51A promoter and related to increased expression of the azole target or as point mutations in cyp51 and therefore related to a lack of appropriate competitive inhibition (Table 2). An example of the former is Penicillium digitatum with a 126 bp sequence tandemly repeated in the cyp51 promoter that has been directly related to a pattern of resistance to different DMIs [130, 131]. Similarly, cyp51 promoter insertions of different sizes have been described in other species, such as Venturia inaequalis, Blumeriella japii and Monilinia fructicola [132–134]. In other plant pathogens, many cyp51 single-point mutations have been implicated in DMI resistance (Table 2) [135–142]. However, the combination of both mechanisms has only recently been reported in the plant pathogen Pyrenopeziza brassicae in relation to resistance to DMIs used in crop protection [143].
Fungicides are applied recurrently over a long period of time and could thereby generate a persistent pressure of azole drugs on saprophytic fungi [144]. The existence of an environmental source of resistant A. fumigatus would be supported by the finding of primary IA caused by azole-resistant A. fumigatus in azole-naive patients [145]. These two resistance mechanisms (TR34/L98H and TR46/Y121F/T289A) have been reported in environmental isolates and also in azole-naive patients from the five continents [22, 72, 73, 78, 80, 82, 84–89, 146–150], strongly suggesting a primary acquisition of resistant isolates from the environment. Furthermore, genetic typing of the clinical A. fumigatus isolates revealed shorter genetic distances between TR34/L98H azole-resistant isolates compared to wild-type isolates, suggesting a common source of resistance and a subsequent spreading phenomenon [22, 129, 146].
It seems quite clear that the extended use of azoles as fungicides is selecting resistant mutants in the environment, but it is unknown whether a specific type of DMI used for crop protection is responsible for the type of resistant mechanism selected. Alternatively, each pathogen, with their specific target-drug interaction, could select one specific type of mechanism; promoter insertions (TR), target point mutations, or a combination of both, as has been described with A. fumigatus and P. brassicae. In fact, each Cyp51A modification is responsible for a different pattern of triazole resistance, as described before.
5 Implications for Treatment and Treatment Options
The occurrence of azole-resistant A. fumigatus, in both patients and the environment, is a matter of global concern as azole resistance can seriously compromise treatment in patients with IA. Mortality rates in patients infected with azole-resistant strains are higher than those afflicted by azole susceptible microorganisms (88 vs. 30–50%) [21].
Reference antifungal susceptibility testing methods (Clinical and Laboratory Standards Institute and The European Committee on Antimicrobial Susceptibility Testing) together with molecular characterization of antifungal resistance mechanisms can provide useful information to optimize antifungal therapy and to detect emerging resistance [48]. However, the high mortality rates observed in patients with IA caused by azole-resistant A. fumigatus isolates poses a serious challenge with respect to timely resistance identification and appropriate therapeutic interventions [151].
The emergence of azole resistance raises concerns about first-line VCZ treatment in high-risk patients with suspected IA [152, 153]. Determination of azole resistance percentages at the hospital level, and within different patient groups or departments, will enable clinicians to decide whether reassessment of azole monotherapy as a primary treatment option is necessary [37, 38]. Recently, an international expert panel recommended that VCZ should be used as a first-line drug as long as the local resistance rate does not exceed 10% and a combination of VCZ with an echinocandin or L-AMB would be the therapeutic alternatives if the resistance rate is superior [17].
In the setting of azole resistance, alternative therapeutic options are limited: L-AMB is an important therapeutic option as no cross-resistance is described. Also, the combination of VCZ or POS with an echinocandin has been suggested as an alternative, although it is assumed that azoles will play a limited role in the treatment of azole-resistant invasive Aspergillus infections [154]. Anidulafungin is currently not approved for the treatment of IA, although combination therapy with VCZ is being explored as an alternative when drug resistance is suspected [155, 156].
6 Future Research Areas
The existence of several azole resistance mechanisms in A. fumigatus and the increasing number of affected patients emphasize the need for surveillance studies to determine each country’s epidemiology, to discover the emergence of new mechanisms of azole resistance, and to assess the risk associated with treatment failure.
The need for systematic antifungal susceptibility testing, particularly in high-risk populations cannot be overstated, for assisting clinicians in selecting appropriate antifungal therapy as early as possible [157]. Additionally, techniques to identify resistance directly in clinical samples have the potential to overcome culture-based diagnostic limitations and should be further investigated [158, 159]. Meanwhile, investment in development of new (or repurposed) antifungal drug classes given the risk of losing azoles as first-line treatment is mandatory [160]. Future research should focus on evaluating the effectiveness of newer pharmaceutical agents that can be used as monotherapy or combinational treatments in order to avoid azole resistance. In addition, optimization of current drugs for the purpose of maximizing therapeutic effect while minimizing toxicities would be another important approach [161].
In agriculture, fungicides are applied recurrently over long periods of time and could thereby generate a persistent pressure of azole drugs on saprophytic fungi [144]. Environmental surveys are warranted to determine the prevalence of these resistance mechanisms in saprophytic fungi and to identify areas with a high burden of resistant A. fumigatus [162]. However, an indiscriminate reduction of fungicides used in agriculture would have a detrimental effect on food production and the economy [163]. Therefore, efforts should focus on unraveling the origin and spread of azole resistance in order to better inform guidelines and policy on the use of clinical and agricultural antifungals [164].
Next-generation sequencing (NGS) studies of Aspergillus-resistant strains would give insight into the dynamics of resistance. Moreover, with greater access to NGS technology, studying isolates without a known resistance mechanism would expand our knowledge of A. fumigatus azole resistance. In this respect, there are already some studies applying NGS to clinical A. fumigatus isolates that have reported both accumulation of mutations and genomic deletions that appeared to have occurred randomly in isolates recovered from aspergilloma [165]. This approach has already been used (including a genome and RNA-seq sequencing) in Erysiphe necator, finding a strong association between cyp51 gene copy number variation, Y136F mutation and fungicide treatment. This work suggests that the development of DMI resistance may be happening in two steps: the first, selection of isolates carrying the Y136F mutation and the second, structural rearrangements that increase the number of cyp51 copies carrying the Y136F [166].
In summary, conclusive evidence linking the use of DMIs to the emergence of A. fumigatus azole resistance is still lacking. A multidisciplinary approach to integrate epidemiological studies in the environment and among clinical isolates is required to track the development and spread of resistance mechanisms in A. fumigatus in order to prevent or minimize its impact [152, 153].
References
Rüping MJ, Vehreschild JJ, Cornely OA. Patients at high risk of invasive fungal infections: when and how to treat. Drugs. 2008;68(14):1941–62.
Guinea J, Torres-Narbona M, Gijón P, Muñoz P, Pozo F, Peláez T, et al. Pulmonary aspergillosis in patients with chronic obstructive pulmonary disease: incidence, risk factors, and outcome. Clin Microbiol Infect. 2010;16(7):870–7.
Sugui JA, Kwon-Chung KJ, Juvvadi PR, Latgé JP, Steinbach WJ. Aspergillus fumigatus and related species. Cold Spring Harb Perspect Med. 2014;5(2):a019786.
Warris A. Azole-resistant aspergillosis. J Infect. 2015;71(1):121–5.
Gonçalves SS, Souza AC, Chowdhary A, Meis JF, Colombo AL. Epidemiology and molecular mechanisms of antifungal resistance in Candida and Aspergillus. Mycoses. 2016;59(4):198–219.
Almyroudis NG, Holland SM, Segal BH. Invasive aspergillosis in primary immunodeficiencies. Med Mycol. 2005;43(1):247–59.
Dimopoulos G, Frantzeskaki F, Poulakou G, Armaganidis A. Invasive aspergillosis in the intensive care unit. Ann NY Acad Sci. 2012;1272:31–9.
Kontoyiannis DP, Marr KA, Park BJ, Alexander BD, Anaissie EJ, Walsh TJ, et al. Prospective surveillance for invasive fungal infections in hematopoietic stem cell transplant recipients, 2001–2006: overview of the Transplant-Associated Infection Surveillance Network (TRANSNET) Database. Clin Infect Dis. 2010;50(8):1091–100.
Pappas PG, Alexander BD, Andes DR, Hadley S, Kauffman CA, Freifeld A, et al. Invasive fungal infections among organ transplant recipients: results of the Transplant-Associated Infection Surveillance Network (TRANSNET). Clin Infect Dis. 2010;50(8):1101–11.
Brown GD, Denning DW, Gow NA, Levitz SM, Netea MG, White TC. Hidden killers: human fungal infections. Sci Transl Med. 2012;4(165):165rv13.
Segal BH. Aspergillosis. N Engl J Med. 2009;360(18):1870–84.
Walsh TJ, Anaissie EJ, Denning DW, Herbrecht R, Kontoyiannis DP, Marr KA, et al. Treatment of aspergillosis: clinical practice guidelines of the infectious diseases society of America. Clin Infect Dis. 2008;46:327–60.
Patterson TF, Thompson GR, Denning DW, Fishman JA, Hadley S, Herbrecht R, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63:e1–60.
Fromtling RA. Overview of medically important antifungal azole derivatives. Clin Microbiol Rev. 1988;1(2):187–217.
Maertens JA. History of the development of azole derivatives. Clin Microbiol Infect. 2004;10(1):1–10.
Miceli MH, Kauffman CA. Isavuconazole: a new broad-spectrum triazole antifungal agent. Clin Infect Dis. 2015;61:1558–65.
Verweij PE, Ananda-Rajah M, Andes D, Arendrup MC, Bruggemann RJ, Chowdhary A, et al. International expert opinion on the management of infection caused by azole-resistant Aspergillus fumigatus. Drug Resist Updat. 2015;21–22:30–40.
Johnson EM, Szekely A, Warnock DW. In vitro activity of voriconazole, itraconazole and amphotericin B against filamentous fungi. J Antimicrob Chemother. 1998;42:741–5.
Manavathu EK, Cutright JL, Chandrasekar PH. Organism-dependent fungicidal activities of azoles. Antimicrob Agents Chemother. 1998;42:3018–21.
Howard SJ, Cerar D, Anderson MJ, Albarrag A, Fisher MC, Pasqualotto AC, et al. Frequency and evolution of azole resistance in Aspergillus fumigatus associated with treatment failure. Emerg Infect Dis. 2009;15(7):1068–76.
van der Linden JW, Snelders E, Kampinga GA, Rijnders BJ, Mattsson E, Debets-Ossenkopp YJ, et al. Clinical implications of azole resistance in Aspergillus fumigatus, The Netherlands, 2007–2009. Emerg Infect Dis. 2011;17:1846–54.
Snelders E, van der Lee HA, Kuijpers J, Rijs AJ, Varga J, Samson RA, et al. Emergence of azole resistance in Aspergillus fumigatus and spread of a single resistance mechanism. PLoS Med. 2008.11;5(11):e219.
Camps SM, Rijs AJ, Klaassen CH, Meis JF, O’Gorman CM, Dyer PS, et al. Molecular epidemiology of Aspergillus fumigatus isolates harboring the TR34/L98H azole resistance mechanism. J Clin Microbiol. 2012;50(8):2674–80.
Baddley JW, Marr KA, Andes DR, Walsh TJ, Kauffman CA, Kontoyiannis DP, et al. Patterns of susceptibility of Aspergillus isolates recovered from patients enrolled in the transplant-associated infection surveillance network. J Clin Microbiol. 2009;47:3271–5.
Mortensen KL, Jensen RH, Johansen HK, Skov M, Pressler T, Howard SJ, et al. Aspergillus species and other molds in respiratory samples from patients with cystic fibrosis: a laboratory-based study with focus on Aspergillus fumigatus azole resistance. J Clin Microbiol. 2011;49:2243–51.
Burgel PR, Baixench MT, Amsellem M, Audureau E, Chapron J, Kanaan R, et al. High prevalence of azole-resistant Aspergillus fumigatus in adults with cystic fibrosis exposed to itraconazole. Antimicrob Agents Chemother. 2012;56:869–74.
Tashiro M, Izumikawa K, Hirano K, Ide S, Mihara T, Hosogaya N, et al. Correlation between triazole treatment history and susceptibility in clinically isolated Aspergillus fumigatus. Antimicrob Agents Chemother. 2012;56:4870–5.
Alastruey-Izquierdo A, Mellado E, Pelaez T, Peman J, Zapico S, Alvarez, et al. Population-based survey of filamentous fungi and antifungal resistance in Spain (FILPOP study). Antimicrob Agents Chemother. 2013;57:3380–7.
Escribano P, Pelaez T, Muñoz P, Bouza E, Guinea J. Is azole resistance in Aspergillus fumigatus a problem in Spain? Antimicrob Agents Chemother. 2013;57:2815–20.
Fischer J, van Koningsbruggen-Rietschel S, Rietschel E, Vehreschild MJ, Wisplinghoff H, Kronke M, et al. Prevalence and molecular characterization of azole resistance in Aspergillus spp. Isolates from German cystic fibrosis patients. J Antimicrob Chemother. 2014;69:1533–6.
Steinmann J, Hamprecht A, Vehreschild MJGT, Cornely OA, Buchheidt D, Spiess B, et al. Emergence of azole-resistant invasive aspergillosis in HSCT recipients in Germany. J Antimicrob Chemother. 2015;70:1522–6.
Jensen RH, Hagen F, Astvad KMT, Tyron A, Meis JF, Arendrup MC. Azole-resistant Aspergillus fumigatus in Denmark: a laboratory-based study on resistance mechanisms and genotypes. Clin Microbiol Infect. 2016;22:(6)570.e1–9.
Balajee SA, Kano R, Baddley JW, Moser SA, Marr KA, Alexander BD, et al. Molecular identification of Aspergillus species collected for the transplant-associated infection surveillance network. J Clin Microbiol. 2009;47:3138–41.
Balajee SA, Marr KA. Phenotypic and genotypic identification of human pathogenic aspergilli. Future Microbiol. 2006;1:435–45.
Vinh DC, Shea YR, Sugui JA, Parrilla-Castellar ER, Freeman AF, Campbell JW, et al. Invasive aspergillosis due to Neosartorya udagawae. Clin Infect Dis. 2009;49:102–11.
Posteraro B, Mattei R, Trivella F, Maffei A, Torre A, De Carolis E, et al. Uncommon Neosartorya udagawae fungus as a causative agent of severe corneal infection. J Clin Microbiol. 2011;49(6):2357–60.
Alanio A, Denis B, Hamane S, Raffoux E, Peffault de Latour R, Menotti J, et al. Azole resistance of Aspergillus fumigatus in immunocompromised patients with invasive aspergillosis. Emerg Infect Dis. 2016;22(1):157–8.
van der Linden JW, Arendrup MC, Melchers WJ, Verweij PE. Azole resistance of Aspergillus fumigatus in immunocompromised patients with invasive aspergillosis. Emerg Infect Dis. 2016;22(1):158–9.
Fuhren J, Voskuil WS, Boel CH, Haas PJ, Hagen F, Meis JF, et al. High prevalence of azole resistance in Aspergillus fumigatus isolates from high-risk patients. J Antimicrob Chemother. 2015;70(10):2894–8.
Lepesheva GI, Waterman MR. Sterol 14alpha-demethylase cytochrome P450 (CYP51), a P450 in all biological kingdoms. Biochim Biophys Acta. 2007;1770(3):467–77.
Hargrove TY, Wawrzak Z, Lamb DC, Guengerich FP, Lepesheva GI. Structure-functional characterization of cytochrome P450 sterol 14α-demethylase (CYP51B) from Aspergillus fumigatus and molecular basis for the development of antifungal drugs. J Biol Chem. 2015;290:23916–34.
Ghannoum MA, Rice LB. antifungal agents: mode of action, mechanisms of resistance, and correlation of these mechanisms with bacterial resistance. Clin Microbiol Rev. 1999;12(4):501–17.
Marichal P, Gorrens J, Vanden Bossche H. The action of itraconazole and ketoconazole on growth and sterol synthesis in Aspergillus fumigatus and Aspergillus niger. Sabouraudia. 1985;23(1):13–21.
Parker JE, Warrilow AG, Price CL, Mullins JG, Kelly DE, Kelly SL. Resistance to antifungals that target CYP51. J Chem Biol. 2014;7:143–61.
Mellado E, Diaz-Guerra TM, Cuenca-Estrella M, Rodriguez-Tudela JL. Identification of two different 14-α sterol demethylase-related genes (cyp51A and cyp51B) in Aspergillus fumigatus and other Aspergillus species. J Clin Microbiol. 2001;39:2431–8.
Mellado E, Garcia-Effron G, Buitrago MJ, Alcazar-Fuoli L, Cuenca-Estrella M, Rodriguez-Tudela JL. Targeted gene disruption of the 14-alpha sterol demethylase (cyp51A) in Aspergillus fumigatus and its role in azole drug susceptibility. Antimicrob Agents Chemother. 2005;49:2536–8.
Hu W, Sillaots S, Lemieux S, Davison J, Kauffman S, Breton A, et al. Essential gene identification and drug target prioritization in Aspergillus fumigatus. PLoS Pathog. 2007;3:e24.
Alcazar-Fuoli L, Mellado E. Current status of antifungal resistance and its impact on clinical practice. Br J Haematol. 2014;166(4):471–84.
Buied A, Moore CB, Denning DW, Bowyer P. High-level expression of cyp51B in azole-resistant clinical Aspergillus fumigatus isolates. J Antimicrob Chemother. 2013;68:512–4.
Bueid A, Howard SJ, Moore CB, Richardson MD, Harrison E, Bowyer P, et al. Azole antifungal resistance in A. fumigatus: 2008 and 2009. J Antimicrob Chemother. 2010;65(10):2116–8.
Diaz-Guerra TM, Mellado E, Cuenca-Estrella M, Rodriguez-Tudela JL. A point mutation in the 14alpha-sterol demethylase gene cyp51A contributes to itraconazole resistance in Aspergillus fumigatus. Antimicrob Agents Chemother. 2003;47:1120–4.
Mann PA, Parmegiani RM, Wei SQ, Mendrick CA, Li X, Loebenberg D, et al. Mutations in Aspergillus fumigatus resulting in reduced susceptibility to posaconazole appear to be restricted to a single amino acid in the cytochrome P450 14alpha-demethylase. Antimicrob Agents Chemother. 2003;47:577–81.
Mellado E, Garcia-Effron G, Alcazar-Fuoli L, Cuenca-Estrella M, Rodriguez-Tudela JL. Substitutions at methionine 220 in the 14-alpha sterol demethylase (Cyp51A) of Aspergillus fumigatus are responsible for resistance in vitro to azole antifungal drugs. Antimicrob Agents Chemother. 2004;48:2747–50.
Chen J, Li H, Li R, Bu D, Wan Z. Mutations in the cyp51A gene and susceptibility to itraconazole in Aspergillus fumigatus serially isolated from a patient with lung aspergilloma. J Antimicrob Chemother. 2005;55:31–7.
Bellete B, Raberin H, Morel J, Flori P, Hafid J, Manhsung RT. Acquired resistance to voriconazole and itraconazole in a patient with pulmonary aspergilloma. Med Mycol. 2010;48:197–200.
Pelaez T, Gijon P, Bunsow E, Bouza E, Sanchez-Yebra W, Valerio M, et al. Resistance to voriconazole due to a G448S substitution in Aspergillus fumigatus in a patient with cerebral aspergillosis. J Clin Microbiol. 2012;50:2531–4.
Krishnan Natesan S, Wu W, Cutright JL, Chandrasekar PH. In vitro-in vivo correlation of voriconazole resistance due to G448S mutation (cyp51A gene) in Aspergillus fumigatus. Diagn Microbiol Infect Dis. 2012;74(3):272–7.
Manavathu EK, Baskaran I, Krishnan S, Alangaden G, Chandrasekar PH. Cytochrome P450 14-alpha-sterol demethylase mutation dependent triazole cross-resistance in Aspergillus fumigatus. In: Proceedings of 43rd Interscience Conference on Antimicrobial Agents and Chemotherapy; Chicago, IL, USA; 2003 Sep 14–17. Abstract M–471.
Howard SJ, Webster I, Moore CB, Gardiner RE, Park S, Perlin DS, et al. Multi-azole resistance in Aspergillus fumigatus. Int J Antimicrob Agents. 2006;28:450–3.
Albarrag AM, Anderson MJ, Howard SJ, Robson GD, Warn PA, Sanglard D, et al. Interrogation of related clinical pan-azole-resistant Aspergillus fumigatus strains: G138C, Y431C, and G434C single nucleotide polymorphisms in cyp51A, upregulation of cyp51A, and integration and activation of transposon Atf1 in the cyp51a promoter. Antimicrob Agents Chemother. 2011;55:5113–21.
Fraczek MG, Bromley M, Bowyer P. An improved model of the Aspergillus fumigatus CYP51A protein. Antimicrob Agents Chemother. 2011;55(5):2483–6.
Warrilow AG, Parker JE, Price CL, Nes WD, Kelly SL, Kelly DE. In vitro biochemical study of cyp51-mediated azole resistance in Aspergillus fumigatus. Antimicrob Agents Chemother. 2015;59(12):7771–8.
da Silva Ferreira ME, Capellaro JL, dos Reis Marques E, Malavazi I, Perlin D, Park S, et al. In vitro evolution of itraconazole resistance in Aspergillus fumigatus involves multiple mechanisms of resistance. Antimicrob Agents Chemother. 2004;48:4405–13.
Alanio A, Sitterle E, Liance M, Farrugia C, Foulet F, Botterel F, et al. Low prevalence of resistance to azoles in Aspergillus fumigatus in a French cohort of patients treated for haematological malignancies. J Antimicrob Chemother. 2011;66:371–4.
Escribano P, Recio S, Pelaez T, Bouza E, Guinea J. Aspergillus fumigatus strains with mutations in the cyp51A gene do not always show phenotypic resistance to itraconazole, voriconazole, or posaconazole. Antimicrob Agents Chemother. 2011;55:2460–2.
Camps SM, van der Linden JW, Li Y, Kuijper EJ, van Dissel JT, Verweij PE, et al. Rapid induction of multiple resistance mechanisms in Aspergillus fumigatus during azole therapy: a case study and review of the literature. Antimicrob Agents Chemother. 2012;56:10–6.
Bader O, Weig M, Reichard U, Lugert R, Kuhns M, Christner M, et al. cyp51A-based mechanisms of Aspergillus fumigatus azole drug resistance present in clinical samples from Germany. Antimicrob Agents Chemother. 2013;57:3513–7.
Rodriguez-Tudela JL, Alcazar-Fuoli L, Mellado E, Alastruey-Izquierdo A, Monzon A, Cuenca-Estrella M. Epidemiological cutoffs and cross-resistance to azole drugs in Aspergillus fumigatus. Antimicrob Agents Chemother. 2008;52(7):2468–72.
Snelders E, Huis In ‘t Veld RA, Rijs AJ, Kema GH, Melchers WJ, Verweij PE. Possible environmental origin of resistance of Aspergillus fumigatus to medical triazoles. Appl Environ Microbiol. 2009;75:4053–7.
Alanio A, Cabaret O, Sitterlé E, Costa JM, Brisse S, Cordonnier C, et al. Azole preexposure affects the Aspergillus fumigatus population in patients. Antimicrob Agents Chemother. 2012;56(9):4948–50.
Zhao Y, Stensvold CR, Perlin DS, Arendrup MC. Azole resistance in Aspergillus fumigatus from bronchoalveolar lavage fluid samples of patients with chronic diseases. J Antimicrob Chemother. 2013;68:1497–504.
Chowdhary A, Sharma C, Kathuria S, Hagen F, Meis JF. Prevalence and mechanism of triazole resistance in Aspergillus fumigatus in a referral chest hospital in Delhi, India and an update of the situation in Asia. Front Microbiol. 2015;6:428.
Kidd SE, Goeman E, Meis JF, Slavin MA, Verweij PE. Multi-triazole-resistant Aspergillus fumigatus infections in Australia. Mycoses. 2015;58:350–5.
Abdolrasouli A, Rhodes J, Beale MA, Hagen F, Rogers TR, Chowdhary A, et al. Genomic context of azole resistance mutations in Aspergillus fumigatus determined using whole-genome sequencing. MBio. 2015;6(3):e00536.
Snelders E, Karawajczyk A, Schaftenaar G, Verweij PE, Melchers WJ. Azole resistance profile of amino acid changes in Aspergillus fumigatus CYP51A based on protein homology modeling. Antimicrob Agents Chemother. 2010;54(6):2425–30.
Garcia-Rubio R, Monteiro MC, Alcazar-Fuoli L, Cuesta I, Pelaez T, Mellado E. Aspergillus fumigatus cyp51A polymorphisms: SNPs with or without significance? In: 7th Advances Against Aspergillosis. Manchester, UK; 2016 March 3–5. Abstract P-37.
Mellado E, Garcia-Effron G, Alcazar-Fuoli L, Melchers WJ, Verweij PE, Cuenca-Estrella M, et al. A new Aspergillus fumigatus resistance mechanism conferring in vitro cross-resistance to azole antifungals involves a combination of cyp51A alterations. Antimicrob Agents Chemother. 2007;51(6):1897–904.
van der Linden JW, Camps SM, Kampinga GA, Arends JP, Debets-Ossenkopp YJ, Haas PJ, et al. Aspergillosis due to voriconazole highly resistant Aspergillus fumigatus and recovery of genetically related resistant isolates from domiciles. Clin Infect Dis. 2013;57:513–20.
Vermeulen E, Maertens J, Schoemans H, Lagrou K. Azole-resistant Aspergillus fumigatus due to TR46/Y121F/T289A mutation emerging in Belgium, July 2012. Eur Surveill. 2012;17(48):20326
Astvad KM, Jensen RH, Hassan TM, Mathiasen EG, Thomsen GM, Pedersen UG, et al. First detection of TR46/Y121F/T289A and TR34/L98H alterations in Aspergillus fumigatus isolates from azole-naive patients in Denmark despite negative findings in the environment. Antimicrob Agents Chemother. 2014;58:5096–101.
Chowdhary A, Sharma C, Kathuria S, Hagen F, Meis JF. Azole-resistant Aspergillus fumigatus with the environmental TR46/Y121F/T289A mutation in India. J Antimicrob Chemother. 2014;69(2):555–7.
Chowdhary A, Sharma C, van den Boom M, Yntema JB, Hagen F, Verweij PE, et al. Multi-azole-resistant Aspergillus fumigatus in the environment in Tanzania. J Antimicrob Chemother. 2014;69:2979–83.
Chen Y, Wang H, Lu Z, Li P, Zhang Q, Jia T, et al. Emergence of TR46/Y121F/T289A in an Aspergillus fumigatus isolate from a Chinese patient. Antimicrob Agents Chemother. 2015;59:7148–50.
Lavergne RA, Morio F, Favennec L, Dominique S, Meis JF, Gargala G, et al. First description of azole-resistant Aspergillus fumigatus due to TR46/Y121F/T289A mutation in France. Antimicrob Agents Chemother. 2015;59:4331–5.
Pelaez T, Monteiro MC, Garcia-Rubio R, Bouza E, Gomez-Lopez A, Mellado E. First detection of Aspergillus fumigatus azole-resistant strain due to cyp51A TR46/Y121F/T289A in an azole-naive patient in Spain. New Microbes New Infect. 2015;6:33–4.
Le Pape P, Lavergne RA, Morio F, Alvarez-Moreno C. Multiple fungicide-driven alterations in azole-resistant Aspergillus fumigatus, Colombia, 2015. Emerg Infect Dis. 2016;22:156–7.
Hagiwara D, Takahashi H, Fujimoto M, Sugahara M, Misawa Y, Gonoi T, et al. Multi-azole resistant Aspergillus fumigatus harboring cyp51A TR46/Y121F/T289A isolated in Japan. J Infect Chemother. 2016;22(8):577–9.
Tangwattanachuleeporn M, Minarin N, Saichan S, Sermsri P, Mitkornburee R, Groß U, et al. Prevalence of azole-resistant Aspergillus fumigatus in the environment of Thailand. Med Mycol. 2016. doi:10.1093/mmy/myw090
Wiederhold NP, Gil VG, Gutierrez F, Lindner JR, Albataineh MT, McCarthy DI, et al. First detection of TR34/L98H and TR46/Y121F/T289A cyp51 mutations in Aspergillus fumigatus isolates in the United States. J Clin Microbiol. 2016;54:168–71.
Lescar J, Meyer I, Akshita K, Srinivasaraghavan K, Verma C, Palous M, et al. Aspergillus fumigatus harbouring the sole Y121F mutation shows decreased susceptibility to voriconazole but maintained susceptibility to itraconazole and posaconazole. J Antimicrob Chemother. 2014;69(12):3244–7.
Hodiamont CJ, Dolman KM, Ten Berge IJ, Melchers WJ, Verweij PE, Pajkrt D. Multiple-azole-resistant Aspergillus fumigatus osteomyelitis in a patient with chronic granulomatous disease successfully treated with long-term oral posaconazole and surgery. Med Mycol. 2009;47:217–20.
Sanglard D. Emerging threats in antifungal-resistant fungal pathogens. Front Med. 2016;3:11–3.
Coste AT, Karababa M, Ischer F, Bille J, Sanglard D. TAC1, transcriptional activator of CDR genes, is a new transcription factor involved in the regulation of Candida albicans ABC transporters CDR1 and CDR2. Eukaryot Cell. 2004;3(6):1639–52.
Morschhäuser J. Regulation of multidrug resistance in pathogenic fungi. Fungal Genet Biol. 2010;47(2):94–106.
Lamping E, Ranchod A, Nakamura K, Tyndall JD, Niimi K, Holmes AR, et al. Abc1p is a multidrug efflux transporter that tips the balance in favor of innate azole resistance in Candida krusei. Antimicrob Agents Chemother. 2009;53(2):354–69.
Samaranayake YH, Cheung BP, Wang Y, Yau JY, Yeung KW, Samaranayake LP. Fluconazole resistance in Candida glabrata is associated with increased bud formation and metallothionein production. J Med Microbiol. 2013;62(2):303–18.
Slaven JW, Anderson MJ, Sanglard D, Dixon GK, Bille J, Roberts IS, et al. Increased expression of a novel Aspergillus fumigatus ABC transporter gene, atrF, in the presence of itraconazole in an itraconazole resistant clinical isolate. Fungal Genet Biol. 2002;36(3):199–206.
da Silva Ferreira ME, Malavazi I, Savoldi M, Brakhage AA, Goldman MH, Kim HS, et al. Transcriptome analysis of Aspergillus fumigatus exposed to voriconazole. Curr Genet. 2006;50:32–44.
Fraczek MG, Bromley M, Buied A, Moore CB, Rajendran R, Rautemaa R, et al. The cdr1B efflux transporter is associated with non-cyp51 a mediated itraconazole resistance in Aspergillus fumigatus. J Antimicrob Chemother. 2013;68:1486–96.
Willger SD, Puttikamonkul S, Kim KH, Burritt JB, Grahl N, Metzler LJ, et al. A sterol-regulatory element binding protein is required for cell polarity, hypoxia adaptation, azole drug resistance, and virulence in Aspergillus fumigatus. PLoS Pathog. 2008;4(11):e1000200.
Moye-Rowley WS. Multiple mechanisms contribute to the development of clinically significant azole resistance in Aspergillus fumigatus. Front Microbiol. 2015;6:70.
Camps SM, Dutilh BE, Arendrup MC, Rijs AJ, Snelders E, Huynen MA, et al. Discovery of a HapE mutation that causes azole resistance in Aspergillus fumigatus through whole genome sequencing and sexual crossing. PLoS One. 2012;7(11):e50034.
Gsaller F, Hortschansky P, Furukawa T, Carr PD, Rash B, Capilla J, et al. Sterol biosynthesis and azole tolerance is governed by the opposing actions of SrbA and the CCAAT binding complex. PLoS Pathog. 2016;12(7):e1005775.
Bromley M, Johns A, Davies E, Fraczek M, Gilsenan JM, Kurbatova N, et al. Mitochondrial complex i is a global regulator of secondary metabolism, virulence and azole sensitivity in fungi. PLoS One. 2016;11:e0158724.
Lessing F, Kniemeyer O, Wozniok I, Loeffler J, Kurzai O, Haert A, et al. The Aspergillus fumigatus transcriptional regulator AfYap1 represents the major regulator for defense against reactive oxygen intermediates but is dispensable for pathogenicity in an intranasal mouse infection model. Eukaryot Cell. 2007;6:2290–302.
Qiao J, Liu W, Li R. Truncated Afyap1 attenuates antifungal susceptibility of Aspergillus fumigatus to voriconazole and confers adaptation of the fungus to oxidative stress. Mycopathologia. 2010;170:155–60.
Richardson M, Lass-Flörl C. Changing epidemiology of systemic fungal infections. Clin Microbiol Infect. 2008;14(Suppl 4):5–24.
Samson RA, Hong S, Peterson SW, Frisvad JC, Varga J. Polyphasic taxonomy of Aspergillus section Fumigati and its teleomorph Neosartorya. Stud Mycol. 2007;59:147–203.
Frisvad JC, Larsen TO. Extrolites of Aspergillus fumigatus and other pathogenic species in Aspergillus Section Fumigati. Front Microbiol. 2016;6:1485.
Alcazar-Fuoli L, Mellado E, Alastruey-Izquierdo A, Cuenca-Estrella M, Rodriguez-Tudela JL. Aspergillus section Fumigati: antifungal susceptibility patterns and sequence-based identification. Antimicrob Agents Chemother. 2008;52:1244–51.
van der Linden JW, Warris A, Verweij PE. Aspergillus species intrinsically resistant to antifungal agents. Med Mycol. 2011;49(Suppl 1):82–9.
Alastruey-Izquierdo A, Alcazar-Fuoli L, Cuenca-Estrella M. Antifungal susceptibility profile of cryptic species of Aspergillus. Mycopathologia. 2014;178:427–33.
Lamoth F. Aspergillus fumigatus-related species in clinical practice. Front Microbiol. 2016;7:683.
Datta K, Rhee P, Byrnes E, Garcia-Effron G, Perlin DS, Staab JF, et al. Isavuconazole activity against Aspergillus lentulus, Neosartorya udagawae, and Cryptococcus gattii, emerging fungal pathogens with reduced azole susceptibility. J Clin Microbiol. 2013;51(9):3090–3.
Alcazar-Fuoli L, Cuesta I, Rodriguez-Tudela JL, Cuenca-Estrella M, Sanglard D, Mellado E. Three-dimensional models of 14 alpha- sterol demethylase (Cyp51A) from Aspergillus lentulus and Aspergillus fumigatus: an insight into differences in voriconazole interaction. Int J Antimicrob Agents. 2011;38:426–34.
Mellado E, Alcazar-Fuoli L, Cuenca-Estrella M, Rodriguez-Tudela JL. Role of Aspergillus lentulus 14-α sterol demethylase (Cyp51A) in azole drug susceptibility. Antimicrob Agents Chemother. 2011;55(12):5459–68.
Balajee SA, Gribskov J, Brandt M, Ito J, Fothergill A, Marr KA. Mistaken identity: Neosartorya pseudofischeri and its anamorph masquerading as Aspergillus fumigatus. J Clin Microbiol. 2005;43:5996–9.
Guinea J, Sandoval-Denis M, Escribano P, Pelaez T, Guarro J, Bouza E. Aspergillus citrinoterreus, a new species of section terrei isolated from samples of patients with nonhematological predisposing conditions. J Clin Microbiol. 2015;53:611–7.
Varga J, Houbraken J, van der Lee HA, Verweij PE, Samson RA. Aspergillus calidoustus sp. nov., causative agent of human infections previously assigned to Aspergillus ustus. Eukaryot Cell. 2008;7:630–8.
Alastruey-Izquierdo A, Cuesta I, Houbraken J, Cuenca-Estrella M, Monzon A, Rodriguez-Tudela JL. In vitro activity of nine antifungal agents against clinical isolates of Aspergillus calidoustus. Med Mycol. 2010;48:97–102.
Meneau I, Sanglard D. Azole and fungicide resistance in clinical and environmental Aspergillus fumigatus isolates. Med Mycol. 2005;43(1):307–11.
Cowen LE, Sanglard D, Howard SJ, Rogers PD, Perlin DS. Mechanisms of antifungal drug resistance. Cold Spring Harb Perspect Med. 2015;5:a019752.
Bowyer P, Moore CB, Rautemaa R, Denning DW, Richardson MD. Azole antifungal resistance today: focus on Aspergillus. Curr Infect Dis Rep. 2011;13(6):485–91.
Dannaoui E, Borel E, Monier MF, Piens MA, Picot S, Persat F. Acquired itraconazole resistance in Aspergillus fumigatus. J Antimicrob Chemother. 2001;47(3):333–40.
Snelders E, Melchers WJ, Verweij PE. Azole resistance in Aspergillus fumigatus: a new challenge in the management of invasive aspergillosis? Future Microbiol. 2011;6:335–47.
Howard SJ, Pasqualotto AC, Anderson MJ, Leatherbarrow H, Albarrag AM, Harrison E, et al. Major variations in Aspergillus fumigatus arising within aspergillomas in chronic pulmonary aspergillosis. Mycoses. 2013;56:434–41.
Chen J, Li H, Li R, Bu D, Wan Z. Mutations in the cyp51A gene and susceptibility to itraconazole in Aspergillus fumigatus serially isolated from a patient with lung aspergilloma. J Antimicrob Chemother. 2004;55:31–7.
Stensvold RC, Jørgensen LN, Arendrup MC. Azole-resistant invasive aspergillosis: relationship to agriculture. Curr Fung Infect Rep. 2012;6:178–91.
Snelders E, Camps SM, Karawajczyk A, Schaftenaar G, Kema GH, van der Lee HA, et al. Triazole fungicides can induce cross-resistance to medical triazoles in Aspergillus fumigatus. PLoS One. 2012;7:e31801.
Hamamoto H, Hasegawa K, Nakaune R, Lee YJ, Makizumi Y, Akutsu K. Tandem repeat of a transcriptional enhancer upstream of the sterol 14alpha-demethylase gene (CYP51) in Penicillium digitatum. Appl Environ Microbiol. 2000;66:3421–6.
Ghosoph JM, Schmidt LS, Margosan DA, Smilanick JL. Imazalil resistance linked to a unique insertion sequence in the PdCYP51 promoter region of Penicillium digitatum. Posthavest Biol Tec. 2007;44:9–18.
Schnabel G, Jones AL. The 14alpha-demethylase (CYP51A1) gene is overexpressed in Venturia inaequalis strains resistant to myclobutanil. Phytopathology. 2001;91:102–10.
Ma Z, Proffer TJ, Jacobs JL, Sundin GW. Overexpression of the 14 alpha-demethylase target gene (CYP51) mediates fungicide resistance in Blumeriella jaapii. Appl Environ Microbiol. 2006;72:2581–5.
Luo CX, Schnabel G. The cytochrome P450 lanosterol 14alpha-demethylase gene is a demethylation inhibitor fungicide resistance determinant in Monilinia fructicola field isolates from Georgia. Appl Environ Microbiol. 2008;74(2):359–66.
Délye C, Laigret F, Corio-Costet MF. A mutation in the 14alpha-demethylase gene of Uncinula necator that correlates with resistance to a sterol biosynthesis inhibitor. Appl Environ Microbiol. 1997;63:2966–70.
Délye C, Bousset L, Corio-Costet MF. PCR cloning and detection of point mutations in the eburicol 14α-demethylase (CYP51) gene from Erysiphe graminis f. sp. hordei, a “recalcitrant” fungus. Current Genetics. 1998;34:399–403.
Butters JA, Zhou MC, Hollomon DW. The mechanism of resistance to sterol 14α-demethylation inhibitors in a mutant (Erg40) of Ustilago maydis. Pest Manag Sci. 2000;56:257–63.
Wyand RA, Brown JK. Sequence variation in the CYP51 gene of Blumeria graminis associated with resistance to sterol demethylase inhibiting fungicides. Fungal Genet Biol. 2005;42(8):726–35.
Fraaije BA, Cools HJ, Kim SH, Motteram J, Clark WS, Lucas JA. A novel substitution I381V in the sterol 14-α demethylase (Cyp51) of Mycosphaerella graminicola is differentially selected by azole fungicides. Mol Plant Pathol. 2007;8:245–54.
Leroux P, Albertini C, Gautier A, Gredt M, Walker AS. Mutations in the CYP51 gene correlated with changes in sensitivity to sterol 14 alpha-demethylation inhibitors in field isolates of Mycosphaerella graminicola. Pest Manag Sci. 2007;63:688–98.
Stammler G, Cordero J, Koch A, Semar M, Schlehuber S. Role of the Y134F mutation in cyp51 and overexpression of cyp51 in the sensitivity response of Puccinia triticina to epoxiconazole. Crop Protect. 2009;28:891–7.
Mair WJ, Deng W, Mullins JG, West S, Wang P, Besharat N, et al. demethylase inhibitor fungicide resistance in Pyrenophora teres f. sp. teres associated with target site modification and inducible overexpression of cyp51. Front Microbiol. 2016;7:1279.
Carter HE, Fraaije BA, West JS, Kelly SL, Mehl A, Shaw MW, et al. Alterations in the predicted regulatory and coding regions of the sterol 14α-demethylase gene (CYP51) confer decreased azole sensitivity in the oilseed rape pathogen Pyrenopeziza brassicae. Mol Plant Pathol. 2014;15(5):513–22.
European Centre for Disease Prevention and Control. Risk assessment on the impact of environmental usage of triazoles on the development and spread of resistance to medical triazoles in Aspergillus species. Stockholm: ECDC 2013; 2013. In: http://ecdc.europa.eu/en/publications/technical_reports/Pages/index.aspx. Accessed 1 Nov 2016.
Verweij PE, Mellado E, Melchers WJ. Multiple-triazole-resistant aspergillosis. N Engl J Med. 2007;356:1481–3.
Chowdhary A, Kathuria S, Xu J, Sharma C, Sundar G, Singh PK, et al. Clonal expansion and emergence of environmental multiple-triazole-resistant Aspergillus fumigatus strains carrying the TR34/L98H mutations in the cyp51A gene in India. PLoS One. 2012;7:e52871.
Bader O, Tünnermann J, Dudakova A, Tangwattanachuleeporn M, Weig M, Groß U. Environmental isolates of azole-resistant Aspergillus fumigatus in Germany. Antimicrob Agents Chemother. 2015;59:4356–9.
Özmerdiven GE, Ak S, Ener B, Ağca H, Cilo BD, Tunca B, et al. First determination of azole resistance in Aspergillus fumigatus strains carrying the TR34/L98H mutations in Turkey. J Infect Chemother. 2015;21:581–6.
Wiederhold NP, Garcia Gil V, Lindner J, Sanders C, Fan H, Sutton DA, et al. Evaluation of Cyp51A mechanisms of azole resistance in Aspergillus fumigatus isolates from the United States. Mycoses. 2015;58(4):55.
Wu CJ, Wang HC, Lee JC, Lo HJ, Dai CT, Chou PH, et al. Azole-resistant Aspergillus fumigatus isolates carrying TR34/L98H mutations in Taiwan. Mycoses. 2015;58:544–9.
Chowdhary A, Sharma C, Hagen F, Meis JF. Exploring azole antifungal drug resistance in Aspergillus fumigatus with special reference to resistance mechanisms. Future Microbiol. 2014;9(5):697–711.
Denning DW, Bowyer P. Voriconazole resistance in Aspergillus fumigatus: should we be concerned? Clin Infect Dis. 2013;57(4):521–3.
Verweij PE, Chowdhary A, Melchers WJ, Meis JF. Azole resistance in Aspergillus fumigatus: can we retain the clinical use of mold-active antifungal azoles? Clin Infect Dis. 2016;62:362–8.
Aigner M, Lass-Flörl C. Treatment of drug-resistant Aspergillus infection. Expert Opin Pharmacother. 2015;16(15):2267–70.
Marr KA, Schlamm HT, Herbrecht R, Rottinghaus ST, Bow EJ, Cornely OA, et al. Combination antifungal therapy for invasive aspergillosis: a randomized trial. Ann Intern Med. 2015;162:81–9.
Panackal AA. Combination antifungal therapy for invasive aspergillosis revisited. Med Mycol Open Access. 2016;2(2):12.
Alanio A, Denis B, Hamane S, Raffoux E, Peffault de la Tour R, Touratier S, et al. New therapeutic strategies for invasive aspergillosis in the era of azole resistance: how should the prevalence of azole resistance be defined? J Antimicrob Chemother. 2016;71(8):2075–8.
Spiess B, Postina P, Reinwald M, Cornely OA, Hamprecht A, Hoenigl M, et al. Incidence of Cyp51 A key mutations in Aspergillus fumigatus—a study on primary clinical samples of immunocompromised patients in the period of 1995–2013. PLoS One. 2014;9(7):e103113.
Chong GM, van der Beek MT, von dem Borne PA, Boelens J, Steel E, Kampinga GA, et al. PCR-based detection of Aspergillus fumigatus Cyp51A mutations on bronchoalveolar lavage: a multicentre validation of the AsperGenius assay in 201 patients with haematological disease suspected for invasive aspergillosis. J Antimicrob Chemother. 2016;71(12):3528–35.
Denning DW, Bromley MJ. Infectious disease. How to bolster the antifungalpipeline. Science. 2015;347:1414–6.
Stewart ER, Thompson GR. Treatment of primary pulmonary aspergillosis: an assessment of the evidence. J Fungi. 2016;2(3):25.
Rivero-Menendez O, Alastruey-Izquierdo A, Mellado E, Cuenca-Estrella M (2016) Triazole resistance in Aspergillus spp.: a worldwide problem? J Fungi 2(3):21.
ECPA Assessment of the Economic Importance of Azoles in European Agriculture: WheatCaseStudy. Bologna: NOMISMA; 2012. In: http://www.ecpa.eu/article/agriculture-today/assessmenteconomicimportance-azoles-european-agriculture-wheat-casestud. Accessed 5 Nov 2016.
Price CL, Parker JE, Warrilow AG, Kelly DE, Kelly SL. Azole fungicides—understanding resistance mechanisms in agricultural fungal pathogens. Pest Manag Sci. 2015;71(8):1054–8.
Hagiwara D, Takahashi H, Watanabe A, Takahashi-Nakaguchi A, Kawamoto S, Kamei K, Gonoi T. Whole-genome comparison of Aspergillus fumigatus strains serially isolated from patients with aspergillosis. J Clin Microbiol. 2014;52:4202–9.
Jones L, Riaz S, Morales-Cruz A, Amrine KC, McGuire B, Gubler WD, et al. Adaptive genomic structural variation in the grape powdery mildew pathogen. Erysiphe necator. BMC Genomics. 2014;15:1081.
Vermeulen E, Maertens J, De BA, Nulens E, Boelens J, Surmont I, et al. Nationwide surveillance of azole resistance in Aspergillus diseases. Antimicrob Agents Chemother. 2015;59:4569–76.
Morio F, Aubin GG, Danner-Boucher I, Haloun A, Sacchetto E, Garcia-Hermoso D, et al. High prevalence of triazole resistance in Aspergillus fumigatus, especially mediated by TR34/L98H, in a French cohort of patients with cystic fibrosis. J Antimicrob Chemother. 2012;67:1870–3.
Amorim A, Guedes-Vaz L, Araujo R. Susceptibility to five antifungals of Aspergillus fumigatus strains isolated from chronically colonised cystic fibrosis patients receiving azole therapy. Int J Antimicrob Agents. 2010;35(4):396–9.
Verweij PE, Te Dorsthorst DT, Rijs AJ, De Vries-Hospers HG, Meis JF. Nationwide survey of in vitro activities of itraconazole and voriconazole against clinical Aspergillus fumigatus isolates cultured between 1945 and 1998. J Clin Microbiol. 2002;40(7):2648–50.
Klaassen CH, de Valk HA, Curfs-Breuker IM, Meis JF. Novel mixed-format real-time PCR assay to detect mutations conferring resistance to triazoles in Aspergillus fumigatus and prevalence of multi-triazole resistance among clinical isolates in the Netherlands. J Antimicrob Chemother. 2010;65(5):901–5.
van der Linden JW, Arendrup MC, Warris A, Lagrou K, Pelloux H, Hauser PM, et al. Prospective multicenter international surveillance of azole resistance in Aspergillus fumigatus. Emerg Infect Dis. 2015;21(6):1041–4.
Liu M, Zeng R, Zhang L, Li D, Lv G, Shen Y, et al. Multiple cyp51A-based mechanisms identified in azole-resistant isolates of Aspergillus fumigatus from China. Antimicrob Agents Chemother. 2015;59:4321–5.
Chowdhary A, Kathuria S, Randhawa HS, Gaur SN, Klaassen CH, Meis JF. Isolation of multiple-triazole-resistant Aspergillus fumigatus strains carrying the TR34/L98H mutations in the cyp51A gene in India. J Antimicrob Chemother. 2012;67:362–6.
Seyedmousavi S, Hashemi SJ, Zibafar E, Zoll J, Hedayati MT, Mouton JW, et al. Azole-resistant Aspergillus fumigatus, Iran. Emerg Infect Dis. 2013;19:832–4.
Mohammadi F, Hashemi SJ, Zoll J, Melchers WJ, Rafati H, Dehghan P, et al. Quantitative analysis of single-nucleotide polymorphism for rapid detection of TR34. Antimicrob Agents Chemother. 2015;60:387–92.
Kikuchi K, Watanabe A, Ito J, Oku Y, Wuren T, Taguchi H, et al. Antifungal susceptibility of Aspergillus fumigatus clinical isolates collected from various areas in Japan. J Infect Chemother. 2014;20:336–8.
Ahmad S, Joseph L, Hagen F, Meis JF, Khan Z. Concomitant occurrence of itraconazole-resistant and -susceptible strains of Aspergillus fumigatus in routine cultures. J Antimicrob Chemother. 2015;70:412–5.
Hsueh PR, Lau YJ, Chuang YC, Wan JH, Huang WK, Shyr JM, et al. Antifungal susceptibilities of clinical isolates of Candida species, Cryptococcus neoformans, and Aspergillus species from Taiwan: surveillance of multicenter antimicrobial resistance in Taiwan program data from 2003. Antimicrob Agents Chemother. 2005;49:512–7.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Funding
Funding was provided by Instituto de Salud Carlos III (FIS:PI15CIII/00019, REIPI RD16CIII/0004/0003).
Conflict of Interest
RGR, MCE and EM have no conflicts of interest to declare.
Rights and permissions
About this article

Cite this article
Garcia-Rubio, R., Cuenca-Estrella, M. & Mellado, E. Triazole Resistance in Aspergillus Species: An Emerging Problem. Drugs 77, 599–613 (2017). https://doi.org/10.1007/s40265-017-0714-4
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40265-017-0714-4