
Abstract
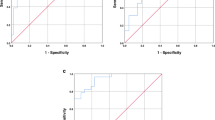
The aim of the study was to establish the best cut-off value for the homeostatic model assessment (HOMA) index in identifying children and adolescents with the metabolic syndrome. The study included 72 non-obese and 68 obese children aged 7 to 16 years. Obesity is defined using the criteria proposed by Coleet al., being included as metabolic syndrome variables waist circumference, systolic blood pressure, diastolic blood pressure and seric values of glucose, uric acid, fasting insulin, leptin, triglycerides and HDL-cholesterol. Children were considered as having the metabolic syndrome when four or more characteristics showed abnormal values. The HOMA index was calculated as the product of the fasting plasma insulin level (μU/mL) and the fasting plasma glucose level (mmol/L), divided by 22.5. HOMA index cut-offs from the 5th to the 95th percentile were used. A receiver operating characteristic (ROC) curve was generated using the different HOMA cut-offs for the screening of the metabolic syndrome. The areas under the ROC curve, 95% confidence intervals, and the point to the ROC curve closest to 1, were calculated. The area under the ROC curve was 0.863 (95% C.I.: 0.797, 0.930). The point closest to 1 corresponds to the 60th percentile of the HOMA index distribution in our sample. HOMA index value at the 60th percentile was 2.28. Cut-off values corresponding to a range of HOMA index from the 50 to the 75 percentile, showed similar distances to 1. HOMA index values for percentiles 50 to 75 ranged from 2.07 to 2.83. In conclusion, HOMA index could be a useful tool to detect children and adolescents with the metabolic syndrome. HOMA cut-off values need to be defined in the paediatric population; however, values near to 3 seem to be adequate.
Resumen
El objetivo del estudio era establecer el mejor punto de corte del índice HOMA (Homeostatic Model Assessment) para la identificación de niños y adolescentes con el síndrome metabólico. Se incluyeron 72 niños noobesos y 68 obesos, con edades entre 7 y 16 años. Se definió obesidad según los criterios propuestos por Cole y cols. Las variables utilizadas para describir el síndrome metabólico fueron las siguientes: Perímetro de la cintura, tensión arterial sistólica y diastólica, glucosa, ácido úrico, insulina en ayunas, leptina, triglicéridos y HDL-colesterol. Se consideraba que un niño tenía el síndrome metabólico cuando presentaba cuatro o más de estas características con valores anormales. El índice HOMA se calculó como el producto de las concentraciones de insulina en ayunas (μU/mL) y la glucosa plasmática en ayunas (mmol/L), dividido por 22.5. Se calcularon puntos de corte del índice HOMA correspondientes a los percentiles entre 5 y 95. Se elaboró una curva ROC (Receiver Operating Characteristics) tomando los diferentes puntos de corte del índice HOMA para la identificación del síndrome metabólico. Se calculó el área bajo la curva ROC, los intervalos de confianza al 95% y el punto de la curva ROC más cercano a 1. El área bajo la curva fue 0.863 (IC 95%: 0.797, 0.930). El punto más cercano a 1 correspondía al percentil 60 del índice HOMA en nuestra muestra. El valor del índice HOMA para el percentil 60 era 2.28. Puntos de corte del índice HOMA correspondientes a los percentiles comprendidos entre 50 y 75, mostraban distancias similares a 1. Los valores de índice HOMA correspondientes a estos percentiles oscilaban entre 2.07 y 2.83. En conclusión, el índice HOMA puede ser un buen instrumento para detectar el síndrome metabólico en niños y adolescentes. Es necesario definir mejor el punto de corte a utilizar en la población pediátrica; sin embargo, valores cercanos a 3 parecen ser los más adecuados.
Article PDF
Similar content being viewed by others


Avoid common mistakes on your manuscript.
References
Cole, T.J., Bellizi M.C., Flegal, K.M., Dietz, W.H. (2000):Br. Med. J.,320, 1240–1243.
Csabi, G., Török, K., Jeges, S., Molnár D. (2000):Eur. J. Pediatr.,159, 91–94.
De Ridder, C.M., De Boer, R.W., Seidell, J.C., Nieuwenhoff, C.M., Jeneson, J.A., Bakker, C.J., Zonderland, M.L., Erich, W.B. (1992):Int. J. Obes.,16, 443–449.
De Vegt, F., Dekker, J.M., Jager, A., Hienkens, E., Kostense, P.J., Stehouwer, C.D., Nijpels, G., Bouter, L.M. and Heine, R.J. (2001):JAMA,285, 2109–2113.
DeFronzo, R.A., Tobin, J.D., and Andres, R. (1979):Am. J. Physiol.,237, E214-E223.
Dresner, A., Laurent, D., Marcucci, M., Griffin, M.E., Dufour, S., Cline, G.W., Slezak, L.A., Andersen, D.K., Hundal, R.S., Rothman, D.L., Petersen, K.F. and Shulman, G.I. (1999):J. Clin. Invest.,103, 253–259.
Edelstein, S.L., Knowler, W.C., Bain, R.P., Andres, R., Barrett-Connor, E.L., Dowse, G.K., Haffner, S.M., Pettit, D.J., Sorkin, J.D. and Muller, D.C. (1997):Diabetes,46, 701–710.
Ford, E.S., Giles, W.H., and Dietz, W.H. (2002):JAMA,287, 356–359.
Fox, K., Peters, D., Armstrong, N., Sharpe, P., and Bell, M. (1993):Int. J. Obes.,17, 11–16.
Hansen, B.C. (1999):Ann. N.Y. Acad. Sci.,892, 1–24.
Hodge, A.M., Boyko, E.J., De Courten, M., Zimmet, P.Z., Chitson, P., Tuomilehto, J., and Alberti, K.G. (2001):Int. J. Obes.,25, 126–131.
Kissebah, A.H., Vydelingum, N., Murray, R., Evans, D.J., Hartz, A.J., Kalkhoff, R.K., and Adams, P.W. (1982):J. Clin. Endocrinol. Metab.,54, 254–260.
Leyva, F., Godsland, I.F., Ghatei, M., Proudler, A.J., Aldis, S., Walton, C., Bloom, S., and Stevenson, J.C. (1998):Arterioscler. Thromb. Vasc. Biol.,18, 928–933.
Livingstone, B. (2000):Eur. J. Pediatr.,159, 14–34.
Maffeis, C., Pietrobelli, A., Grezzani, A., Provera, S., Tatò, L. (2001):Obes. Res.,9, 179–187.
Mattews, D.R., Hosker, J.P., Rudenski, A.S., Naylor, B.A., Treacher D.F., and Turner, R.C. (1985):Diabetologia,28, 412–419.
Molnár, D. (2004):Int. J. Obes. Relat. Metab. Disord.,28 (suppl 3), S70-S74.
Moreno, L.A., Fleta, J., Mur, L., Rodríguez, G., Sarría, A., Bueno, M. (1999):Eur. J. Clin. Nutr.,53, 429–433.
Moreno, L.A., Joyanes, M., Mesana, M.I., González-Gross, M., Gil, C.M., Sarría, A., Gutiérrez, G., Garaulet, M., Pérez-Prieto, R., Bueno, M., Marcos, A. and for the AVENA Study Group (2003):Nutrition 19, 481–486.
Moreno, L.A., Mesana, M.I., Fleta, J., Ruiz, J.R., González-Gross, M., Sarría, A., Marcos, A., Bueno, M., and the AVENA Study groups:Ann. Nutr. Metab.,49, 71–76.
Moreno, L.A., Pineda, I., Rodríguez, G., Fleta, J., Sarría, A., Bueno, M. (2002):Acta Paediatr.,91, 1307–1312.
Must, A., Jacques, P.F., Dallal, G.E., Bajema, C.J. and Dietz, W.H. (1992):N. Engl. J. Med.,327, 1350–1355.
Popkin, B.M. and Doak, C.M. (1998):Nutr. Rev.,56, 106–114.
Pouliot, M.C., Despres, J.P., Lemieux, S., Moorjani, S., Bouchard, C., Tremblay, A., Nadeau, A., and Lupien, P.J. (1994):Am. J. Cardiol.,73, 460–468.
Rexrode, K.M., Carey, V.J., Hennekens, C.H., Walters, E.E., Colditz, G.A., Stampfer, M.J., Willett, W.C., and Manson, J.E. (1998):JAMA,280, 1843–1848.
Rimm, E.B., Stampfer, M.J., Giovannuci, E., Ascherio, A., Spiegelman, D., Colditz, G.A., and Willett, W.C. (1995):Am. J. Epidemiol.,141, 1117–1127.
Sarría, A., Moreno, L.A., García-Llop, L.A., Fleta, J., Morellón, M.P., and Bueno, M. (2001):Acta Paediatr.,90, 387–392.
Savva, S.C., Tornaritis, M., Savva, M.E., Kourides, Y., Panagi, A., Silikiotou, N., Georgiou, C., and Kafatos, A. (2000):Int. J. Obes.,24, 1453–1458.
Seidell, J.C., Oorsterlee, A., Deurenberg, P., Hautvast, J.G.A.J., and Ruijs J.H.J. (1988):Eur. J. Clin. Nutr.,42, 805–815.
Tresaco, B., Bueno, G., Moreno, L.A., Garagorri, J.M., Bueno, M. (2003):J. Physiol. Biochem.,59, 217–224.
Trevisan, M., Liu, J., Bahsas, F., Menotti, A., for the Risk Factor and Life Expectancy Research Group (1998):Am. J. Epidemiol.,148, 958–966.
Uwaifo, G.I., Fallon, E.M., Chin, J., Elberg, J., Parikh, S.J., and Yanovski, J.A. (2002):Diabetes Care,25, 2081–2087.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Tresaco, B., Bueno, G., Pineda, I. et al. Homeostatic model assessment (HOMA) index cut-off values to identify the metabolic syndrome in children. J. Physiol. Biochem. 61, 381–388 (2005). https://doi.org/10.1007/BF03167055
Received:
Issue Date:
DOI: https://doi.org/10.1007/BF03167055