
Abstract
Objective
To assess the utility of continuous metabolic syndrome score (cMetS) for predicting metabolic syndrome (MS) and determine the cut-off values in overweight and obese children.
Methods
This study was conducted among 104 children (7–14 y) attending obesity clinics of a tertiary care hospital in Mumbai, India. The cMetS was computed by standardizing the residuals of waist circumference (WC), mean arterial blood pressure (MAP), high density lipoprotein cholesterol (HDL-C), triglycerides (TG), and Homeostatic Model Assessment for Insulin Resistance (HOMA-IR) by regressing them according to age and sex and aggregating them. The optimal cut-off of cMetS for predicting MS was determined by the receiver operation characteristic (ROC) curve analysis.
Results
The cMetS increased significantly with increase in the number of MS risk factors. It was significantly high in children with MS than those without it (boys: 1.070 + 1.834 vs. -1.478 + 2.262; girls: 2.092 + 1.963 vs. -2.253 + 2.140; combined children group: 1.572 + 1.950 vs. -1.907+ 2.374; p < 0.001). The score predicted MS with high accuracy in girls; (AUC of 0.95, 95% CI: 0.90–1.00), moderate accuracy in boys (AUC of 0.79, 95% CI: 0.65–0.92) and in the combined group (AUC of 0.87, 95% CI 0.80–0.94) respectively. The cut-off of cMetS yielding maximal sensitivity and specificity for predicting the MS was −1.009 in boys (sensitivity 93% and specificity 62%); −0.652 in girls (sensitivity 96.4% and specificity 77%) and − 0.6881 in the combined group (sensitivity 91.2% and specificity 70.2%).
Conclusions
cMetS predicted MS with moderate to high accuracy. It had high sensitivity and specificity in predicting MS in overweight and obese children.
Similar content being viewed by others


Avoid common mistakes on your manuscript.
Introduction
Metabolic syndrome (MS) encompasses clustering of cardiometabolic risk factors consisting of abdominal adiposity, elevated levels of blood pressure (BP), serum triglycerides (TG) and glucose, as well as low serum high density lipoprotein-cholesterol (HDL-C) [1]. The presence of MS is associated with increased risk of cardiovascular disease, diabetes, some cancers, and all-cause mortality later in life [2].
The pandemic of childhood obesity has resulted in significant concerns regarding associated co-morbidities in the pediatric population with MS [3] . This condition is well defined in adults, however in pediatric age group; there is no universal and uniform definition for MS. Its prevalence has large variations according to the classification system used [4,5,6]. Traditional MS criteria are further limited by identifying risk only when a person exhibits abnormalities beyond the cut-off for three of the components of MS. Use of continuous metabolic syndrome risk score (cMetS) therefore has been suggested to overcome the limitations posed by dichotomous classification [4]. The American Diabetes Association and the European Association for the Study of Diabetes has recommended use of continuous value of MS risk score for investigating the association of MS with potential risk factors in children and adolescents [7].
The cMetS risk score is more robust measure of MS. Being a continuous variable, cMetS assumes that the increased cardiovascular risk is a progressive function of several MS risk factors [8]. It has greater statistical power; is more sensitive and less error prone compared with categoric measures of MS [9]. The continuous score is more reliable in predicting young adult risk from late childhood [10].
With this background of lack of a consensus definition for MS in children and cardiovascular risk being a progressive function of several components of MS, this study was aimed to identify prevalence of MS in overweight and obese children using cMetS, to identify the cut-offs’ for an adverse MS and compare the cMetS with the number of MS risk factors.
Material and Methods
This cross-sectional study was a part of Obesity Management Clinic in overweight and obese children attending Pediatrics Department Bhabha Atomic Research Centre Hospital. The Ethical permission was obtained (NP/BARC/2018/11), the consent of parents and assent from the children was sought. One hundred four overweight and obese children (7–14 y) underwent detailed clinical examination. Children with secondary obesity were excluded.
Weight (Wt) was measured on an electronic digital scale to the nearest 0.1 kg (Capri electronics, Model MI-120 T). Height (Ht) was measured to the nearest 0.1 cm using Stadiometer. Waist circumference (WC) was measured with an inelastic tape to the nearest 0.1 cm measuring at the end of normal expiration from the narrowest point between the lower borders of the rib cage and the iliac crest. The authors used Indian cut-off of >/=75th WC percentile to identify children at risk for MS [11]. BMI was computed using the following formula: BMI: weight (kg)/height (m)2. Children were classified as overweight and obese according to the Revised IAP growth charts 2015; adult equivalent of 23 and 27 cut-off presented in age- and gender-specific Revised Indian Academy of Pediatrics (IAP) growth standards were used to classify children as overweight and obese [12]. Blood pressure – Systolic (SBP) and diastolic blood pressure (DBP) was measured on right arm of the child with appropriate sized cuff, in a sitting position after 10 min rest by using mercury sphygmomanometer (Diamond, India). Average of two measurements was recorded. The SBP and DBP were compared with age and gender specific percentiles of BP measurements provided in the Report of the Second Task Force on Blood Pressure Control in Children [13]. Mean arterial pressure (MAP) was calculated as systolic blood pressure – diastolic blood pressure)/3 + diastolic blood pressure.
Blood sample was collected after 10–12 h fasting and analysed in the BARC Hospital Pathology Department. High density lipoprotein (HDL) and triglycerides (TG) were measured by enzymatic colorimetric method. Fasting blood glucose (FBS) and Serum insulin (S-Insulin) were determined with Glucose oxidase method and Chemiluminescence method respectively. Insulin resistance (IR) was determined using homeostatic model assessment for insulin resistance or HOMA-IR model as product of fasting glucose (mg/dl) x fasting insulin (μIU/ml)]/405 [14].
MS was defined according to the National Cholesterol Education Programme Adult Treatment Panel – III modified for age criteria by De Ferranti et al. [15]. Children with presence of any three components: TG >/= 100 mg/dl, HDL level < 50 mg/dl, Fasting Glucose (FBS) >/= 110 mg/dl, WC > 75th percentile for age and gender and systolic blood pressure > 90th percentile for gender, age and height were categorized as having MS.
The cMetS was calculated using the Residual Z- score approach as described by Eisenmann [9]. The variables to be represented in the score i.e., WC, MAP, HOMA, HDL-C, and TG were first standardized by regressing them on the age in boys and girls separately. The standardized residual Z-score were saved. The standardized HDL-C was multiplied by (−1), as it is inversely related to metabolic risk. The standardized residuals for the individual risk factors were summed to create the cMetS. A higher score is indicative of a less favourable MS profile.
Statistical analyses was conducted using SPSS version 25 (SPSS Inc. Chicago, IL) statistical package. All variables were checked for normality; normalised using log transformation and presented as mean ± standard deviation. Frequencies were reported in number (percentage). The independent sample T test was used to compare continuous variables and the Chi square test was used to compare proportions. Comparison of continuous variables between more than two groups was done by ANOVA test. To estimate valid cut-off values of cMetS for predicting MS, the receiver operation characteristic (ROC) curve analysis was performed with an estimation of the sensitivity and specificity. The estimated cut-off values were determined using the minimum value which represents the maximum sum of sensitivity and specificity.
Results
One hundred four overweight and obese children (48% boys and 52% girls) participated in this study. The general characteristics of the children including anthropometric and biochemical measurements according to gender are presented in Table 1. There was no significant difference in mean age, weight, height, BMI, SBP, DBP, MAP, TG, FBS, S-Insulin and HOMA-IR between boys and girls. However boys had high mean WC and low mean HDL levels compared to girls (P < 0.05).
Table 2 presents the prevalence of individual metabolic risk factors, number of risk factors and prevalence of MS in children according to NCEP-ATP-III criteria [15]. Overall, 85.6%, 71.2% 48.1%, 36.5% and 8.7% children had low HDL, high WC, TG, SBP and FBS. Regarding presence of number of risk factors of MS, 19.2%, 23.1%, 33.7% and 20.2% children had one, two, three and four risk factors respectively. Three boys (2.9%) did not have any risk factor and one boy had all five risk factors for MS. There was no significant gender difference in either the prevalence of individual risk factor or the number of risk factors present.
The prevalence of MS in children was 54.8%. There was no significant difference in the prevalence between the boys (58.0%) and girls (51.9%). Obese children with MS had significantly higher BMI, WC, SBP, DBP and TG than those without MS (p < 0.001).
The cMetS was constructed as mentioned in methods section. Table 3 demonstrates the relationship between cMetS and the number of MS risk factors. Children with higher number of MS risk factors and with presence of MS had higher cMetS (p < 0.001). ANOVA result after categorizing the children into </= 1, 1, 2 & +3 risk factors groups revealed that mean cMetS score increased significantly with increase in the number of risk factors, (p < 0.001). The mean cMetS was significantly high in children with metabolic syndrome than those without it (boys: 1.070 ± 1.834 vs. -1.478 ± 2.262; girls: 2.092 ± 1.963 vs. -2.253 ± 2.140; combined children group: 1.572 ± 1.950 vs. -1.907 ± 2.374; p < 0.001).
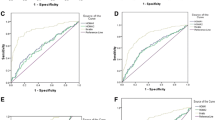
To evaluate cMetS, ROC curve analysis was carried out for boys and girls separately and combined children group to find how the cMetS performed to predict MS (Fig. 1a–c). The result demonstrated that cMetS was highly accurate in girls; AUC of 0.95 (95% CI: 0.90–1.00) and moderately accurate in boys; AUC of 0.79 (95% CI: 0.65–0.92). The cMetS cut-off to predict MS in girls was −0.652 (sensitivity 96.4% and specificity 77%) and in boys it was −1.009 (sensitivity 93% and specificity 62%) respectively. For the combined group cMetS was moderately accurate to predict MS with AUC of 0.87 (95% CI 0.80–0.94). A cMetS cut-off −0.6881 had 91.2% sensitivity and 70.2% specificity in this group. The authors observed that, more children i.e., 63.5% (n = 66) had MS scores above this cut-off; prevalence of MS now was 8.7% higher than that found according to the classification proposed by de Ferranti et al. [15].

a ROC curve for Metabolic syndrome in (a) total population, (b) boys and (c) girls
Discussion
In this study population of overweight and obese children, a high prevalence (54.8%) of MS was observed (boys 58.0% and girls 51.9%) using NCEP – ATP III criteria. Children and adolescents who have high levels of BMI are likely to have multiple risk factors, excess adiposity, and higher prevalence of metabolic syndrome [3, 16,17,18,19,20,21].
The cMetS was constructed using residual Z score method described by Eisenmann [9] and a graded relationship was observed between cMetS and the number of MS risk factors in boys, girls and combined children group. Increase in the mean cMetS was noticed with increase in the number of MS risk factors and those with equal or more than 3 risk factors had the highest cMetS. The cMetS was significantly high in children with MS. The mean cMetS amongst children with MS was 1.57 ± 1.95, compared to −1.907 ± 2.374 in those without MS. Similar findings were observed in boys and girls. The present findings are consistent with the findings of high cMetS in children with MS than those without it [3,4,5, 17, 18].
The results of the ROC analysis indicated different cut-off points of cMetS in boys and girls and it was found to be performing highly accurate in girls and moderately accurate in boys for predicting MetS. The score was highly sensitive and specific in both the genders and in the combined group. Various studies on the utility of cMetS have documented the score to be highly sensitive and specific to predict MS [4, 5, 17]. Regarding the optimal cut-offs’ of cMetS, higher value was observed in girls compared to boys. In a study on the efficacy of cMetS in Indian children by Pandit et al., similar finding of higher cut-off in girls compared to the boys has been reported [17]. It is important to highlight here that prevalence of MS using dichotomous definition in present study population was high in boys than girls though statistically not significant but cMetS was higher in girls. This again puts emphasis on the continuous nature of the MS.
Review of literature has demonstrated different cut-offs for cMetS using different statistical methods and different criteria to define MS. The cut-offs’ in the present study population are sample specific as cMetS is calculated using the residual Z scores of the individual components of MS hence it cannot be compared with other studies. This is one limitation of the study. The other limitation is inability to study the influence of biological maturity on cMetS due to less number of children in pre-pubertal age group.
Studies have demonstrated significant relationship between childhood MS, defined by cMetS, and adult cardiovascular risk [10, 21]. The range of cMetS found in present study population supports the observation that cardiovascular risk status varies even within the “high-risk” overweight and obese children [22]. Children with higher cMetS and therefore, unhealthy metabolic profile are at increased risk of complications. They should be prioritized for receiving aggressive care for managing their obesity and changes in the cMetS over a time period will signify the effectiveness of an intervention [23]. Also this cohort with unhealthy metabolic score will need long- term follow until they reach adulthood to identify the influence of cMetS on the adult MS, cardiovascular disease, atherosclerosis and diabetes.
Recently, reference values for cardiometabolic risk factors for European, American and Iranian children are available [5, 24]. There is a need to have reference values for the cardiometabolic risk factors for Indian children. This will allow standardization of cMetS and also make the score comparable to the reference values. Thus it will increase the prospects to estimate and compare prevalence and trends of cardiometabolic risk in children. This score is becoming widely used in pediatric epidemiological research and additional studies are needed for using this score in clinical practice.
Conclusions
The cMetS predicted MS with moderate to high accuracy. It had high sensitivity and specificity in predicting MS in overweight & obese children. With the pandemic of obesity and increase in burden of cardiovascular diseases and diabetes in our country, there is a need to have reference values for the cardiometabolic risk factors for Indian children.
References
National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and treatment of high blood cholesterol in adults (adult treatment panel III) final report. Circulation. 2002;106:3143–421.
Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes Care. 2005;28:1769–78.
Thivel D, Malina RM, Isacco L, Aucouturier J, Meyer M, Duche' P. Metabolic syndrome in obese children and adolescents: dichotomous or continuous? Metab Syndr Relat Disord. 2009;7:549–55.
Heshmat R, Heidari M, Ejtahed HS, et al. Validity of a continuous metabolic syndrome score as an index for modeling metabolic syndrome in children and adolescents: the CASPIAN-V study. Diabetol Metab Syndr. 2017;9:89.
Guseman EH, Eisenmann JC, Laurson KR, Cook SR, Stratbucker W. Calculating a continuous metabolic syndrome score using nationally representative reference values. Acad Pediatr. 2018;18:589–92.
Minakshi B, Chithambaram NS. Early identification of risk factors and diagnosis of metabolic syndrome in overweight and obese children above 6 years of age. Int J Contemp Pediatrics. 2017;4:1439–44.
Kahn R, Ferrannini E, Buse J, Stern M. The metabolic syndrome: time for a critical appraisal. Joint statement from the American Diabetes Association and the European Association for the Study of diabetes. Diabetes Care. 2005;28:2289–304.
Villa JKD, e Silva AR, Santos TSS, Ribeiro AQ, Sant'Ana LFdaR. Metabolic syndrome risk assessment in children: use of a single score. Rev Paul Pediatr [Internet]. 2015;33:187–93. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-05822015000200187&lng=en. https://doi.org/10.1016/j.rpped.2014.11.001. Accessed 15 April 2019.
Eisenmann JC. On the use of a continuous metabolic syndrome score in pediatric research. Cardiovasc Diabetol. 2008;7:17.
Kelly AS, Steinberger J, Jacobs DR, Hong CP, Moran A, Sinaiko AR. Predicting cardiovascular risk in young adulthood from the metabolic syndrome, its component risk factors, and a cluster score in childhood. Int J Pediatr Obes. 2011;6:e283–9.
Khadilkar A, Ekbote V, Chiplonkar S, et al. Waist circumference percentiles in 2-18 year old indian children. J Pediatr. 2014;164:1358–62.
Khadilkar V, Yadav S, Agrawal KK, et al. Revised IAP growth charts for height, weight and body mass index for 5- to 18-year-old Indian children. Indian Pediatr. 2015;52:47–55.
Report of the Second Task Force on Blood Pressure Control in Children—1987. Task Force on Blood Pressure Control in Children. National Heart, Lung, and Blood Institute, Bethesda, Maryland. Pediatrics 1987;379:1–25.
Majid H, Masood Q, Khan AH. Homeostatic model assessment for insulin resistance (HOMA-IR): a better marker for evaluating insulin resistance than fasting insulin in women with polycystic ovarian syndrome. J Coll Physicians Surg Pak. 2017;27:123–6.
de Ferranti SD, Gauvreau K, Ludwig DS, Neufeld EJ, Newburger JW, Rifai N. Prevalence of the metabolic syndrome in American adolescents: findings from the third National Health and Nutrition Examination Survey. Circulation. 2004;110:2494–7.
Wittcopp C, Conroy R. Metabolic syndrome in children and adolescents. Pediatr Rev. 2016;37:193–202.
Pandit D, Chiplonkar S, Khadilkar A, Kinare A, Khadilkar V. Efficacy of a continuous metabolic syndrome score in Indian children for detecting subclinical atherosclerotic risk. Int J Obes [Internet]. 2011;35:1318–24.
Okosun IS, Boltri JM, Lyn R, Davis-Smith M. Continuous metabolic syndrome risk score, body mass index percentile, and leisure time physical activity in American children. J Clin Hypertens. 2010;12:636–44.
Andrabi SMS, Bhat MH, Andrabi SR, et al. Prevalence of metabolic syndrome in 8-18-year-old school-going children of Srinagar city of Kashmir India. Indian J Endocr Metab. 2013;17:95–100.
Tandon N, Garg MK, Singh Y, Marwaha RK. Prevalence of metabolic syndrome among urban Indian adolescents and its relation with insulin resistance (HOMA-IR). J Pediatr Endocrinol Metab. 2013;26:1123–30.
Freedman DS, Khan LK, Serdula MK, Dietz WH, Srinivasan SR, Berenson GS. The relation of childhood BMI to adult adiposity: the Bogalusa heart study. Pediatrics. 2005;115:22–7.
Prince RL, Kuk JL, Ambler KA, Dhaliwal J, Ball GDC. Predictors of metabolically healthy obesity in children. Diabetes Care. 2014;37:1462–8.
Magnussen CG, Cheriyan S, Sabin MA, et al. Continuous and dichotomous metabolic syndrome definitions in youth predict adult type 2 diabetes and carotid artery intima media thickness: the cardiovascular risk in young Finns study. J Pediatr. 2016;171:97–103.e3.
Stavnsbo M, Resaland GK, Anderssen SA, et al. Reference values for cardiometabolic risk scores in children and adolescents: suggesting a common standard. Atherosclerosis. 2018;278:299–306.
Acknowledgements
The authors thank all children and their parents who agreed for the participation in this study. They acknowledge help of Dr. Susan Cherian, Head Pathology, BARC Hospital and Dr. A. R. Kulkarni, MO-In-charge, Medical Section, BARC Hospital.
Author information
Authors and Affiliations
Contributions
SPS: Data collection, statistical analysis, manuscript preparation and editing the manuscript. ASA: Data collection and editing the manuscript. ASA is the guarantor for this paper.
Corresponding author
Ethics declarations
Conflict of Interest
None.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sawant, S.P., Amin, A.S. Use of Continuous Metabolic Syndrome Score in Overweight and Obese Children. Indian J Pediatr 86, 909–914 (2019). https://doi.org/10.1007/s12098-019-02994-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s12098-019-02994-5